
Abstract
Study Design
Retrospective review.
Objectives
Cannabis is an antinociceptive which has been evaluated as a possible adjunct or substitute for opioid use in the treatment of acute pain. The aim of this study was to evaluate the association between preoperative cannabis usage and consumption of opioids for postoperative analgesia.
Methods
Patients who underwent one- or two-level posterior lumbar fusion surgery were categorized as cannabis users or non-cannabis users based on preoperative diagnoses of cannabis use. Total morphine equivalent dose was calculated for both in-house opioid consumption and postoperative prescription opioid usage. Age, ASA, BMI, depression, tobacco use, estimated blood loss, OR time, LOS, disposition to rehab, 30-day readmission, in-house opioid consumption and postoperative prescription opioid usage were compared between groups using t-tests.
Results
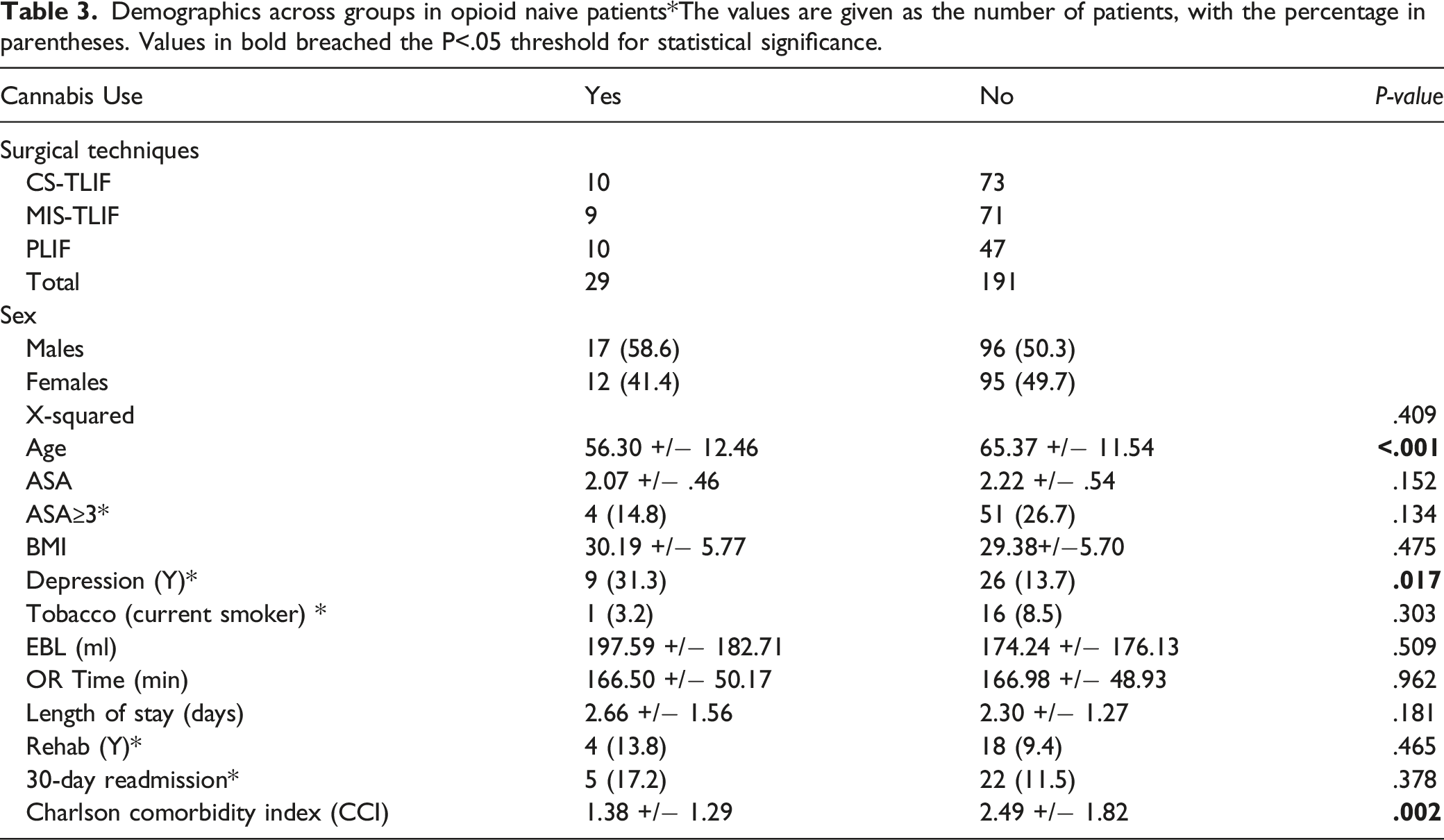
Of the 220 opioid naïve patients, 29 (13%) patients were identified as cannabis users while 191 (87%) were non-cannabis users. There were no significant associations between opioid naïve cannabis usage and ASA, BMI, tobacco use, EBL, OR time, LOS, disposition to rehab, or readmission. Opioid naïve cannabis users had greater association with depression (31.3% vs 13.7%, P=.017) and younger age (56.37 years vs 65.37 years, P<.001). Interestingly, cannabis use was associated with a lower Charlson Comorbidity Index (CCI), with 1.38 vs 2.49 (P=.002). Cannabis users were found to have increased postoperative prescription opioid usage (2545.41 POST-MED vs 1379.72 POST-MED, P=.019).
Conclusions
Cannabis usage is associated with increased usage of opioids postoperatively, both while in-patient and post-discharge, after posterior lumbar spinal fusion surgery.
Introduction
Postoperative pain management following spinal surgery remains a challenge for both clinicians and patients despite advances in pain management modalities. Opioids have traditionally been the mainstay of pain control in the acute postoperative setting, and in the United States, orthopaedic surgeons represent the third highest prescribers of opioid medications.1,2 However, they are associated with a variety of dose-related adverse effects, including respiratory depression, altered cognition, urinary retention, gastrointestinal dysfunction. 3 Perhaps the most concerning of these adverse effects is the strong psychological effect of addiction and the downstream debilitating effects of opioid misuse and dependence.
Over 4% of the adult population in the United States misuse prescription opioids, and overdose-related deaths were estimated to be more than 33 000 in 2015. 4 Due to the ongoing opioid epidemic in America, more attention is being given to alternative pain management strategies. Multimodal pain management approaches that incorporate opioids with additional form of treatment such as peripheral nerve blocks, acetaminophen, gabapentin, or NSAIDS are being implemented in the perioperative setting to reduce opioid analgesic use, mitigate the risk of associated adverse effects, while still adequately managing postoperative pain.5,6
Cannabis has antinociceptive properties which have been evaluated as a possible adjunct or substitute for opioid use in the treatment of acute pain.7-13 Usage of cannabinoid products has been gaining progressive societal and legal acceptance in the United States over the past several decades, and according to the 2019 National Survey of Drug Use and Health, cannabis continues to be the most commonly used illicit recreational drug. 14 As of November 2021, a total of 36 states, the District of Columbia, Guam, Puerto Rico, and U.S. Virgin Islands have approved comprehensive medial cannabis programs. 15 As the prevalence of cannabis consumption increases, surgeons are likely to see a corresponding increase in the number of cannabis users presenting with surgical indications for lumbar spine procedures.16,17 However, little is known about the role of cannabis in the treatment of perioperative pain and there is a paucity of data on the effects of cannabis post-operatively following spine procedures. 18
The aim of this study was to evaluate the association between preoperative cannabis usage and consumption of opioids for postoperative analgesia. Due to the prevalence of cannabis in pain management, we hypothesized that cannabis usage may be associated with decreased usage of opioid analgesics in postoperative pain relief in patients undergoing spine surgery.
Materials and Methods
Institutional review board approval was obtained prior to study initiation (IRB approval number 2020P000467). Informed consent was not required as this was a retrospective review and there was a waiver of consent. A retrospective review was performed of all patients undergoing one- or two-level posterior lumbar interbody fusion surgery at a single institution from April 2016 to March 2020. These surgeries included transforaminal lumbar interbody fusion (TLIF) with cortical screw (CS) instrumentation (CS-TLIF), minimally invasive transforaminal lumbar interbody fusion (MIS-TLIF) or posterior lumbar interbody fusion (PLIF). Patients were excluded if they had a revision procedure, if they were taking chronic opioids pre-operatively, or if the surgery involved more than two levels.
Demographic data were obtained, including patient age, gender, American Society of Anesthesiology score (ASA), BMI, depression, preoperative opioid use, smoking status, depression, cannabis usage, and Charlson Comorbidity Index (CCI). CCI predicts the ten-year survival percentage based on prevalent comorbid conditions calculated from a final score out of 37 points. Calculated factors include, but not limited to age of patient, and history of myocardial infarctions, chronic kidney disease, transient ischemic attacks, or congestive heart failure. Patient cohorts were grouped by cannabis users and non-cannabis users based on self-reported cannabis usage pre-operatively. Operative variables included number of operative levels, operative time, estimated blood loss (EBL), and intraoperative complications. Hospitalization data included opioid consumption while inpatient and post-discharge, discharge location, and 30-day re-encounters.
Opioid consumption was calculated as the total morphine equivalent dose (MED) of all opioid medications administered over the course of the patient’s inpatient hospitalization. All spine patients are started on a standardized pain regimen post-operatively including Acetaminophen 1000 mg three times daily, Oxycodone 5-15 mg every four hours as needed (prn) for pain, Tizanidine 2-4 mg every eight hours every prn muscle spasm/pain, and breakthrough IV hydromorphone. Postoperative pain medications are prescribed based on the individual needs of each patient given their level of reported pain. If patients are unable to tolerate oxycodone or oxycodone is not effective, patients receive Tramadol 25-50 mg every six hours prn pain or Dilaudid 2-6 mg every four hours prn pain. Post-discharge opioid consumption was calculated as the total MED of all opioid medications prescribed following discharge from the hospital and is referred to as “POST-MED.” Note that separate POST-MED analyses were done for patients who were not on pre-operative opioids (opioid naïve) and all patients. This is because individuals who were not opioid naïve would likely have a higher tolerance to opioid medications and possibly require more opioids to control pain over the same time period compared to opioid naïve patients.
Homogeneity of variances.
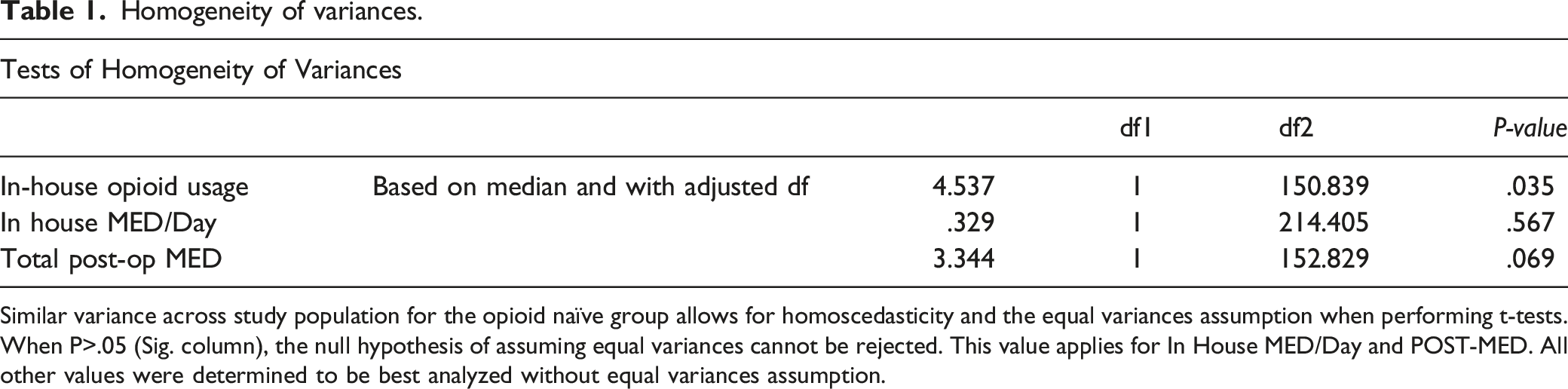
Similar variance across study population for the opioid naïve group allows for homoscedasticity and the equal variances assumption when performing t-tests. When P>.05 (Sig. column), the null hypothesis of assuming equal variances cannot be rejected. This value applies for In House MED/Day and POST-MED. All other values were determined to be best analyzed without equal variances assumption.
Results
Demographics across groups in the entire study population*The values are given as the number of patients, with the percentage in parentheses.
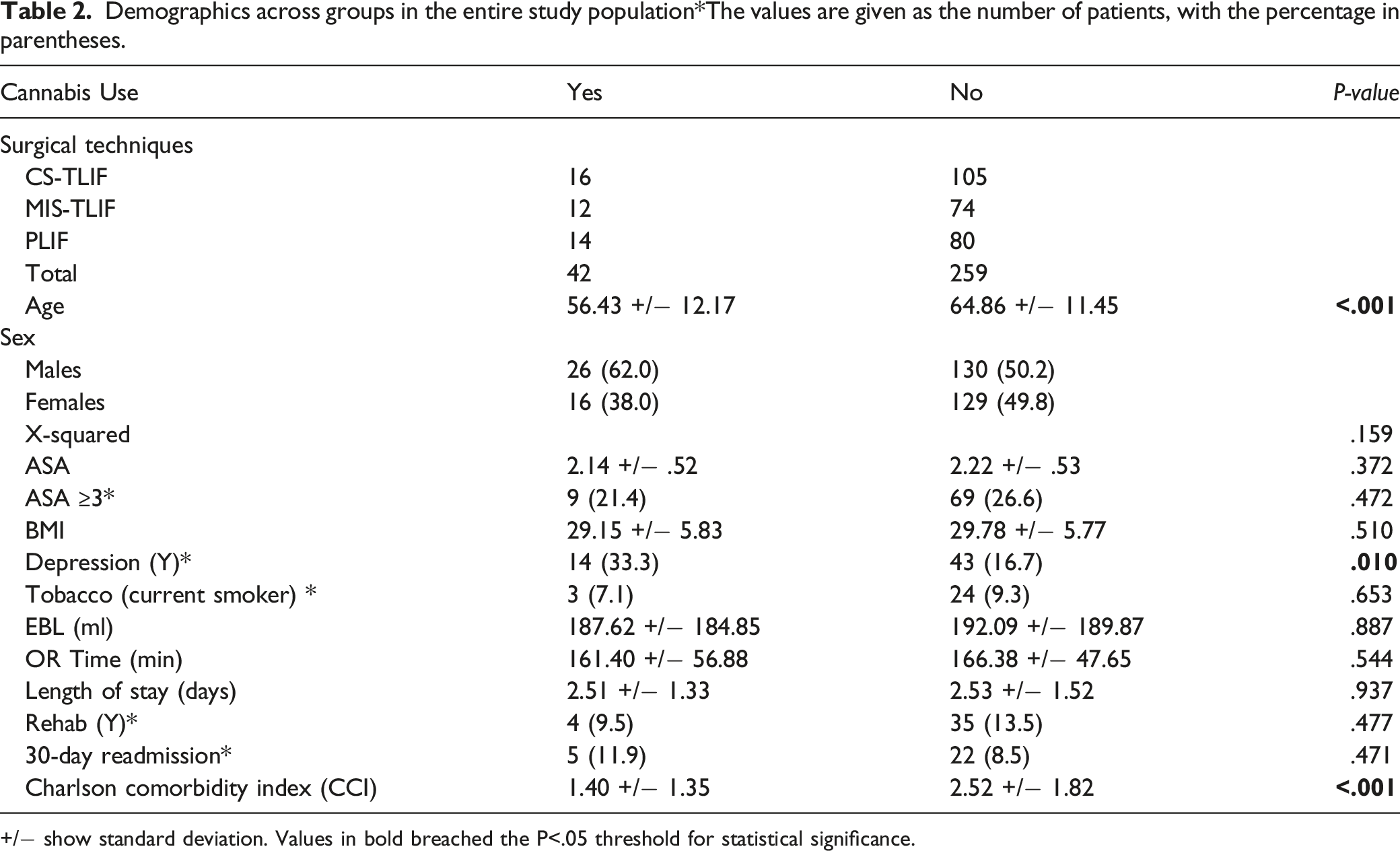
+/− show standard deviation. Values in bold breached the P<.05 threshold for statistical significance.
Demographics across groups in opioid naive patients*The values are given as the number of patients, with the percentage in parentheses. Values in bold breached the P<.05 threshold for statistical significance.
Opioid intake across groups for entire study population.

Opioid intake across groups for opioid naive patients.

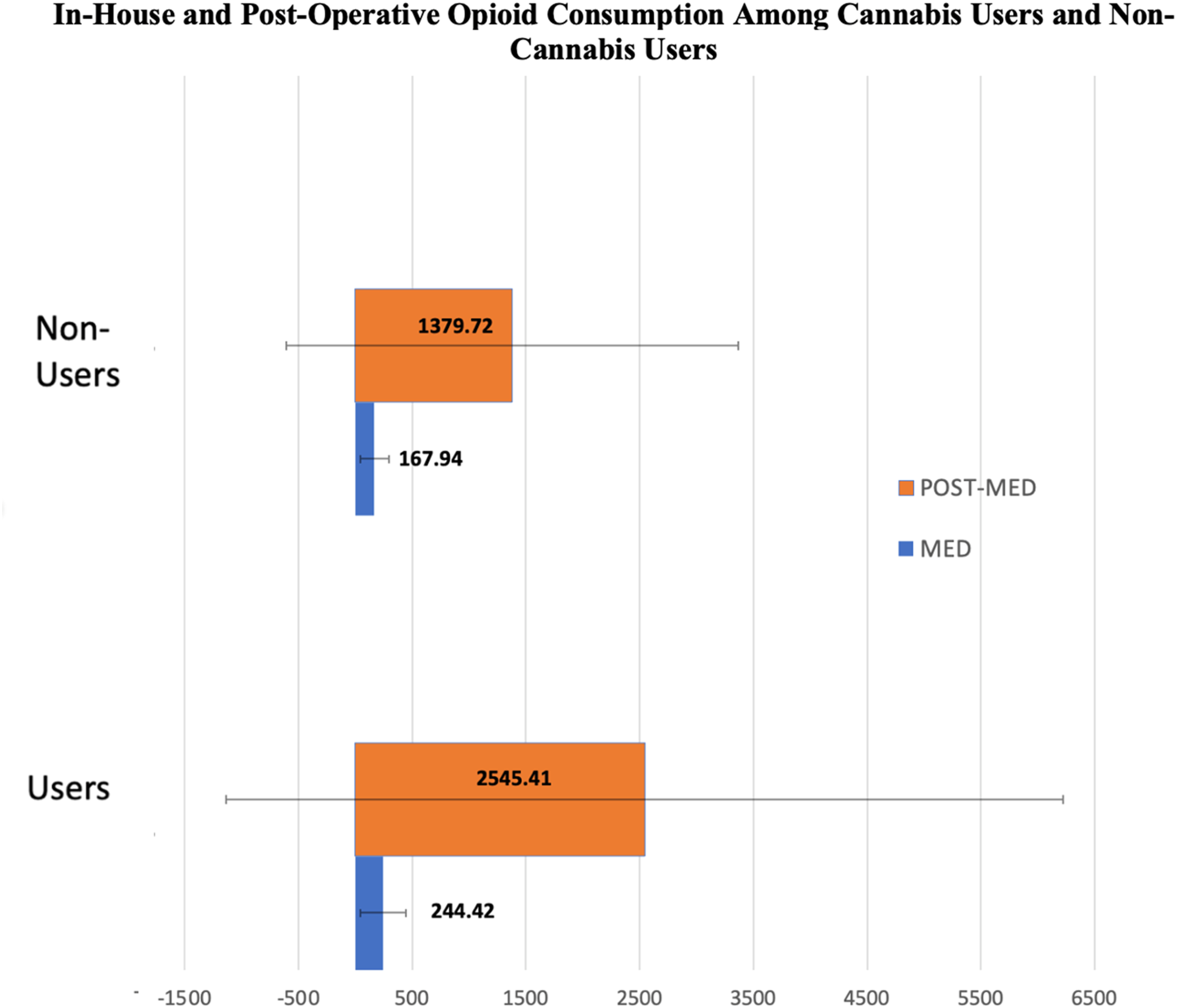
In-house vs Post-Op Opioid Consumption Among Cannabis Users and Non-Users. Units Expressed in MED.
Discussion
In the face of the ongoing opioid epidemic, alternative pain management strategies are needed to decrease consumption of opioids postoperatively. There is insufficient data on the impact of preoperative cannabis usage on postoperative pain management and opioid consumption following spinal procedures. This study is one of the first of its kind to understand the intersection between cannabis consumption and opioid use. Therefore, the aim of this study was to evaluate the association between preoperative cannabis usage and consumption of opioids for postoperative analgesia. We hypothesized that cannabis usage may be associated with decreased usage of opioid analgesics in postoperative pain relief in patients undergoing spine surgery. Interestingly, our data shows that cannabis usage was associated with increased usage of opioids with inpatient daily opioids (MED/day) and post-discharge opioid amount (POST-MED).
As the number of cannabis users continues to grow in America, a growing area of interest is the effect of cannabis on perioperative pain management.10-13,17-25 Cannabis use in the United States is growing, and adults aged 45-59 are 9.4 times more likely to use cannabis than adults aged 60-98. 26 This statistic is supported by our data, as there was a lower mean age for cannabis use among the total patient population and the opioid naïve group.
As the prevalence of cannabis usage increases in middle-age and senior populations, orthopaedic healthcare providers should be mindful and take a complete history including cannabis use in these older patient demographics, as preoperative cannabis status may be a predictor of increased post-surgical pain medication requirements in these patients. This trend in cannabis use may also explain the statistical difference of the CCI of cannabis users, since CCI awards 1 point for age categories every 10 years over 50. It is reasonable to see a difference of about 1 point in CCI between cannabis users and non-users in our study population, who have a mean age that falls in range of 50-60 and 60-70, respectively.
Pain management in the acute postoperative setting remains a challenge in spine surgery. Adequate pain control is associated with improved outcomes, fewer adverse events, and earlier mobilization. 1 Conversely, poor pain control postoperatively has been associated with less patient satisfaction and increased economic burden due to prolonged hospitalization. 1 Moreover, poor pain control can lead to narcotic over-prescription and potential for dependence. A better understanding of a healthy approach to postoperative pain management needs is likely to lead to improved outcomes and patient satisfaction.
Our results are consistent with a recent study by Jamal et al, 27 in which recreational cannabis smokers required 23% higher dosage of morphine postoperatively following abdominal surgery. In a prospective randomized study, Jefferson et al 25 showed that cannabis users required significantly more opioid rescue analgesia in the immediate postoperative period in patients undergoing elective surgery. Similarly, Liu et al 12 evaluated the effects of cannabinoid use on pain in the perioperative period in patients undergoing major orthopaedic surgeries and found that cannabinoid users had higher pain scores both at rest and with movement when compared to non-cannabinoid users. However, their study did not demonstrate a difference in postoperative opioid requirements. Similar findings have been demonstrated in other studies showing no overall benefit of cannabis use.
It is unclear why preoperative cannabis usage may lead to increased pain or opioid requirements in the postoperative setting. There are a few theories regarding the modulation of cannabinoid type 1 and 2 receptors in cannabis users that may lead to receptor downregulation, internalization and desensitization after prolonged exposure.9,22 Additionally, opioid and cannabinoid receptors have been shown to be colocalized in the spinal cord, locus coeruleus, and striatum, which are involved in processing painful stimuli. 10 Analgesic effects of cannabinoids are partially mediated by delta and kappa opioid-receptors, which may explain the interaction between the two. 22 However, the exact pathoanatomic mechanism remains unclear and additional investigation is warranted. Another hypothesis is that cannabis users are self-medicating for increased pain pre-operatively compared to non-cannabis users.28,29 This is supported by a recent prospective population survey which found that patients believe that cannabis and cannabinoid products could be effective for pain management. 28 However, despite these expectations, results of clinical trials investigating the analgesic efficacy of cannabinoids have been largely disappointing, demonstrating only moderate-quality evidence for relief of chronic pain and non-superiority to placebo for treatment of acute pain.9,10,30
Although our study focused on effects of cannabis on pain management following spine surgery, previous literature has suggested cannabis usage has postoperative implications following major orthopaedic procedures such as mortality benefit. 20 As it stands, the existing literature is mixed, with some studies demonstrating adverse effects of cannabis usage: paranoia, anxiety, dry mouth, dizziness, abdominal pain, hyperemesis, codependence on other substances, cardiovascular complications, hypercoagulability, and surgical anesthetic complications, while others report positive effects such as improved quality of life, reduced pain, and even reduced costs.10,21,22 Although this was not the focus of this study, these are important considerations for clinicians when counseling patients on cannabis usage pre-operatively prior to spine surgery.
There are a number of limitations to this study, including being a retrospective case review at a single institution. Although postoperative pain regimens were standardized, different techniques of interbody fusion surgery across several surgeons were used within the study population. This may have contributed to some differences in opioid pain requirements post-operatively. Furthermore, while we could quantify the total number of opioid prescription medications given to patients post-discharge from the hospital, we were not able to account for whether the patients consumed all of the opioids prescribed. Cannabis usage was identified based on each patient’s electronic medical records, including diagnoses from previous care providers, and this may not accurately capture the entire cohort of cannabis users in the study population. It was not within the scope of the study design to contact patients to determine post-operative cannabis usage, although this may be a direction for future studies. Despite growing acceptance of cannabis usage, there remains a stigma for reporting drug use to physicians, as demonstrated in prior studies. 19 Differences between patients in the reason for consumption (medicinal vs recreational), type of cannabis product consumed, route of administration, quantity of consumption, cumulative exposure to cannabinoids, and timing of most recent usage preoperative, were not discriminable within the cannabis user cohort. Furthermore, we were unable to account for cannabis usage in the postoperative period. Although this may potentially confound the results of post-discharge opioid consumption, this would be unlikely to influence inpatient opioid consumption.
Despite these limitations, this study has considerable implications for optimizing postoperative pain management in spine patients. Pre-operative cannabis usage should be a consideration in managing postoperative pain in candidates for posterior lumbar interbody fusion surgery. As the prevalence of cannabis usage continues to grow, an increasing number of patients who present for posterior lumbar spine surgery may use cannabis preoperatively. It may be prudent to anticipate increased postoperative opioid medication needs in this group of patients. Additional research in the form of prospective studies may help further elucidate these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.