
Abstract
Study Design
A retrospective comparative study
Objectives
This study aimed to evaluate the radiographical changes in cervical sagittal alignment (CSA) and clinical outcomes after tumor resection using a posterior unilateral approach without spinal fixation for patients with cervical dumbbell-shaped schwannoma (DS).
Methods
Seventy-three patients with DS who were followed up for at least 2 years were included. The Eden classification was used to designate the types of DS. The CSA and range of motion (ROM) were analyzed using radiographs. The clinical outcomes were assessed using the Japanese Orthopaedic Association (JOA) score and JOA cervical myelopathy questionnaire.
Results
The CSA in the neutral, flexion, and extension position and cervical ROM were not significantly reduced in the follow-up period. The JOA scores showed significant improvement after surgery. The postoperative radiographic parameters and clinical outcomes of Eden type II or III DS, which needed facetectomy for the resection, did not show any statistically significant difference compared with those of Eden type I tumor, which was resected without facetectomy. Fifty-two cases (71.2%) achieved gross total resection, whereas 21 cases (28.8%) remained in partial resection (PR). One case underwent reoperation due to the regrowth of the remnant tumor whose margin was at the entrance of the intervertebral foramen.
Conclusions
Tumor resection using the posterior unilateral approach preserved CSA and resulted in favorable clinical outcomes in patients with DS. When the resection ends in PR, the proximal margin of the remnant tumor should be located distally away from the entrance of the foramen to prevent regrowth.
Keywords
Introduction
Most spinal cord tumors are localized in the intradural space, but they occasionally present as dumbbell-shaped tumors that extend into the intra- or extra-vertebral foramen. 1 Among spinal cord tumors, dumbbell-shaped tumors have an incidence of 18%, of which 44% occur in the cervical spine. 1 Schwannomas are the most frequent primary spinal cord tumor, of which dumbbell-shaped tumors account for 6%–23%.2,3
Several approaches should be considered for resecting dumbbell-shaped tumors, including anterolateral one-way, posterior one-way, and combined approaches.3-8 Among them, the posterior approach is usually selected in the majority of cases with cervical dumbbell-shaped schwannomas (DS). Although the combination of posterior decompression and fusion surgery is occasionally required to open up enough space and resect the tumor safely, it may cause postoperative complications related to spinal instrumentation.4-7,9-18 By contrast, conventional wide laminectomy has a risk of causing spinal deformities, which leads to postoperative cervical instability and subsequent kyphosis due to more extensive damage to the posterior elements of the spinal column.4,6,7,10,19
Based on these findings, the posterior unilateral approach without fixation is usually adopted for patients with cervical DS in our institute.4,10,20 This approach helps to preserve the posterior elements on the contralateral side such as muscles, facet capsules, and interspinous and supraspinous ligaments. However, in cases where the tumor is localized below the C2 vertebral level, a certain amount of the facet joint is necessarily removed at the intraforaminal space, which raises a concern about postoperative cervical spinal instability and functional impairment. Therefore, investigating the clinical association with the postoperative radiographical changes of the cervical spine is essential to determine the benefits of the posterior unilateral approach for patients with cervical DS.
This study aimed to examine the radiographical changes in cervical alignment and surgical outcomes after removing cervical DS using the posterior unilateral approach, and comprehensively validate the feasibility and efficacy of this surgical approach.
Materials and Methods
Study Design, Patient Demographics, and Characteristics
A total of 73 patients with cervical DS that required tumor resection using the posterior unilateral approach at our institute between 2009 and 2019 were included in this study. The inclusion criteria were as follows: 1) diagnosed with cervical DS (Eden type I, intra- and extradural; II, intra- and extradural and paravertebral; or III, extradural and paravertebral 21 ) at least at 18 years of age; 2) absence of trauma, congenital vertebral deformity, neuromuscular disorders, or other pathological conditions (cervical deformity, spondylosis myelopathy, etc.); 3) absence of previous spinal surgery; and 4) a minimum of 2-year follow-up after surgery. The exclusion criteria were as follows: thoracic spinal cord tumors in which the central region of the tumor was below the T1; intramedullary spinal cord tumor; non dumbbell-shaped tumor which localized only at the extradural or extraforaminal space; Eden type IV DS (foraminal and paravertebral). Tumor resection was performed in patients with sensory (numbness or pain in the upper or lower extremities) or motor (muscle weakness or paralysis) disturbance that was refractory to any conservative therapy and that remained unchanged or progressed their symptoms. All information regarding demographics (age at surgery, sex, postoperative follow-up period, Eden classification, and tumor location), imaging, and surgical data (number of totally and partially resected laminae, surgical time, estimated blood loss [EBL], percentage of tumor resection, length of hospital stay, and percentage of postoperative complications) were retrospectively obtained by reviewing the patients’ records and radiological images.
This study was approved by the Committee on Ethics and Institutional Review Board (approval number: #20110142), and all subjects provided informed consent for inclusion before tumor resection.
Surgical Method
Five of our board-certified spinal surgeons performed all of the surgeries. A midline incision was made along the spinous processes, and the cervical muscles were detached from the spinous processes only at the side where the tumor was located. Thus, the muscles on the other side were preserved without any invasion. Hemilaminectomy was performed using a drill at the tumor level for cervical DS resection. For Eden type I tumors that only included intra- and extradural portions, the dura mater and arachnoid membrane were longitudinally opened to resect the tumor. To prevent the damage of normal spinal cord, intradural part of the tumor was reduced within an intra-capsular fashion using a cavitron ultrasound surgical aspirator (CUSA), and the entire capsule was eventually removed.4,5 After the resection, the dura mater together with the arachnoid membrane was sutured with 5-0 monofilament absorbable suture string. For Eden type II and III tumors that included paravertebral elements, approximately one-half to two-thirds of the inside facet joint was removed in cases where the tumor was localized below the C2 vertebral level. For Eden type II tumors, after resecting the intradural part, the extradural and paravertebral parts of the tumor were resected using the CUSA (Figure 1A–F). For Eden type III tumor that did not contain the intradural element, the extradural and paravertebral portions of the tumor were resected after the same facetectomy approach. Representative images of dumbbell-shaped tumor resection. (A–C) Two-thirds of the inside facet joint was removed (dotted line). The tumor was resected with nerve root preservation. (D–F) The extradural/paravertebral part of the tumor was resected.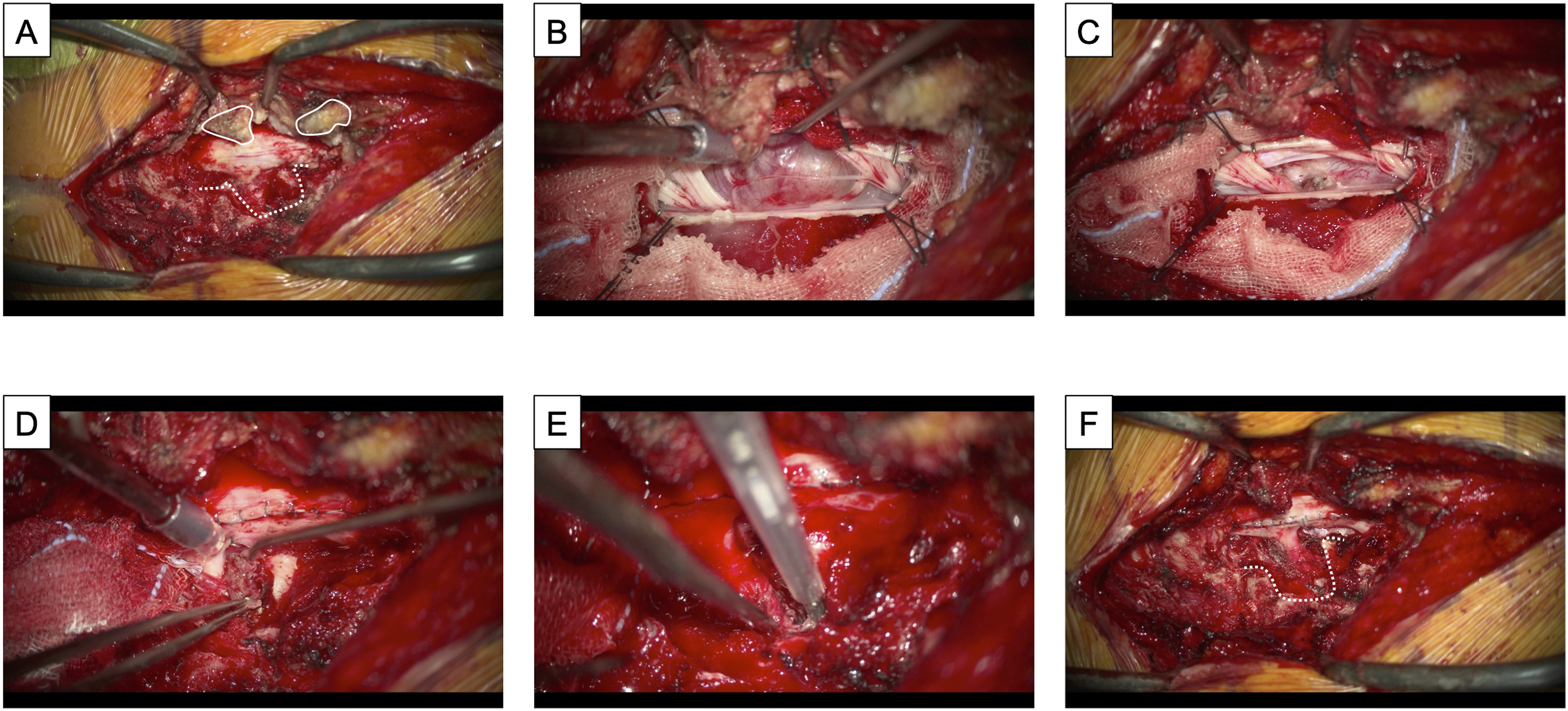
The detached muscles were sutured, and the wound was closed. Intraoperative spinal cord monitoring was performed in all cases. All patients started ambulation at least 4 days postoperatively and were cautiously monitored for symptoms related to cerebrospinal fluid leakage or neurological deficit. Magnetic resonance imaging (MRI) was performed after surgery to confirm the extent of the lesion resection.
Radiographical and MRI Data
Cervical spine radiological assessment was performed on all study participants at “preoperation” and “final follow-up.” The cervical sagittal profiles, including the C2-7 angle in the neutral, flexion, and extension position and cervical range of motion (ROM: [C2-7 angle in the extension position] − [C2-7 angle in the flexion position]) were examined. In cases where the tumor was localized at the C2 vertebral level, the C0-2 and C0-7 angles, formed by the McGregor’s line (connecting the posterior part of the hard palate and the most caudal part of the occiput) and the inferior endplate of C2 or C7 vertebra, were also assessed. An experienced spine surgeon reviewed the medical records and radiographs of all patients. The intraobserver reliability examined by the intraclass correlation coefficient (ICC; 1, 1) and ICC (1, 3) formula was .85 and .94, respectively. To assess the interobserver error, 30 randomly chosen radiographs were measured independently by 3 spine surgeons not directly involved in the surgeries. The interobserver reliability tested using the ICC (2, 1) and ICC (2, 3) formula was .84 and .92, respectively.
MRI was performed postoperatively to confirm the extent of tumor resection, which was classified into 2 types according to the operative records: gross total resection (GTR) and partial resection (PR). The standard definition of GTR was used in the present study (ie, removal of 100% of the tumor based on the absence of remnant tumor documented microscopically and no evidence of neoplasm in the site of tumor origin). The procedure was considered as PR when a small tumor fragment or extraforaminal/paravertebral portion was left in place based on the documented removal of 50%–99% of the tumor on intraoperative ultrasonography or postoperative MRI findings.
22
The remnant tumor location was categorized into 3 areas according to the proximal tumor margin (Figure 2): Zone 1, remaining in the spinal canal; Zone 2, not protruding into the spinal canal but touching the posterolateral corner of the intervertebral disc or the vertebral body at the entrance of the intervertebral foramen; and Zone 3, in the intervertebral foramen distally from the posterolateral corner of the intervertebral disc or the vertebral body at its entrance.
20
Locations of the remnant tumor margin
20
Zone 1, remaining in the spinal canal; Zone 2, touching the posterolateral corner at the entrance of the intervertebral foramen; Zone 3, in the intervertebral foramen distally from the posterolateral corner.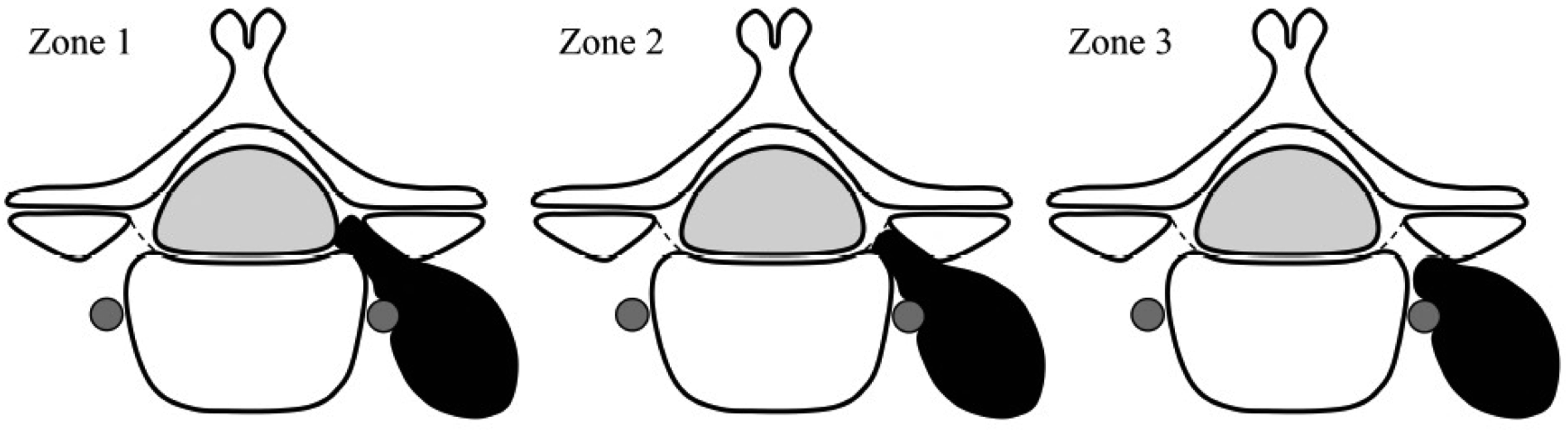
Clinical Outcomes and Functional Evaluation
The clinical outcomes and functional effectiveness were assessed at “preoperation” and “final follow-up” using the Japanese Orthopaedic Association (JOA) scoring system (17 possible points) and the JOA cervical myelopathy evaluation questionnaire (JOACMEQ; the score for each of the 5 domains ranges from 0 to 100, with higher scores indicating better condition). 23 Additionally, the degree of the neck or shoulder pain or stiffness, chest tightness, arm or hand pain or numbness, or chest to toe pain or numbness was assessed using the visual analog scale (VAS) included in the JOACMEQ (the score ranges from 0 to 10, with lower scores indicating a comfortable condition without any pain or numbness). The JOA score recovery rate was calculated as follows: (final follow-up JOA score − preoperative JOA score)/(17 − preoperative JOA score) × 100 (%).
Statistical Analysis
All data are expressed as the mean ± standard error of the mean, and categorical variables are presented as percentages. The demographic and clinical characteristics, surgical data, radiographical findings, and clinical outcomes were compared between preoperation and final follow-up using the Wilcoxon signed-rank test, or between Eden type I and Eden type II or III groups using the Mann–Whitney U test. A correlation analysis was performed using a Spearman test. Statistical significance was considered at P < .05. All statistical analyses were performed using SPSS version 26.0 (Chicago, IL).
Results
Patients’ Demographics, Clinical Characteristics, and Surgical Data
Patient Demographics, Clinical Characteristics, and Surgical Data of all Patients.
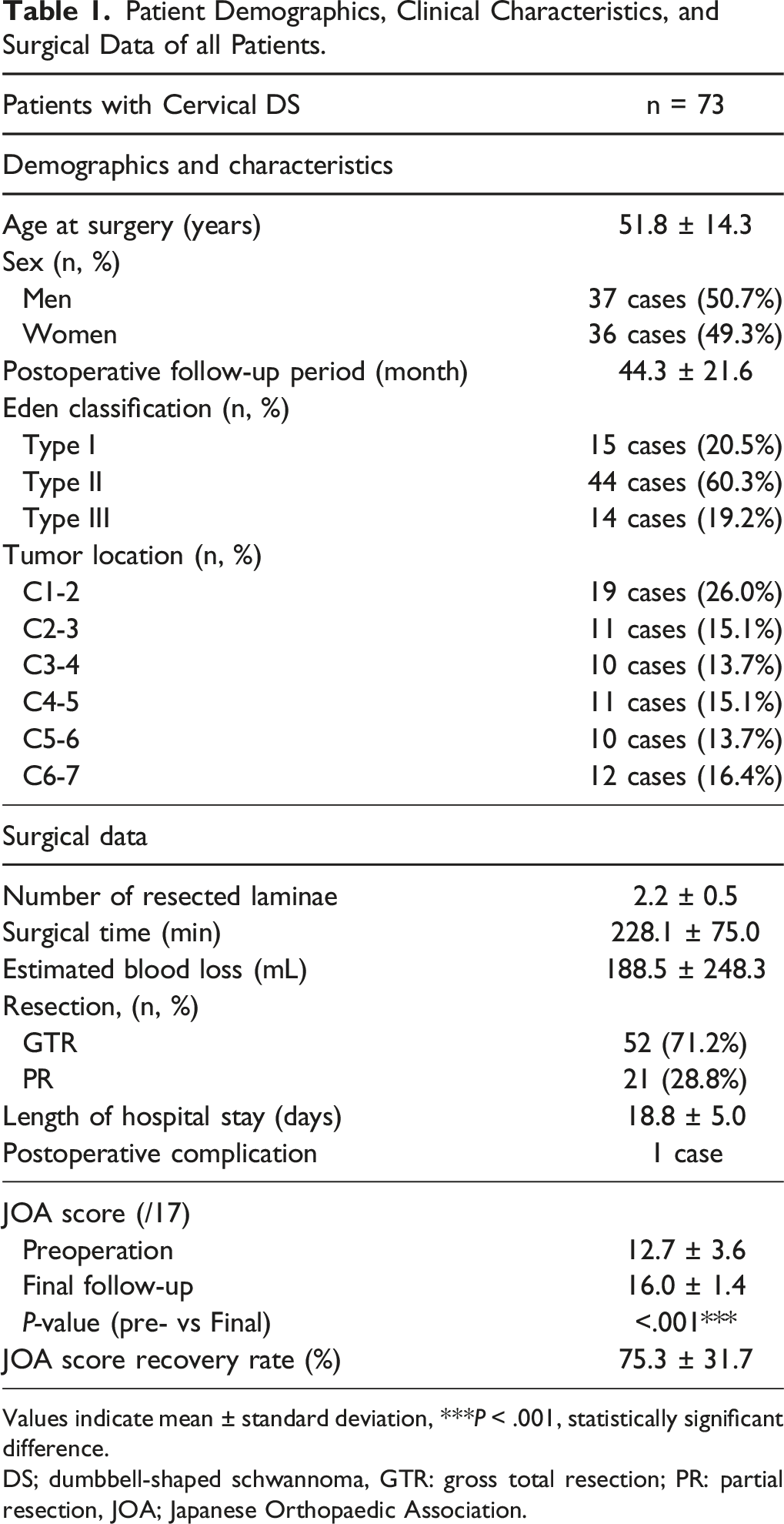
Values indicate mean ± standard deviation, *** P < .001, statistically significant difference.
DS; dumbbell-shaped schwannoma, GTR: gross total resection; PR: partial resection, JOA; Japanese Orthopaedic Association.
Postoperative Changes in Cervical Alignment
Comparison of Preoperative and Final Follow-Up Each Cervical Sagittal Parameter Among all Cases.
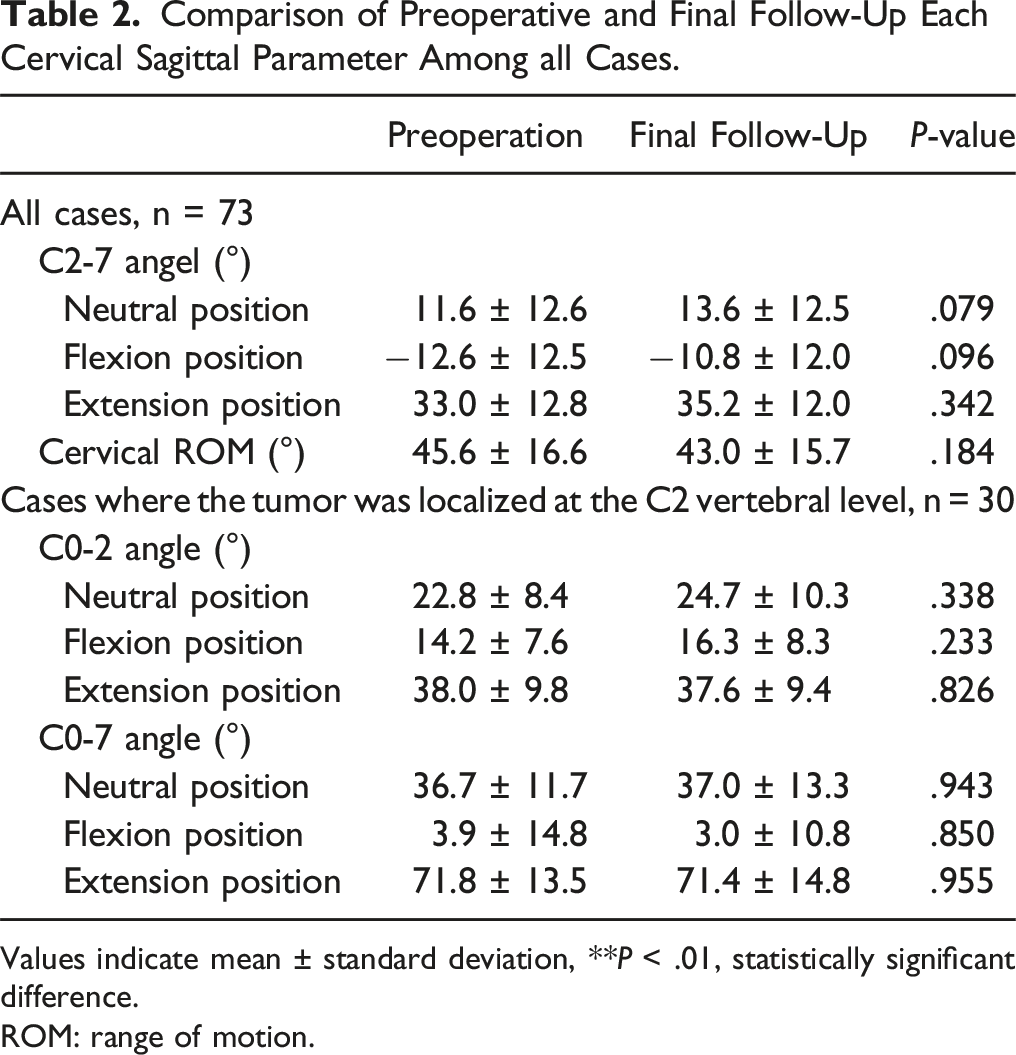
Values indicate mean ± standard deviation, ** P < .01, statistically significant difference.
ROM: range of motion.
Correlation Analysis Between the Postoperative Changes for C2-7 Angle or Cervical ROM With Age at the Surgery, the Number of Resected Laminae, Preoperation JOA Score, or Final Follow-Up JOA Score.
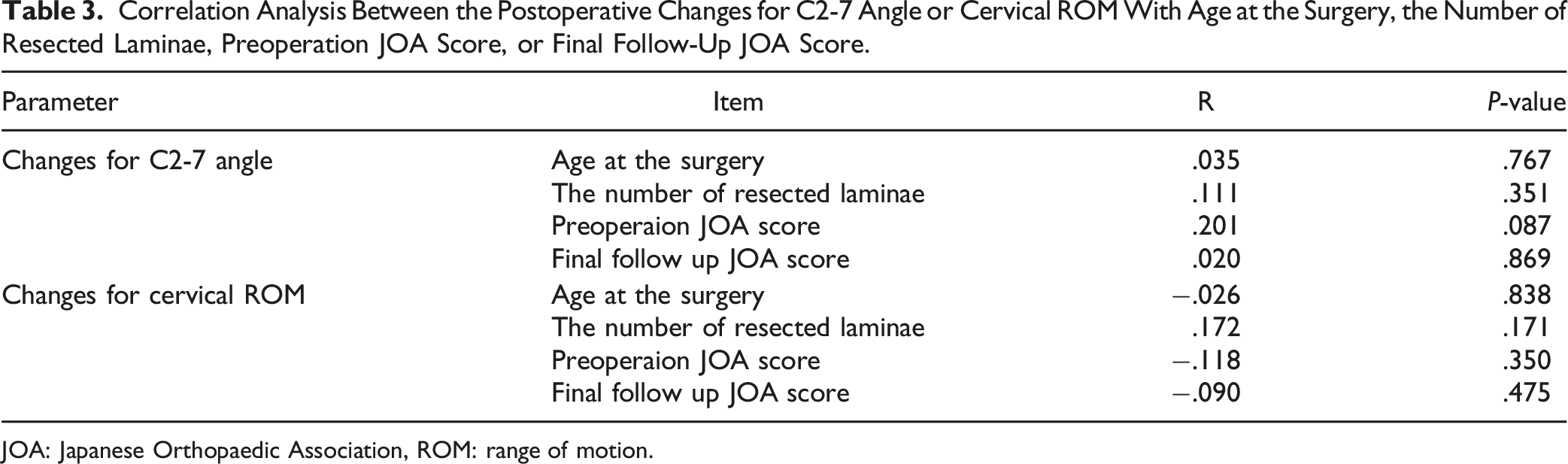
JOA: Japanese Orthopaedic Association, ROM: range of motion.
Influence of Posterior Unilateral Approach With or Without Facetectomy on Postoperative Cervical Alignment and Clinical Outcomes
Comparison of Each Cervical Sagittal Parameter Between Eden Type I and Eden Type II or III Group.
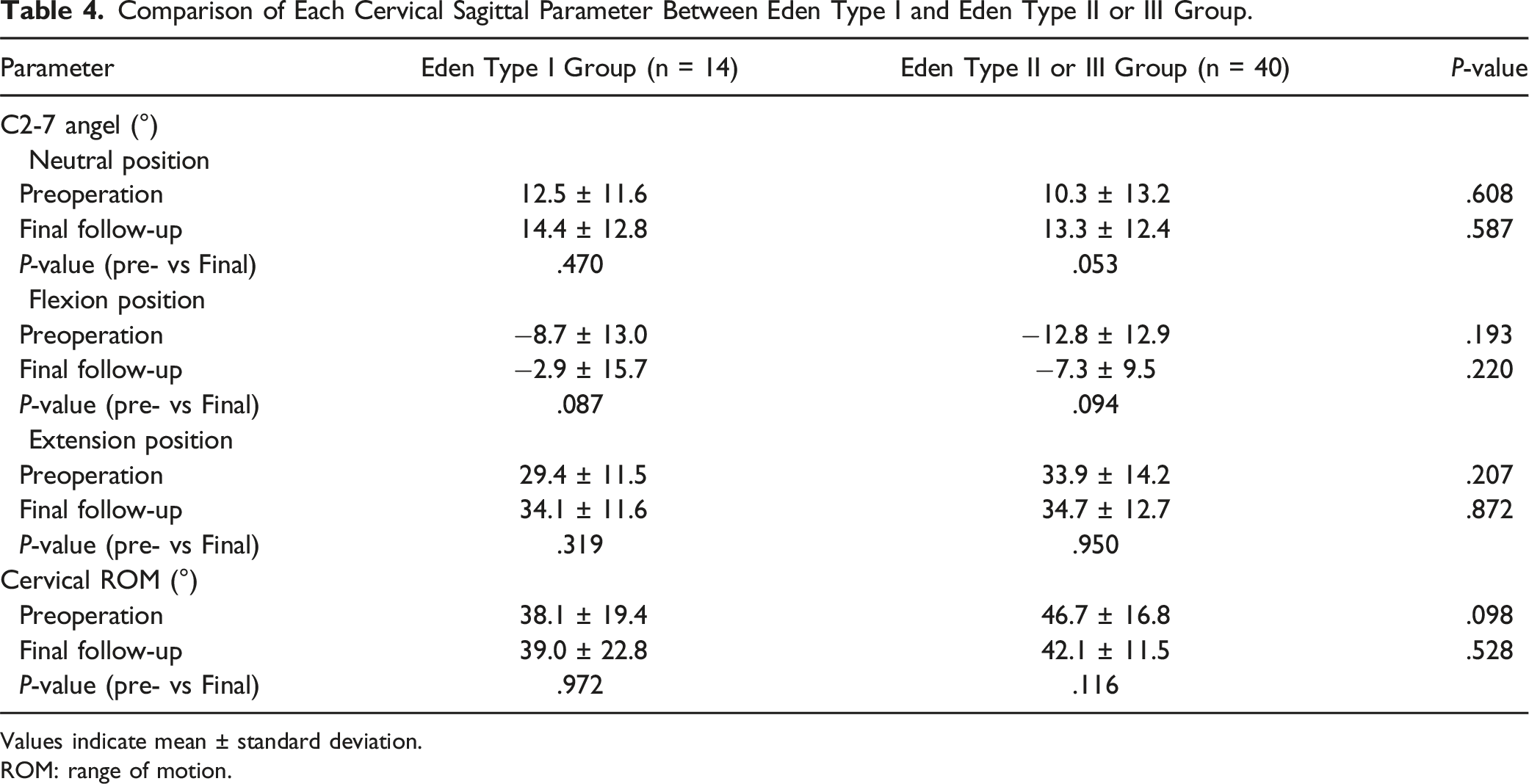
Values indicate mean ± standard deviation.
ROM: range of motion.
Comparison of Each Clinical Outcomes Between Eden Type I and Eden Type II or III Group.
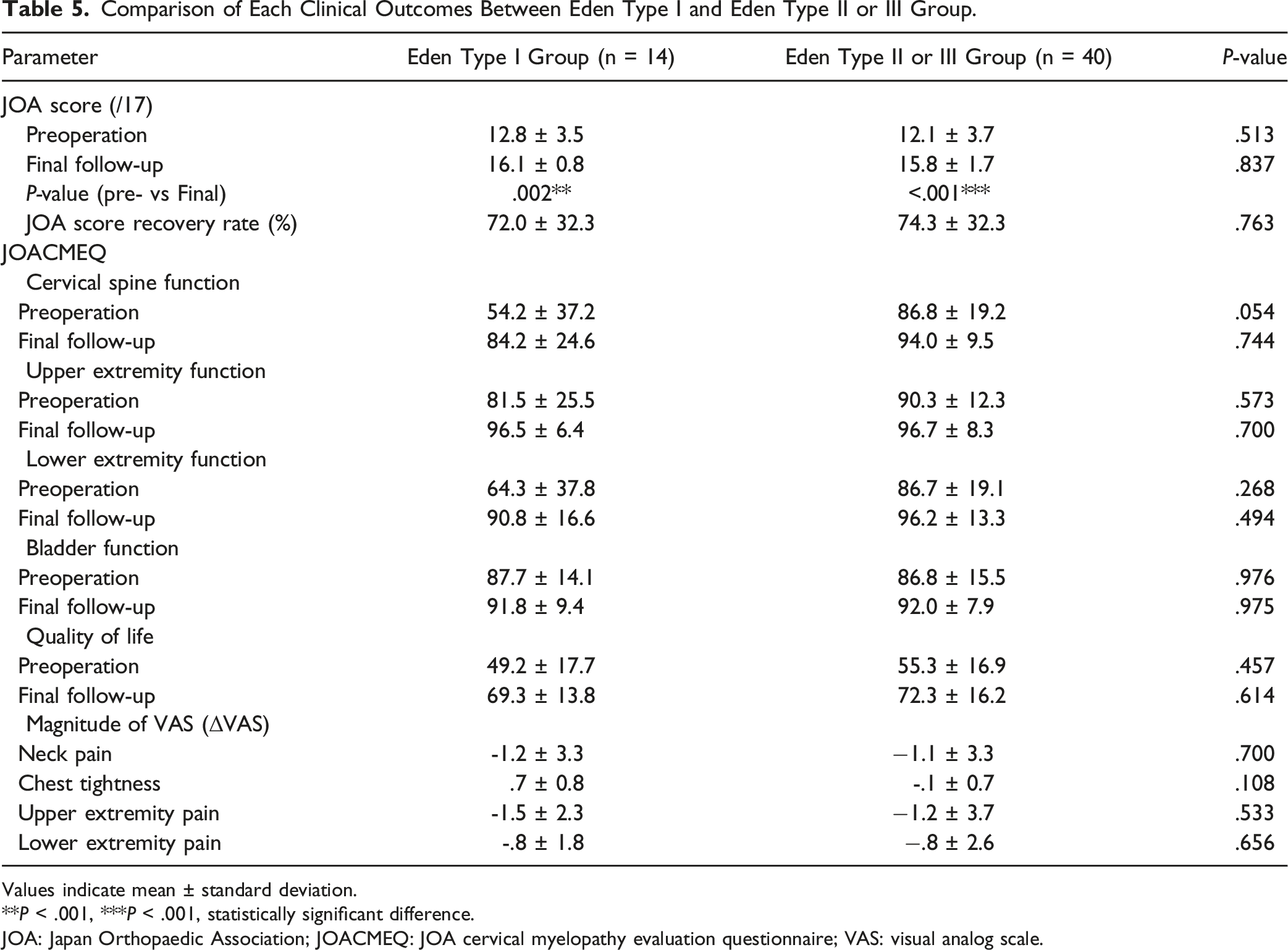
Values indicate mean ± standard deviation.
**P < .001, ***P < .001, statistically significant difference.
JOA: Japan Orthopaedic Association; JOACMEQ: JOA cervical myelopathy evaluation questionnaire; VAS: visual analog scale.
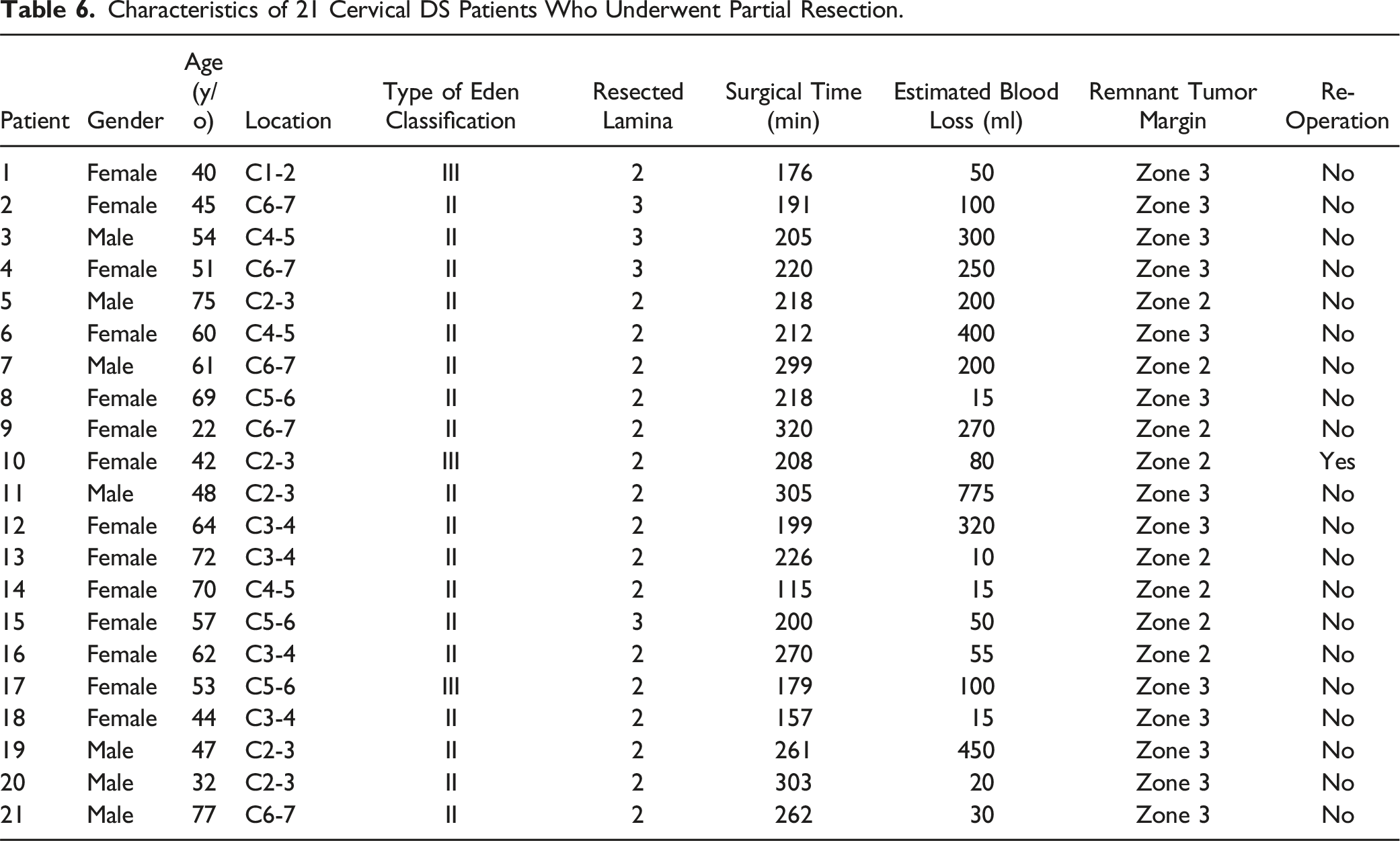
Clinical Profiles of Patients with Cervical DS Who Underwent PR
Characteristics of 21 Cervical DS Patients Who Underwent Partial Resection.
Representative Case
A 48-year-old male patient complained of hand clumsiness and gait disturbance. His MRI showed a dumbbell-shaped tumor (Eden type II) on the left side at the C3/4 spinal level (Figure 3A). The posterior unilateral approach with facetectomy was selected for tumorectomy, which resulted in GTR. Two years postoperatively, his MRI did not show any tumor recurrence (Figure 3B), and plain radiographs revealed no spinal instability at the C3/4 level (Figure 3C–D). The patient was in good condition without any symptoms. Representative MR and radiographic images of a patient with cervical DS. (A–B) The arrow indicated the area where the resected tumor existed at the C3/4 level. (C–D) No occurrence of spinal instability was observed at the lesion level.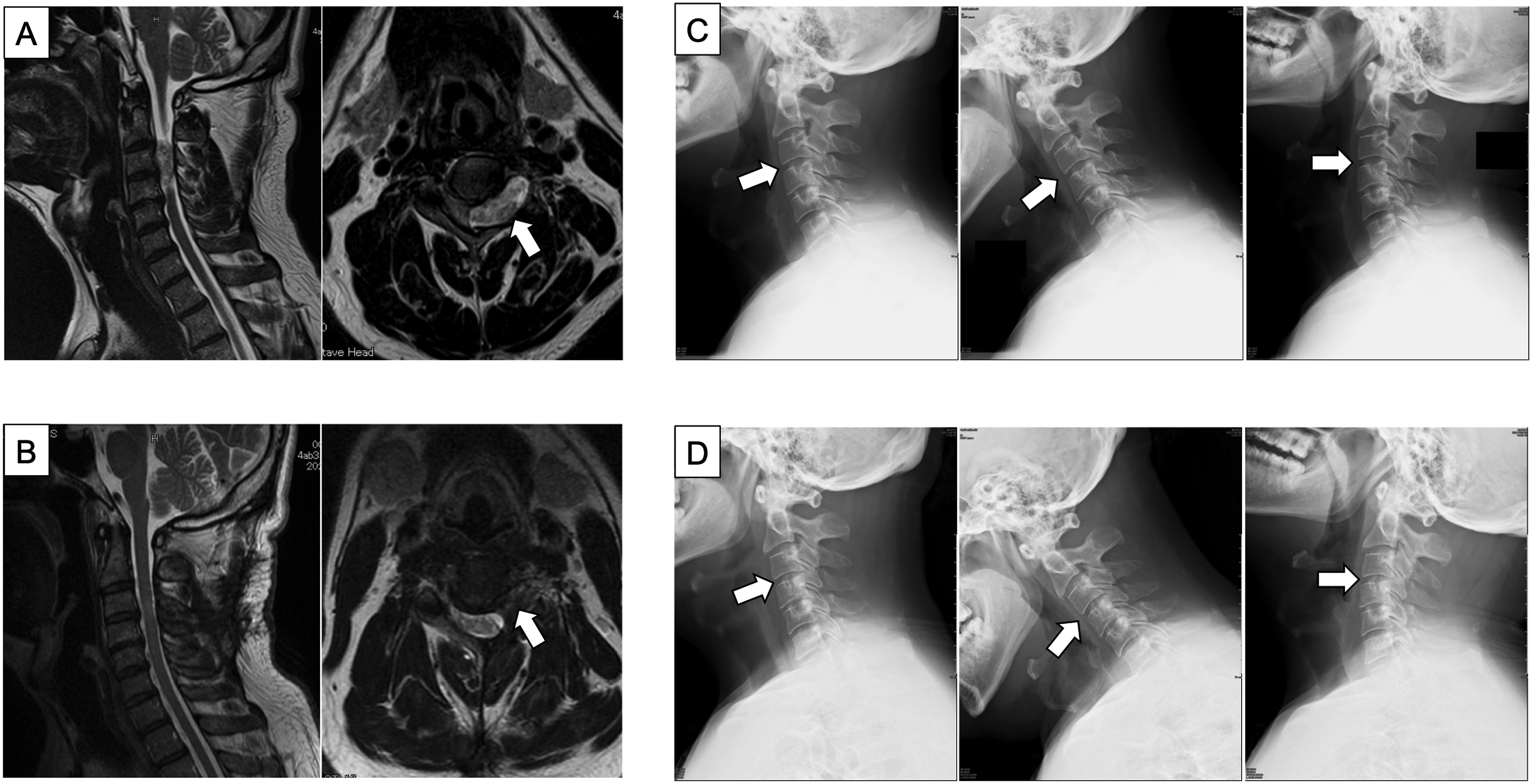
Discussion
Herein, we clarified the efficacy of the posterior unilateral approach for cervical DS. This approach achieved GTR in 71.2% of the cases, preserved cervical function with the maintenance of spinal alignment and ROM, and contributed to the neurologic recovery. Even though the resection was partially limited, these benefits were guaranteed by removing the tumor distally from the entrance of the intervertebral foramen (Zone 3). However, when the remnant tumor margin was located at the entrance of the foramen (Zone 2), there was a risk for tumor regrowth, requiring additional surgery. Therefore, the posterior unilateral approach is a good surgical indication if it completes GTR or possibly reaches resection close to the vertebral artery at Zone 3.
During the surgical procedure, the facet joint must be occasionally sacrificed to remove the dumbbell-shaped tumor, which could cause postoperative cervical malalignment.1,4-6,8,9,14,24 Several reports showed cervical spine instability after tumor resection combined with facetectomy.4,12,20,25 Katsumi et al indicated that postoperative deformity or instability after total laminectomies occurred in 20.5% of patients with cervical spinal cord tumors. 26 Conversely, in the present study, the C2-7 angle and cervical ROM did not change, and spinal instability did not occur after tumor resection because the posterior unilateral approach preserved the muscle layer and facet joints on the contralateral side of the existing tumor. Thus, this surgical approach could be useful from the perspective of postoperative management.
In recent years, spinal fusion surgery using instrumentation was often required to prevent post-laminectomy deformity and stabilize the spine to prevent cervical deformity and instability after tumor excision.14,16,17,24,27 Nevertheless, this procedure has several disadvantages, including blurred postoperative MRI due to metallic artifacts and biofilm formation around the spinal instrumentation.15,18 In addition, more than 3 vertebrae must be fused using bilateral instrumented fixation in some cases, resulting in the loss of mobility of the additional motion segment. 24 From these points of view, the posterior unilateral approach without spinal fixation is selected for cervical DS resection in our institution. Unfortunately, there were no cases that underwent spinal fixation in combination with cervical DS resection at our institution. Thus, we were unable to compare the postoperative surgical results and the effects on the cervical spinal function of patients treated with the posterior unilateral approach. Future comparative studies should be performed.
The axis has the largest spinous process among the cervical vertebrae, and it holds more attachment sites for shallow and deep extensor muscles. 28 Katsumi et al reported that a reduction in the area of insertion of the semispinalis cervicis muscle was associated with the development of spinal instability in spinal cord tumor resection via C2 laminectomy. 26 Nori et al revealed that detachment of the deep extensor muscles from the C2 spinous process was directly related to the risk of developing spinal kyphosis after resection of cervical intramedullary spinal cord tumor. 29 In the present study, both local and whole cervical alignments did not significantly change before and after surgery in cases of dumbbell tumors localized at the C2 vertebral level. Moreover, new occurrences of cervical malalignment, instability, or deformity were not observed at the final follow-up. This was because the contralateral posterior extensor muscle from the C2 spinous process was preserved using the unilateral approach. Therefore, even in cases of dumbbell tumors localized at the C2 vertebral level, this approach has the advantage of preventing postoperative cervical malalignment.
The regrowth rate of the remnant tumor after PR ranged from 16.7% to 60% in patients with intraspinal dumbbell-shaped tumors.4,30 Ryu et al reported that 7 out of 31 patients with cervical DS (22.6%) showed remnant tumor growth after PR during the mean follow-up period of 16 months, and two underwent reoperations due to the newly developed neurological symptoms caused by the growth. 19 We previously demonstrated that 47.6% of patients who underwent PR for cervical DS showed remnant tumor growth during the mean follow-up period of 61 months, and one patient underwent reoperation due to spinal cord compression with neurologic deterioration. In addition, there was significant difference in the regrowth probability between the proximal tumor margins at Zone 3 and those at Zone 1 or 2. Regarding a higher risk factors of remnant tumor growth, the anatomical location of the tumor margin, such as Zone 1 or 2, are significantly correlated to its regrowth. 20 Similar results were observed in the current study, which revealed no tumor regrowth in patients who underwent PR to Zone 3. Moreover, 1 of the 8 patients whose resected margin was limited to Zone 2 needed additional surgical resection due to regrowth. Thus, based on these results, aiming for GTR or at least resection to Zone 3 is necessary for stabilizing outcomes using the posterior unilateral approach.
To date, the JOA score and neck disability index (NDI) have been used to evaluate postoperative outcomes in the cervical spine.27,28 However, the JOA score is evaluated from the medical providers’ perspective. Therefore, it tends to preoperatively give a lower score and, conversely a good postoperative score. The NDI is a patient-reported scoring system, but it assesses neck pain alone. By contrast, the JOACMEQ was developed to measure the patient-reported clinical outcomes for cervical disorders and comprehensively evaluate the bodily function, pain, and quality of life. 23 The current study used the JOACMEQ to clarify multifaceted evidence regarding the impact of the posterior unilateral approach on surgical outcomes in patients with cervical DS. Thus, this assessment allowed us to demonstrate the efficacy and validity of the posterior unilateral approach, especially in postoperative cervical function and pain.
Our study has several important limitations that should be noted. First, the present study had a retrospective design, which inevitably lowered the evidence level. Second, we did not include cases of bilateral laminectomy or combined fixation and thus could not demonstrate the superiority of our technique. Third, the postoperative follow-up period in this study was short to evaluate the development of postoperative cervical spinal deformity. Therefore, future investigation will be necessary with long-term observational duration to validate the proposed surgical approach. However, this study comprehensively evaluated the posterior unilateral approach for cervical DS resection using patient-reported outcomes and radiographic parameters. The current results emphasized the usefulness of this procedure without compromising postoperative cervical spinal function.
Conclusion
The present study evaluated the cervical spinal function and clinical outcomes after tumor resection using the posterior unilateral approach without spinal fixation in patients with cervical DS. This surgical technique did not influence the postoperative cervical spinal angle in each position or cervical ROM and maintained acceptable sagittal alignment with satisfactory functional and clinical outcomes at the final follow-up. GTR is preferable. However, when the extent of tumor resection ends to PR, the proximal margin of the remnant tumor should be located in Zone 3 to prevent its regrowth.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.