
Abstract
The treatment of chronic back pain is a challenging problem. Facet joint infiltration is an established treatment for chronic low back pain caused by arthrosis of the lumbar facet joints. Due to the increasing number of patients with chronic low back pain, this therapy has become more frequent. We treated a 51-year-old male patient, who developed an epidural hematoma 2 months after infiltration therapy. Our case shows that even a delayed onset of spinal epidural hematoma is possible and should be kept in mind as a possible cause of acute myelopathy after spinal intervention.
Case report
A 51-year-old man came to our outpatient clinic due to low back pain (LBP) without neurologic problems. The physical examination revealed no motor or sensory deficits. A trauma was denied. Laseque’s and Bragard’s sign had been initially slightly positive on the left side, whereas on the right side both were negative. The patient had been complaining about LBP for over 3 years and had consulted several resident doctors in the past. Due to the intensive, immobilizing pain, the patient was admitted to the hospital. In our hospital, we suggest a concept of inpatient gradual diagnosis. This includes stepwise structural and functional components. In the inpatient clinic, the patient was assessed again and the pain was judged as a central LBP without a radicular component.
As a first step, the patient was pharmacologically treated with Novalgin® 500 mg (Metamizol) four times per day, Valoron N retard® 100/8 mg (Tilidin and Naloxon) twice per day, and Oxygesic® 10 mg (Oxycodon) up to six times a day on request, as well as Mydocalm® 50 mg (Tolperisonhy-drochlorid) at night. Additionally, the patient received physiotherapy. As a standard procedure in our clinic, immobilized patients received Monoembolex® 3000 (Certoparin Sodium) subcutaneously as thrombosis prophylaxis every evening. Thrombosis prophylaxis was ended when the patient left the hospital.
A magnetic resonance imaging (MRI) of the lumbar vertebral column shows signal amplification especially in facet joints of the segments L5/S1 and insinuates arthrosis (Figure 1). Due to unresponsiveness to pharmacologic therapy, we went one step further and recommended facet joint infiltration. 1 On the following day, infiltrations of the facet joints of L3/L4, L4/L5, and L5/S1 were performed. We are performing facet joint injection in a procedure room for minor surgeries. There the procedure is conducted under aseptic conditions. The patient is lying on an operating table in prone position. The procedure is done under fluoroscopy to confirm needle placement. This image-guided technique is easy to perform with better results and reduces complications and thus is preferred to blind injections. 2
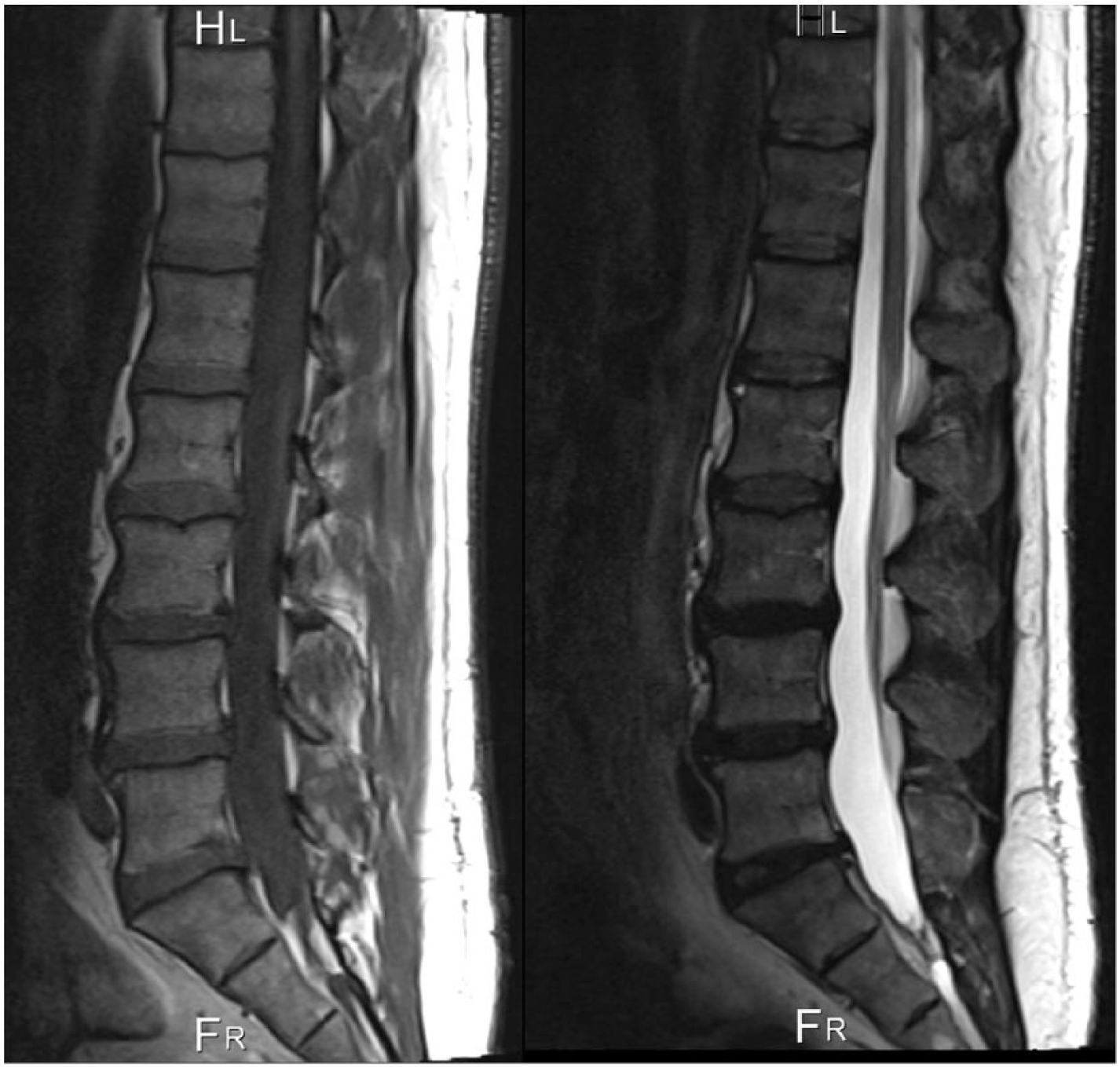
MRI in T1 (left) and T2 (right) showing the vertebral column and spinal cord of the patient prior to injection. Signs of arthrosis can be seen. No hints for larger vascular malformations can be observed.
The skin above the targeted facet joints is anesthetized with 1% Xylonest® (Prilocaine). A 23-G cannula was inserted under fluoroscopic guidance into each of the six joints. A mixture of 2% Lidocaine and 40 mg Triamcinolone was slowly injected. We applied in total a 6-mL mixture of Lidocaine 2% and 40 mg Triamcinolone, or 1 mL into each joint. Two hours after injection, the patient reported a vast reduction of pain. The following day, the injection site was clinically inconspicuous and the patient discharged with significantly reduced pain symptoms.
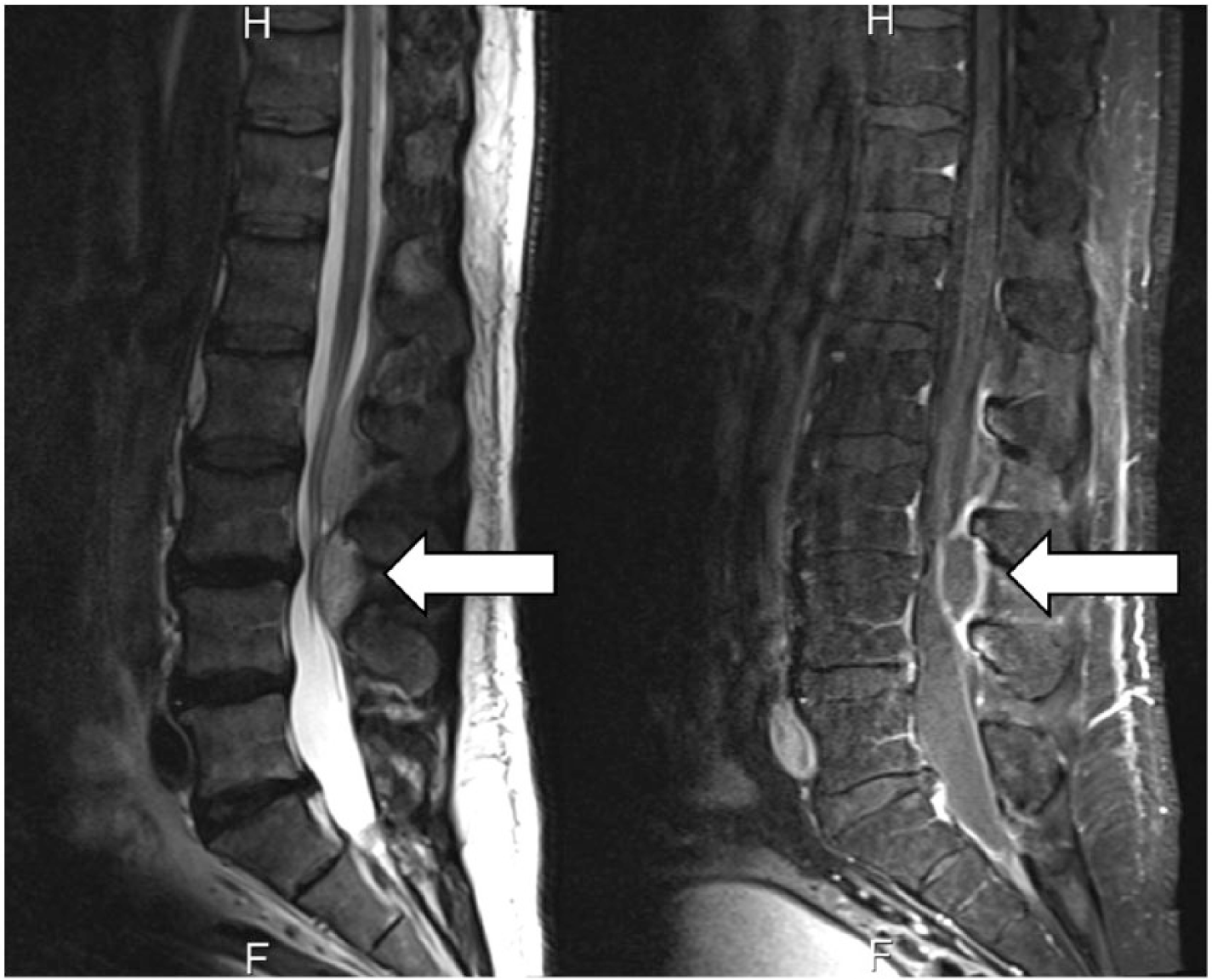
After 2 months, the patient consulted our outpatient clinic with immobilizing pain in the low back. Furthermore, the patient complained about episodes of incontinence. He did not report any leg pain or tingling in the legs. There was no sensory or motor dysfunction. Stool function was reported as normal. The patient had neither fever nor was any sign of inflammation at the injection sites apparent. After immediate hospitalization, another MRI of the lower spine as well as laboratory examination was conducted. No pathological changes were seen in the midstream urine specimen. The laboratory parameters showed a slight incline in C-reactive protein (34.8 mg/L) and creatinine (1.33 mg/dL). In particular, hemoglobin and thrombocyte count were normal. To complete our differential diagnosis, a serology for Borrelia burgdorferi was performed, yielding a negative result. MRI showed an epidural hematoma in the area of the facet joints of the segments L3/L4 (Figure 2). The space-occupying lesion led to a spinal stenosis and interfered with the caudal spinal nerves. The patient received a urine catheter. We strongly recommended immediate surgery to remove the hematoma and thereby relieve pressure on the spinal nerves. However, the patient refused any surgical intervention. In respect to his wishes, the patient was treated conservatively with short-term controls of his neurological status and laboratory examination. The patient recovered slowly. At the fifth day of hospitalization, an additional MRI of the low back was undertaken (Figure 3). There was a noticeable reduction in the size of the hematoma. The bladder function recovered completely, and pain was markedly decreasing. The patient was discharged from hospital after 6 days. We recommended follow-up visits and an immediate visit to our emergency department in any case of neurological deficits.

Initial MRI after inpatient admission 2 months after facet joint injection. A large hematoma has developed.
Follow-up MRI after 5 days of conservative treatment. A reduction in size of the hematoma and an improvement of neurological symptoms were apparent.
Discussion
Chronic LBP is one of the main causes of disability in the western world with a huge economic burden to society. In Germany, about 70% of adults have at least one episode of back pain per year. 3 One source of chronic LBP is lumbar facet joint degeneration with an incidence of 15%–45% among patients with LBP. 4 Various therapeutic techniques in the treatment of chronic facet joint pain are described ranging from intra-articular injections, medial branch blocks, and radiofrequency neurotomy of lumbar facet joint nerves. There is good evidence for the use of conventional radiofrequency neurotomy as well as for lumbar facet joint nerve blocks regarding the treatment of chronic lumbar facet joint pain resulting in short-term and long-term pain relief and functional improvement. Only limited evidence exists for intra-articular facet joint injections and pulsed radiofrequency thermoneurolysis. 2
MRI often reveals degenerative findings of the disk or facet joints of one or more lumbar motion segments. However, these MRI findings can also be observed in healthy population with no apparent symptoms. Hence, it can be challenging to match radiologic findings with patient’s symptoms. 5 Because of the broad variety of therapeutic methods, we prefer an inpatient gradual diagnostic as an established concept used to determine therapeutic strategies in patients with chronic LBP and gives relevant information about the exact level of painful arthrosis. 6 We perform test infiltrations of the facet joints with administration of analgesic and anti-inflammatory agents at different levels of the lower spine to determine the exact level of the pain causing structure as part of the inpatient gradual diagnostics. The procedure is done as mentioned above. This image-guided technique is easy to perform, gives better results, and reduces complications. Therefore, it is preferred to non-guided injections. 2 In case of positive response to a test infiltration in terms of pain relief, additional procedures can be performed if necessary. Even the effect of surgery can be temporarily simulated. Hofmann et al. 7 report that inpatient gradual diagnostic changed the treatment strategy in 39% of cases. Therefore, facet joint infiltration is a helpful procedure for diagnostic as well as for therapeutic purposes. 8 In our case, the patient had an excellent response to the facet joint infiltration and the patient was discharged. The combined use of an anesthetic and a glucocorticoid results in a better outcome than without the latter. This response pattern is the current gold standard for diagnosing the facet syndrome.9,10
Reports about immediate complications are available. Carr et al. 11 mention an overall complication rate after spine injections of 1.9% without differentiating the different types of injections. However, less attention is given to the rare, but nevertheless severe, delayed complications as reported in our case. Although studies and case reports about complications after infiltration therapy exist, the prolonged onset of an epidural hematoma has not been reported yet. 3 The etiology of the epidural hematoma still remains unclear to us. In general, several factors can be responsible for the occurrence and progression of a spinal hematoma. Among these factors are idiopathic, anatomical, mechanical, and pharmacological factors like coagulation disorders, vascular malformations, and in particular multiple attempts at needle placement or multiple injections.
The patient did not show any vascular malformation in MRI. Furthermore, coagulation disorders were not reported, and no abnormal laboratory parameters occurred prior to injection. In particular, we checked for idiopathic thrombocytopenic purpura. 12 As Wulf 13 suggests, we do not believe that thrombosis prophylaxis with Monoembolex® was a reason for the development of the hematoma.
Needle placement was performed under X-ray guidance by an experienced surgeon. Usually, complications occur either directly or shortly after the procedure. There are only a few cases of delayed onset of epidural hematomas after spinal injections reported. Nam et al. 14 describe a similar case of a 50-year-old man, who developed an epidural hematoma 1 month after an epidural block. The authors proposed a spontaneous formation of the hematoma. In spite of this, we believe that there is a connection to the injection since the location of the hematoma fits with that of the injection site. Furthermore, the patient was in good health and we saw no evidence of vascular malformations or coagulopathies.
Conclusion
Facet joint infiltration is in general a safe procedure; nevertheless, clinicians should be aware of the potential risk of serious complications. It is important to acknowledge that spinal hematomas can occur direct or delayed after facet joint infiltration. Thus, the patient should be informed about symptoms of spinal epidural hematoma in order to undergo examination early enough. Physicians must keep the cohesion of this rare but serious complication in mind, to allow a rapid diagnosis and treatment, including surgery, which may be of help to the patient.
Footnotes
Acknowledgements
The authors would like to thank Dr Jonathan Lindquist for editing the text.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institutions do not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for his anonymized information to be published in this article.