
Abstract
Study Design:
Narrative review.
Objectives:
To provide an updated overview of the management of acute traumatic central cord syndrome (ATCCS).
Methods:
A comprehensive narrative review of the literature was done to identify evidence-based treatment strategies for patients diagnosed with ATCCS.
Results:
ATCCS is the most commonly encountered subtype of incomplete spinal cord injury and is characterized by worse sensory and motor function in the upper extremities compared with the lower extremities. It is most commonly seen in the setting of trauma such as motor vehicles or falls in elderly patients. The operative management of this injury has been historically variable as it can be seen in the setting of mechanical instability or preexisting cervical stenosis alone. While each patient should be evaluated on an individual basis, based on the current literature, the authors’ preferred treatment is to perform early decompression and stabilization in patients that have any instability or significant neurologic deficit. Surgical intervention, in the appropriate patient, is associated with an earlier improvement in neurologic status, shorter hospital stay, and shorter intensive care unit stay.
Conclusions:
While there is limited evidence regarding management of ATCCS, in the presence of mechanical instability or ongoing cord compression, surgical management is the treatment of choice. Further research needs to be conducted regarding treatment strategies and patient outcomes.
Introduction
Traumatic spinal cord injury (SCI) is a devastating event for patients and challenges physicians and the health care system. Individuals affected by SCI have characteristic motor, sensory, and autonomic physiologic disturbances as well as financial and psychosocial challenges. In the United States, there are approximately 17 700 new cases of SCI annually. 1 These injuries occur most frequently after traumatic events from motor vehicle accidents and falls, and males are more commonly affected than females. 1 The magnitude of functional impairment following a SCI is classified based on the preserved neurologic function below the level of injury. Complete SCI is defined as total loss of motor and sensory neurologic function below the level of injury, whereas incomplete SCI is characterized by partial preservation of some motor and sensory neurologic function below the level of injury.
Central cord syndrome (CCS) is the most commonly encountered incomplete SCI subtype. Approximately 11 000 patients suffer an incomplete SCI with CCS each year in the United States. 2 CCS is commonly the result of a traumatic event but may also be the consequence of intramedullary tumors or syringomyelia. Acute traumatic central cord syndrome (ATCCS) is typically the result of a hyperextension injury and may occur in the setting of a fracture or dislocation or in the presence of preexisting cervical stenosis. ATCCS incidence has a bimodal distribution, affecting patients under the age of 30 years old following high-impact trauma and elderly patients after low-energy injuries. 3 The physical exam findings of ATCCS are classically characterized as motor and sensory disturbance that is predominantly in the upper extremities with emphasis on hand dysfunction and sparing of or milder findings in the lower extremities. Because this injury may present in the setting of mechanical instability or with preexisting stenosis alone, treatment has historically been variable among surgeons. Patient-specific characteristics such as fracture pattern, medical comorbidities, and neurologic status factor into treatment decisions. The purpose of this narrative review is to provide an updated, evidence-based overview of current ATCCS management.
Acute Traumatic Central Cord Syndrome
Identification and differentiation of ATCCS from other types of cord injuries is important due to its very different outlook and due to the potential role and timing of surgical care. ATCCS was first described in 1954 by Schneider et al as a SCI with “disproportionately more motor impairment of the upper than of the lower extremities, bladder dysfunction, usually urinary retention, and varying degrees of sensory loss below the level of the lesion.” 4 Hayes et al more recently described ATCCS as showing greater weakness in the upper limbs than in the lower limbs as demonstrated by patients with a cervical level of injury with a lower average bilateral upper extremity motor score (C5-T1 segments) compared with the lower extremity motor score (L2-S1 segments). 5 Additionally, patients with ATCCS will have sacral sparing as defined by sensory score greater than zero for light touch or pin prick in the perianal region. 5 Frequently, ATCCS patients have bladder involvement that is commonly manifested as urinary retention. 5 This constellation of early symptoms is unique to CCS and differs from other forms of incomplete SCI such as Brown-Séquard syndrome, anterior cord syndrome, posterior cord syndrome, or cauda equina syndrome.
The mechanism of ATCCS is most commonly associated with a hyperextension injury of the cervical spine. Classically, an anterior-posterior compression force injures the spinal cord, where underlying cervical stenosis and spondylosis predisposes one to a cord injury. While a bony injury may not occur at this time, ATCCS is also seen after cervical spine fractures with or without dislocation as well as the result of acute disc herniation. 4,6,7 Anteriorly, osteophytes as well as calcified or noncalcified herniated discs may lead to narrowing of the canal at a focal area. During the traumatic event, the anterior space occupying lesion can impinge the spinal cord and possibly impact anterior spinal artery flow, while posteriorly the ligamentum flavum may infold into the canal resulting in posterior thecal sac compression. 4,7 While the classical reasoning by Schneider for disproportionate arm versus leg dysfunction relied on the notion that the affected medial aspect of the lateral corticospinal (CST) tract fibers supply arm function, his work predicated on that of Foerster, who presumed that the lateral CST, like the fasciculi cuneatus and gracilis and the lateral spinothalamic tract, had a somatotopic organization. 4,8 Neuroanatomic tracer and Marchi degeneration studies in monkeys have demonstrated that corticospinal fibers supplying the upper and lower limbs are diffusely distributed within the lateral CST of the posterolateral funiculus of the spinal cord. 9,10 There is increasing thought that the pattern of weakness seen in ATCCS has little to do with focal injury and more to do with relative preservation of extrapyramidal fiber tracts, therefore producing a clinical syndrome consisting of disproportionate arm and hand weakness. 11 Furthermore, in an magnetic resonance imaging and pathological analysis, Quencer et al found ATCCS to be characterized by diffuse white matter injury of the lateral columns, with sparing of the central gray matter. 12 These findings bring into question the original pathoanatomic basis for this injury and even the term “central cord syndrome.”
ATCCS exhibits unique characteristics from other forms of SCI including its potential for spontaneous recovery and lack of certainty regarding presence of instability or exact mechanism of injury, further complicating treatment algorithms. The remainder of the article will synthesize the recent literature in an attempt to explain an evidence-based treatment algorithm.
Initial Management
While the aim of this article is to discuss the overall management of CCS with or without mechanical instability, it is critical to remember that, above all, CCS is an incomplete spinal cord injury; therefore, while a detailed description on the ideal medical management of a spinal cord injury is beyond the scope of this article, it is critical to have a basic understanding of the medical management of SCI when treating a patient with ATCCS.
Initial management of patients with SCI begins in the field, with appropriate triage by emergency responders. Resuscitation according to the acute traumatic life support protocols should be followed and rigid immobilization of the spinal column is paramount to prevent further cord damage. 13 Immobilization is typically accomplished with the use of a backboard, rigid cervical collar, or manual stabilization such as a logroll technique or inline cervical stabilization for transfers. 14 The goals of medical management of SCI are prevention of secondary injury and neuroprotection. The initial neurological insult from compression, laceration, distraction, or swelling causes damage to the microvasculature of the cord and results in hemorrhage, vasogenic edema, and worsening ischemia. 15 -17 An inflammatory cascade is initiated, leading to expansion of the zone of injury. 17 -19 Hemodynamic management and abating the inflammatory response are the mainstays of medical management.
The purpose of hemodynamic management after acute SCI is to optimize perfusion of the penumbra adjacent to the injury site and mitigate the effects of impaired spinal cord autoregulation. 20 However, the efficacy of blood pressure augmentation is not clear. Classic studies by Levi et al in 1993 and Vale et al in 1997 purported improved outcomes when the mean arterial pressures (MAP) was kept above 85 or 90 mm Hg for 5 to 7 days. In spite of these studies, the contemporary clinical evidence is less clear. 21 -23 Hawryluk et al reported on 100 patients with acute SCI and found that patients with higher average MAP values had improved recovery in the first 2 to 3 days after their injury. 24 In contrast, Martin et al found in their study of 105 patients with cervical and thoracic SCI that episodes of hypotension and vasopressor requirements did not correlate with changes in American Spinal Injury Association (ASIA) motor score in the acute setting, regardless of MAP goals. 20 Despite some contradictory evidence, the current recommendation of the American Association of Neurosurgeons and Congress of Neurosurgeons is to avoid hypotension, with the target of MAP between 85 and 90 mmHg for 7 days postinjury. 25 Furthermore, there is currently a Phase III non-inferiority prospective, randomized trial underway to compare maintenance of normotension versus induced hypertension that will hopefully elucidate the role of MAP goals in the acute management of SCI. 26
Methylprednisolone is one of the most extensively studied pharmacological agents employed to interrupt the inflammatory cascade that causes secondary injury in SCI. 17,27 Glucocorticoids inhibit cell membrane breakdown and lipid peroxidation and hydrolysis. Maintaining cell membrane integrity prevents the release of vasoreactive by-products of arachidonic acid metabolism, thereby improving blood flow to the site of the SCI. 18,28 -30 The landmark National Spinal Cord Injury Study (NASCIS) trials, published between 1990 and 1998, investigated the clinical efficacy of high-dose methylprednisolone in acute SCI. 18,29,30 However, the validity of the NASCIS trials has been heavily criticized for its post hoc time course, with many deeming the 8-hour timeframe as arbitrary and without physiologic basis. 27,28 Administration of methylprednisolone also carries the risk of significant adverse effects, including infections, gastrointestinal ulcers, prolonged intensive care stay, and overall mortality. 31 -35 In 2013, the Congress of Neurosurgery issued a Level 1 recommendation against the use of methylprednisolone for acute SCI, citing the lack of Class I or Class II medical evidence to support a clinical benefit and inconsistent Class III evidence likely related to random chance. 27 In 2016, AOSpine suggested administration of 24-hour infusion of methylprednisolone to patients within, but not after, 8 hours of injury, and recommended against 48-hour infusion of methylprednisolone. 28
Currently, there is still variation in the medical management of SCI and the roles of both methylprednisolone and MAP goals are controversial. Additional research is underway to investigate the role of neuroprotective agents such as riluzole, granulocyte-colony stimulating factor, glibenclamide, minocycline, Cethrin (VX-210), anti-Nogo-A antibody, as well as alternative therapies such as therapeutic hypothermia and hyperbaric oxygen treatment. 36,37 Of importance is the consideration of disproportionate representation of ATCCS patients in comparison cohorts of SCI studies, as patient with central cord syndromes can be expected to have a better recovery potential than all other incomplete cord injuries. They are also prognostically different than patients with an established complete cord injury. This important aspect has not been addressed proactively in many of the SCI studies reviewed above.
Conservative Management
The management of ATCCS has remained controversial with a multitude of studies evaluating surgical versus conservative treatment strategies (Table 1). One of the critical issues determining the ideal treatment is that there is significant heterogeneity in the diagnosis, and this can make evaluation of the literature challenging. While many of the following studies report acceptable treatment with conservative care, it is paramount to understand that conservative care should only be considered in patients without associated instability. From a historical perspective and under consideration of significant surgical limitations of its time, Schneider et al reported that surgical intervention in patients with ATCCS is actually contraindicated due to substantial neurologic improvement with conservative treatment. 3,6 In 1977, Shrosbree presented a case series of 99 patients with ATCCS that were treated conservatively with traction or immobilization. 38 In their analysis, 39 patients had isolated hyperextension injuries while 60 patients had compression injuries or associated cervical fracture/dislocations. They found that patients who present with a more severe initial neurologic deficit are less likely to improve as much as those with a lesser deficit. 38 Ishida and Tominaga reported the results of a prospective multicenter case series of 22 patients treated conservatively for ATCCS without cervical fracture(s). 39 Nearly all patients had significant improvement in neurologic function by 6 weeks after their initial injury. 39 From this largely historic context we do know that ATCCS has an inherent recovery potential even without surgery.
Surgery Versus Conservative Treatment.
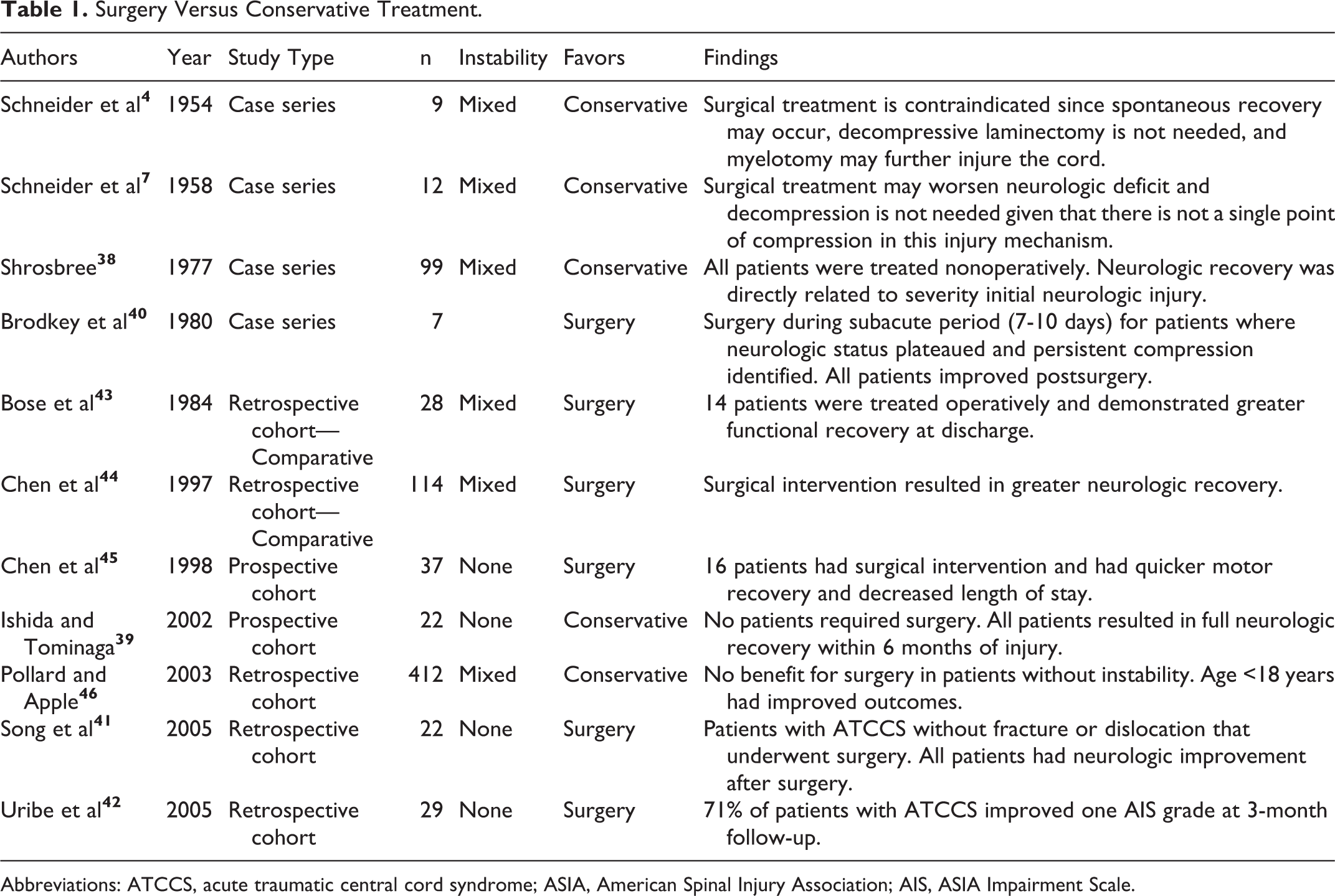
Abbreviations: ATCCS, acute traumatic central cord syndrome; ASIA, American Spinal Injury Association; AIS, ASIA Impairment Scale.
Nonsurgical Versus Surgical Intervention
Brodkey et al retrospectively evaluated 7 patients who underwent surgical intervention for ATCCS after neurologic recovery had plateaued and a persistent compressive lesion was identified on myelogram. 40 All patients in their cohort experienced improved neurologic recovery secondary to removing the source of ongoing compression. 40 Song et al in a retrospective case series reported the outcomes of 22 patients who underwent surgical management of ATCCS without fracture dislocation. 41 All patients had a surgically amenable lesion causing ongoing spinal cord compression. Patients that failed conservative management were excluded. However, surgical timing was determined by the initial rate of neurologic recovery and surgery was only felt to be indicated once neurologic improvement had plateaued. 41 All patients in this cohort experienced neurologic improvement after surgery. Uribe et al reported the results of a retrospective case series of patients treated for ATCCS without fracture or dislocation treated with expansile laminoplasty. 42 At the 3-month follow-up, 71% of patients had improved one AIS (ASIA Impairment Scale) grade. 42
Bose et al compared patients with ATCCS treated with conservative versus surgical management. 43 Patients in the nonoperative cohort did not have evidence of spinal instability. Patients who underwent operative intervention demonstrated structural spinal instability or had plateaued neurologically. They identified that patients undergoing surgical intervention did not develop a neurologic decline postoperatively and had greater functional recovery at discharge compared to the conservative cohort. 43 The author concluded that surgical intervention was a safe and effective treatment in ATCCS. In 1997, a retrospective cohort study by Chen et al compared conservative versus surgical management for patients with ATCCS. 44 They compared nonhomogenous cohorts in which patients with ATCCS (n = 86) without fracture and/or dislocation were treated nonoperatively and patients with fracture and/or dislocation as well as those with ongoing cord compression were treated surgically. 44 In the conservatively managed cohort, 11 patients had signs of ongoing spinal cord compression. Surgical intervention resulted in greater neurologic recovery in the patients with ongoing spinal cord compression compared with those treated conservatively. 44 In 1998, Chen et al reported the results of 37 patients with cervical spondylosis treated for ATCCS. 45 Patients who failed to improve by one motor grade after the initial injury were treated surgically. Sixteen patients underwent surgical intervention on average 9.3 days after the injury. The authors concluded that patients undergoing surgical intervention had a quicker motor recovery and decreased length of stay compared with patients treated conservatively. At 2 years, there was no significant clinical difference identified between the cohorts. 45 In a retrospective cohort study, Pollard and Apple evaluated the results of patients with incomplete SCI, including patients with ATCCS with cervical spondylosis without cervical fracture or dislocation, which were treated nonoperatively versus surgically. 46 Both groups demonstrated neurologic improvement and there was no statistical difference in patient outcomes identified between the 2 management strategies. 46 Younger age (less than 18 years) correlated with improved neurologic outcomes in patients from both cohorts. 46
Both conservative and surgical interventions for ATCCS without fracture and/or dislocation have been demonstrated to result in improved neurologic status. 3,6,38 -42 Patients treated with surgery were identified to have a shorter length of hospital stay as well as a hastened initial neurologic recovery period compared with patients treated conservatively. 45 However, long-term follow-up has failed to demonstrate any significant neurologic differences in patients undergoing conservative versus surgical treatment for ATCCS. 47 For patients with ATCCS and ongoing spinal cord compression, Chen et al demonstrated improved neurologic recovery with surgical decompression as well as decreased length of stay and a decreased risk of developing chronic myelopathy. 44,45 Germane to all of these studies is a trend toward neurologic improvement without surgery over some period of time following ATCCS; however, they do so without providing clarity on the timing for an intervention.
Early Versus Delayed Surgical Intervention
Early surgical intervention, within 24 hours of injury, for SCI in the setting of spinal instability, fracture, and dislocation has become generally well established in the literature. 48 La Rosa et al performed a systematic review evaluating the time to surgical decompression after SCI. 49 They identified that patients with acute SCI who underwent early surgical intervention had superior outcomes compared with patients undergoing delayed surgical intervention as well as those treated conservatively. 49 The Surgical Timing in Acute Spinal Cord Injury Study evaluated early surgical intervention in patients with acute SCI versus delayed surgical intervention. 50 Early surgical intervention was defined as within 24 hours of injury and delayed surgery was greater than 24 hours after injury. Patients that underwent early surgical intervention had greater improvement in the ASIA motor scores compared with the delayed cohort. 50 However, these studies incorporate all forms of incomplete SCI, and in the setting of ATCCS with its potential for recovery with nonsurgical care, timing of surgery has been less clearly defined.
Several studies evaluating timing of surgery in patients with ATCCS have found no difference in overall outcomes between early and late surgical interventions (Table 2). Chen et al evaluated 2 cohorts based on timing of surgery. 51 The first cohort received surgery less than 4 days from injury, and the second cohort underwent a procedure greater than 4 days from injury. 51 Patients with ATCCS from a hyperextension injury, fracture, and/or dislocation as well as instability and acute disc herniation were included. All patients had improvement in neurologic function at 6 months follow-up after injury. No statistical differences were identified between the cohorts. 51 Stevens et al also compared patients with ATCCS based on the timing of surgery. The first subgroup had surgery within 24 hours of injury, the second subgroup had surgery greater than 24 hours from the injury, and the third subgroup had surgery during a second admission. No statistical difference was identified between the early and late surgical subgroups. 52 In another retrospective study, Aarabi et al evaluated patients with ATCCS into 3 groups based on time to surgical intervention: surgery less than 24 hours, 24 to 48 hours, greater than 48 hours from injury. 53 Again, no difference in neurologic outcome was seen between the cohorts. 53 Similarly, Kepler et al evaluated patients undergoing surgical intervention for ATCCS and differentiated patients into a group treated less than or after 24 hours from the time of injury. 54 These authors again identified no short-term change in neurologic status at 7 days for each cohort; furthermore, there was no change in length of stay or length of time in the intensive care unit. 54 The patient population in all of these studies were heterogeneous and involved a only subset of patients with fractures or dislocations. Since there were no subgroup analyses, it is difficult to draw conclusions from these retrospective studies in the setting of mechanical instability.
Early Versus Delayed Surgery for ATCCS.
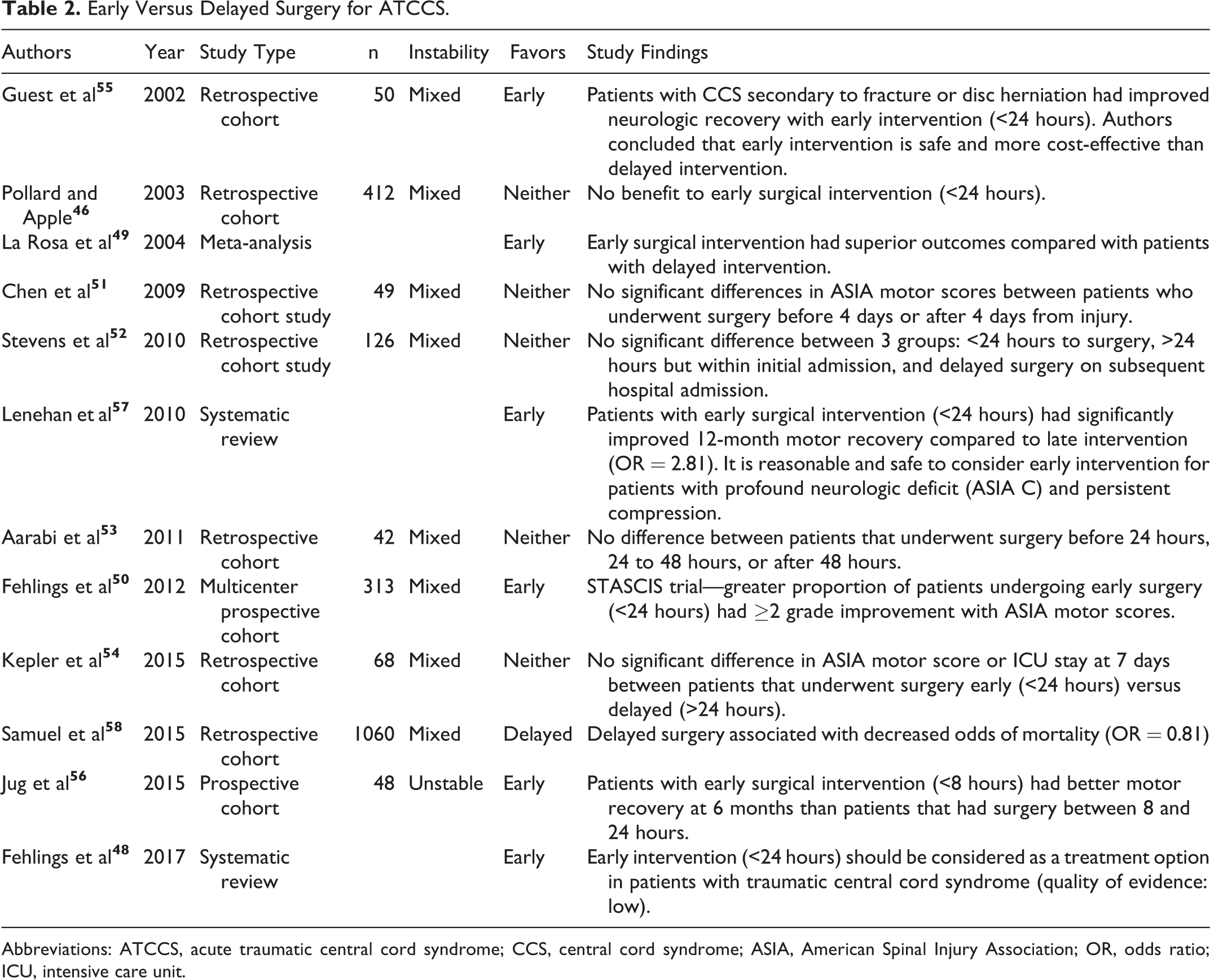
Abbreviations: ATCCS, acute traumatic central cord syndrome; CCS, central cord syndrome; ASIA, American Spinal Injury Association; OR, odds ratio; ICU, intensive care unit.
Contrary to the findings above, several studies evaluating the effect of timing of surgery have demonstrated improved outcomes with early intervention. Guest et al evaluated 50 patients with ATCCS and divided the cohort into patients by mechanism of injury. 55 The first cohort included patients with fracture and/or dislocation, or acute disc herniation, and the second cohort included patients with preexisting cervical spinal stenosis and hyperextension injuries. Each cohort was subdivided by time of surgical intervention, less than 24 hours from injury or greater than 24 hours from injury. They determined that patients with ATCCS secondary to fracture and/or dislocation or acute disc herniation had improved neurologic recovery with early intervention compared with patients undergoing late intervention. 55 Timing of surgery in the cohort whose injury was secondary to hyperextension injury was not demonstrated to have effect on motor recovery. 55 All patients who underwent early surgical intervention had shorter length of stay as well as shorter intensive care unit stays. 55 The authors determined that early surgical intervention is safe, may improve outcomes in the proper injury setting, and could be more cost-effective than delayed surgical intervention. Similarly, a single-center prospective study assessing neurological recovery in 48 patients with mechanical instability undergoing surgery within 8 hours or between 8 and 24 hours after injury found significantly better motor recovery for the within 8-hour group. 56 Lenehan et al, in a systematic review of the literature, evaluated surgical decompression within 24 hours versus delayed decompression occurring after 24 hours from injury in patients with ATCCS without fracture or dislocation. 57 They identified that patients undergoing early decompression had a greater likelihood of improving in ASIA motor score compared with the delayed surgical patients at both the 6-month and 12-month follow-up. 57
In the overall largest study of its kind, Samuel et al performed a retrospective cohort study evaluating 1060 patients with ATCCS who underwent surgical intervention and found differing results. 58 They divided the cohort into 2 subgroups, those who underwent surgery within 24 hours from injury and those who had surgery greater than 24 hours from injury. The delayed operative group had a mean duration of 3.5 days until surgery, and after controlling for preexisting comorbidity and injury severity, they found that this group had a lower inpatient mortality rate. However, this study did not specify the presence of cervical fractures or dislocations and instead based severity on the injury severity score. 58
Prognostic Factors in Patients With ATCCS
Several studies have sought to identify initial postinjury factors and findings that are predictors for recovery of ATCCS. Initial severity of neurologic exam, age, presence of fracture or dislocation, presence of hematoma, and ongoing spinal cord compression are significant prognostic factors of poor patient outcomes. 3,42 -45 Additionally, elderly patients with significant comorbidities have been shown to have a worse prognosis, a lower rate of operative intervention, and a higher inpatient mortality rate. 58 Schroeder et al identified that patients with ATCCS associated with fracture have a worse initial neurologic status but better neurologic recovery in the first week after injury compared with those without fracture. 59 In a separate study, Schroeder et al found that patients with increased T2 signal intensity in their spinal cord on magnetic resonance imaging had a more severe initial neurological injury but had minimal early deterioration compared with those with less cord signal intensity. 60
Other Considerations in the Management of ATCCS
In addition to the treatment strategies and timing of surgical intervention, there remain many controversial management topics for patients with ATCCS. Anti-coagulation therapy is one such area of controversy. Fehlings et al recommended the routine use of anticoagulant therapy after SCI beginning at 72 hours after injury to the high propensity of any cord injury patient to develop venous thromboembolism. 28 More specifically, they recommended the use of low-molecular-weight heparin or fixed-dose unfractionated heparin. However, the authors rated the level of evidence supporting these recommendations to be limited.
Medical management of patients with SCI remains an area of active biomedical and pharmaceutical research. Ongoing studies are evaluating the effectiveness of GM1 Ganglioside, riluzole, and minocycline as medications to limit secondary injury after SCI and promote neurologic recovery. Neuro-regenerative agents are also being investigated such as those that target the blockade of the Rho/ROCK pathway allowing for neuronal regeneration.
Conclusion and Recommendation
The level of evidence for the management of ATCCS is limited, and an evidence-based argument can be made for multiple treatments for patients with ATCCS. However, in patients with mechanical instability, the role of surgery is critical to both address the ATCCS as well as the instability. Furthermore, it is the authors’ preferred treatment to perform an early decompression in patients with continued spinal cord compression. The timing of the decompression is less clear, as several studies have attempted to address the need for early versus delayed intervention with mixed results. Based on the current literature, it is the authors’ preferred treatment to perform early decompression and stabilization in patients that have any instability or that have a significant neurologic deficit. Surgical intervention, in the appropriate patient, is associated with an earlier improvement in neurologic status, shorter hospital stay, and shorter intensive care unit stay. Each patient with ATCCS should be evaluated on an individual basis and a risk-benefit analysis should be conducted to identify the proper management strategy. Further research is needed to identify other potential strategies for improving patient outcomes after ATCCS.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was organized and funded by AOSpine International through the AOSpine Knowledge Forum Trauma, a focused group of international spine experts acting on behalf of AOSpine. Study support was provided directly through the AOSpine Research Department.