
Abstract
Study Design:
Health utility analysis.
Objectives:
To determine the health state utility (HSU) of 1- and 2-level anterior cervical discectomy and fusion (ACDF) and cervical disc replacement (CDR).
Methods:
Data from the Medtronic Prestige Cervical Disc investigational device exemption studies was used. Four groups were defined: 1-level ACDF, 1-level CDR, 2-level ACDF, and 2-level CDR. The 36-item Short Form Health Survey (SF-36) was collected at baseline, 12 months, 24 months, 36 months, and 60 months postoperatively and converted into utility scores for each time point. A repeated-measures 1-way analysis of variance (ANOVA) was used to detect differences among groups. Tukey’s method for multiple comparisons was used to determine which means within the groups were statistically different (P < .05).
Results:
We found a statistically significant difference in HSU among groups as determined by repeated-measures 1-way ANOVA (P = .0008). Post hoc analysis indicated that 1-level ACDF had a statistically lower utility score compared with 1- and 2-level CDR (P = .04 and P = .02, respectively). Similarly, 2-level ACDF had lower utility values compared with 2-level CDR (P = .010). One-level ACDF utility values were not different from 2-level ACDF values (P = .55). Similarly, 1-level CDR and 2-level CDR did not have different utility values (P = .67).
Conclusions:
Overall, CDR had higher health state utility scores for 1- and 2-level procedures at every time point. This study indicates that CDR results in a higher postoperative health utility state than ACDF, and may therefore be an effective alternative to ACDF for treating degenerative conditions of the cervical spine.
Keywords
Introduction
Cervical disc replacement (CDR) is an increasingly accepted and utilized strategy for the treatment of symptomatic cervical degenerative disc disease (DDD). Although anterior cervical discectomy and fusion (ACDF) is generally considered the gold standard for the treatment of DDD, CDR may provide superior outcomes in terms of arm and neck pain, neurological outcomes, range of motion, and decreased secondary surgical procedures. 1 –10 Furthermore, increased range of motion may theoretically reduce the rate of adjacent level disease. 11,12
In a health care atmosphere where increasing awareness of the costs of care may guide treatment practices it is important to compare interventions in their efficient utilization of resources. The 36-Item Short Form Health Survey (SF-36) is a nonspecific Health-Related Quality of Life (HRQoL) assessment that has been validated to measure morbidity and surgical outcomes in common spinal disorders. 13,14 This assessment can be translated into a measure of cost-effectiveness called the health state utility (HSU) value. Applying the HSU in cost-effectiveness analysis (CEA) provides a measure of the effectiveness of a procedure in terms of the change it produces in a patient’s life. Utility values can range from 0 to 1, with 0 representing death and 1 representing perfect health. These health state utility values are aggregated to generate quality-adjusted life years (QALYs). Data from the SF-36 can be converted into HSU scores, allowing direct comparison of the health status of patients receiving different interventions.
While CEAs have previously been used to compare CDR with ACDF in the treatment of DDD, few have incorporated HSU into the model analysis. 15 –18 The ability to accurately define the utility of an intervention is a critical component to determining the overall value of that strategy. The purpose of this study was to therefore determine the HSU of 1- and 2-level ACDF and CDR at various postoperative time points. These values will form the basis for future CEA models that attempt to define treatment strategies involving ACDF and CDR.
Materials and Methods
We performed a secondary analysis of the prospectively collected Short Form 36 (SF-36) data from the 1- and 2-level Prestige LP CDR investigation device exemption (IDE) studies. We did not conduct a randomized control trial. We secondarily analyzed deidentified data from a Food and Drug Administration (FDA) IDE prospective randomized control trial, and therefore did not require institution review board approval. In the 1-level study, 240 patients underwent ACDF and 280 underwent CDR. The patients in the CDR group were adults with symptomatic cervical DDD that required surgery at a single-level between C3 and C7. All patients had radiculopathy and/or myelopathy that did not respond to nonoperative management. All patients had no previous surgical intervention at the involved or adjacent levels. Additionally, all patients had preoperative Neck Disability Index (NDI) scores ≥30, and preoperative neck and arm pain questionnaires ≥20. All patients in the control (ACDF) group were from a previously conducted FDA IDE, and had identical inclusion and exclusion criteria. Similarly, in the 2-level study, 229 patients underwent ACDF and 223 underwent CDR. Overall, 4 potential operative states were considered: 1-level ACDF, 1-level CDR, 2-level ACDF, and 2-level CDR. Inclusion and exclusion criteria for the 2-level patients in the CDR group were the same as those for the 1-level study, only that they experienced symptoms at 2 contiguous levels.
As part of the study, the SF-36 data was collected at baseline, 12 months, 24 months, 36 months, and 60 months postoperatively. SF-36 data was converted into health state utilities at each time point using the Short Form–6 Dimension (SF-6D) algorithm, which is a preference-based index obtained from a sample of the general population using the recognized valuation technique of standard gamble. 19 The standard gamble technique presents an individual with a choice between a particular health state and a gamble that can either improve or worsen that health state. The individual is then asked what probability of improvement would make them indifferent to choosing between the current health state and the gamble. The SF-6D is composed of 6 multilevel dimensions describing a total of 18 000 unique health states. Based on preference weights obtained from a sample of the population, the SF-6D algorithm assigns a utility value to a particular health state or to a treatment state. Using a noncommercially licensed application of the SF-6D algorithm, the SF-36 data from the IDE studies was converted to utility values at each of the time points. The SF-6D has been validated in comparison with other health state utility tools such as the EuroQol 5D, and has been used in a number of cost-effectiveness studies. 20 –22
Statistical Analysis
All statistical analyses were performed with Prism Graphpad V7 (La Jolla, CA, USA). The means and standard deviations of HSU scores were calculated for each potential operative state. The mean utility scores for each state were compared to detect an overall difference among groups with the use of a repeated-measures 1-way analysis of variance (ANOVA). Tukey’s method for multiple comparisons was performed to assess for individual differences between the means of the 4 groups. Statistical significance was taken at P < .05.
Results
Table 1 summarizes the calculated health state utility values for 1- and 2-level ACDF and CDR for each of the time points. There was a statistically significant difference between groups as determined by 1-way ANOVA with repeated measures, F(2, 9) = 15.63, P = .0008 (Figure 1). A Tukey’s post hoc analysis indicated that 1-level ACDF had a statistically lower utility score at all time points when compared with 1- and 2-level CDR (P = .04 and P = .02, respectively) (Table 2). Similarly, two-level ACDF was shown to have a lower utility value at all time points when compared with 2-level CDR (P = .010). One-level ACDF and 2-level ACDF were not shown to have different utility values from one another at any time point (P = .55). Similarly, 1-level CDR and 2-level CDR did not differ in their utility values at any time point (P = .67).
Heath Utility Scores for 1- and 2-Level ACDF and CDR at Each Time Point.
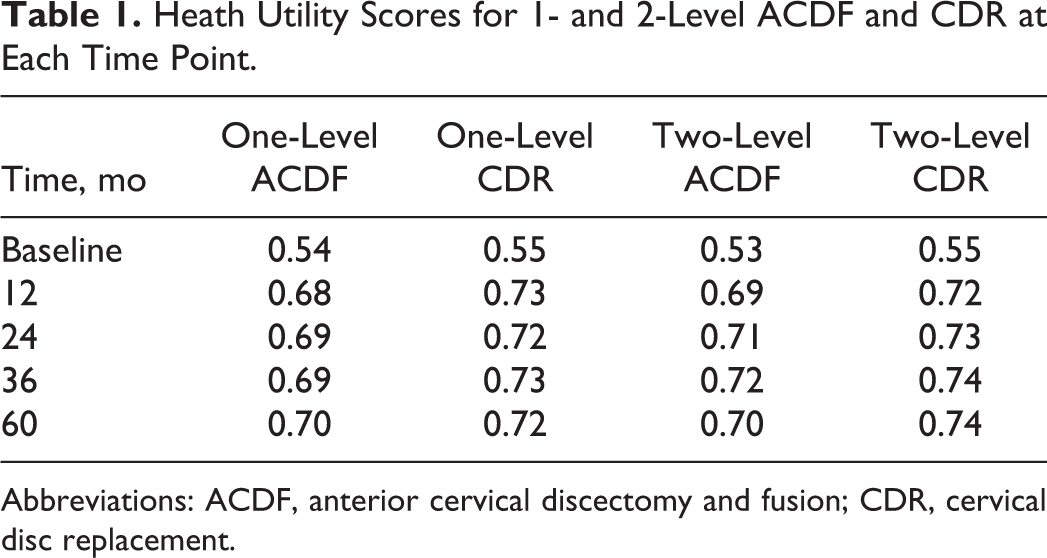
Abbreviations: ACDF, anterior cervical discectomy and fusion; CDR, cervical disc replacement.
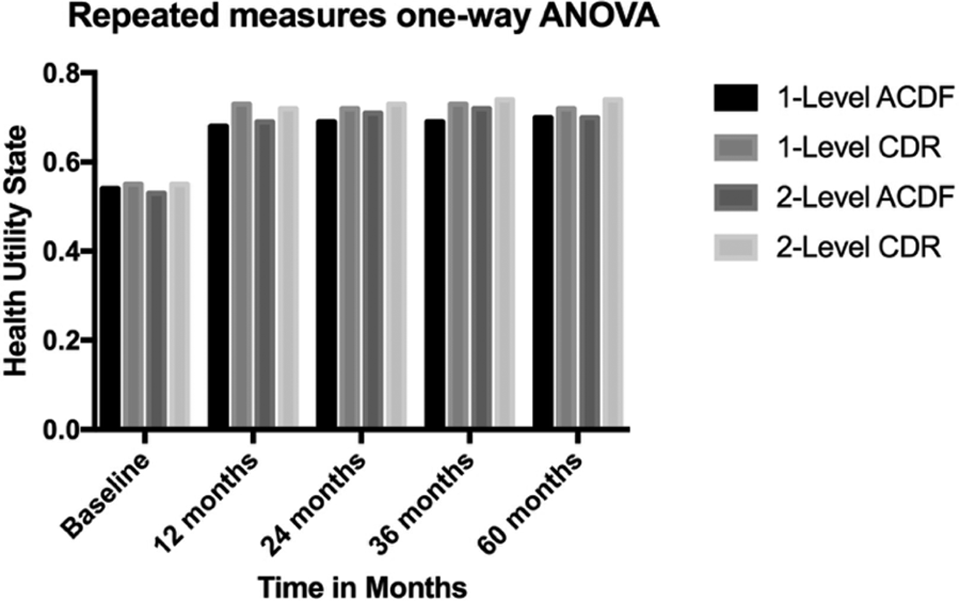
Results of the one-way repeated-measures analysis of variance. ACDF, anterior cervical discectomy and fusion; CDR, cervical disc replacement.
Tukey’s Post Hoc Analysis Comparing Means for Each Simulation.
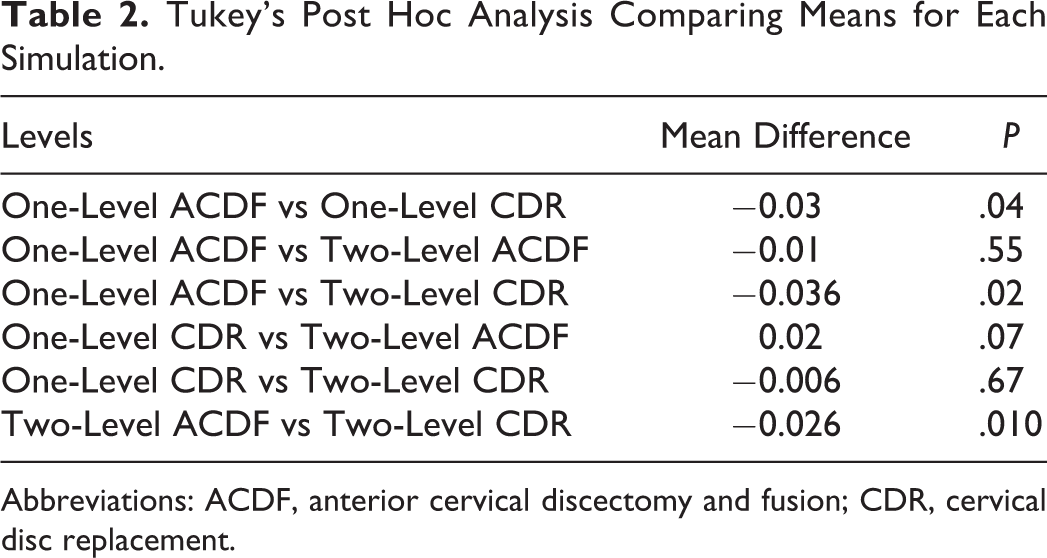
Abbreviations: ACDF, anterior cervical discectomy and fusion; CDR, cervical disc replacement.
Discussion
ACDF and CDR are 2 effective and successful strategies for the treatment of symptomatic degenerative disc disease. There have been a number of FDA IDE randomized control studies that have reported short- and medium-term results for both 1- and 2-level ACDF and CDR. 1 –10 These IDE disc arthroplasty studies have provided a wealth of patient-derived outcomes for both CDR and ACDF, including SF-36, EuroQol 5D, and Neck Disability Index (NDI). In order to perform a CEA, these patient-derived outcomes require conversion to a HSU value. The objective of our study was to be the first to directly define the HSU of 1- and 2-level ACDF and CDR at 5 years.
The utility values in our model were derived from the SF-36 data from a FDA IDE trial comparing outcomes of CDR and ACDF. SF-36 was the chosen metric as it is a validated means of translating these scores into a quantitative health utility value for use in CE modeling. 14,19 Using this data, the baseline health state for 1- and 2-level DDD was determined. The baseline health state scores were similar to those previously published, which reported a single level DDD HSU of 0.54. 23 For the single level cohort, there was a statistical difference between CDR and ACDF at every time point. Similarly, in the 2-level cohort, the calculated HSUs were significantly different at all time points in favor of CDR. The 1- and 2-level ACDF and CDR groups all showed a significant improvement from the baseline scores at all time points. Furthermore, the improvement in HSU appeared to be maintained out to 5 years in all the groups. This would suggest that ACDF and CDR both show a similar durability in the improvement of HSU at an intermediate time point, with a greater HSU in 1- and 2-level CDR compared with 1- and 2-level ACDF.
A number of cost-effectiveness analyses have been carried out for different CDR devices. Radcliff et al 16 obtained QALYs using 7-year follow-up data from the ProDisc-C IDE study and conducted a Monte Carlo simulation to compare cost-effectiveness of CDR compared with ACDF for single-level procedures. The authors found that CDR on average per-patient had a cost savings of $12 789 and QALY gains of 0.16 compared to ACDF. They also determined CDR to be more cost-effective in 90.8% of the 10 000 simulations. Several other studies have also found CDR to be more cost-effective than ACDF for single-level procedures. 17,18 For 2-level procedures, Ament et al 15 found CDR to be associated with a greater cost of $2139 per patient, but also observed QALY gains of 0.087 per patient compared with ACDF. This yielded an incremental cost-effectiveness ratio of $24 594, far lower than the commonly used $50 000 per QALY. The authors therefore suggest that CDR is an extremely cost-effective alternative to ACDF, and postulated this may be due to the faster recovery and earlier improvement in health states after CDR.
Our results suggest the benefits of CDR over ACDF with regard to HSU, and several studies have also demonstrated the clinical benefits of CDR over ACDF. Burkus et al 24 independently analyzed 5-year follow-up data from the Prestige CDR IDE study. Of the 271 patients who completed 5-year follow-up, 144 were treated with the investigational device (CDR) and 127 were treated with ACDF for single level DDD. 24 The authors found that at both 36- and 60-month time points postoperatively, the CDR cohort had a greater improvement in neck disability index scores as compared to the ACDF cohort. Similarly, neurologic success rates were 8%, 9.6%, and 6.1% greater in the CDR group as compared with the ACDF group at 24-, 36-, and 60-month follow-up, respectively (P = .006, P = .004, and P = .051, respectively). The ACDF group experienced a 1.9% revision rate and 3.4% rate of supplemental fixation compared with a 0% revision rate and 0% supplemental fixation rate in the CDR group. The authors concluded that the Prestige CDR provided superior range of motion and outcomes than ACDF for single level procedures, and was noninferior for a number of other outcomes such as arm pain, neck pain, adjacent segment ossification, dysphagia, implant removal, and adjacent-level surgery. A number of other studies echoed these results for different types of CDR devices. 3,6,7,10,25 While we cannot conclude from our study that devices other than the one we investigated have superior HSU scores over ACDF, the homogeneity of results from clinical studies investigating different CDR devices does suggest we may extrapolate our results to other devices.
An important aspect of the 2 treatment modalities (CDR vs ACDF) involves preservation of range of motion. Radiographic and cadaveric studies have demonstrated that ACDF restricts range of motion, which may have an effect on the biomechanics at adjacent levels. 26 –28 While the debate remains as to whether adjacent-level degeneration results from fusion or is simply a progression of the natural history of DDD, it is important to note that the CDR devices preserve substantial range of motion postoperatively. 11,12 Kim et al 12 demonstrated that range of motion of the functional spinal unit and overall range of motion during the early postoperative period (<3 months) was statistically smaller compared with preoperative range of motion, but after 3 months returned to levels comparable to preoperative. This maintenance of range of motion may be not only a benefit in itself but also may reduce the biomechanical strains placed on the cervical spine. Theoretically, this may in turn reduce adjacent segment degeneration and need for adjacent-level surgery, which is corroborated by some of the clinical studies comparing adjacent-level surgery following CDR and ACDF. 2,4
We observed that at 5 years for both 1- and 2-level procedures CDR provides superior health state utility. These findings, complemented by the literature on outcomes and cost-effectiveness of CDR compared to ACDF, suggest CDR as an effective alternative to ACDF for treating 1- and 2-level DDD.
Limitations
There are several limitations worth noting in the present study. This study represents the results of a single manufacturer’s implant. The results presented here may not be applicable to other CDR devices, though we remain confident that our results could be extrapolated to other devices. Another potential limitation of this study is the use of the SF-36 to calculate the HSU of patients having undergone CDR or ACDF. While conversion of the SF-36 to a SF-6D is an accepted means of obtaining a HSU value, the SF-36 remains a general health instrument and is not specific to the spine. A more spine-specific measure of HRQoL would have provided a more accurate assessment of the true postoperative state of the patients in the 2 cohorts. Finally, we used data from a FDA IDE study, and therefore the data we used is subject to the same limitations of the original study.
Conclusions
The health utility values for 1- and 2-level ACDF and CDR were calculated for the preoperative baseline state, and at the 12-, 24-, 36-, and 60-month postoperative state. Overall, CDR was found to have a higher health utility state for 1- and 2-level procedures at every time point. One- and 2-level ACDF procedures did not differ in their health utility state at any time point. Similarly, 1- and 2-level CDR demonstrated similar health utility score at every time point. This study suggests that CDR results in a higher postoperative health utility state than ACDF. Future prospective randomized trials are needed to confirm the results of this study that demonstrate CDR may be an effective alternative to ACDF for managing degenerative conditions of the cervical spine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.