
Abstract
Study Design
A retrospective comparative study.
Objectives
This study investigated radiographical changes in global spinal sagittal alignment (GSSA) and clinical outcomes after tumor resection without spinal fusion in patients with thoracic dumbbell tumors.
Methods
Thirty patients with thoracic dumbbell tumors who were followed up for at least 3 years were included in this study. Variations in the outcome variables were analyzed using individual GSSA parameters measured on radiography. Clinical outcomes were assessed using the modified McCormick scale (MMCS), Japan Orthopaedic Association (JOA) score, and visual analog scale (VAS). To assess the impact of the affected levels on these outcomes, we divided the patients into three groups according to the location of the tumor (upper [T1-4], middle [T5-8], or lower [T9-12] thoracic spine).
Results
The GSSA parameters (cervical lordosis, T1 slope, thoracic kyphosis [global, upper, middle, and lower], thoracolumbar kyphosis, lumbar lordosis, sacral slope, pelvic incidence, and pelvic tilt) of all the patients did not change significantly after surgery. Eleven of thirty patients had preoperative gait disturbances but they could walk without support (MMCS grade I or II) at the final follow-up. The JOA score and VAS showed significant postoperative improvements. No statistically significant differences were observed in each postoperative sagittal profile or clinical outcome between the upper, middle, and lower groups.
Conclusions
Tumor resection without spinal fusion did not affect the various GSSA parameters and resulted in satisfactory clinical outcomes, indicating that spinal fusion may not always be necessary when resecting thoracic dumbbell tumors.
Keywords
Introduction
Dumbbell-shaped tumors are relatively rare neoplasms, with an incidence rate of 18% of all spinal cord tumors. 1 The tumors most commonly occur in the cervical spine (44%), followed by the thoracic spine. 1 To date, several surgical approaches, including anterolateral one-way, posterior one-way, and combined approaches, have been considered for resecting such tumors.2-8 In particular, a posterior one-way approach, such as laminectomy with unilateral facetectomy, is a standard technique that allows the safe removal of the intra- or extraspinal and foraminal components of the tumors with sufficient space after direct decompression at the level of tumor localization.3,5,7 However, this approach might cause postoperative spinal deformities, such as local instability or subsequent kyphosis. This is because it causes more extensive damage to the posterior elements of the spinal column than that caused by the usual resection of thoracic spinal cord tumors localized to the spinal canal.3,4,6 Although concomitant spinal fusion is occasionally required to prevent post-laminectomy deformity and stabilize the spine after tumor resection, it may cause postoperative complications related to spinal instrumentation.9-11 Thus, the appropriate surgical procedure for resecting thoracic dumbbell tumors is still controversial.
Postoperative global spinal sagittal alignment (GSSA) has recently been regarded as an increasingly important subject associated with clinical and functional outcomes in patients with spinal cord tumors.12-15 Some reports have shown that spinal deformity occurs at a rate of approximately 10% following surgery for spinal cord tumors.1,3,12 Postoperative spinal sagittal malalignment can lead to neurological deterioration, pain, and posture problems.12-16 However, several studies have focused on assessing only the changes in sagittal alignment around the levels of tumor resection and have not examined the postoperative changes in overall GSSA.13,14,17 As no studies have examined radiographical changes in GSSA after surgical resection without spinal fusion in patients with thoracic dumbbell tumors, investigating the clinical association of the procedure with the GSSA parameters is essential to identify the benefits of the surgical procedure.
This study aimed to examine radiographical changes in various GSSA profiles and clinical outcomes following surgical resection without spinal fusion in patients with thoracic dumbbell tumors and evaluate the possible factors that influence postoperative GSSA.
Materials and Methods
Study Design, Patient Demographics, and Characteristics
Thirty patients with thoracic dumbbell tumors who required primary resection via the posterior approach without spinal instrumentation at our institution between 2007 and 2017 were included and consecutive in this study. For tumor resection, all patients underwent spinous process-splitting laminectomy (SPSL) or hemilaminectomy (HL) with unilateral facetectomy (approximately one-half to two-thirds of the inside facet joint was removed) at the affected level, depending on the extent of the tumor. The inclusion criteria were as follows: (1) diagnosis of thoracic dumbbell tumor (Eden type I, intradural and extradural; II, intradural, extradural, and paravertebral; III, extradural and paravertebral; or IV, foraminal and paravertebral 18 ) at 18 years of age or above; (2) absence of congenital vertebral deformity, trauma, neuromuscular disorders, or other pathological conditions; (3) no history of spinal surgery; and (4) a minimum of 3-year follow-up after surgery. The exclusion criteria were as follows: history of postoperative radiotherapy and/or chemotherapy and presence of cervical or lumbar spinal cord tumors with the center of the tumor located above C7 or below L1, intramedullary spinal cord tumors, non-dumbbell tumors localized to only the spinal canal, and extradural spinal cord tumors, such as metastatic tumors. To analyze the impact of the affected levels on postoperative GSSA parameters and clinical outcomes, the 30 patients who met the criteria for the study were divided into three groups based on tumor location (in which the central region of the tumor was located at the level of upper, T1-4; middle, T5-8; or lower, T9-12) as previously reported for assessing ossification of the posterior longitudinal ligament and thoracic spinal cord tumors.14,19 All information regarding demographics (age at surgery, sex, Eden classification, tumor location, and histopathology of tumor), imaging, and surgical data (surgical time, estimated blood loss [EBL], surgical procedure, rate of tumor resection, postoperative complications, and postoperative follow-up period) were retrospectively obtained by reviewing the patient’s records and radiological images.
This study was approved by the Ethics and Institutional Review Board (Keio university school of medicine, approval number: #20110142), and all participants provided informed consent to be included in the study before tumor resection.
Radiographical and Magnetic Resonance Imaging Data
All patients in this study underwent whole-spine radiological assessment at the preoperative and final follow-up stages. Radiographic findings included standing erect whole-spine posteroanterior and lateral radiographs. To obtain lateral radiographs, the patients stood looking straight ahead with their knees locked, feet shoulder-width apart, elbows bent, and knuckles in the supraclavicular fossa bilaterally. 20
We examined the following GSSA profiles: C2-7 cervical lordosis (CL), T1 slope, T1-12 global thoracic kyphosis (GTK), T10–L2 thoracolumbar kyphosis (TLK), L1-5 lumbar lordosis (LL), sacral slope (SS), pelvic incidence (PI), and pelvic tilt (PT). GTK was subdivided into three segments, including T1-4 upper thoracic kyphosis (UTK), T5-8 middle thoracic kyphosis (MTK), and T9-12 lower thoracic kyphosis (LTK). Three of the study authors independently analyzed the radiographs. An experienced spine surgeon reviewed the medical records and radiographs of all the patients. The intraobserver reliability tested using the intraclass correlation coefficient (ICC; 1, 1) and ICC (1, 3) formula was .83 and .92, respectively. To assess the interobserver error, 30 randomly chosen radiographs were assessed by three spine surgeons who were not directly involved in the surgeries independently. The interobserver reliability tested using the ICC (2, 1) and ICC (2, 3) formula was .85 and .93, respectively.
MRI was performed postoperatively to confirm the extent of tumor resection, which was classified into two types according to the operative records: gross total resection (GTR) and partial resection (PR). The standard definition of GTR was used in this study (i.e., 100% removal of the tumor based on the absence of a remnant tumor documented microscopically and no evidence of neoplasm at the site of tumor origin). The procedure was considered PR when a small tumor fragment or an extraforaminal or paravertebral portion was not resected, based on a documented removal of 50%–99% of the tumor on intraoperative ultrasonography or postoperative MRI findings. 21
Clinical Outcomes and Functional Evaluation
Clinical outcomes and functional effectiveness were assessed at the preoperative and final follow-up stages using the Japanese Orthopaedic Association (JOA) scoring system (11 possible points), and the degree of chest-to-toe pain or numbness was assessed using the visual analog scale (VAS; the score ranges from 0 to 100, with lower scores indicating a comfortable condition without any pain or numbness). The JOA score recovery rate (%) was calculated as follows: (final follow-up JOA score − preoperative JOA score)/(11 − preoperative JOA score) × 100. We also evaluated the degree of gait disturbance preoperatively and at the final follow-up using the modified McCormick scale (MMCS; grade I, normal gait; grade II, mild gait disturbance not requiring support; grade III, gait disturbance requiring support; grade IV, requiring assistance; and grade V, wheelchair needed).22,23
Statistical Analysis
All continuous data are expressed as means ± standard error of the means, and categorical data are presented as percentages. Radiographical findings and clinical outcomes were compared between the preoperative and final follow-up stages using the Wilcoxon signed-rank test, between the upper, middle, and lower groups using the Kruskal–Wallis test, followed by Dunn’s multiple comparisons post-hoc test, and between SPSL and HL groups using the Mann–Whitney U test, respectively. P values <.05, <.01, and <.001 were considered statistically significant. All statistical analyses were performed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Patients’ Demographics, Clinical Characteristics, and Surgical Data
The current study included 17 men (56.7%) and 13 women (43.3%) with ages at surgery ranging from 20 to 86 years (mean age, 50.1 ± 17.2 years). According to the Eden classification, 2 cases (6.7%) were type I, 9 (30.0%) were type II, 12 (40.0%) were type III, and 7 (23.3%) were type IV. The most frequent tumor locations were the T8-9 and T9-10 levels (5 cases [16.7%]).
Demographics, Clinical Characteristics, and Surgical Data of all Patients.
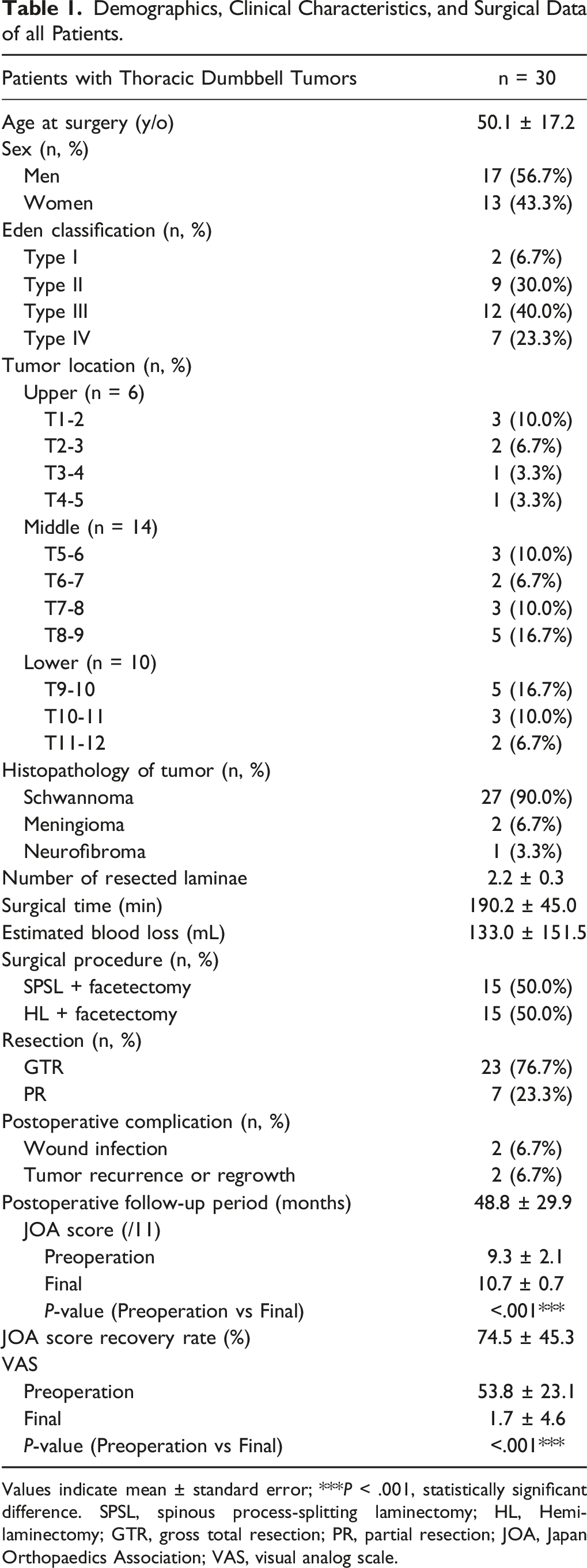
Values indicate mean ± standard error; ***P < .001, statistically significant difference. SPSL, spinous process-splitting laminectomy; HL, Hemilaminectomy; GTR, gross total resection; PR, partial resection; JOA, Japan Orthopaedics Association; VAS, visual analog scale.
Postoperative Changes in Sagittal Spinal Alignment
Comparison of Preoperative and Final Follow-Up Spinal Sagittal Parameters of the Patients.
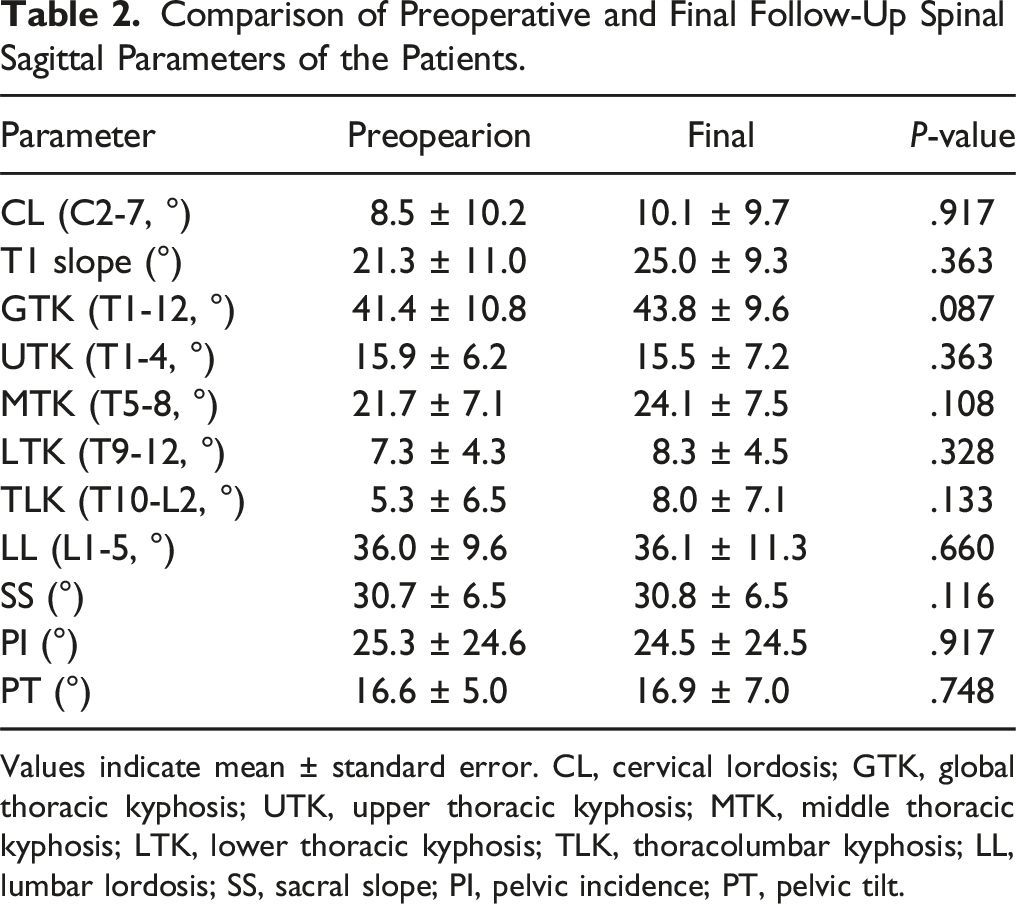
Values indicate mean ± standard error. CL, cervical lordosis; GTK, global thoracic kyphosis; UTK, upper thoracic kyphosis; MTK, middle thoracic kyphosis; LTK, lower thoracic kyphosis; TLK, thoracolumbar kyphosis; LL, lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt.
Correlation Analysis Between the Postoperative Changes in Individual Thoracic Kyphosis Parameters and Age at Surgery or Preoperative UTK, MTK, LTK, or GTK.
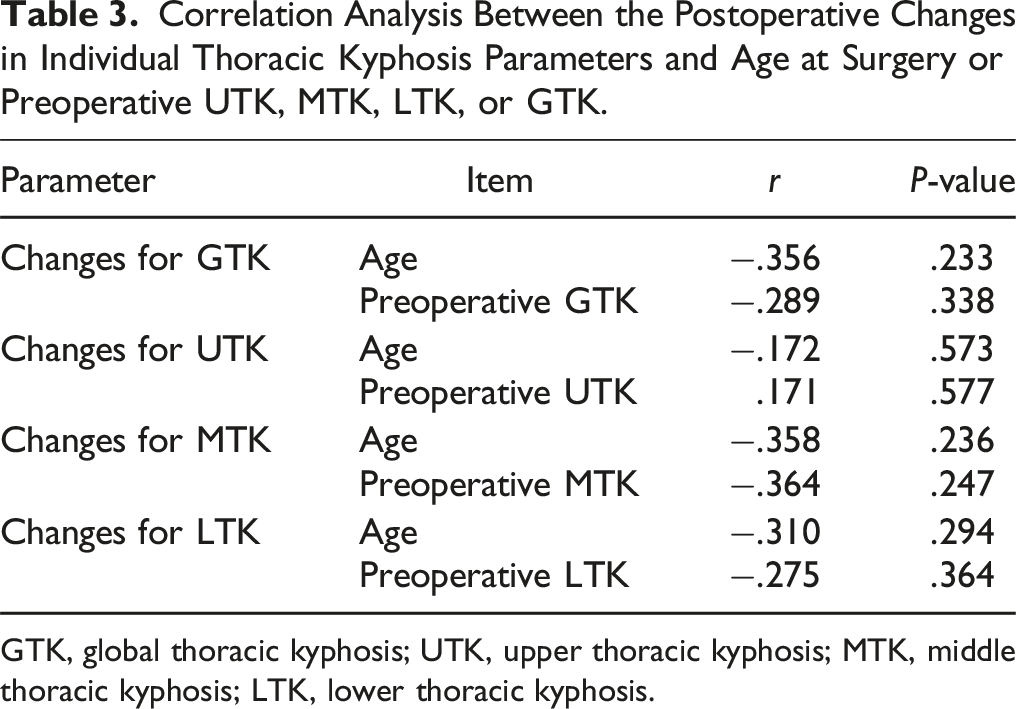
GTK, global thoracic kyphosis; UTK, upper thoracic kyphosis; MTK, middle thoracic kyphosis; LTK, lower thoracic kyphosis.
Changes in Each Modified McCormick Scale Grade After Thoracic Dumbbell Tumor Resection Without Spinal Fusion
Summary of Changes in the MMCS Grade of Patients at the Final Follow-Up.
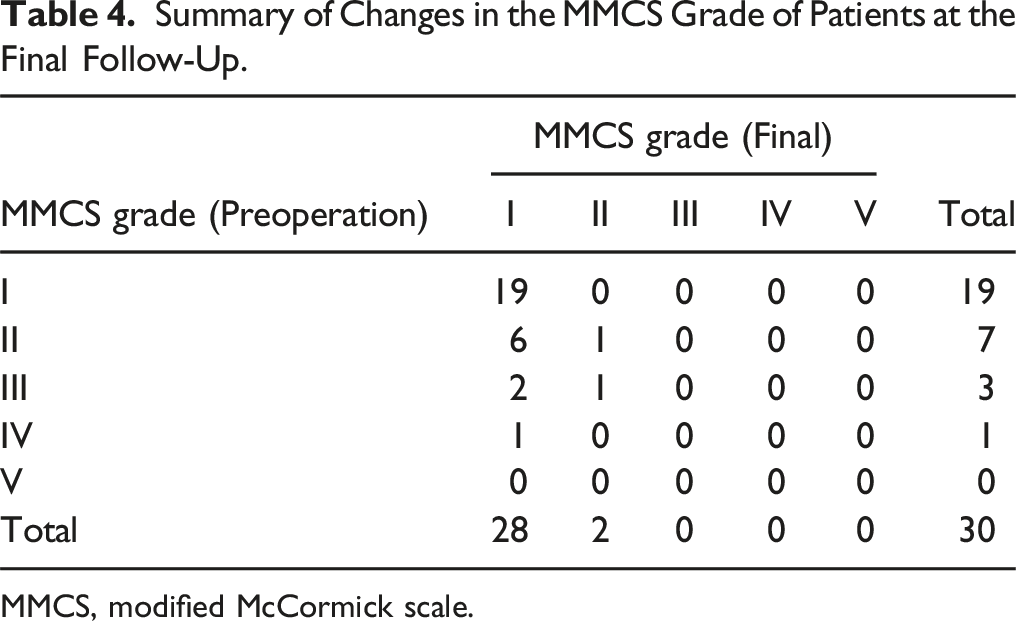
MMCS, modified McCormick scale.
Comparison of Each Sagittal Spinal Profile and Clinical Outcomes Between the Upper, Middle, and Lower Groups
Comparison of Each Sagittal Spinal Parameter Between the Upper, Middle, and Lower Groups.
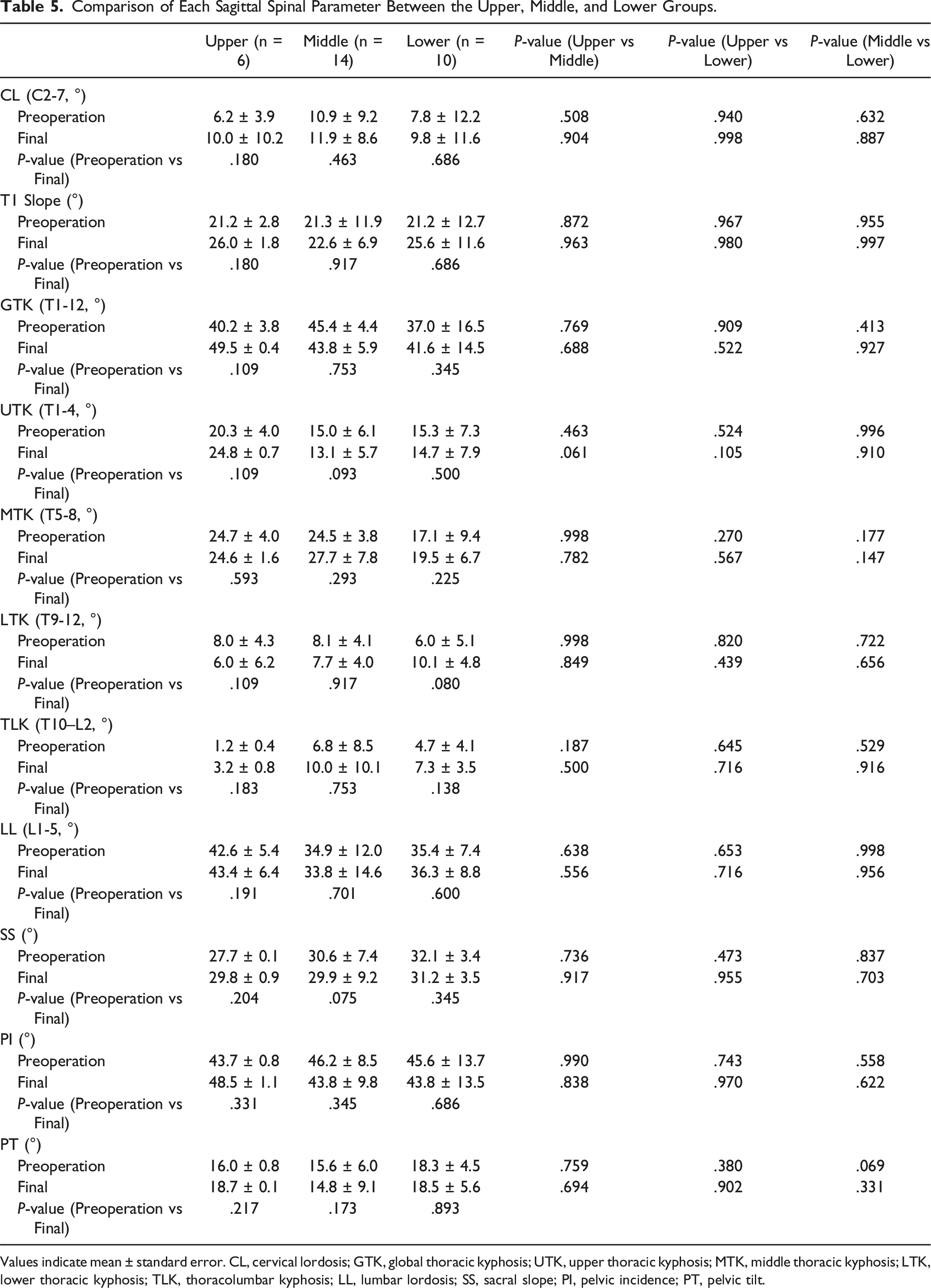
Values indicate mean ± standard error. CL, cervical lordosis; GTK, global thoracic kyphosis; UTK, upper thoracic kyphosis; MTK, middle thoracic kyphosis; LTK, lower thoracic kyphosis; TLK, thoracolumbar kyphosis; LL, lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt.
Comparison of Neurological Status and Clinical Outcomes Between the Upper, Middle, and Lower Groups.
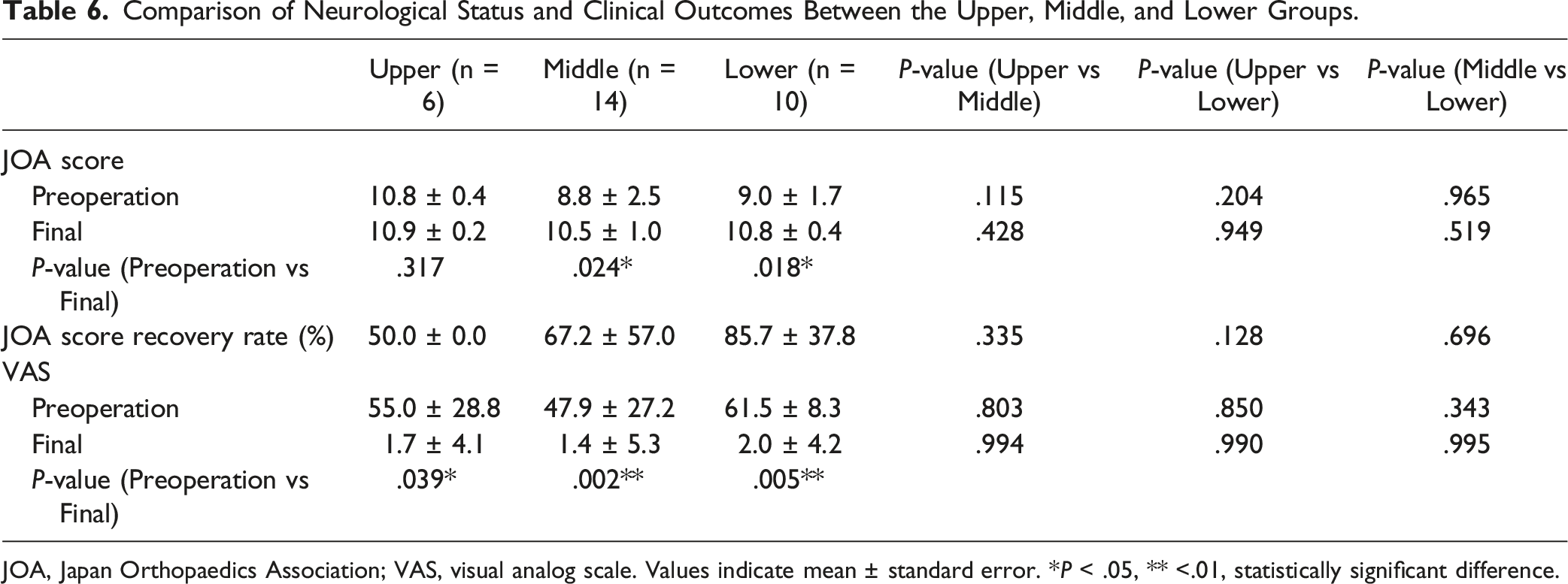
JOA, Japan Orthopaedics Association; VAS, visual analog scale. Values indicate mean ± standard error. *P < .05, ** <.01, statistically significant difference.
Comparison of Each Sagittal Spinal Parameter by Surgical Approach
Comparison of Each Sagittal Spinal Parameter Between the SPSL and HL Groups.
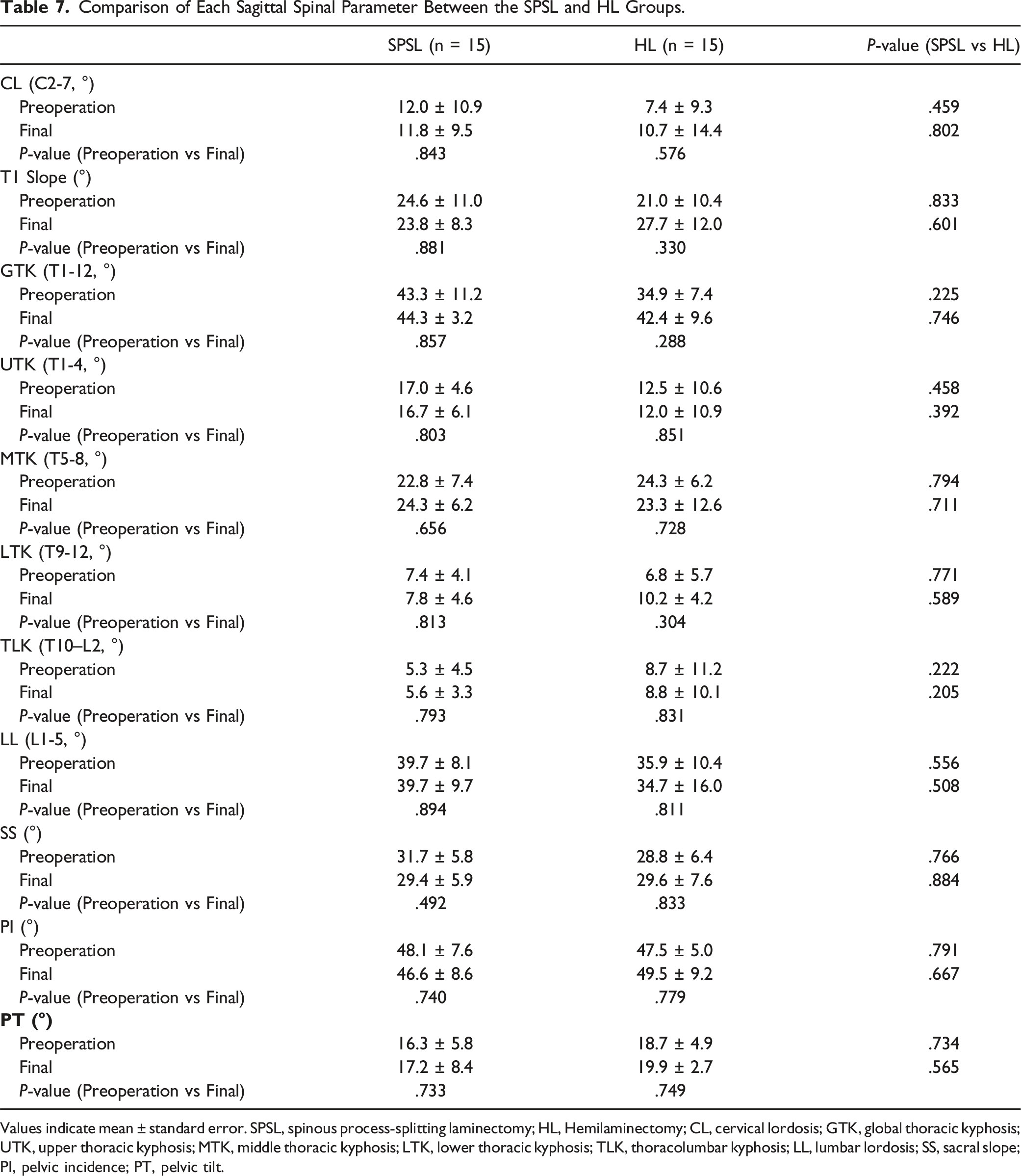
Values indicate mean ± standard error. SPSL, spinous process-splitting laminectomy; HL, Hemilaminectomy; CL, cervical lordosis; GTK, global thoracic kyphosis; UTK, upper thoracic kyphosis; MTK, middle thoracic kyphosis; LTK, lower thoracic kyphosis; TLK, thoracolumbar kyphosis; LL, lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt.
Representative Case
A 31-year-old woman patient complained of lower extremities numbness and gait disturbance. Her MRI showed a dumbbell-shaped tumor (Eden type II) on the left side at the T10/11 spinal level (Figure 1A). The posterior SPSL approach with facetectomy was selected for tumorectomy, which resulted in GTR. The histopathologic finding of the tumor was schwannoma. Four years postoperatively, her MRI did not indicate any tumor recurrence (Figure 1B), the patient was in good condition without any symptoms. Global spinal sagittal alignment did not show any significant progression of instability or degeneration on 4-year postoperative whole spine standing sagittal radiographs for this patient (Figure 1C–D). Representative MR and radiographic images of a patient with thoracic dumbbell tumor. (A–B) The arrow indicated the area where the resected tumor existed at the T10/11 level in the preoperative and postoperative T2-weighted MR images. (C–D) No occurrence of spinal instability or deformity was observed at the lesion level. Whole spine standing sagittal radiographs did not demonstrated significant changes from preoperation to 4-year postoperation (CL, 8.6° to 5.3°; T1 slope, 12.8° to 11.5°; GTK, 28.7° to 33.2°; UTK, 9.1° to 8.0°, MTK, 12.1° to 16.9°; LTK, 7.5° to 8.5°; TLK, 2.3° to 8.1°; LL, 41.3° to 41.2°; SS, 32.2° to 29.1°; PI, 47.3° to 40.1°; PT, 15.1° to 11.0°). CL, cervical lordosis; GTK, global thoracic kyphosis; UTK, upper thoracic kyphosis; MTK, middle thoracic kyphosis; LTK, lower thoracic kyphosis; TLK, thoracolumbar kyphosis; LL, lumbar lordosis; SS, sacral slope; PI, pelvic incidence; PT, pelvic tilt.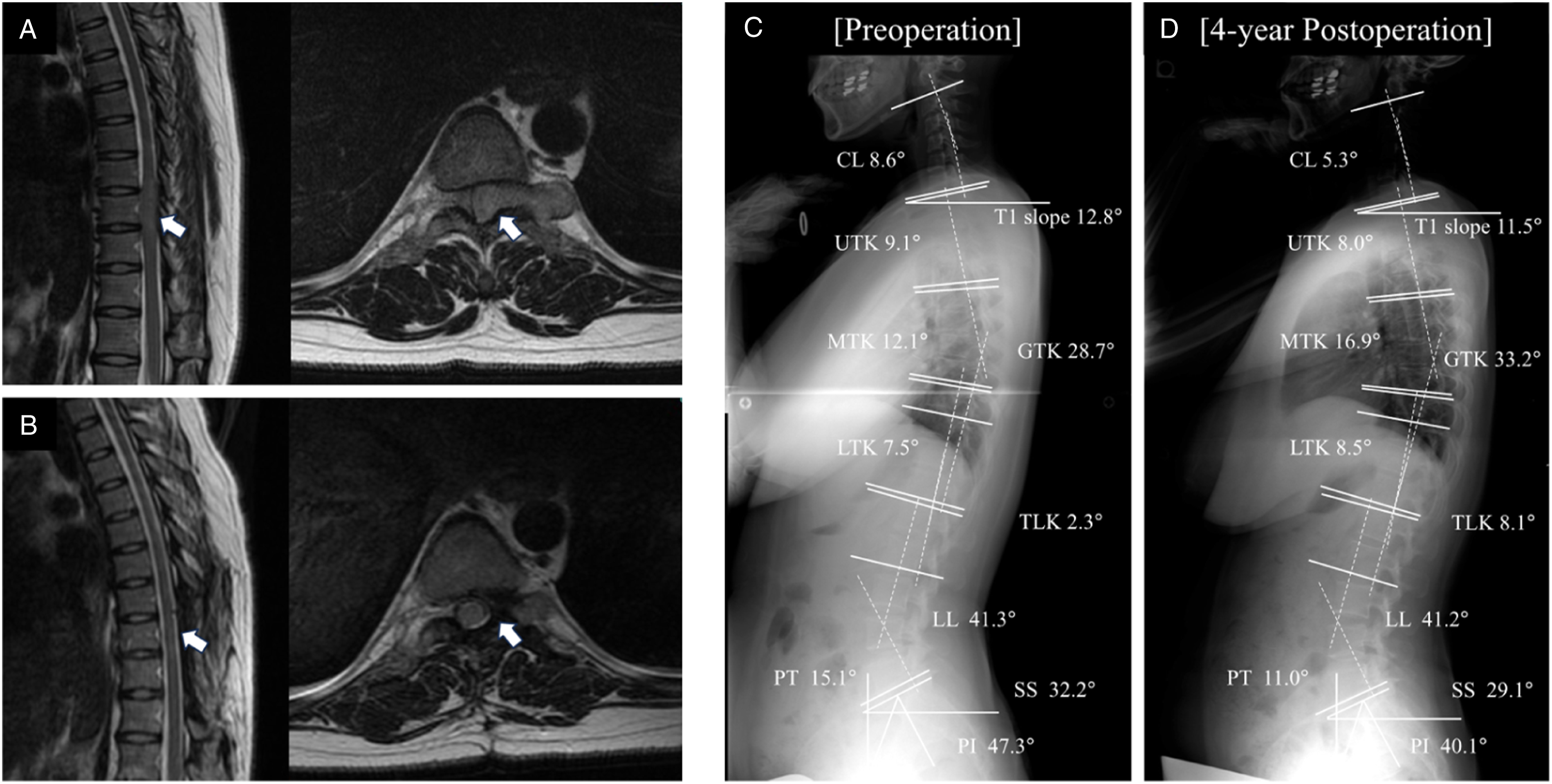
Discussion
This study is the first to compare various GSSA parameters before and after surgical resection without spinal fusion in patients with thoracic dumbbell tumors. We found that individual GSSA parameters were unaffected by tumor removal, and clinical outcomes significantly improved. In addition, when the participants were grouped on the basis of tumor distribution (upper, middle, and lower thoracic spine), no significant group differences were observed in individual preoperative and postoperative GSSA profiles. Our findings have important implications for studies that aim to evaluate the utility of tumor resection without spinal fusion in patients with thoracic dumbbell tumors as no studies have examined changes in postoperative GSSA parameters.
During the resection of thoracic dumbbell tumors, the facet joint must be occasionally sacrificed to remove the intra- or extra-foraminal and paravertebral portion of the tumor, which may cause postoperative spinal sagittal malalignment.2-5 Furthermore, several reports have shown that removing more than two laminae or performing facetectomy during an initial surgery would increase the incidence of postoperative spinal deformity.4,8-10 In contrast, Aizawa et al. reported that 10 patients with thoracic dumbbell tumors who underwent hemilaminectomy and facetectomy without spinal fusion had limited postoperative changes in local kyphosis and scoliosis angles on radiographs. 5 Rong et al. reported that 14 patients with thoracic dumbbell tumors had no aggravating deformity or instability after surgery. 24 Moreover, Ishikawa et al. examined the mid-to-long-term clinical and radiological outcomes of patients who underwent unilateral total facetectomy without instrumented fusion for the resection of thoracic dumbbell tumors. They indicated that no patient demonstrated postoperative instability or spinal deformity that required additional surgery. 7 However, these studies focused on assessing only the radiographical changes in local sagittal parameters around the levels of tumor resection and did not examine changes in the overall GSSA. Our study showed that various GSSA parameters did not change significantly after surgery, and the surgical outcomes were satisfactory, suggesting that resection without spinal fusion is valuable for improving the outcomes of patients with thoracic dumbbell tumors.
Previous reports have demonstrated that the development of postoperative spinal deformity would depend on the tumor localization level.13,14,16,17 Particularly, concerning thoracic spinal cord tumors, Kobayashi et al. reported that sagittal spinal alignment did not change postoperatively in patients who underwent middle and lower thoracic intraspinal tumor resection, even without spinal fusion. In contrast, postoperative kyphosis may increase when the tumor is located in the upper thoracic spine. 14 Ishikawa et al. reported that postoperative radiographic measurements and clinical outcomes were comparable between patients with thoracolumbar dumbbell tumor and those with middle thoracic dumbbell tumors after tumor resection without spinal fusion. 7 Furthermore, in this study, no significant differences were observed in both preoperative and postoperative GSSA parameters of the upper, middle, and lower groups. These discrepancies among the studies may be due to differences in the number of resected laminae. In particular, the upper thoracic levels (T1-4) are included in the cervical–thoracic junction (CTJ), which is in the C7-T3/4 region, and the CTJ is strongly correlated with postoperative instability owing to its anatomical features. Moreover, the transition from the mobile articulated cervical spine, which is lordotic, to the rigid thoracic spine, which is kyphotic in the CTJ, creates a mechanical vulnerability that may increase postoperatively. 25 In intraspinal canal tumors, the number of resected laminae is necessarily significant because the tumor grows and invades the spinal canal craniocaudally. In contrast, dumbbell-shaped tumors often require the resection of a relatively small number of laminae because the tumor invasion into the spinal canal is less and into the intervertebral foramen and paravertebral bodies is extensive. Thus, it is likely that the number of resected laminae due to these developmental tumor patterns could influence the surgical invasion of the posterior supporting tissues and contribute to progressive kyphosis.
Concomitant spinal fusion with instrumentation is occasionally required to prevent post-laminectomy deformities or instability in patients with dumbbell-shaped spinal cord tumors. Moreover, if postoperative spinal sagittal alignment and clinical outcomes deteriorate, fixation could be considered as a second-stage surgery for the thoracic spine after careful observation.9,10 This procedure has several disadvantages, including blurred postoperative MRI findings due to metallic artifacts and biofilm formation around the spinal instrumentation. 11 In addition, more than three vertebrae must be fused using bilateral fixation in some cases, resulting in the loss of mobility in the additional mobile segment. 3 Unfortunately, no patient had undergone tumor resection with spinal fixation for thoracic dumbbell tumors at our institution. Thus, we could not compare the postoperative surgical results and the effects on GSSA between patients treated with and without spinal fusion. Therefore, comparative studies should be conducted in future.
In patients with thoracic dumbbell tumors, the association between changes in GSSA on radiography after surgical resection and related clinical symptoms remains unclear.2-5 Ishikawa et al. showed in their study that VAS for pain and the Oswestry disability index (ODI) for patient-reported outcomes were acceptable in 80% of the patients with thoracic dumbbell tumors who underwent tumor resection without spinal fusion. Furthermore, the SF-36 scores were comparable or better than the reference values of the standard Japanese population. Moreover, disc and facet joint degeneration, observed on MRI, did not progress after surgery. 7 In the present study, no patient showed changes in global sagittal balance or complained of low back pain from the period after surgery until the final follow-up. Unfortunately, we could not evaluate whether there was a significant difference in health-related quality of life (HRQOL) before and after tumor removal. Furthermore, we did not use preoperative or postoperative patient-based questionnaires. Therefore, future investigations on the clinical correlates of HRQOL, ODI, and physiologic GSSA preservation would be helpful to validate our clinical findings and identify the actual benefits of surgical resection without fusion in patients with thoracic dumbbell tumors. Moreover, we intend to include this investigation in a future prospective study.
Our study had several significant limitations. First, it used a retrospective approach, which inevitably lowered the level of evidence. Second, the sample size was relatively small, and the statistical power was insufficient to draw conclusions about the precise clinical outcomes of patients with thoracic dumbbell tumors. Moreover, thoracic sagittal alignment, such as GTK, worsened postoperatively in only three of 30 patients, which is too low to allow a statistical comparison between the worsening and non-worsening groups. Third, we did not include a comparison group that underwent fixation; thus, we could not show the superiority of surgical resection without spinal fusion. Finally, the postoperative follow-up period in this study was relatively short to investigate the development of postoperative spinal malalignment. Therefore, future evaluations with a long-term observation period are necessary to validate our proposed surgical procedure. Despite these limitations, this study showed actual results concerning the absence of notable changes in various GSSA parameters in patients with thoracic dumbbell tumors after tumor resection without spinal fusion. The significance of the present study is highlighted by the unprecedented analyses that focused on the presence or absence of variations in each postoperative GSSA profile in patients with thoracic dumbbell tumors who underwent tumor resection without spinal fusion.
Conclusion
The present study evaluated the changes in various GSSA parameters and clinical outcomes after tumor resection without spinal fusion in patients with thoracic dumbbell tumors. This surgical procedure did not affect the individual postoperative GSSA profiles investigated in this study, and it maintained acceptable sagittal alignment with satisfactory functional and clinical outcomes at the final follow-up. However, as the number of patients in this study was relatively small, future studies with larger sample sizes are necessary to provide more precise conclusions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.