
Abstract
Study Design
Retrospective Cohort Study.
Objectives
Our study aims to analyze the effect of preoperative marijuana use on outcomes and postoperative opioid use in patients who have undergone lumbar decompression without fusion.
Methods
All patients >18 years of age who underwent lumbar decompression from 2017-2022 with documented preoperative marijuana use at our academic institution were retrospectively identified. A 3:1 propensity match incorporating demographics, procedure type, and levels decompressed was performed to compare preoperative marijuana users and non-users. 1-year preoperative and postoperative opioid consumption in milligrams of morphine equivalents and postoperative outcomes including readmissions, reoperations, and complications, were obtained. A multivariate regression model was performed to measure the effect of marijuana use on the likelihood of a spine reoperation.
Results
Of the 340 included patients, 85 were preoperative marijuana users. There were no significant differences in medical complications, 90-day readmissions, or opioid consumption preoperatively or postoperatively (P > .05). We identified a trend towards patients who used marijuana having more reoperations for any cause (20.0% vs 11.37%, P = .067). Multivariate logistic regression analysis suggested that preoperative marijuana use was a significant predictor of all-spine reoperations (OR = 2.06, P = .036).
Conclusions
In lumbar decompression patients, preoperative marijuana use does not impact opioid consumption, readmissions, or medical complications, but is a significant predictor of future postoperative reoperations. Additional research is necessary to further explore the role of marijuana use in spine surgery.
Introduction
In the United States, marijuana use has become significantly more widespread over the past two decades. 1 Based on 2020 data, an estimated 49.6 million adults use marijuana either medically or recreationally, which increased by approximately 55% over the previous 5 years. 2 Increasingly permissive legislatures in many states and changing societal attitudes have helped spur this increase in marijuana consumption. 3 As a result, it is important to continue to explore its influence on patient health as well as its potential medicinal benefits. While there is considerable research on the effects of marijuana use in other specialties, the impact of marijuana use in spine surgery has not been extensively studied.
It has been well established that chronic use of opioids leads to poorer outcomes, yet 98% of patients are prescribed opioids after surgery, which can lead to chronic use. 4 Studies have shown that increased opioid use is associated with higher morbidity and decreased improvement in pain and physical function after spine surgery.5,6 Currently, one of the most common indications for a medical marijuana prescription is chronic low back pain, either with or without radiculopathy. 7 The analgesic properties of marijuana may allow its incorporation into management regimens, thereby reducing opioid prescriptions. 8 However, several discrepancies exist in the orthopaedic literature regarding patient outcomes in marijuana users after surgery and its benefits are as of yet unproven.
While some studies have analyzed the effect of marijuana after spinal fusion, no existing studies have done so for outcomes after lumbar decompression without fusion. Lumbar decompression remains the gold-standard treatment for spinal stenosis, so understanding the impact of marijuana use in this patient population is imperative. 9 The purpose of our study was to (1) investigate the effect of preoperative marijuana use on clinical outcomes, and (2) determine if preoperative marijuana use impacts the quantity of opioids prescribed (in milligram of morphine equivalents (MME)) both 1-year preoperatively and postoperatively.
Methods
Inclusion Criteria
Upon obtaining Institutional Review Board approval (Thomas Jefferson University, Office of Human Research Institutional Review Board, Approval #19D.508), all patients 18 years of age or older who underwent one-to four-level lumbar decompression with documented marijuana (medical and/or recreational) use at our academic medical institution between 2014 and 2020 were retrospectively identified. Informed consent was waived due to the retrospective nature of the study. Patients were excluded if the lumbar decompression was performed as a revision procedure or indicated for neoplasm, infection, or trauma.
Data Extraction
Patient demographics, surgical characteristics, and surgical outcomes were collected through a manual chart review of the electronic medical record (EMR) and Structured Query Language (SQL) search. The EMR was manually reviewed to determine marijuana use up to the last preoperative appointment. Data regarding the strain, potency, intake method, or duration of marijuana use were unavailable. A 3:1 propensity match controlling for age, sex, race, body mass index (BMI), levels decompressed, smoking status, and Charlson Comorbidity Index (CCI) was then performed to match patients with documented marijuana use to non-users from an internal database of lumbar decompressions.
Ninety-day readmissions, complications, and reoperations within three years of the index procedure were recorded. Reoperations included epidural hematomas, repair of cerebrospinal fluid leaks, and subsequent fusion and decompression procedures. For each patient, the total quantity of opioid prescriptions in morphine milligram equivalents (MME) prescribed one year preoperatively and one year postoperatively was collected through our state’s Prescription Drug Monitoring Program (PDMP) database.
Statistical Analysis
Descriptive statistics, including mean and standard deviation, were used to report patient demographics, surgical characteristics, and surgical outcomes. A Shapiro-Wilk test was used to analyze the normality of each continuous variable. Parametric data were analyzed with independent t-tests, while non-parametric data were analyzed with Mann-Whitney U tests. Categorical variables were analyzed with Pearson’s chi-square analysis. A multivariate logistic regression model was developed to measure the effect of marijuana use on the likelihood of undergoing a spine reoperation for any cause when accounting for age, sex, BMI, smoking status, CCI, and the number of levels decompressed. R software, version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria), was used for data analysis. Statistical significance was set at P < .05.
Results
Patient Demographics
Patient Demographics and Opioid Consumption.
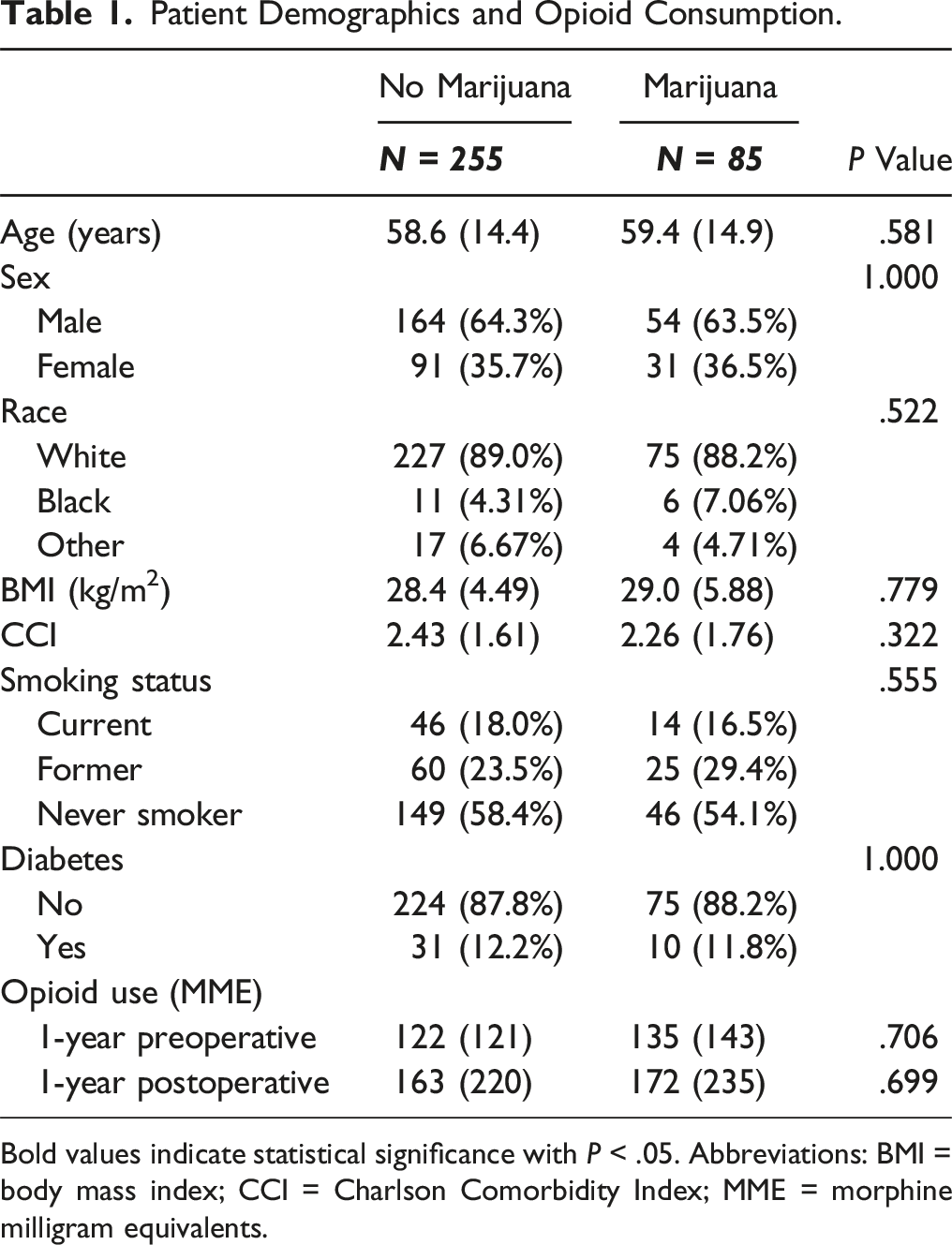
Bold values indicate statistical significance with P < .05. Abbreviations: BMI = body mass index; CCI = Charlson Comorbidity Index; MME = morphine milligram equivalents.
Surgical Characteristics.
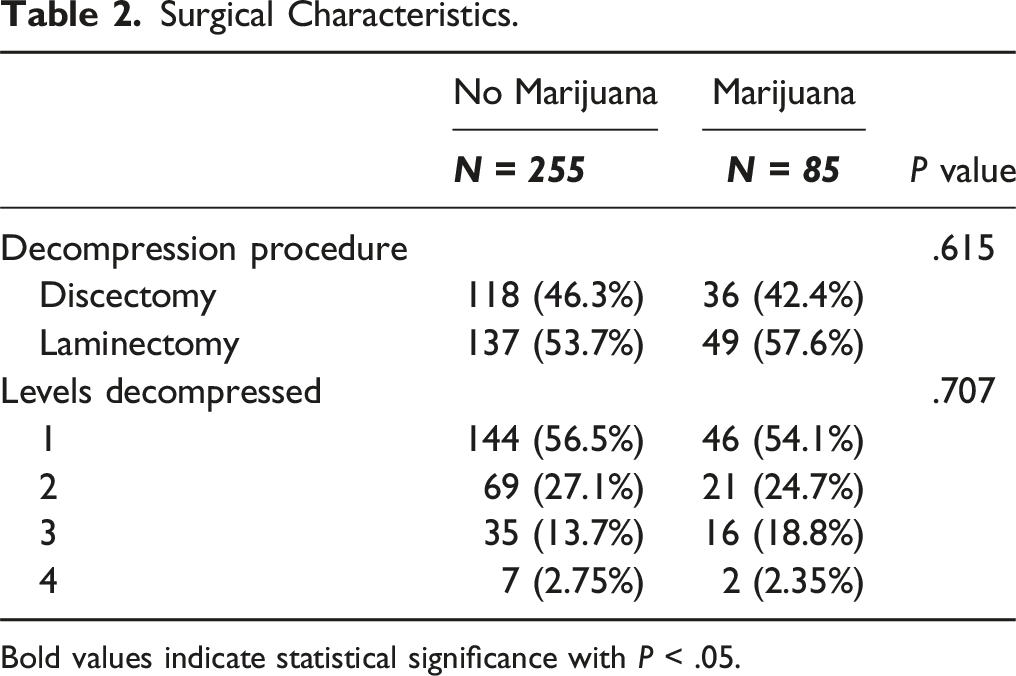
Bold values indicate statistical significance with P < .05.
Opioid Use
There were no significant differences in 1-year preoperative (135 ± 143 vs 122 ± 123 MME, P = .706) or 1-year postoperative (172 ± 235 vs 163 ± 220 MME, P = .699) opioid use based on MME between patients who used marijuana and patients who did not (Table 1).
Surgical Characteristics and Outcomes
Postoperative Outcomes.
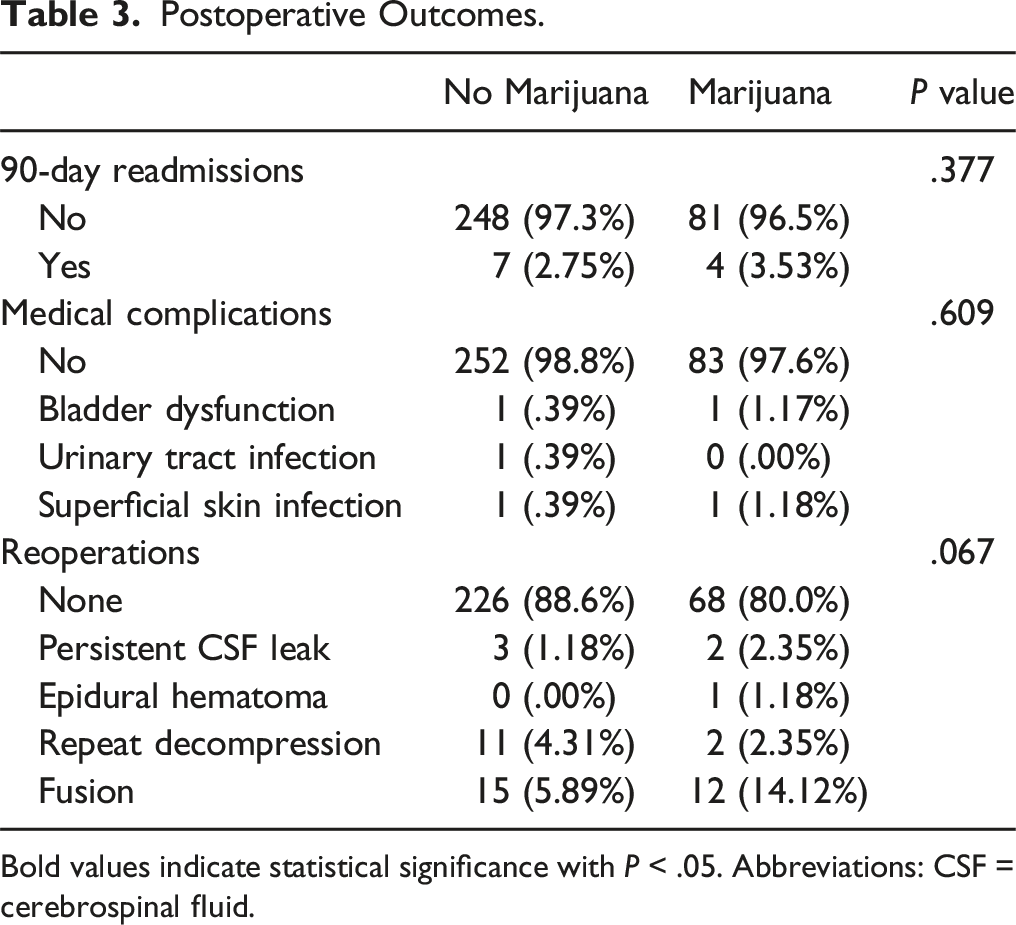
Bold values indicate statistical significance with P < .05. Abbreviations: CSF = cerebrospinal fluid.
Multivariate Logistic Regression for Reoperations.
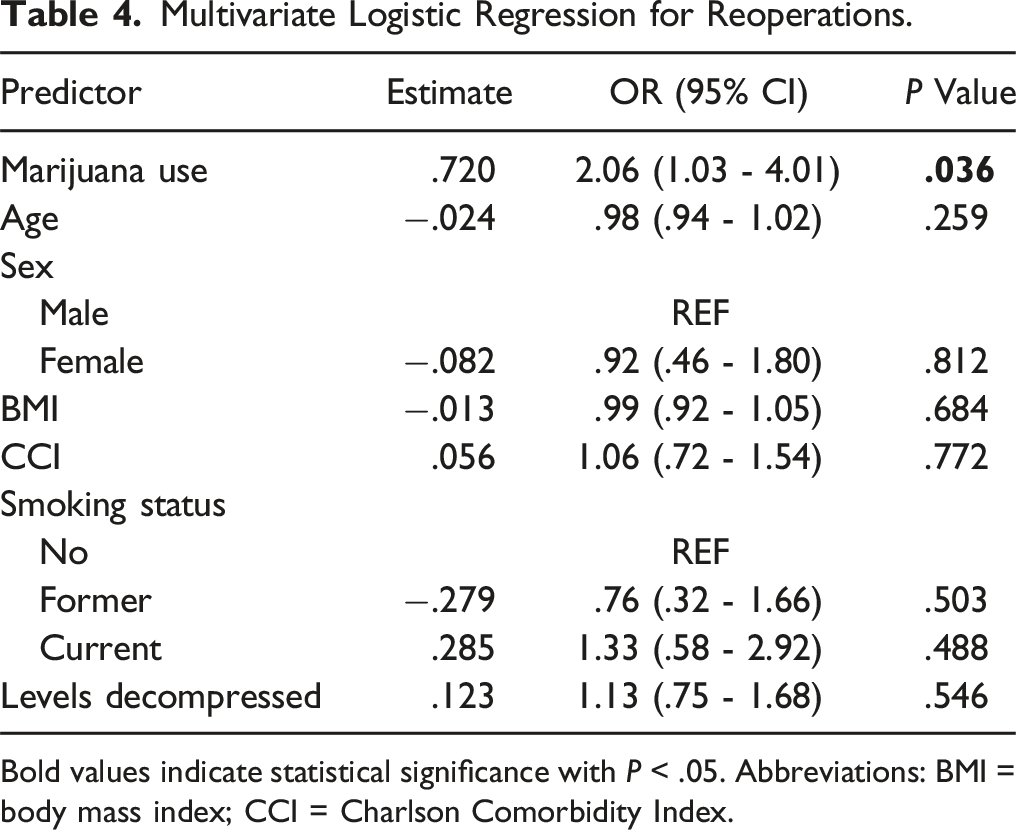
Bold values indicate statistical significance with P < .05. Abbreviations: BMI = body mass index; CCI = Charlson Comorbidity Index.
Discussion
Lumbar decompression is one of the most utilized spine procedures in the United States. Hence, identifying factors affecting postoperative outcomes and opioid use is valuable, particularly with the current opioid epidemic and the known consequences of chronic opioid use. 7 As marijuana legislation expands, it has become a promising alternative for pain management in spine surgery. 10 While few studies investigate its use in spine surgery, to our knowledge, none have analyzed the effects of marijuana use on patients undergoing lumbar decompression without fusion. Our findings suggest that preoperative marijuana use does not impact the amount of opioids prescribed nor does it increase postsurgical complications or readmissions. However, multivariate regression analysis identified that it is significantly correlated with increased lumbar spine reoperations in the subsequent three years.
The effects of preoperative marijuana use on postoperative outcomes after lumbar decompression may be of great interest to spine surgeons due to its impact on clinical outcomes, including mitigating healthcare costs and improving patient satisfaction.11-13 In our study, marijuana use did not significantly impact either postsurgical complication or readmission rates. Prior retrospective studies analyzing outcomes between marijuana users and non-users have reported varying findings regarding marijuana’s effect on postoperative outcomes. One study analyzing differences in patients undergoing inpatient spine surgery found that patients who used marijuana had more medical complications as well as higher hospital costs. 14 A separate retrospective study consisting of 102 patients undergoing transforaminal lumbar interbody fusion found patients experienced similar rates of complications, regardless of whether they used marijuana or not. A propensity-matched national database study of 704 patients undergoing thoracolumbar fusion for adult spinal deformity showed lower rates of complications in marijuana users.15,16 When analyzing marijuana’s effect on readmission rates, a retrospective propensity matched study found there were no differences in readmission rates after lumbar fusion, although there was a greater readmission rate identified in a propensity matched retrospective cohort study in a population of patients undergoing anterior cervical discectomy and fusion.17,18 Outside of spine surgery, other orthopaedic literature has also shown significant associations between preoperative marijuana use and medical complications and readmissions. 19 Future studies are necessary to clarify the effects of marijuana on these outcomes, but spine surgeons should consider informing patients of the potential postoperative risks associated with marijuana use.
Excellent outcomes following spine surgery are reliant on achieving adequate perioperative pain management, which is a key driver of patient satisfaction. As a result, spine surgery is at higher risk of causing patients to become persistent opioid users, with the rate ranging from 4% to 26% depending on the surgical invasiveness.10,20,21 Spine patients have often had prior exposure to opioids as part of the non-operative treatment for their pain, and opioids remain the most widely employed method of pain management postoperatively. Additionally, patients with preoperative opioid use before spine surgery often fail to discontinue their opioid intake postoperatively, even if the opioids were consumed solely for the medical conditions for which they required surgery.22,23 Hence, there is an urgent need for solutions that provide adequate pain management without opioids. Marijuana may be an alternative option.24,25 Due to the indirect activation of μ-opioid receptors by cannabinoids, marijuana has the potential to allow spine surgeons to decrease the volume of opioid prescriptions by incorporating marijuana into pain management regimens. 26
Marijuana’s theoretical benefit to mitigate opioid consumption has been contested by various studies in the literature. Our study did not identify a significant difference in preoperative or postoperative opioid use between marijuana users and non-users, which aligns with previous studies which also analyzed marijuana’s effect on opioid use in patients undergoing ACDF and lumbar fusion respectively.17,18 Furthermore, some studies have reported increased opioid usage after spine surgery in marijuana users. A retrospective review of 220 posterior lumbar fusion patients by Moon et al. 27 found an association between cannabis use and increased use of opioids both while in-patient and post-discharge. Another retrospective review also showed an association between a history of cannabis use and increased postoperative opioid use following elective ACDF. 28 In fact, there is concern that marijuana use increases opioid use by acting as a gateway drug, as marijuana attenuates dopamine release, which has been shown to inversely correlate with addiction severity and craving.29,30 Several national studies on addiction have shown marijuana users were less likely to decrease opioid use than non-users and had an increased likelihood of developing opioid use disorders.31-33 Hence, the analgesic effects of marijuana and its potential to increase dependence may counteract each other and explain why studies have not shown a decrease in opioid use.
Interestingly, our multivariate regression analysis found that marijuana use was a significant predictor of spine reoperations within three years of index lumbar decompression. While long-term opiate use and smoking have previously been associated with an increased risk of reoperations, this is the first clinical study to observe a relationship between marijuana use and reoperations after lumbar decompression.34,35 We found that most reoperations were due to recurrent index-level pathology that warranted additional decompression or fusion procedures. Possible explanations for these findings are that spine surgeons utilize subsequent procedures as a therapeutic option for pain management or may feel inclined to assist patients in decreasing their reliance on marijuana to manage their chronic back pain. While our study did not analyze differences in patient-reported outcomes between marijuana users and non-users, other studies have shown greater postoperative pain levels in marijuana users after spine fusion. In one study, at both six months and a year postoperatively, marijuana users experienced more severe back pain, indicated by higher VAS-Back and ODI scores, and lower physical health, indicated by lower PCS-12 scores.17,18 The inclusion of patient-reported outcomes in future studies will aid in contextualizing our findings, but overall, this discussion emphasizes our lack of understanding of marijuana use and its effect on postoperative pain after spine surgery.
Our study had some limitations, including our reliance on our state’s PDMP registry, which utilizes interstate data sharing; however, this feature does not yet apply to all states. Therefore, opioid prescriptions may be underestimated if prescriptions were filled in states without opioid data sharing. While we were able to review each patient’s chart for documentation of marijuana use, we were unable to determine the potency or strain of marijuana, methods or amount of consumption, or frequency of use. We were also unable to verify if each patient consumed each opioid prescription. Additionally, we could not confirm if patients continued cannabis use in the postoperative period, which could affect patient outcomes and opioid prescriptions. Finally, patients were under the care of various surgeons at our institution, introducing variability in surgical technique and postoperative care; however, this may ultimately increase the generalizability of the study.
Conclusion
Preoperative marijuana use increases the risk of reoperations after lumbar decompression but does not impact rates of medical complications or readmissions, or preoperative or postoperative opioid consumption. Given our limited understanding, further research on marijuana use in spine surgery is warranted to validate these findings and identify the impact of marijuana on surgical outcomes as well as the role, if any, marijuana may have as an alternative analgesic therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.