
Abstract
Objective
To determine whether pain is associated with gait instability in patients with lumbar disc herniation (LDH).
Methods
This retrospective cross-sectional study used data from electronic medical records. Among patients with lumbar back pain caused by LDH between January 2017 and July 2019, patients that underwent gait analysis were included. LDH was diagnosed using magnetic resonance imaging. An OptoGait photoelectric cell system was used for gait evaluation. Instability was measured using a gait symmetry index. Multivariate linear regression analysis was performed to determine the association between lumbar pain and gait instability.
Results
A total of 29 patients (12 females [41.4%] and 17 males [58.6%]; mean ± SD age, 40.6 ± 12.0 years) with LDH were enrolled in the study. With each 1-point increase in lumbar pain on the numeric rating scale, the symmetry index of the stance phase (0.33; 95% confidence interval [CI] 0.04, 0.62), swing phase (0.78; 95% CI 0.14, 1.43) and single support (0.79; 95% CI 0.15, 1.43) increased.
Conclusions
Gait instability in patients with LDH may occur due to an increase in pain.
Introduction
Lumbar disc herniation (LDH), a leading cause of lumbar pain, is the displacement of the nucleus pulposus beyond the normal range due to external forces or degenerative changes in the lumbar disc. 1 LDH is the most common cause of sciatica, affecting 796.1 per 100 000 person-years in the Republic of Korea. 2 Lumbar and radiating leg pain are the main symptoms of LDH and these affect the patient’s activities of daily living and quality of life. 3
Gait is a product of the simultaneous dynamic movement of several joints in the lower extremities, moving the body from one point to another by alternating the stance and swing phases. 4 Factors that affect normal gait include sex, age, weight, body weight support and muscle strength of the lower extremities.5,6 Accordingly, if there is injury to any of the tissues that are involved in gait, the complex gait mechanism would be disturbed and movement efficiency would decline.5,6
Several studies have investigated the effects of pain on gait. For example, a previous study found that chronic pain was associated with a slower gait in older adults. 7 Another study demonstrated that pain reduction reduces gait asymmetry in patients with chronic lumbar pain. 8 LDH-related pain is usually more severe than non-specific lumbar pain and is often associated with radiating pain. Patients with LDH had greater pelvic rotation when walking, and the relative phase of the horizontal rotation of pelvis and thorax decreased compared with healthy subjects. 9 However, this previous study mainly investigated gait, pelvic rotation and the coordination of the thorax and arms, but no detailed analysis of gait symmetry was presented. 9 This current study aimed to examine the association between pain and gait instability among patients with LDH.
Patients and methods
Study design and patient population
This retrospective cross-sectional study used the electronic medical record (EMR) of patients with LDH that had lumbar pain. The reporting of this study conforms to the STROBE statement. 10 The medical charts of all patients that visited the Jaseng Hospital of Korean Medicine, Seoul, Republic of Korea between January 2017 and July 2019 and underwent gait analysis were extracted. The inclusion criteria were as follows: (i) patients with protruded or extruded discs confirmed on magnetic resonance imaging (MRI); (ii) as none of the patients underwent clinical examination and gait measurements on the same day, to increase the validity of the measured parameters, only patients in whom the difference between the date of clinical examination and the date of gait analysis was ≤7 days were included in the study. The exclusion criteria were as follows: (i) patients aged <20 years that might have different responses to lumbar pain;11,12 (ii) patients with no lumbar disease that had visited the hospital with problems such as neck or ankle diseases; (iii) patients that did not undergo lumbar MRI or those whose MRI did not include findings of disc protrusion or extrusion; and (iv) patients in whom their gait analysis values were erroneous.
The study protocol was approved by the Institutional Review Board of Jaseng Hospital of Korean Medicine (Approval number: JASENG 2019-07-005; Approval date: 8 August 2019; Location: 536, Gangnam-daero, Gangnam-gu, Seoul, Republic of Korea) and followed relevant guidelines. The requirement of informed consent from the study population was waived by the same Institutional Review Board and all data were de-identified.
Demographics and numeric rating scale for pain
Sex, age, weight, numeric rating scale (NRS) pain score and hospitalization status of patients were collected from the EMR. Amis Technology version 3.01.00 (Amis Technology, Seoul, Republic of Korea) was used for the EMR. The information in the EMR was measured by a Korean medical doctor during the patient’s first visit. Lumbar and radiating pain was measured using the NRS. 13 NRS is a patient-guided score that rates pain level on a scale of 0 to 10, where 0 denotes no pain and 10 denotes excessive pain.
Diagnosis of lumbar disc herniation
The diagnosis of LDH in this study was based on MRI results. LDH was categorized according to the degree of herniation of the nucleus pulposus as follows: (i) disc bulge: when the nucleus pulposus exceeded the normal range by more than 3 mm but there was no annulus fibrosus tear; (ii) protruded disc: when the nucleus pulposus was close to extrusion, but part of the lateral annulus fibrosus was intact; and (iii) extruded disc: when the annulus fibrosus was torn across its entire thickness from the medial side to the lateral side, such that a part of the nucleus pulposus extruded the lumbar disc. 14 This study included only those with protruded or extruded discs because it is difficult to be confirm that the disc herniation is the cause of back pain in patients with only bulging discs. 15 Additionally, lumbar disc degeneration was examined by a radiologist based on MRI signal intensity, disc structure, distinction between the nucleus and annulus and disc height. 16
Gait parameters
Gait parameters were measured using the OptoGait photoelectric cell system (Microgate, Bolzano, Italy). 17 The OptoGait system was placed on the sidebars of a treadmill. The system comprised a transmission bar and a reception bar. Each rod measured 100 × 8 cm and contained 96 photodiodes. Data were extracted at 1000 Hz and stored in a computer using OptoGait software version 1.11.50 (Microgate).
One physiotherapist that had passed the national examination after undergoing a 4-year regular physical therapy college curriculum was responsible for operating the system software and for data collection. The subjects attended the gait test wearing light-weight and comfortable clothes and walked barefoot on the treadmill at a speed of 0.83 m/s for 5 min. 18 Gait was recorded for 3 min, excluding the first and last minutes. The instability in step (cm), stance phase (%), swing phase (%), single support (%), step time (s), cadence (steps/min) and distance (cm) were analysed (Table 1), which were commonly investigated in previous studies.6–8
Definition of the gait parameters used in a study to investigate the association between pain and gait instability.

The gait stability index was used to measure gait instability.
19
The index is used to measure the asymmetry between the left and right that arises during gait as a percentage. Perfect symmetry is represented as 0% and increasing values indicate increasing asymmetry.

Statistical analyses
All analyses were performed using R Studio software (version 1.1.463; Copyright 2009–2018; R Studio, Boston, MA, USA). Continuous variables are represented as mean ± SD and categorical variables as frequency and percentage. Multivariate linear regression analysis was performed to determine the association between lumbar pain and gait instability. In the multivariate model, changes in association were observed by adding covariates; and the interaction between the NRS of lumbar pain and the NRS of radiating pain was estimated separately. For the main analysis, the covariates that were selected were sex5,20 and age. 5 For the sensitivity analysis, body mass index (BMI) 21 and radiating pain was additionally adjusted. A P-value <0.05 was considered statistically significant.
Results
This retrospective study reviewed the medical charts of 114 patients that underwent gait analysis. Of the 114 subjects, 96 patients underwent lumbar MRI, of which 70 MRIs were performed in hospital and were examined by radiologists. The remaining MRIs from other medical institutions were diagnosed by two resident Korean medical doctors in rehabilitation medicine with a clinical experience of at least 3 years. In case of inconsistency in the diagnosis (n = 5), a third party, a Korean medical rehabilitation specialist with 7 years of clinical experience, made the diagnosis. Of the 114 patients, 85 were excluded for the following reasons: (i) aged <20 years because they might have different responses to lumbar pain (n = 4); (ii) patients with no lumbar disease that had visited the hospital with problems such as neck or ankle diseases (n = 8); (iii) patients that did not undergo lumbar MRI or those whose MRI did not include findings of disc protrusion or extrusion (n = 22); (iv) those patients in whom the gait analysis values were erroneous (n = 2); and (v) those patients in whom the clinical examination and the date of the gait analysis was >7 days apart (n = 49). A total of 29 patients (12 females [41.4%] and 17 males [58.6%]; mean ± SD age, 40.6 ± 12.0 years) with LDH met the inclusion criteria and were enrolled in the study. The clinical and demographic characteristics of the study cohort are presented in Table 2. The majority of patients (n = 28, 96.6%) were hospitalized. A total of 23 of 29 patients (79.3%) had disc herniation in the L4–L5 area and 19 of 29 (65.5%) were diagnosed with lumbar disc extrusion.
Demographic and clinical characteristics of the patients (n = 29) with lumbar disc herniation that were enrolled in a study to investigate the association between pain and gait instability.
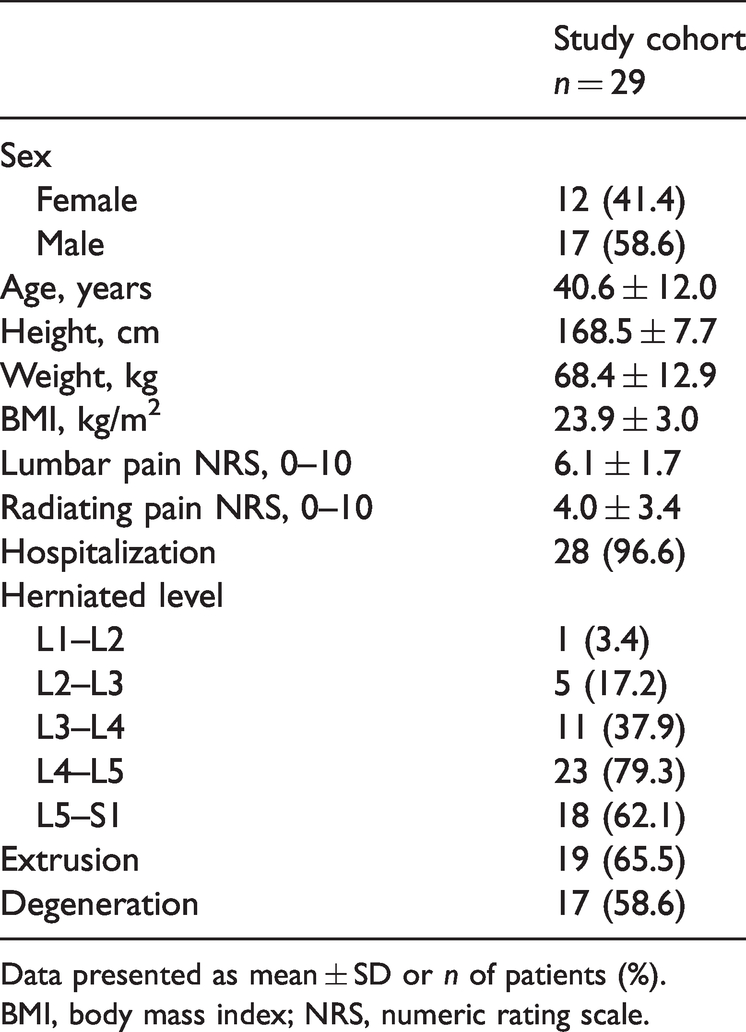
Data presented as mean ± SD or n of patients (%).
BMI, body mass index; NRS, numeric rating scale.
The distribution of gait and symmetry index is presented in Table 3. Figure 1 presents the distribution of pain and symmetry index. There was a positive correlation between the stance phase, swing phase, single support and lumbar pain NRS. Additionally, the distribution of the corresponding symmetry indices was similar.
The distribution of gait and the symmetry index in a study that enrolled patients (n = 29) with lumbar disc herniation to investigate the association between pain and gait instability.
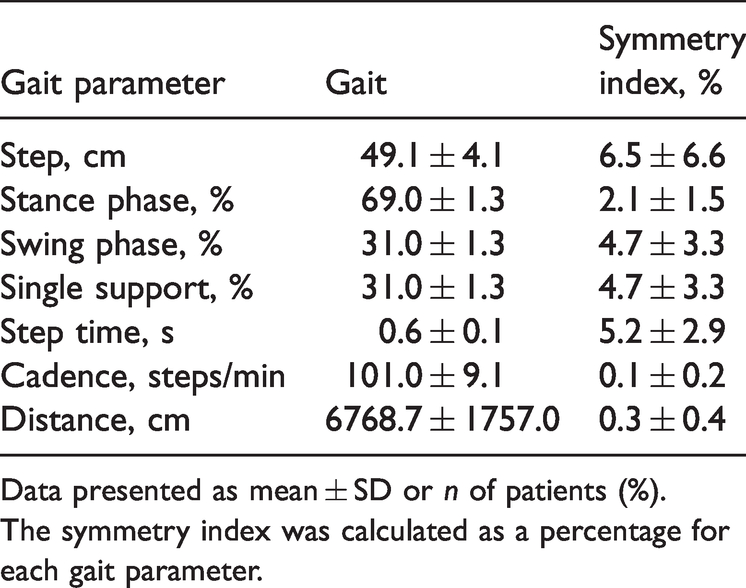
Data presented as mean ± SD or n of patients (%).
The symmetry index was calculated as a percentage for each gait parameter.

The distribution of symmetry index by lumbar pain. The y-axis shows the symmetry index and the x-axis shows the lumbar pain using numeric rating scale (NRS) scores. The blue line represents the linear association between symmetry index and lumbar pain. PCI, phase coordination index. The colour version of this figure is available at: http://imr.sagepub.com.
The association between lumbar pain NRS and gait instability was significant in all models (Table 4). When sex and age were adjusted (model 2), a 1-point increase in the NRS of lumbar pain was significantly associated with the symmetry index of the stance phase (0.33; 95% confidence interval [CI] 0.04, 0.62), swing phase (0.78; 95% CI 0.14, 1.43) and single support (0.79; 95% CI 0.15, 1.43). The above trend remained constant even after including BMI and radiating pain corrections (model 3). However, the interaction between lumbar pain and radiating pain was not significant.
Multivariate linear regression analysis of the association between lumbar pain and gait instability in patients (n = 29) with lumbar disc herniation.

Multivariate linear regression analysis: the independent variable was numeric rating scale (NRS) scores of lumbar pain; and the dependent variable was symmetry index of gait parameter (%). All estimates are presented with the 95% confidence interval (CI). Model 1: univariate model, NRS of pain; model 2: multivariate model, adjusted with sex, age, and body mass index (BMI); model 3: multivariate model, adjusted with sex, age, BMI and NRS of radiating pain. Interaction: interaction with NRS of lumbar pain and radiating pain in model 3. *P < 0.05.
Discussion
To the best of our knowledge, this is the first study to analyse the effects of pain on gait instability in patients with LDH. This current retrospective cross-sectional study analysed EMR data and MRIs reviewed by clinicians. The results of this current study demonstrate that lumbar pain was significantly associated with instability in the stance phase, swing phase and single support. A previous study found that lumbar pain might be associated with increased stance phase and reduced swing phase. 8 The results of the current study demonstrate that the gait instability of the corresponding phases in patients with LDH may be affected by pain.
The gait cycle is divided into a stance phase and a swing phase. The stance phase is when the soles of the feet come into contact with the ground and support the body weight. The swing phase is when the feet are in the air. In the normal gait cycle, the stance phase accounts for approximately 60% and the swing phase accounts for approximately 40% of the overall activity. 22 Since the swing phase occurs in the contralateral lower limb while the stance phase occurs in the other lower limb, an abnormality in the stance phase of one side naturally leads to abnormality in the swing phase. Also, during the stance phase, up to 10–50% of the gait cycle consists of single support; and there is a correlation between swing phase and single support. 23
Gait instability due to pain in patients with LDH is considered to be related to a fear-avoidance behaviour in patients.24,25 This behaviour comprises the avoidance of movement because of the fear of pain and this fear has a significant effect on physical activity.26,27 This mechanism can lead to changes in the pelvic angle. 28 Patients with lumbar pain avoid flexion for fear of pain, excessively increasing lordosis during gait and leading to changes in the pelvic angle. 29 In addition, pelvic deviations can be observed in patients with LDH, during their attempts to avoid pain, 30 and this fear-avoidance behaviour causes physical changes, which lead to step instability. 28
Furthermore, neuromuscular impairment and physical instability caused by muscular dystrophy may affect patients. 31 Patients with LDH are more likely to develop neuromuscular impairment; 31 and the cross-sectional area of the psoas muscle may decrease, depending on the level and severity of disc herniation. 32 This mechanism can lead to muscular and gait instability. 33 Instability can also be caused by motor control problems of the core muscles (e.g. the transversus abdominis and lumbar multifidus muscles). 32 In addition, weakness in the individual muscles during gait increases the activation of weak muscles and leads to compensatory activation of other muscles. 34 However, this compensation is generally inefficient and produces unbalanced joint moments. 34 In particular, hip abductors, hip flexors and plantar flexors are sensitive to muscle weakness. 34 Further studies on the volume and function of muscles affecting gait in patients with LDH are warranted.
This current study had several limitations. First, the number of patients was small, so there might have been a selection bias. Although the characteristics of this current sample were similar to those of previous studies,35,36 studies with larger sample sizes are needed to ensure generalizability of the results. Secondly, as this was a retrospective cross-sectional study, the dates of clinical examination and gait measurement did not coincide. Although the sample was restricted based on examination dates (i.e. the difference between the date of clinical examination and the date of gait analysis was ≤7 days), measurement bias still existed. Thirdly, to investigate the mechanisms of gait instability, movement and coordination in other areas (e.g. pelvic, shoulder) should be examined. These limitations may be resolved in future studies by prospective patient recruitment.
In conclusion, in patients with LDH, lumbar pain was found to be associated with gait instability. Therefore, gait instability may occur in patients with LDH due to an increase in pain.
Footnotes
Acknowledgements
We thank Mi-Hye Kim, Jae-Min Son and Hoo-In Jo for preparing the study’s dataset.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from funding agency in the public, commercial, or not-for-profit sectors.