
Abstract
Study Design
Retrospective validation protocol.
Objective
The International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI) is the most comprehensive tool for classifying spinal cord injuries (SCI), but it is not adapted for the evaluation of trauma patients. The objective is to develop and validate a streamlined tool, the Montreal Acute Classification of Spinal Cord Injury (MAC-SCI) that can be integrated in the evaluation of trauma patients to detect and characterize traumatic SCI (tSCI).
Methods
The completion rate of the ISCNSCI during initial evaluation after tSCI was estimated at a Level-1 trauma center specialized in SCI care. Using a modified Delphi technique, we designed the MAC-SCI, a new tool to detect and characterize the severity grade and level of SCI in the polytrauma patient. A cohort consisting of 35 consecutive tSCI patients with complete ISNCSCI documentation was used to validate the MAC-SCI. The severity grade and neurological level of injury (NLI) were assessed using the MAC-SCI, and compared to those obtained with the ISNCSCI.
Results
Only 33% of 148 patients admitted after a tSCI had a complete ISNCSCI performed at initial presentation. The MAC-SCI retains 53 of the 134 elements from the ISNCSCI. There was a 100% concordance in severity grade between the MAC-SCI and ISNCSCI. The NLI were within 2 levels between the MAC-SCI and ISNCSI for 100% of patients.
Conclusion
The MAC-SCI is a streamlined tool that accurately detects and characterizes tSCI in the acute trauma setting. It could be implemented in trauma protocols to guide the management of SCI patients.
Level of Evidence
Level III Diagnostic criteria.
• Prompt detection of spinal cord injury is essential in trauma patients because it can be associated with acute respiratory failure and neurogenic shock. The International Standards for Neurological Classification of Spinal Cord Injury worksheet (ISNCSCI) is the most widely used and comprehensive classification of SCI patients but is not adapted to trauma assessment protocol.
• This study validated a quick, simple and accurate neurological examination tool to detect and characterize spinal cord injury in the acute trauma patient: the Montreal Acute Classification of Spinal Cord Injury (MAC-SCI).
• The MAC-SCI should be used in trauma assessment protocols to increase adherence to a standardized neurological examination, enhance reproducibility between tests and observers, and ultimately better patient care in the acute management of traumatic spinal cord injuries.What This Paper Adds
What is Already Known on This Topic
What This Study Adds
How This Study Might Affect Research, Practice or Policy
Introduction
Spinal cord injury (SCI) is a global health issue and is most often secondary to trauma. It has an estimated prevalence between 252 000 and 373 000 people in the United States 1 where approximately 17 900 new patients are admitted annually to emergency departments with an acute traumatic SCI (tSCI). 2 Falls and motor vehicle accidents are now the leading cause of tSCI 3 such that a large proportion of tSCI patients present with polytrauma in the emergency departments. Prompt detection of a SCI is essential because it can be associated with acute respiratory failure and neurogenic shock, and requires tight hemodynamic support and early spinal surgery to promote recovery. 4
The context of polytrauma necessitates standardized assessment of all injuries. The Advanced Trauma Life Support (ATLS) is a well-known systematic protocol aiming on managing life threatening issues in an orderly fashion. 5 The primary survey consists of a rapid 5-step examination known as the ABCDE (Airway, Breathing, Circulation, Disability and Exposure) to identify life-threatening injuries. The Disability step refers to the following concept: “A rapid neurologic evaluation establishes the patient’s level of consciousness and pupillary size and reaction; identifies the presence of lateralizing signs; and determines spinal cord injury level if present.” 5 Once the patient has been stabilized during the primary survey, a more exhaustive evaluation can begin using the secondary survey. It consists of a system by system evaluation to identify injuries missed during the primary survey.
However, the ATLS remains elusive as to how the SCI level should be determined. The ATLS suggests that a comprehensive neurological examination of motor and sensory functions be performed, and mentions that the International Standards for Neurological Classification of Spinal Cord Injury worksheet (ISNCSCI)6,7 can be used to document the patient’s neurological examination. Unfortunately, the ISNCSCI has not been developed specifically for the early acute management of trauma patients, and it is well known that in an acute trauma setting, full completion of the ISNCSCI remains difficult. Data from the Rick Hansen Spinal Cord Injury Registry (RHSCIR) reveal that completion rates of the ISNCSCI exam within 7 days of admission for an acute tSCI are only 12% in Canadian trauma centers specialized in acute SCI care. 8 Many barriers can explain these low completion rates. For an experienced user, a complete ISNCSCI examination can take up to 45 minutes with a fully awaken and collaborative patient, 9 which is time consuming for a trauma situation. Furthermore, potential patient’s intrinsic barriers include associated injuries, closed head injury, intoxication, intubation, pain, sedation and language barriers. 10 Extrinsic barriers include the unfavorable environment in the trauma bay and the limited time for the neurological evaluation between life-saving interventions and examinations. These multiple barriers underscore the limitations of the ISNCSCI for use during the acute management of trauma patients.
To overcome these barriers, we have developed a new neurological assessment tool specifically adapted to the initial evaluation of trauma patients to detect and characterize SCI. While being applicable in the acute trauma setting, the Montreal Acute Classification of Spinal Cord Injury (MAC-SCI) includes a subset of the elements of the ISNCSCI documentation, thus preserving basic principles of the ISNCSCI such as the assessment of the severity grade and neurological level of the injury (NLI). Through this study, we will assess the ability of the MAC-SCI to determine the severity grade and NLI, in comparison with the ISNCSCI exam.
Methods
This retrospective study was reviewed and approved by our local ethics committee (Ethics board “de la recherche CIUSSS du Nord-de-l'Île-de-Montréal”). The approval number is 2022-2446. and all participants gave their written consent.
Co-Design of MAC-SCI
Completion of ISNCSCI Exam in Acute Trauma Setting
We reviewed the medical charts of all patients admitted for a tSCI between June 1 2018, and September 30 2021, to retrieve the ISNCSCI documentation performed during the initial trauma assessment. The ISNCSCI documentation was implemented as a standard clinical evaluation tool in our electronic medical chart system June 1 2018. The completion rate of ISCNSCI documentation (complete vs incomplete) was evaluated, as well as the completion rate of each of the 134 elements.
Modified Delphi Method
Using a modified Delphi method, 11 we presented the completion rates for the ISNCSCI exams to 2 orthopedic surgeons specialized in spine surgery, 1 orthopedic surgery resident at the PGY-3 level, 2 physical and rehabilitation medicine physicians specialized in spinal cord injury management and 1 medical student. Based on these findings and on their clinical experience with the evaluation and management of SCI, these clinicians were asked to propose a simplified tool to detect and characterize SCI using any element of the ISNCSCI that they considered as relevant in an acute trauma setting. The selected elements were collected for each clinicians on an ISNCSCI worksheet and combined within a single spreadsheet. An ISNCSCI sheet including only the dermatomes and myotomes selected by the majority of the clinicians was presented to all the clinicians for a second iteration during which a consensus was reached on which elements to include in the MAC-SCI.
The MAC-SCI: Montreal Acute Classification of Spinal Cord Injury
The MAC-SCI includes a subset of 53 elements taken from the ISNCSCI (Figure 1): C2 to C4 and T2 to L1 dermatomes for light touch, C5 to T1 and L2 to S1 myotomes as well as the information from the rectal examination: voluntary anal contraction (VAC), superficial anal sensation (SAS) and deep anal sensation (DAP). Similar to VAC and DAP, assessment of SAS of light touch at S4-5 using the MAC-SCI is scored as present or absent, without consideration of laterality and magnitude (i.e. it is considered as present if any sensation is preserved on 1 or both sides). In case any myotome is non-testable in the extremities (e.g. limb fracture, associated injury, etc.) or if the patient complains of exclusively sensitive symptoms, the corresponding dermatome for light touch (from C5 to T1 and L2 to S1) is assessed and a corresponding comment can be added in the examination barriers box on the MAC-SCI form. Assessment of pin prick sensation is not performed in the MAC-SCI. Montreal acute classification of spinal cord injury (MAC-SCI).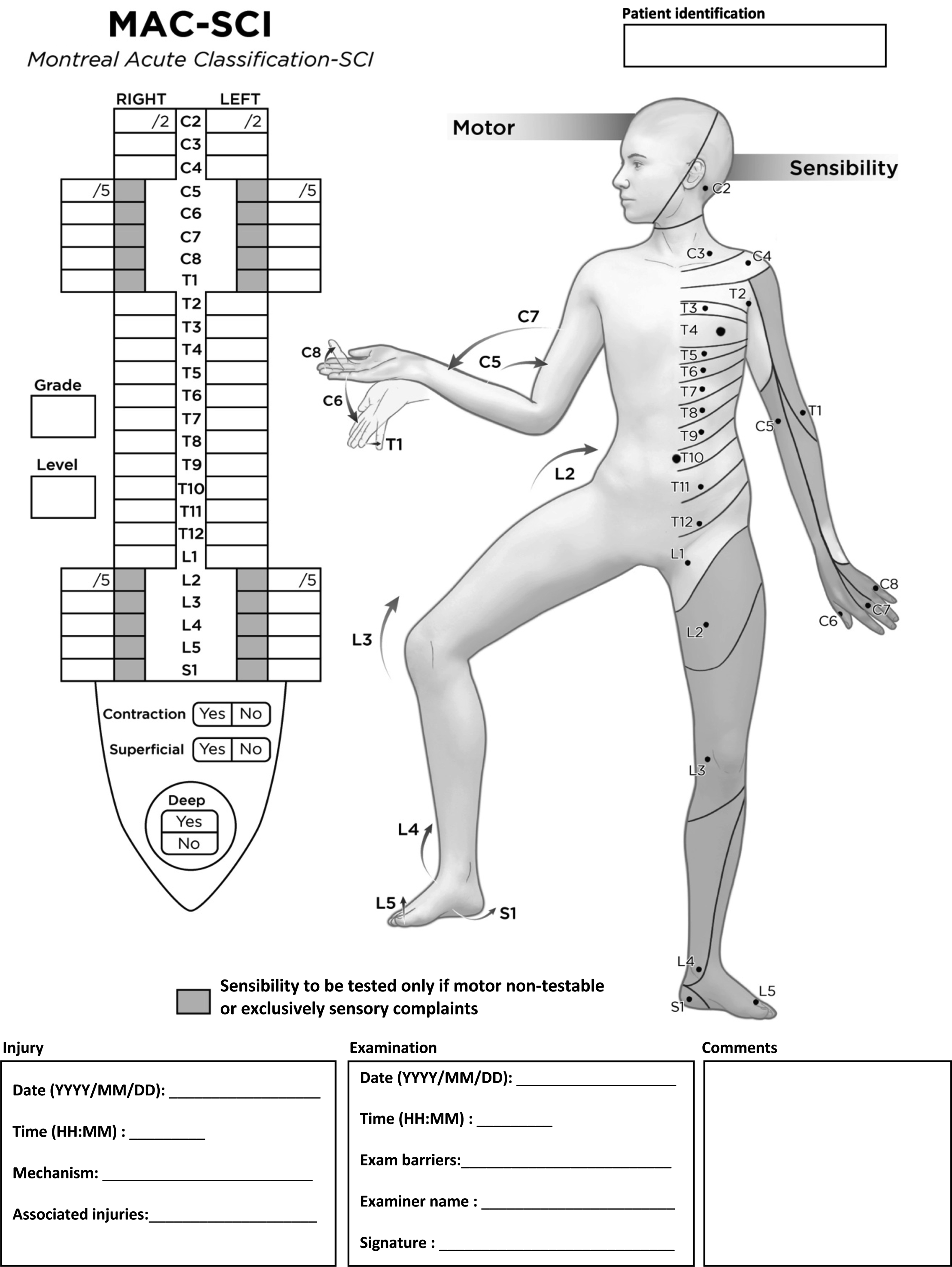
Within the MAC-SCI, dermatomes are graded on a scale from zero to 2. Zero for no sensation of light touch, 1 for diminished or altered sensation, and 2 for normal sensation. Myotomes are graded according to the Medical Research Council Muscle Scale 12 where zero is no contraction, 1 is contraction without movement, 2 is movement with gravity eliminated, 3 is full range of motion against gravity, 4 is full range of motion with resistance and 5 is normal resisted movement. Upper extremity myotomes from C5 to T1 are as follows: C5 elbow flexion, C6 wrist extension, C7 elbow extension, C8, fingers flexion and T1 fingers abduction. Lower extremity myotomes from L2 to S1 are: L2 hip flexion, L3 knee extension, L4 ankle dorsiflexion, L5 hallux extension and S1 ankle plantarflexion. MAC-SCI’s simplified rectal examination consists of superficial anal sensation, deep anal sensation and voluntary anal contraction.
The neurological level of injury (NLI) using the MAC-SCI is defined as the most distal segment of the spinal cord with normal sensory and motor function allowing full range of motion against gravity on both sides of the body (motor grade of 3 or more), provided that all proximal levels present intact motor and sensory function (motor grade of 5 and sensory function of 2).
Severity grade of the MAC-SCI follows the same principles of the American Spinal Injury Association Impairment Scale (AIS). If there is no motor function or preserved sensation in the rectal examination (no VAC, no SAS and no DAP) the severity grade is classified as A (complete injury). If there is preserved DAP or SAS but no VAC the severity grade is classified as B (sensory incomplete). If the is VAC, the severity grade is classified as C (motor incomplete) if there is less than 50% of the myotomes distal to the NLI that have a motor grade of 3 or more, or classified as D (motor incomplete) if there is 50% or more of the myotomes distal to the NLI that have a motor grade of 3 or more. An additional consideration is if there is motor preservation more than 3 levels distal to a motor level, the patient is now considered motor incomplete C if there is less than 50% of the myotomes distal to the NLI that have a motor grade of 3 or more, or D if there is 50% or more of the myotomes distal to the NLI that have a motor grade of 3 or more. The motor level is defined as the most distal myotome that has a motor grade of 3 or more, provided that all proximal levels present intact motor function (motor grade of 5). The motor level can be different on the right and left side.
Validation of MAC-SCI
Study Design
A retrospective analysis was carried out on a validation cohort of tSCI patients who had a complete ISNCSCI exam performed during the trauma assessment and ATLS at our Level-1 trauma center specialized in SCI care. These patients were identified from our electronic database of SCI patients admitted between June 1 2018, and September 30 2021. An estimated sample size of 35 was required to detect a 10% disagreement rate between the ISNCSCI and the MAC-SCI with a power of 80% and a level of significance of .05. 13
Validation Cohort
Baseline Characteristics of the Validation Cohort.
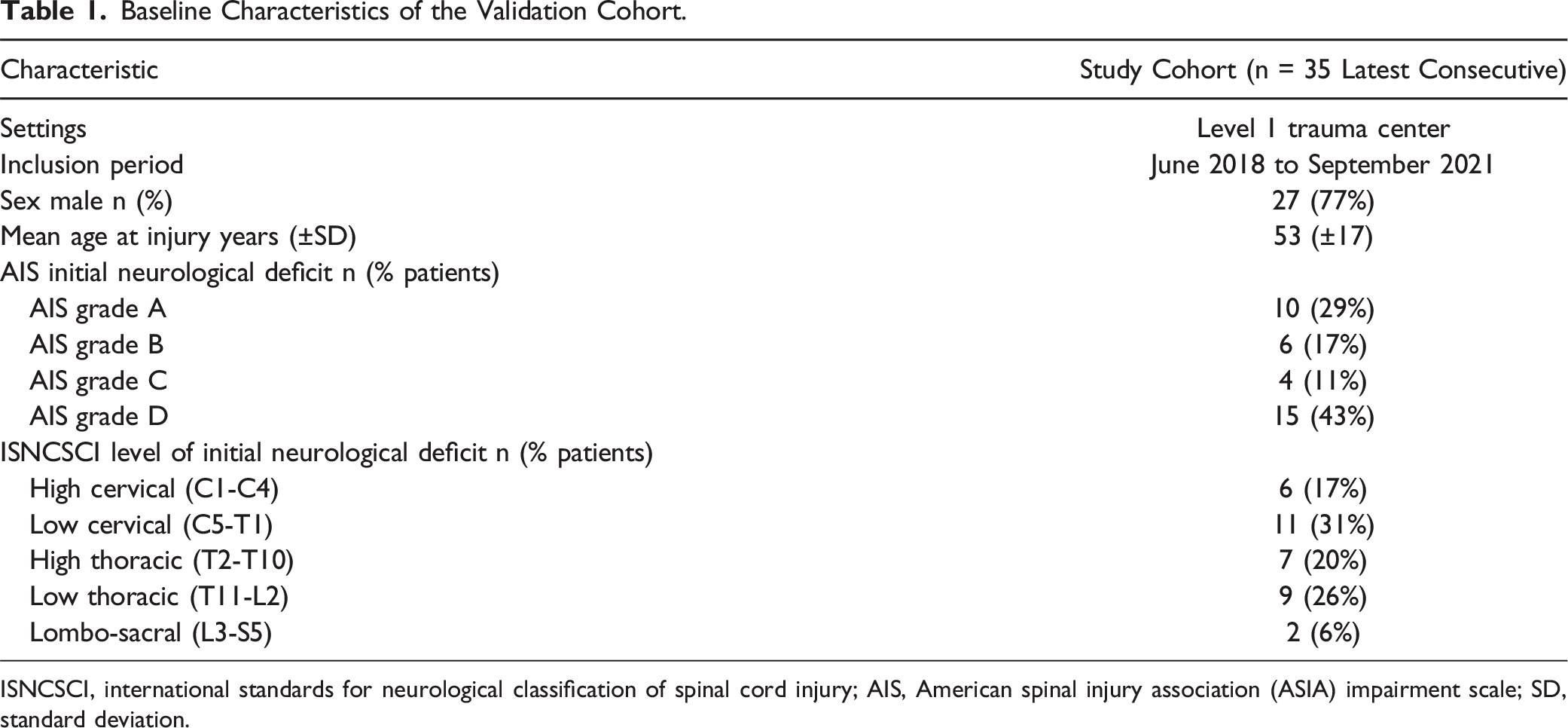
ISNCSCI, international standards for neurological classification of spinal cord injury; AIS, American spinal injury association (ASIA) impairment scale; SD, standard deviation.
Data Collection and Validation
We extracted the MAC-SCI from the ISNCSCI performed during the initial trauma assessment for all 35 patients of the validation cohort, and transferred the MAC-SCI on a spreadsheet. Two independent assessors (RPR and AD) determined the severity grade and NLI based exclusively on the information included in the MAC-SCI. The AIS grade and NLI were subsequently obtained from the complete ISNCSCI using the Version 2.0 (2019 updates) ISNCSCI algorithm. 14
Main Outcomes
The first main outcome was the ability of the MAC-SCI to detect and grade the severity of the SCI. This was determined by the concordance between the severity grade derived from the MAC-SCI and the AIS grade derived from the ISNCSCI. Another main outcome was the ability of the MAC-SCI to localize the SCI within 1 or 2 levels of the NLI derived from the ISNCSCI.
Statistical Analysis
The proportion of the concordance in the assessment of the severity grade and NLI between the MAC-SCI and ISNCSCI was calculated. Secondarily, the ability of the MAC-SCI to discriminate between cervical (C0 to C7) vs thoracic (T1 to T9) vs thoraco-lumbar (T10 to L2) vs lumbo-sacral (L3 to S5) injuries was also determined, in comparison with the ISNCSCI.
Results
Completion of ISNCSCI Exam in Acute Trauma Setting
From June 1 2018 to September 30 2021, 49 of 148 spinal cord injured patients had complete ISNCSCI documentation at the initial trauma evaluation, resulting in a completion rate of 33%. Figure 2 presents the completion rates for each element of the ISNCSCI. Completeness of ISNCSCI and each individual element at admission with retained dermatomes and myotomes for the MAC-SCI.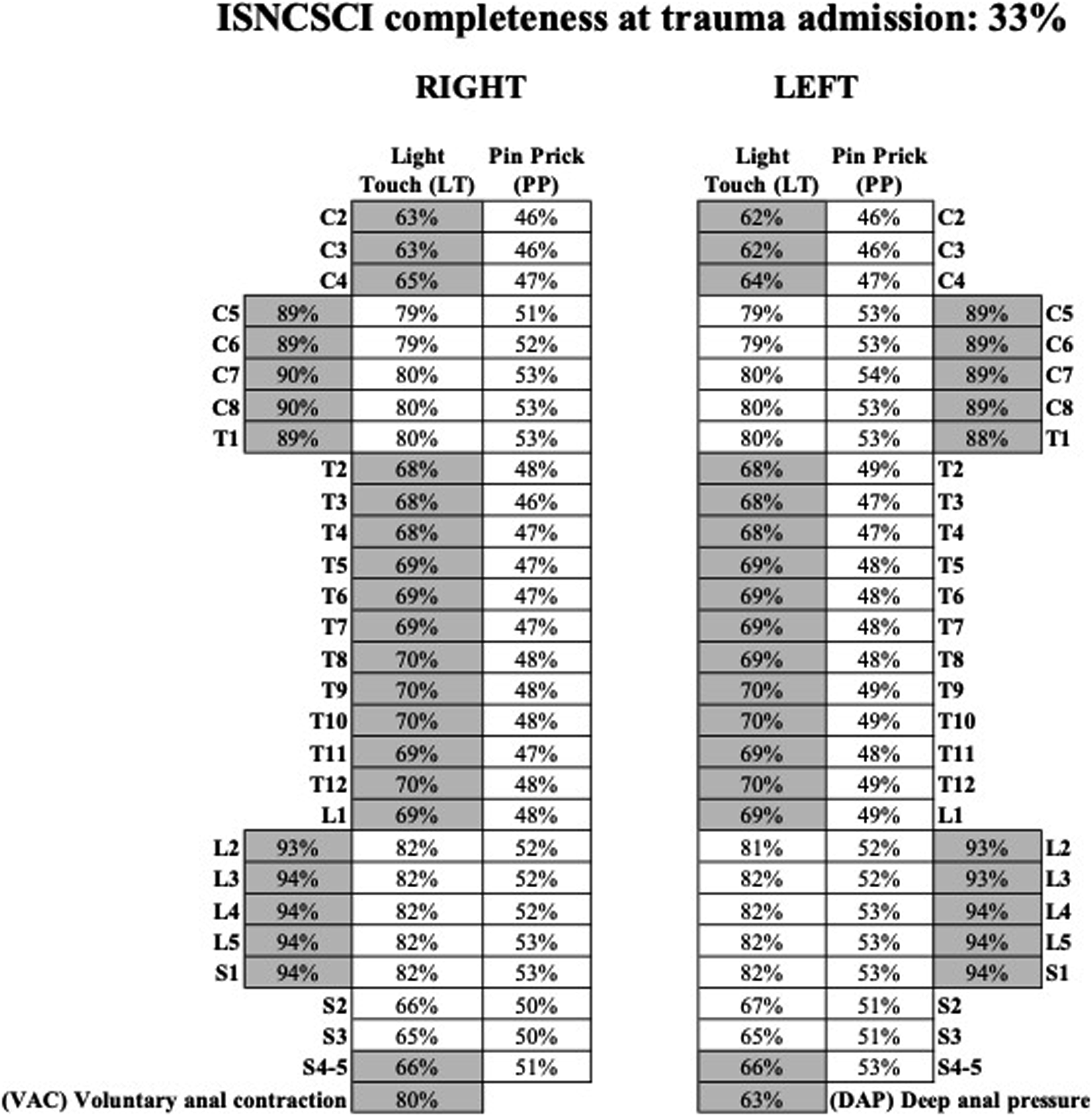
Validation of the MAC-SCI
MAC-SCI Validation Results.

MAC-SCI, Montreal acute classification of spinal cord injury; ISNCSCI, international standards for neurological classification of spinal cord injury; AIS, American spinal injury association (ASIA) impairment scale.
Discussion
The difficulty for performing a full ISNCSCI exam during the initial evaluation of trauma patients led to the development of the MAC-SCI, a streamlined neurological examination tool specifically dedicated to acute trauma patients. Full completion of the ISNCSCI at our Level-1 trauma center specialized in SCI care was only 33% during initial trauma assessment, paralleling the low completion rates observed in other trauma centers specialized in SCI care. 8 We have also observed that for all levels of the upper and lower extremities, myotome assessment was more likely to be completed, followed by light touch and pin prick assessment. For other levels, light touch assessment was systematically more likely to be completed than pin prick assessment. Considering that this behavior is also generalized among other trauma centers specialized in SCI care, 8 our participants of the Delphi process have prioritized myotome assessment over dermatomal assessment in the extremities, and light touch over pin prick assessment for other levels in the MAC-SCI, in order to facilitate clinical translation in the acute trauma setting.
The MAC-SCI was 100% accurate in determining the completeness of the SCI in terms of severity grade, when compared to the ISNCSCI. No spinal cord injuries were missed with the MAC-SCI. With the accuracy of 100% for locating the NLI within 2 levels of that obtained with the ISNCSCI, the MAC-SCI was also effective in localizing the level of the SCI. More specifically, the MAC-SCI was 100% accurate to discriminate between cervical vs thoracic vs thoraco-lumbar vs lumbo-sacral SCI, which are landmarks often used to guide the investigation and early management of SCI (levels for imaging, intubation for impending ventilatory failure and procedures for spinal immobilization).
The MAC-SCI was able to detect and characterize SCI with only 1 neurologic modality (motor or sensory function) per neurologic level, which results in 60% fewer elements to assess than the ISNCSCI. By retaining only the most significant elements of the original ISNCSCI, the MAC-SCI may overcome multiple barriers preventing a complete ISNCSCI examination in an emergent trauma setting. In particular, the MAC-SCI inherently requires less time to perform, and it is expected that both patients and clinicians will be more motivated to complete the neurological assessment using this new tool. The MAC-SCI could be particularly useful when additional emergent interventions are required or when a patient’s alertness is limited. The flexibility to use the dermatome assessment of light touch for the extremities in case of non-testable myotomes highlights the specificity of the MAC-SCI for the trauma setting, since trauma patients may have associated injuries to the extremities that limit strength testing.
Attempts have been made in the past to develop a simplified neurological examination tool for the acute management of SCI, supporting the important need for a streamlined neurological evaluation in an emergency setting. The SPEED 15 was intended to be performed by first line clinicians to detect SCI, but its oversimplification (scoring from zero to 8) makes it impossible to determine with accuracy the severity grade and the NLI, which are 2 key principles of the ISNCSCI. For example, the severity grade and NLI are important aspects for clinicians to decide on the need, timing and level (ie cervical vs thoracic vs lumbo-sacral) for CT imaging of the spine and magnetic resonance imaging of the spinal cord, which are not included routinely as part of the ATLS imaging protocol. Moreover, as opposed to the MAC-SCI, this previous method does not allow comparison with subsequent ISNCSCI exams, when for example, a neurological deterioration is suspected. Conversely, all elements of the MAC-SCI are included in the ISNCSCI, such that direct comparisons can be made for corresponding elements. Another attempt at simplifying the ISNCSCI is the Expedited-ISNCSCI, 16 although it has never been validated in a clinical study. This tool has been designed primarily for rehabilitation and follow-up purposes, and not for the acute trauma setting. 16 Furthermore, performing the E-ISNCSCI examination relies on a previous complete ISNCSCI examination, which makes it unsuitable for use in trauma protocols when a neurological examination is performed for the first time after the trauma.
The optimal window for performing the MAC-SCI evaluation is the acute period during which distractors such as associated injuries, pain and the need for additional emergent evaluations/interventions would make a complete ISNCSCI documentation unrealistic to perform. More specifically, we suggest that MAC-SCI be used within trauma assessment protocols such as the ATLS, and ISCNSCI be performed promptly when the ATLS is complete and all barriers precluding complete ISCNSCI documentation are overcome.
Limitations
The MAC-SCI is not intended to replace the ISNCSCI. It is crucial that a complete baseline ISNCSCI exam be performed whenever feasible following the acute trauma assessment. As for any trauma patient, every effort should be made to collect a good patient history in conjunction with the MAC-SCI, with particular attention to subjective symptoms, such as axial spinal pain and sensory deficits in the extremities such as paresthesia and numbness. The presence of subjective sensory deficits in the extremities is particularly important because it could help to detect a SCI that would not be identified solely from the MAC-SCI, such as a cervical central cord syndrome with sensory deficits in the upper extremities but preserved motor strength.17,18 In case patients complain about sensory deficits in the extremities, we recommend that light touch assessment be performed in dermatomes of corresponding extremities if motor testing shows normal strength for all myotome. Although isolated sensory radiculopathies are not considered as SCI per se, subjective sensory symptoms in the absence motor deficit should also warrant dermatome assessment in the corresponding extremities in addition to motor testing, because it could help to detect the presence of injuries such as isolated facet fracture and/or dislocation or traumatic disc herniation.
In conclusion, the MAC-SCI is a streamlined, simple and accurate neurological examination tool to detect and locate SCI in the trauma patient. It allows rapid detection and accurate location of the SCI while determining the completeness of the SCI with perfect concordance with the AIS grade. This new neurological examination tool should be used in trauma assessment protocols. We believe a simple and streamlined neurological evaluation tool like the MAC-SCI would lead to a better adherence to a standardized neurological examination, increased reproducibility between tests and observers, and ultimately better patient care in the acute management of tSCI.
Footnotes
Authors’ Contributions
JMMT participated in the study design, data measurement, data analysis, drafting of the manuscript, revision and final acceptance of the manuscript and in securing funding. RPR participated in the study design, data collection, data measurement, data analysis, drafting of the manuscript and revision and final acceptance of the manuscript. AD participated in the study design, data collection, measurement, data analysis, drafting of the manuscript and revision and final acceptance of the manuscript. ARD participated in the study design, data analysis, revision and final acceptance of the manuscript. MMB participated in the study design, data analysis, revision and final acceptance of the manuscript. EBM in the study design, data analysis, revision and final acceptance of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
Dr Mac-Thiong reports grants from Fonds de recherche du Québec - Santé, grants from Medtronic research chair in spinal trauma at Université de Montréal, grants from Praxis Spinal Cord Institute, during the conduct of the study; other from Spinologics Inc., grants from Medtronic, grants from DePuy-Synthes, grants from Canadian Institutes of Health Research, grants from Craig H Neilsen Foundation, grants from New Frontiers in Research Fund, grants from Fonds de recherche du Québec, grants from Canada Foundation for Innovation, grants from U.S. Department of Defense, grants from Medline Industries, grants from Vertex Pharmaceutical, grants from Abbvie, grants from Asahi Kasei Pharma, outside the submitted work; Dr Pelletier-Roy has a scholarship from Medtronic research chair in spinal trauma at Université de Montréal; Antoine Dionne a scholarship from Medtronic research chair in spinal trauma at Université de Montréal and from PRogramme d’Excellence en Médecine pour l’Initiation En Recherche (PREMIER) at Université de Montréal; Dr Richard-Denis reports grants from Fonds de recherche du Québec – Santé, grants from Praxis Spinal Cord Institute, during the conduct of the study; other from Spinologics Inc., grants from Canadian Institutes of Health Research, grants from Craig H Neilsen Foundation, grants from New Frontiers in Research Fund, grants from Medline Industries, grants from Fonds de recherche du Québec, outside the submitted work; Dr Bourassa-Moreau reports grants from Medtronic, grants from Depuy-Synthes, outside the submitted work; Dr Briand reports grants from Fonds de recherche du Québec – Santé and scholarship from Canadian Institutes of Health Research.