
Abstract
Study Design
Retrospective cohort study.
Objective
To assess the association between undergoing spine surgery in an ambulatory surgical center (ASC) vs a hospital outpatient department (HOPD) and (a) perioperative opioid prescription patterns and (b) prolonged opioid use.
Methods
Data from the Merative MarketScan Database included patients aged 18-64 who underwent single-level or multilevel anterior cervical discectomy and fusion (ACDF) or lumbar decompression between January 2017 and June 2021. Primary outcomes included receipt of a perioperative opioid prescription, perioperative oral morphine milligram equivalents (MMEs), and prolonged opioid use (defined as opioid prescription 91-180 days post-surgery). Secondary outcomes included the number of perioperative opioid prescriptions filled (single/multiple) and type of initial perioperative opioid filled (potent/weak). Analysis of prolonged opioid use was limited to opioid-naive patients. Propensity score matching (1 ASC to 3 HOPD cases) and logistic regression models were used for analysis.
Results
The study included 11,654 ACDF and 26,486 lumbar decompression patients. For ACDF, ASCs had higher odds of an initial potent opioid prescription (OR = 1.18, 95% CI 1.08-1.30, P < .001) and higher total adjusted mean MMEs (+21.14, 95% CI 3.08-39.20, P = .02). For lumbar decompression, ASCs had increased odds of an initial potent opioid (OR = 1.23, 95% CI 1.16-1.30, P < .001) but lower odds of multiple opioid prescriptions (OR = 0.90, 95% CI 0.85-0.96, P < .001). There was no significant association between the surgery setting and prolonged opioid use.
Conclusion
Differences in perioperative opioid prescribing were observed between ASCs and HOPDs, but there was no increase in prolonged opioid use in ASCs. Further research is needed to optimize postoperative pain management in different outpatient settings.
Keywords
Introduction
Opioids are commonly prescribed after spine surgery. However, perioperative opioid prescriptions related to spine surgery have been associated with prolonged opioid use. 1 The expansion of spine surgeries classified as outpatient, which often involves same-day discharge, provides decreased opportunities to manage pain in the hospital. 2 This shift in surgery setting may encourage the increased prescription of perioperative opioids to prevent unplanned postoperative health care utilization related to pain control and to prevent transitions to chronic postsurgical pain due to increased acute postoperative pain intensity.3,4
Importantly, outpatient surgery is offered to patients who meet specific inclusion criteria. Specifically, patients with higher American Society of Anesthesiologists Physical Status Classification System scores, significant comorbidities, or increased risk of postoperative complications may not be considered suitable for outpatient settings. 5 Additionally, factors such as limited social support or lack of adequate home recovery resources can further restrict eligibility for outpatient surgery. Outpatient surgery settings are also not homogeneous as spine surgery procedures can be performed in either ambulatory surgical centers (ASCs) or hospital outpatient departments (HOPDs). Care in ASCs is often less comprehensive and generally involves shorter facility stays. Moreover, significant cost savings have been reported for outpatient spine procedures performed at ASCs compared to HOPDs. 6 Additionally, Durand et al reported increased emergency department (ED) visits after outpatient spine surgery in an HOPD vs ASC, with postoperative pain being the most common reason for ED visits. 7 This suggests that setting-specific differences in perioperative care processes likely extend to pain management, including opioid prescribing.
Given the importance of appropriate opioid prescription practices combined with the continued expansion of spine surgery procedures performed at ASCs, we aimed to compare receipt of a perioperative opioid prescription and total perioperative oral morphine milligram equivalents (MMEs) between the ASC vs HOPD setting for two common spine surgery procedures, accounting for setting-related differences in patient case mix. We also examined the association between the specific outpatient surgery setting and prolonged opioid use in opioid-naive patients who filled a perioperative opioid prescription.
Methods
Study Design
This retrospective cohort study used data from the Merative MarketScan Commercial Claims and Encounters Database and included index spine procedures performed between January 1, 2017 and June 30, 2021 (cohort flowchart in Figure 1). To capture primary index procedures, we initially identified the first spine surgery (anterior cervical discectomy and fusion [ACDF], cervical disc arthroplasty [CDA], lumbar decompression, or lumbar fusion) per unique patient in 2017-2021 in any inpatient or outpatient claim. See Table A1 in Appendix for procedure codes. We then limited the cervical cohort to patients who underwent ACDF (Current Procedural Terminology [CPT] 22551) without a concurrent CDA, lumbar fusion, or lumbar decompression. The lumbar cohort included patients who underwent lumbar laminotomy/ microdiscectomy (CPT 63030) or lumbar laminectomy (CPT 63047) without a concurrent lumbar fusion, ACDF, or CDA. Procedures were limited to those performed in an ASC or HOPD in patients aged 18-64, and those that could not be classified as single-level or multilevel based on CPT codes were excluded. Index spine procedures associated with International Classification of Diseases, 10th Revision (ICD-10) diagnosis codes for neoplasms (C00-D49), intraspinal abscess (G06.1), osteomyelitis (M86.*), vertebral fracture with spinal cord injury (S14.*, S24.*, S34.*), or vertebral dislocation (S13.*, S23.*, S33.*) were also excluded. All patients required continuous enrollment in the insurance database for 12 months preoperatively and 6 months postoperatively as well as pharmacy enrollment in the year of surgery to ensure complete capture of comorbidities and outcomes. Patients with any additional surgical procedures within the next 6 months (defined as having a CPT code representing anesthesia) were excluded to increase confidence that postoperative opioid prescriptions were related to the index surgery (see Table A1 in Appendix). Additionally, those with a known history of opioid use disorder per ICD-10 diagnosis codes in the past 12 months (see Table A1 in Appendix) were excluded. Patients with a missing enrollee identifier or living outside of the four primary United States Census regions were also excluded. Cohort creation for anterior cervical discectomy and fusion and lumbar decompression patients.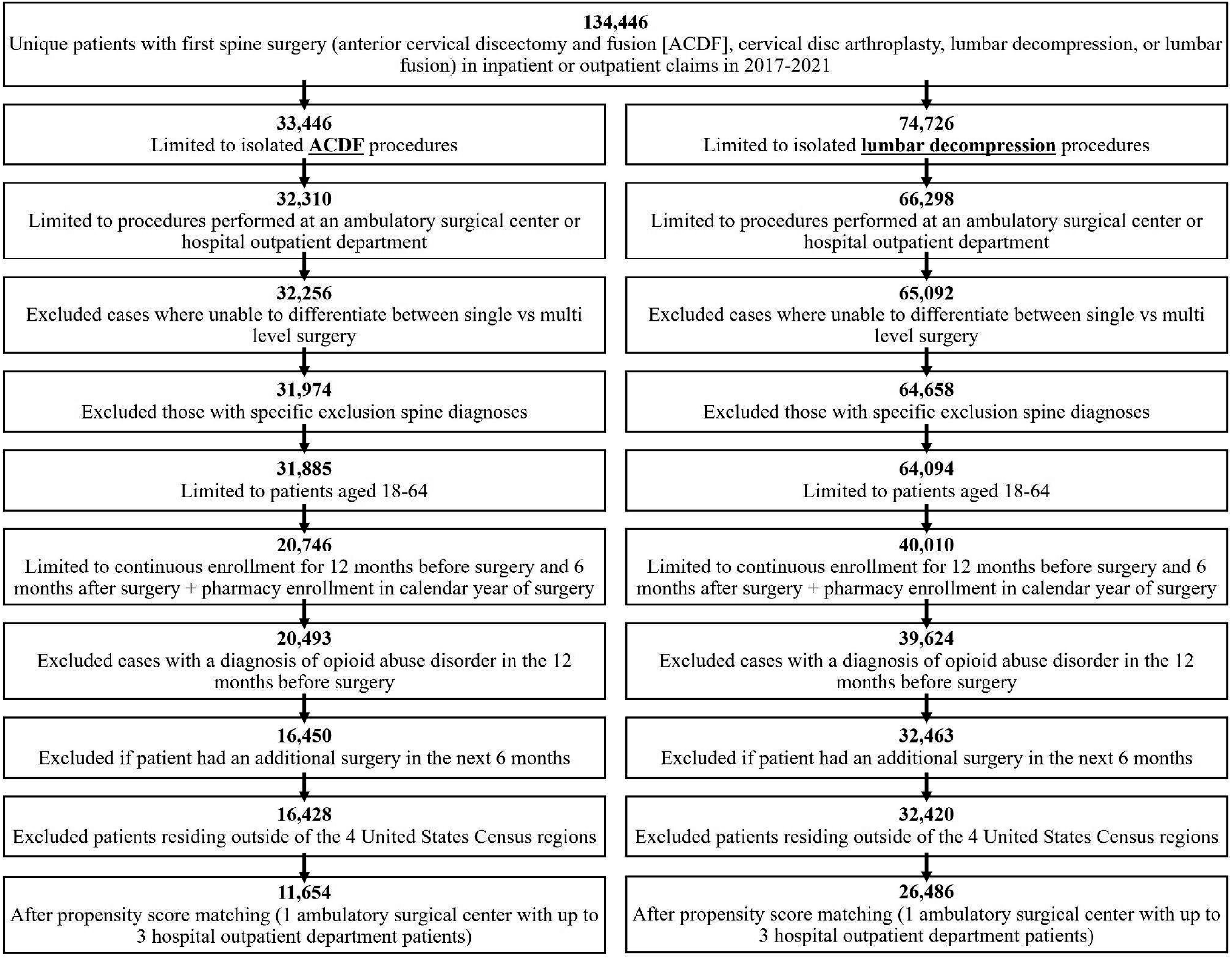
Outcomes and Other Variables of Interest
Primary outcomes of the study included (a) filling a perioperative opioid prescription (yes/no), (b) total MMEs filled during the perioperative period, and (c) prolonged opioid use. Aligned with previous studies on opioid use in elective surgery, the perioperative period was defined as from 30 days before surgery through 14 days after surgery, to capture prescriptions that may be prescribed and filled in preparation for postoperative pain management for an elective outpatient surgery.8-11 Prolonged opioid usage was defined as filling an opioid prescription between 91 days and 180 days following surgery. Codeine, transdermal fentanyl, hydrocodone, hydromorphone, morphine, oxycodone, oxymorphone, and tramadol were classified as opioids in this study, with the exception of opioids with brompheniramine, chlorpheniramine, pseudoephedrine, phenylephrine, and guaifenesin in the generic name since they are likely cough/cold preparations. 12 Prescriptions with zero or negative quantity or missing National Drug Code information were excluded. Perioperative MMEs were calculated by multiplying quantity and dose, summing across all opioid prescriptions filled during the perioperative period, and using standard conversions. 13 Perioperative MMEs were trimmed at the 95th percentile since extreme values likely reflect errors in the claims. Secondary outcomes included the number of perioperative opioid prescriptions filled (single/multiple) and type of the initial perioperative opioid filled (e.g., codeine) for patients filling an opioid prescription. The strength of the initial opioid was further characterized as potent (i.e., oxycodone, oxymorphone, hydromorphone, morphine, fentanyl) or weak (i.e., tramadol, codeine, hydrocodone) based on the World Health Organization Analgesic Ladder. 14 Additionally, to further contextualize pain management in the two settings, we identified the incidence of 30-day all-cause and pain-related ED visits since inadequate pain management may lead to unplanned health care utilization (see Table A1 in Appendix).
Demographic covariates of interest included age (in years), sex (male, female), geographic region (Northeast, Midwest, South, West), and primary insurance coverage (consumer-driven health plan, high-deductible health plan, health maintenance organization, preferred provider organization, other). Clinical comorbidities were defined based on ICD-10 diagnosis codes (see Table A1) from inpatient and outpatient claims in the prior 12 months. We calculated the Charlson-Deyo comorbidity index, 15 and identified the presence of tobacco use (yes/no), obesity (yes/no), other pain condition (defined as non-neck pain for ACDF and non-back pain for lumbar decompression; yes/no), mood or anxiety disorder (yes/no), and non-opioid substance use (yes/no). 16 Preoperative opioid history was calculated based on opioid prescriptions filled 31-365 days before surgery and classified as naive (no prescriptions filled), chronic (10+ prescriptions or 120+ day supply filled), or intermittent (<10 prescriptions and <120 day supply filled). Other clinical covariates included surgery year (2017, 2018, 2019, 2020, 2021) and single-level vs multilevel procedure (see CPT codes in Table A1). As proxies for procedural complexity, instrumentation was identified for ACDF procedures (yes/no; see CPT codes in Table A1); and lumbar decompression procedures were classified by whether a laminectomy was performed. We also identified whether non-opioid analgesic prescriptions (acetaminophen, celecoxib, nonsteroidal anti-inflammatory drugs) or gabapentinoid prescriptions (gabapentin, pregabalin) were filled in the perioperative period of 30 days before to 14 days after surgery.
Statistical Analysis
All statistical analyses were completed separately for the ACDF and lumbar decompression cohorts and performed in SAS version 9.4 (SAS Institute, Cary, NC). Demographic and clinical factors and outcomes were summarized using frequencies and percentages for categorical variables and medians and interquartile ranges for continuous variables. Given the large cohort sizes where P-values can easily approach statistical significance, standardized differences (STD) were used to compare demographic and clinical factors and outcomes between the surgery settings for each procedure type. A STD reflects the magnitude of imbalance in between-group proportions for a characteristic, and a STD >0.10 was used to reflect a meaningful between-group difference. 17
To reduce confounding related to a healthier case mix for procedures in an ASC vs HOPD, we used a caliper-propensity score without replacement matching technique to match 1 ASC patient with up to 3 HOPD patients. Given the ratio of ASC to HOPD patients, we used a one-to-many match to reduce loss of patients in the analysis. An exact match was used for single-level vs multilevel procedure status to minimize confounding related to procedural variation between the two settings. Additionally, we used a caliper of 0.10 to match on demographic and clinical variables that may predispose the individual to have surgery in one setting over the other. These variables included age, sex, geographic region, health insurance, individual Charlson-Deyo comorbidities, tobacco use, obesity, other pain conditions, mood or anxiety disorder, non-opioid substance use, preoperative opioid history, and surgery year. The variables used for matching were selected before analysis began based on clinical judgment of factors that may vary by surgery setting and availability of variables in the dataset. We examined the candidate variables for collinearity, which was not observed, before creating the propensity score. Between-setting comparisons of demographic and clinical factors were then repeated in the matched cohorts for each procedure type to assess success of matching.
Using the propensity score-matched cohorts, multivariable models examined the associations between undergoing surgery in an ASC (versus HOPD) and the outcomes. These models were further adjusted for the procedural complexity proxies (instrumentation for ACDF; laminectomy for lumbar decompression) and perioperative non-opioid analgesics and gabapentinoids to try to isolate the role of surgery setting. The outcomes of filling a perioperative opioid prescription (yes vs no) and 30-day ED visits were examined in all patients. The outcomes of filling multiple (2+ vs 1) perioperative opioid prescriptions, perioperative MMEs (trimmed at 95th percentile), and filling a potent (versus weak) opioid prescription were modeled only in those who filled a perioperative opioid prescription due to the nature of the variables. The models for prolonged opioid use were further restricted to opioid-naive patients who filled a perioperative opioid prescription to identify onset of new prolonged use. Additionally, prolonged opioid use was modeled with and without accounting for potential differences in perioperative opioids (MMEs, first opioid strength) to better understand the role of surgery setting. All categorical outcomes were modeled using binary logistic regression models. The continuous outcome of perioperative MMEs was modeled using a generalized linear model with a gamma distribution and log link and conversion of the estimates to adjusted mean differences (marginal means) on the data scale. Adjusted odds ratios (OR) or mean differences and 95% confidence intervals are reported for all regression models, with a two-tailed alpha of P < .05 to indicate statistical significance.
Results
Demographic and Clinical Characteristics of Patients Stratified by Surgery Setting for Cervical and Lumbar Procedures After Propensity Score Matching.
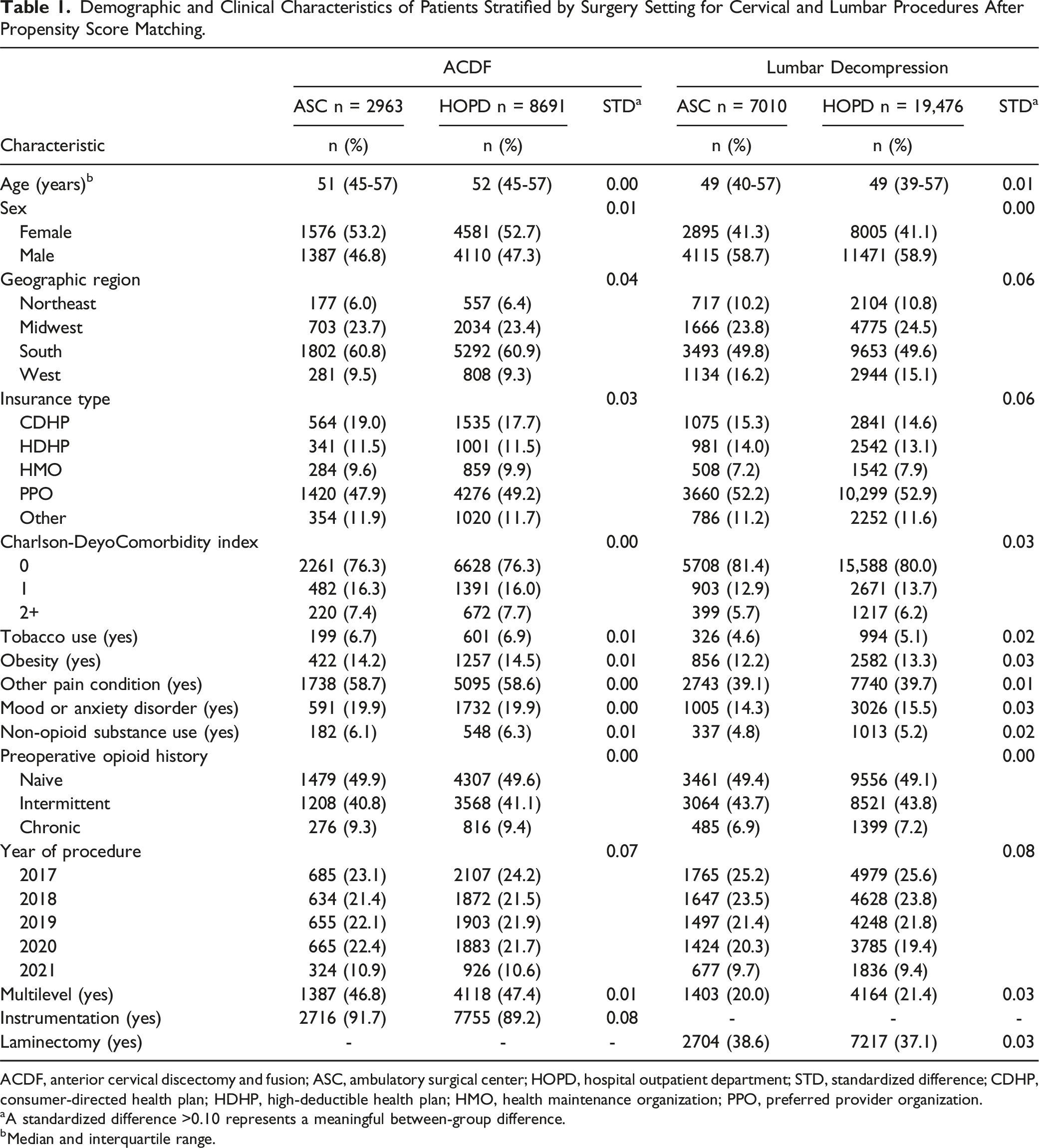
ACDF, anterior cervical discectomy and fusion; ASC, ambulatory surgical center; HOPD, hospital outpatient department; STD, standardized difference; CDHP, consumer-directed health plan; HDHP, high-deductible health plan; HMO, health maintenance organization; PPO, preferred provider organization.
aA standardized difference >0.10 represents a meaningful between-group difference.
bMedian and interquartile range.
Characteristics of Prescriptions Filled and Emergency Department Visits Stratified by Surgery Setting for Cervical and Lumbar Procedures after Propensity Score Matching.
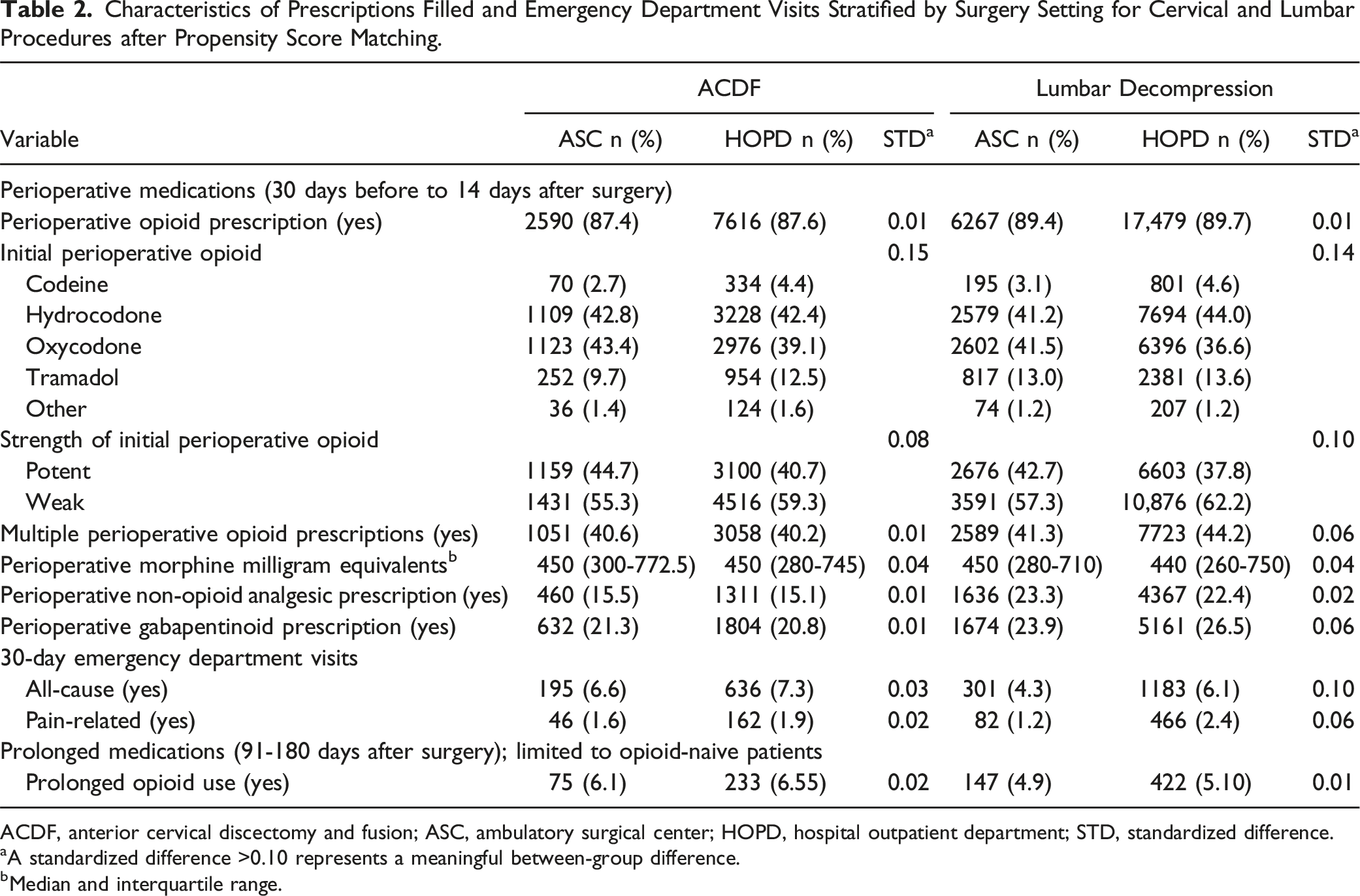
ACDF, anterior cervical discectomy and fusion; ASC, ambulatory surgical center; HOPD, hospital outpatient department; STD, standardized difference.
aA standardized difference >0.10 represents a meaningful between-group difference.
bMedian and interquartile range.
Associations Between Receiving Care in an ASC (Versus HOPD) and Opioid-Related Outcomes for Cervical and Lumbar Procedures. a
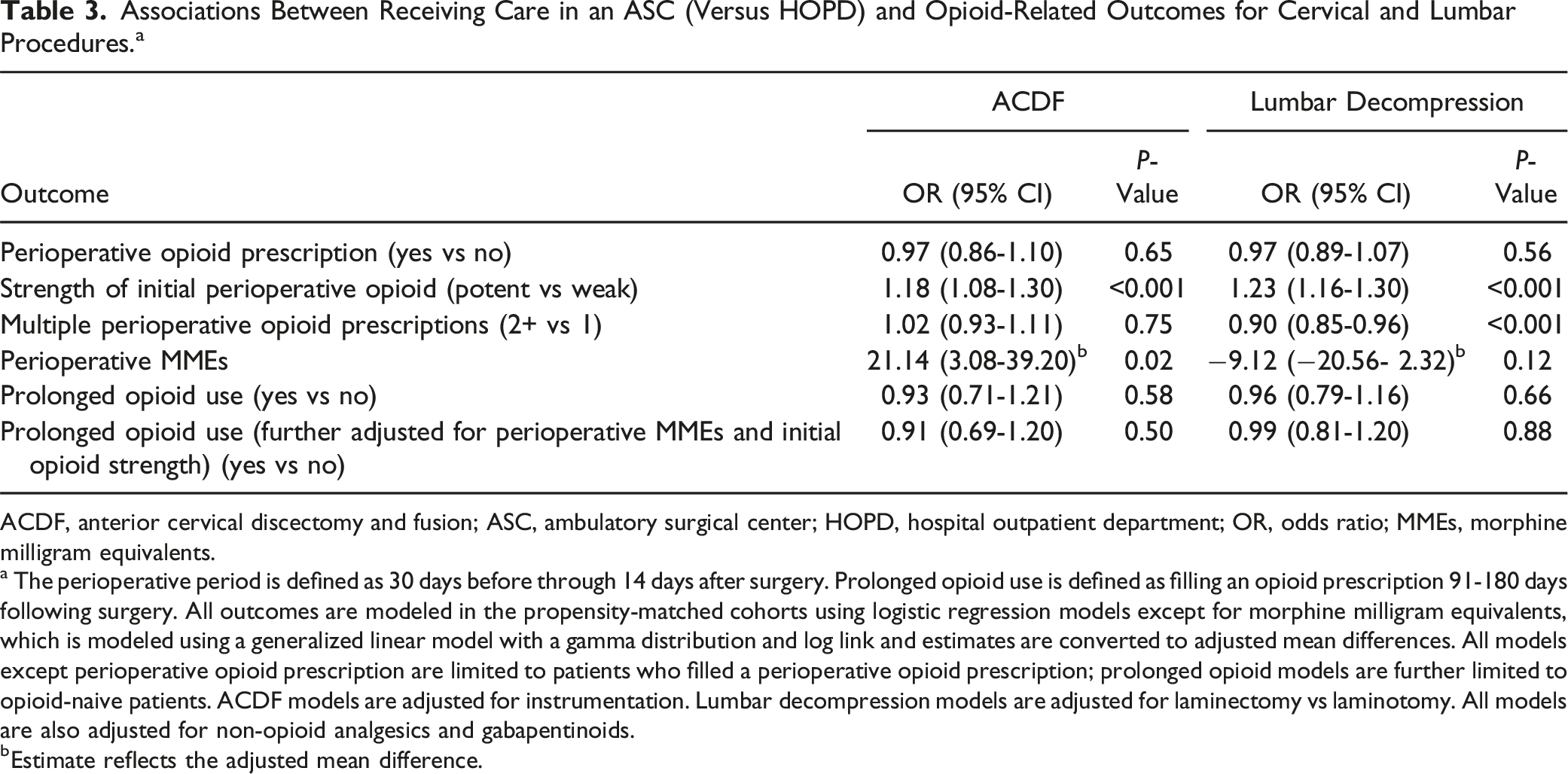
ACDF, anterior cervical discectomy and fusion; ASC, ambulatory surgical center; HOPD, hospital outpatient department; OR, odds ratio; MMEs, morphine milligram equivalents.
a The perioperative period is defined as 30 days before through 14 days after surgery. Prolonged opioid use is defined as filling an opioid prescription 91-180 days following surgery. All outcomes are modeled in the propensity-matched cohorts using logistic regression models except for morphine milligram equivalents, which is modeled using a generalized linear model with a gamma distribution and log link and estimates are converted to adjusted mean differences. All models except perioperative opioid prescription are limited to patients who filled a perioperative opioid prescription; prolonged opioid models are further limited to opioid-naive patients. ACDF models are adjusted for instrumentation. Lumbar decompression models are adjusted for laminectomy vs laminotomy. All models are also adjusted for non-opioid analgesics and gabapentinoids.
bEstimate reflects the adjusted mean difference.
For the secondary outcome of 30-day ED visits, there was no association between surgery setting and all-cause visits (OR = 0.89, 95% CI 0.76-1.05, P = .18) or pain-related visits (OR = 0.84, 95% CI 0.60-1.17, P = .29) for ACDF. For lumbar decompression, undergoing surgery at an ASC vs HOPD was associated with lower incidence of both all-cause (OR = 0.69, 95% CI 0.61-0.79, P < .001) and pain-related 30-day ED visits (OR = 0.48, 95% CI 0.38-0.61, P < .001).
Discussion
This study aimed to examine the associations between the specific outpatient surgery setting and perioperative and prolonged opioid patterns for two commonly performed spine surgeries. It extends the current literature on opioid use after spine surgery by looking specifically at differences associated with specific outpatient surgery settings. There were no associations between surgery setting and filling a perioperative opioid prescription. However, across both ACDF and lumbar decompression procedures, undergoing surgery in an ASC was associated with higher likelihood of an initial potent opioid prescription even after accounting for between-setting differences in patient case mix through matching and adjusting for other perioperative non-opioid medications. For ACDF, surgery in an ASC was also associated with higher total perioperative MMEs but no differences in multiple opioid prescriptions while lumbar decompression in an ASC was associated with decreased likelihood of filling multiple opioid prescriptions but no differences in total MMEs. Surgery setting was not associated with prolonged opioid use for either spine procedure in opioid-naive patients.
Recent trends indicate a significant increase in ambulatory services for spine surgeries within ASCs and HOPDs over the past decade. 18 ASCs specifically have shown higher increase in utilization compared to HOPDs throughout the years for orthopaedic surgeries. 19 One key factor contributing to the growing preference for ASCs over HOPDs is reports of cost-effectiveness of the former. 6 However, some studies highlight limited costs savings for ASCs, 20 and there is a notable absence of standardized criteria in the literature for patient eligibility for spine surgeries at ASCs, which could challenge safety and quality. 21 In the current study, those with a higher general comorbidity burden as well as specific comorbidities (e.g., tobacco use, obesity), which could contribute to increased complications risks in spine surgery,22-27 were less likely to undergo surgery in an ASC. However, interestingly, a history of chronic or intermittent preoperative opioid use was not associated with undergoing surgery in an ASC vs HOPD despite the association of this factor with poorer outcomes following spine surgery. 28 Regional differences in ASC utilization were also noted, with the lowest proportion in the Northeast, potentially due to the disparate geographic availability of ASCs (e.g., 13.6% in the Northeast vs 39.8% in the South). 29 These differences in patient case mix between the two outpatient surgery settings highlight the importance of accounting for these characteristics to understand contributions of setting to practice patterns. We, therefore, used a matching approach to account for patient selection differences between HOPDs and ASCs and improve interpretation of our findings.
Among various specialties, orthopedic surgery patients were most likely to return to the ED for pain management, underscoring the critical role of effective postoperative pain control to reduce unplanned health care utilization. 30 Simultaneously, spine surgery has a high rate of prolonged opioid use.31-33 For example, Goyal et al found that the incidence of persistent opioid use was 30% for posterior lumbar fusion and 19% for lumbar decompression and discectomy among all patients. 31 Existing literature has examined patient characteristics linked to prolonged opioid use following spine surgery to identify those at risk following spine surgery and prevent this common complication.33-35 Dunn et al found that preoperative opioid use and pain scores were associated with chronic opioid usage after major spine surgery. 34 A systematic review by Mohan et al highlighted several baseline risk factors associated with prolonged opioid use following spine surgery, including preoperative opioid use, depression, anxiety, drug abuse, female gender, fibromyalgia, lower back pain, tobacco use, and chronic pulmonary disease. 36 Specifically regarding surgery setting, studies have highlighted undergoing spine surgery in an inpatient (versus outpatient) setting as a predictor of prolonged opioid use.9,32 Additionally, perioperative prescribing, particularly MMEs, is a known risk factor for prolonged opioid use. 37 It is, therefore, essential to achieve a balance between adequate perioperative pain relief and the risk of long-term opioid dependency.
Comparisons of perioperative opioid patterns within different outpatient settings, specifically between ASCs and HOPDs, have been underexplored. In our study, there was no significant adjusted association between surgery setting and filling a perioperative opioid prescription for either ACDF or lumbar decompression. However, among patients filling prescriptions, characteristics of those prescriptions differed by setting. Patients at ASCs were more likely to receive an initial prescription for a potent opioid and were also more likely to have higher total perioperative MMEs when undergoing ACDF. In contrast, for lumbar decompression in an ASC, patients had lower odds of filling multiple opioid prescriptions but were more likely to be initially prescribed a potential opioid. Patient expectations for pain management may contribute to the tendency for prescribing more potent opioids to meet anticipated postoperative comfort levels. Additionally, differences in discharge protocols between ASCs and HOPDs can play a role, with ASCs possibly favoring stronger opioids due to their limited postoperative oversight of patients. Finally, because patients discharged from ASCs often need to manage pain independently, there may be increased use of potent opioids to address the reduced access to immediate follow-up care and pain management resources. Of note, despite the significant associations observed, the estimates were small (e.g., OR <2.0), and clinical meaningfulness of these associations should be examined in future work.
Regarding adequacy of pain management, one study identified increased 90-day ED visits after spine surgery, often due to postoperative pain, in patients who underwent ACDF, laminectomy, or microdiscectomy at HOPDs vs ASCs. 6 While their result aligns with our current finding of lower 30-day ED visits for lumbar decompression in ASC vs HOPD, we did not identify an association between surgery setting and ED visits after ACDF. However, the general pattern of findings across both studies suggests comparable to decreased ED visits for patients undergoing outpatient spine surgery in an ASC vs HOPD, which suggests adequate perioperative pain management in ASCs, despite shorter time frames in the facility.
Additionally, despite differences in perioperative opioid prescribing, including increased MMEs for patients undergoing ACDF in an ASC vs HOPD, we observed no significant difference in prolonged opioid use between the surgery settings for opioid-naive patients undergoing either ACDF or lumbar decompression. This finding contrasts with the Waterman et al study of a 2012-2017 mixed orthopaedic population including lumbar fusion that identified the lowest proportion of persistent opioid use in those undergoing surgery in an ASC (18%) compared to HOPD (24%) or inpatient (26%). 38 The current findings may differ based on changes in practice patterns over time.
This study is not without limitations. The retrospective nature of the data only allows us to identify opioids based on prescriptions filled, which may not fully represent either prescriptions written or opioids consumed. The dataset lacks granularity regarding the surgical approach (e.g., open, tubular, or endoscopic), which likely influences opioid prescribing patterns, particularly in the early postoperative period. We were also unable to account for potential differences in opioids given pre-discharge, which could differ between the two surgery settings. While we adjusted for prescription non-opioid analgesics, we were unable to comprehensively account for different patterns of these medications that can influence opioid prescribing and use since many of these medications are non-prescription. Additionally, the reliance on a commercial claims database limits the generalizability of the findings, as the included patients may not represent the entire spectrum of patients undergoing spine surgery, especially those who are uninsured or on different types of insurance plans. The study’s focus on a specific age group (18-64 years) further narrows generalizability to older adults who may have more multimorbidity. Furthermore, although the use of propensity score matching improved comparability of patients between the two surgery settings, there may have been undercoding or miscoding of diagnoses representing comorbidities in the claims, which could affect the accuracy of our findings. We were also unable to account for other potentially relevant factors such as patient preferences and surgeon expertise. These limitations warrant careful interpretation of the results. Future research should prioritize the comparison of pain scores to more accurately assess the appropriateness and effectiveness of pain management in each surgical setting. Additionally, future research should explore patient preferences and the role of multidisciplinary approaches to pain management in various surgical settings to provide a more comprehensive understanding of how prescribing practices may be optimized to align with patient needs and promote effective pain management.
This analysis of opioid patterns by specific outpatient surgery setting identified no differences in the overall proportion of patients filling a perioperative opioid prescription but some differences in perioperative opioid characteristics. Our data suggest that perioperative opioid prescribing patterns for spine surgery in ASCs (e.g., with an initial potent opioid) may be addressing pain effectively despite short facility stays, without increasing long-term opioid dependency risks. This investigation further highlights the role of surgical setting in contributing to perioperative pain management. Further research is needed to identify the most appropriate care patterns within and across surgery settings to effectively and safely manage postoperative pain following outpatient spine surgery.
Supplemental Material
Supplemental Material - Opioid Use Following Spine Surgery in Ambulatory Surgical Centers Versus Hospital Outpatient Departments
Supplemental Material for Opioid Use Following Spine Surgery in Ambulatory Surgical Centers Versus Hospital Outpatient Departments by Rodnell Busigó Torres, Husni Alasadi, Akiro H. Duey, Junho Song, Jashvant Poeran, Brocha Z. Stern, and Saad B. Chaudhary in Global Spine Journal.
Footnotes
Acknowledgments
We would like to express our gratitude to Hanish Kodali, MBBS, MPH for his assistance with the initial cohort creation and data analysis. Although his contributions did not fulfill the criteria for full authorship, his support was invaluable to the early stages of our project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported in part through the computational resources and staff expertise provided by Scientific Computing and Data at the Icahn School of Medicine at Mount Sinai and supported by the Clinical and Translational Science Awards (CTSA) grant UL1TR004419 from the National Center for Advancing Translational Sciences.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.