
Abstract
Study Design
Mixed-methods approach.
Objectives
Intra-operative spinal cord injury (ISCI) is a devastating complication of spinal surgery. Presently, a uniform definition for ISCI does not exist. Consequently, the reported frequency of ISCI and important risk factors vary in the existing literature. To address these gaps in knowledge, a mixed-methods knowledge synthesis was undertaken.
Methods
A scoping review was conducted to review the definitions used for ISCI and to ascertain the frequency of ISCI. The definition of ISCI underwent formal review, revision and voting by the Guidelines Development Group (GDG). A systematic review of the literature was conducted to determine the risk factors for ISCI. Based on this systematic review and GDG input, a table was created to summarize the factors deemed to increase the risk for ISCI. All reviews were done according to PRISMA standards and were registered on PROSPERO.
Results
The frequency of ISCI ranged from 0 to 61%. Older age, male sex, cardiovascular disease including hypertension, severe myelopathy, blood loss, requirement for osteotomy, coronal deformity angular ratio, and curve magnitude were associated with an increased risk of ISCI. Better pre-operative neurological status and use of intra-operative neuromonitoring (IONM) were associated with a decreased risk of ISCI. The risk factors for ISCI included a rigid thoracic curve with high deformity angular ratio, revision congenital deformity with significant cord compression and myelopathy, extrinsic intradural or extradural lesions with cord compression and myelopathy, intramedullary spinal cord tumor, unstable spine fractures (bilateral facet dislocation and disc herniation), extension distraction injury with ankylosing spondylitis, ossification of posterior longitudinal ligament (OPLL) with severe cord compression, and moderate to severe myelopathy.
Conclusions
ISCI has been defined as “a new or worsening neurological deficit attributable to spinal cord dysfunction during spine surgery that is diagnosed intra-operatively via neurophysiologic monitoring or by an intraoperative wake-up test, or immediately post-operatively based on clinical assessment”. This paper defines clinical and imaging factors which increase the risk for ISCI and that could assist clinicians in decision making.
Introduction
Intra-operative spinal cord injury (ISCI) is one of the most feared and devastating complications of spine surgery.1,2 To date, studies have described ISCI using various definitions and diagnostic criteria. Therefore, the reported frequency and risk factors of ISCI have also varied in the literature. Part of this variability in definition is due to differences in the methods used to determine and define ISCI. Specifically, some studies use findings of intra-operative neuromonitoring (IONM) to define ISCI, while others rely only on post-operative neurological examination findings. The lack of a standardized definition and diagnostic criteria for ISCI is a major challenge in finding solutions to minimize ISCI. Unifying nomenclature and developing standardized diagnostic criteria are essential for accurately quantifying the frequency of ISCI and determining the risk factors associated with it. To the authors’ knowledge, there has been no systematic synthesis of the literature to date that defines ISCI, examines the frequency and outcomes of ISCI, describes the role of IONM, and/or reviews the management strategies in the case of ISCI (both with and without the use of IONM). Additionally, the factors that heighten the risk for sustaining an ISCI have been poorly characterized.
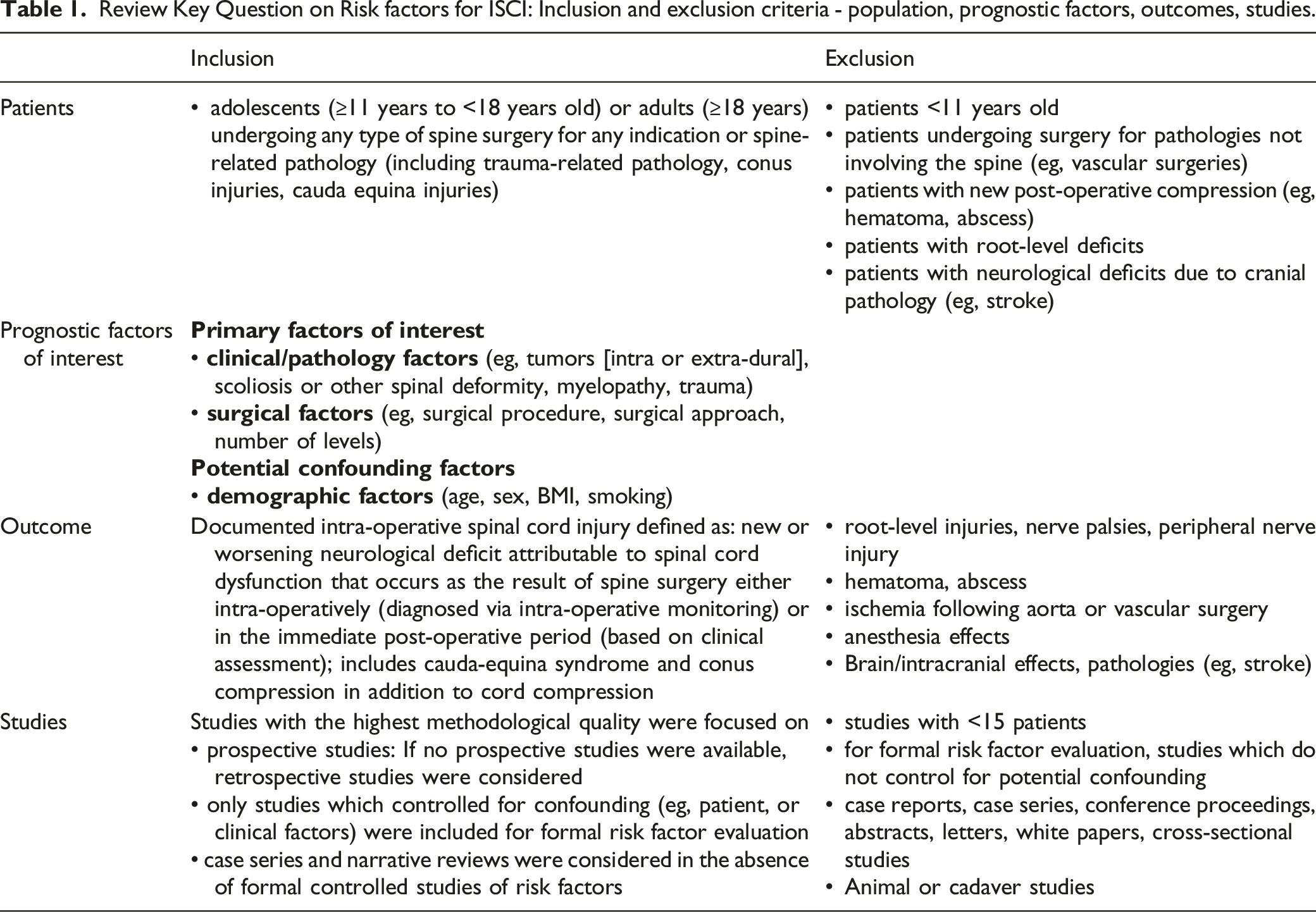
To address these gaps in knowledge, a mixed-methods knowledge synthesis was undertaken. To begin, a formal systematic review was planned and the protocol was registered on PROSPERO (CRD42022298841). The original contextual and key questions as well as the PICOTS (P = Population, I = Intervention, C = Comparators, O = Outcomes, T = Timing, S = Study Design) are found in Table 1. Briefly, the proposed review intended to, (i) Provide context regarding case definitions and diagnostic criteria of ISCI, as well as the use and accuracy of IONM. (ii) Evaluate the risk factors for the development of ISCI. (iii) Address key questions related to comparative effectiveness and harms of ISCI management options. Review Key Question on Risk factors for ISCI: Inclusion and exclusion criteria - population, prognostic factors, outcomes, studies.
Broad scoping literature searches of published literature were conducted, along with input from experts from the Guidelines Development Group (GDG), that yielded substantial yet limited evidence to perform a full systematic review, except for the question regarding risk factors and accuracy of IONM. Given this, our original plan was revised to incorporate scoping reviews that addressed (1) definitions, frequency, and risk factors for ISCI, (2) the use and accuracy of IONM for diagnosis of ISCI, and (3) reported management approaches for ISCI and related harms.
The purpose of this study was to conduct a mixed-methods knowledge synthesis of the literature to address the following questions:
Contextual Question
What definitions and/or monitoring thresholds are used to define ISCI, and what is the reported frequency of ISCI in the existing literature?
Key Question
What are the high-risk factors for ISCI?
Methods
A scoping review was conducted to address the contextual question on the definition and frequency of ISCI. A systematic review was conducted to address the key question examining risk factors for ISCI. Evidence gathered from these underwent review and discussion by the GDG using the Delphi process. Methods used for the systematic review of ISCI risk factors were in accordance with the Agency for Healthcare Research and Quality’s (AHRQ) Methods Guide for Effectiveness and Comparative Effectiveness Review. 3 The contextual question was answered based on the U.S. Preventive Services Task Force (USPSTF) methods 4 for contextual questions, and based on the citations identified via formal literature search as well as additional gray literature.
Study Design
The study was designed with a mixed-methods approach that incorporated evidence from a scoping review and a systematic review, as well as input from a GDG of experts on the topic.
Literature Search Strategies
Literature Databases
The Cochrane Library and MEDLINE® were extensively searched. Included studies were limited to publications in English. Search terms that were used are summarized in Figure 1. Citations from the search were deduplicated and dual-screened for inclusion. In addition, sources of gray literature were reviewed, including professional society guidelines, select pertinent book chapters, and other similar literature, primarily for the contextual question on the definition and frequency of ISCI. Citations suggested by the GDG were compared against the criteria for inclusion and exclusion. The EndNote library was searched using Key Words “risk”. Search Strategy.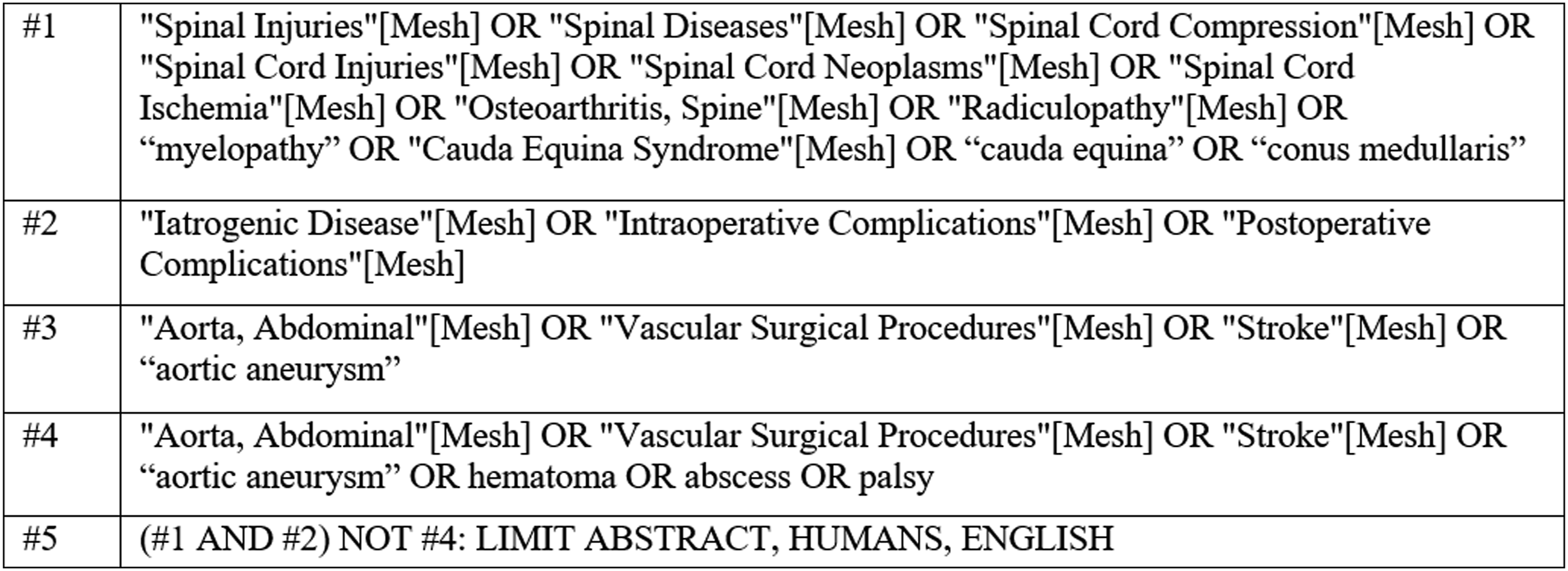
Publication Date Range
The search included citations from database inception to January 26, 2022.
Hand Searching
Reference lists of included studies, systematic reviews, and pertinent gray literature were also evaluated for relevant studies.
Process for Selecting Studies
For the contextual question on the definition and frequency of ISCI
Consistent with other reviews that support guideline updates, studies with the least potential for bias using a “best evidence” approach were focused on. Randomized control trials (RCTs) and high-quality prospective comparative cohort studies that controlled for confounding factors were included as the primary evidence source. In the absence of high-quality studies, lower-quality studies (eg case series) and narrative reviews were also considered.
For the systematic review on risk factors of ISCI, the pre-established criteria summarized in Table 1 were used to screen citations (titles and abstracts) identified by the literature search. Any citation deemed not relevant for full-text review was reviewed by a second researcher to assure accuracy and completeness. Potentially eligible citations identified for inclusion by at least one of the reviewers were retrieved for full-text screening. Each full-text article was independently reviewed for eligibility by two team members. Any disagreements were resolved by consensus. Studies excluded after full-text review with reasons for exclusion are listed in Appendix A.
Data Abstraction and Management
To address the contextual question on definition and frequency, the information on IONM definitions or thresholds and the resolution or persistence of neurological deficit was noted from the selected studies. Data was collected on how the included studies determined there was a neurological deficit. Neurological deficit is determined using clinical neurological assessment and categorizing the degree of deficit based on a grading system. Commonly used grading systems in research and clinical practice for categorizing the severity of a neurological deficit due to spinal cord injury are the American Spinal Injury Association (ASIA) Impairment Scale (AIS) grading system, McCormick grade, and Medical Research Council (MRC) scale for Muscle Strength grading system. Neurological deficit can also be detected by changes in IONM parameters. These include somatosensory evoked potentials (SSEPs) that monitor the integrity of the dorsal column-medial lemniscal pathway, motor evoked potentials (MEPs) and transcranial motor evoked potentials (TcMEPs) that monitor the integrity of the corticospinal tracts, and electromyography (EMG) that indicates the integrity of individual nerves. 5 Importantly, clinical examination and IONM are not mutually exclusive when reporting on ISCI and studies can use either or both methods to document ISCI.
After studies were selected for inclusion in the systematic review on risk factors, standardized data abstraction included the following (at minimum): patient characteristics (age, sex, comorbidities), assessment and categorization of injury severity (AIS) and level of spinal cord injury, indication for spine surgery (eg, scoliosis, tumor), clinical/disease characteristics (eg, myelopathy), surgical factors (eg approach, levels, instrumentation), adjunctive treatments (eg, steroids, vasopressors), and study-related characteristics (eg, sample size, design, control of confounding, the timing of follow-up).
Assessment of Methodological Risk of Bias of Individual Studies
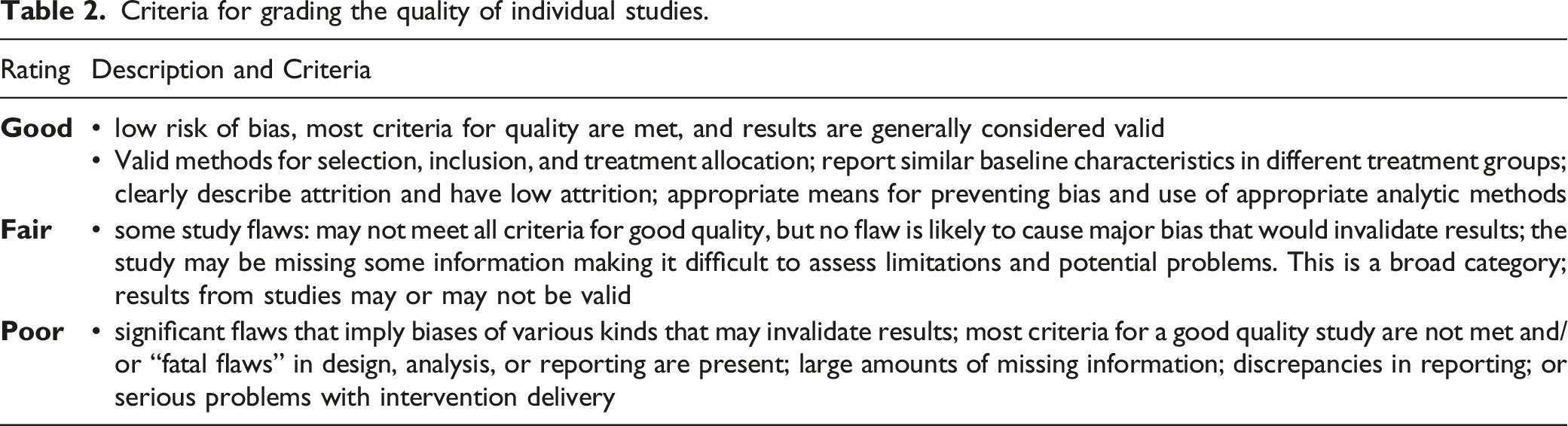
The studies that described ISCI frequency were small case series and were not critically appraised. All were of poor quality.
Criteria for grading the quality of individual studies.
Data Synthesis
The data was qualitatively summarized in tables using ranges, descriptive analyses, and interpretation of the results. Data on the frequency of ISCI were qualitatively synthesized.
Adjusted odds ratios provided by authors were reported. Clinical and methodological heterogeneity across studies precluded the pooling of studies.
Grading the Strength of Evidence for Major Comparisons and Outcomes
The overall quality and strength of evidence (SOE) was assessed based on the application of Grading of Recommendations, Assessment, Development, and Evaluations (GRADE), described in the AHRQ Methods Guide. 3 GRADE guidance related to synthesis of risk factors was used.7,8 The SOE was assigned an overall grade of high, moderate, low, or very low. SOE was evaluated by one methodologist and then reviewed independently by a second for consistency and validity before the final assessment. Disagreements were resolved by consensus. For the systematic review of risk factors, studies were initially considered to be a high quality of evidence. The evidence was downgraded based on the aggregate assessment of risk of bias across studies reporting on the outcome, consistency, imprecision, directness, and publication bias. Strength of evidence was not applied to the results for the contextual question.
Results
Contextual Question
What definitions and/or monitoring thresholds are used to define ISCI, and what is the reported frequency of ISCI in the existing literature?
Definition of Intra-operative Spinal Cord Injury
Contextual Question: Criteria/thresholds for intra-operative SCI and frequency.
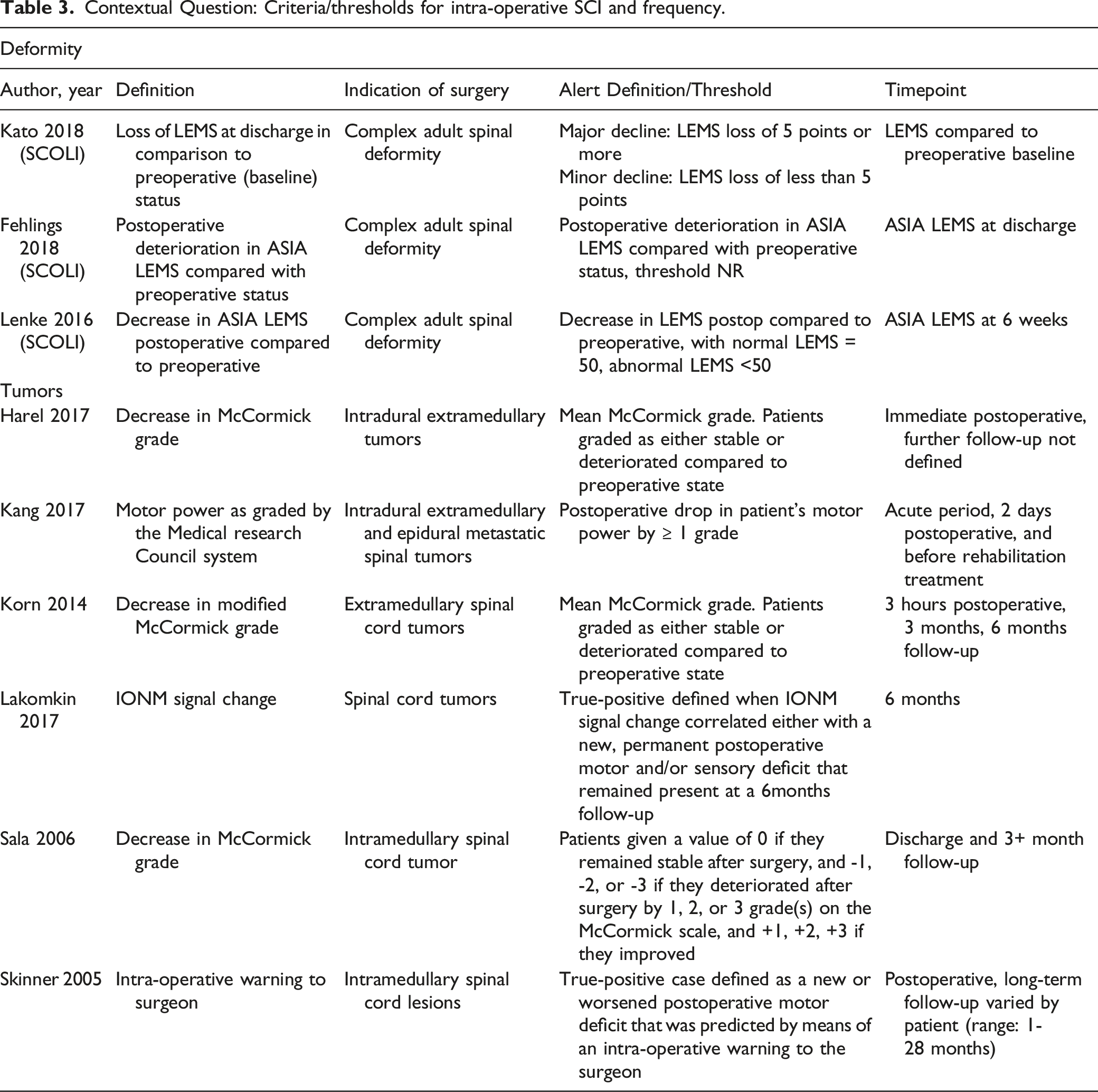
The search generated several studies which were grouped based on indication for surgery into those on deformity surgery and those on tumor surgery. As seen in Table 3, the definitions in the deformity (Kato 2018, 10 Fehlings 2018, 11 Lenke 2016 12 ) groups were centered on deterioration in lower extremity motor score (LEMS). LEMS in these studies was described using the ASIA grading system. In contrast, the tumor studies defined ISCI based on change in McCormick grade, MRC grading system, or IONM prompts (Harel 2017, 13 Kang 2017, 14 Korn 2015, 15 Lakomin 2017, 16 Sala 2006, 17 Skinner 2005 18 ). These studies reported the criteria for defining an ISCI as either a change compared to preoperative LEMS/ASIA score, a LEMS change of 5 points, change in McCormick grade, or in the case of neurophysiologic monitoring, a signal that correlated with a post-operative motor deficit. Briefly, these include MEP amplitude changes of more than 50-80%, SSEP amplitude changes of more than 50-60%, latency prolongation of 10% or 3 milliseconds, TcMEP amplitude change of more than 50-80%, muscle threshold of more than 100 V, EMG amplitude change of more than 50%, sustained bursts/trains, lack of waveform, or a D-wave decrease in amplitude of more than 50%.
The following definition was put forth by the GDG after reviewing evidence from the scoping review and subsequently voting and discussing it in depth, in accordance with the Delphi Process
9
: “a new or worsening neurological deficit attributable to spinal cord dysfunction during spine surgery that is diagnosed intra-operatively via neurophysiologic monitoring, by an intraoperative wake-up test or immediately post-operatively based on clinical assessment.”
Deficits can include dysfunction attributable to injury of the spinal cord, conus medullaris, or cauda equina.
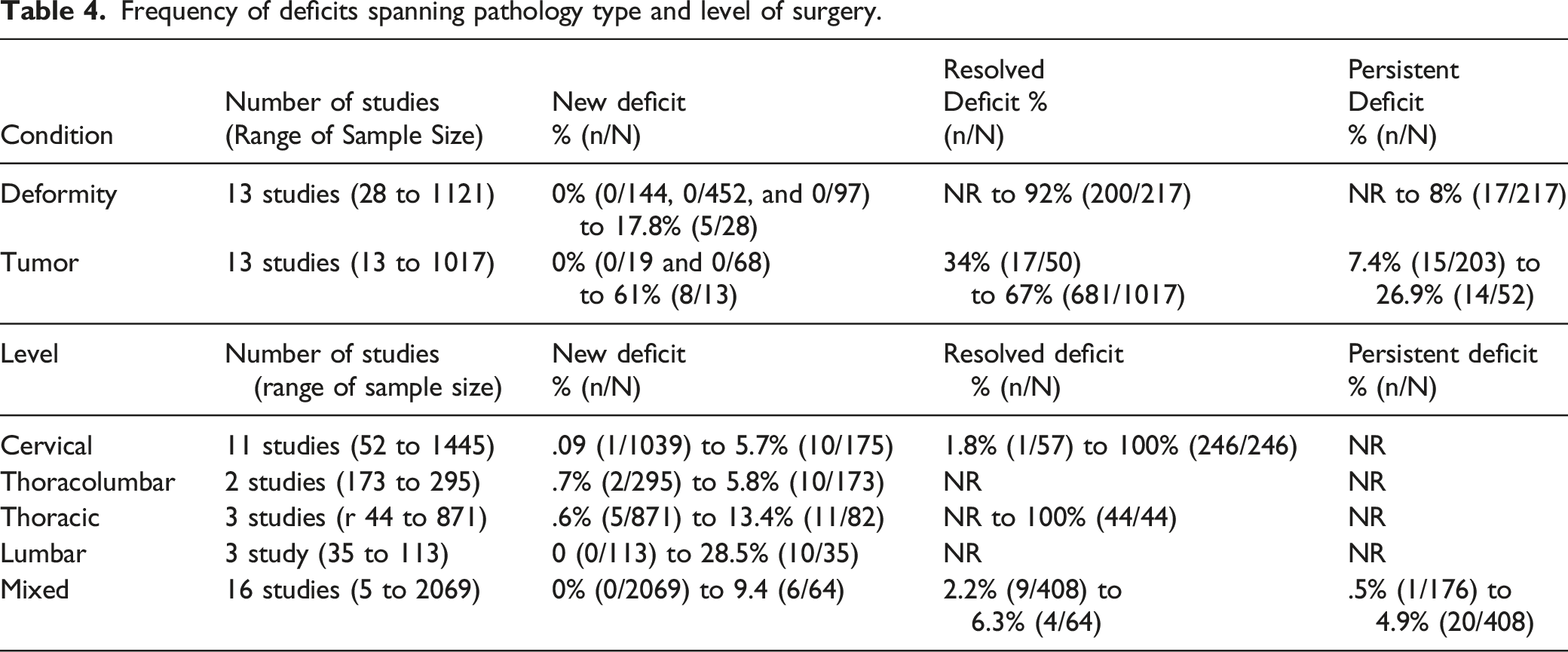
Frequency of Intra-operative SCI
Frequency of deficits spanning pathology type and level of surgery.
Key Question
What Are the High-Risk factors for ISCI?
Risk Factors for ISCI
From the 226 citations identified via literature search, a total of six studies were identified that provided data regarding the frequency of ISCI and conducted multivariable analysis, including four studies (Fehlings 2018,
11
Chen 2012,
19
Kim 2021,
20
Romero-Munoz 2019
21
) that were recommended by clinical experts (Figure 2). An additional surgeon consensus survey (Iyer 2022)
22
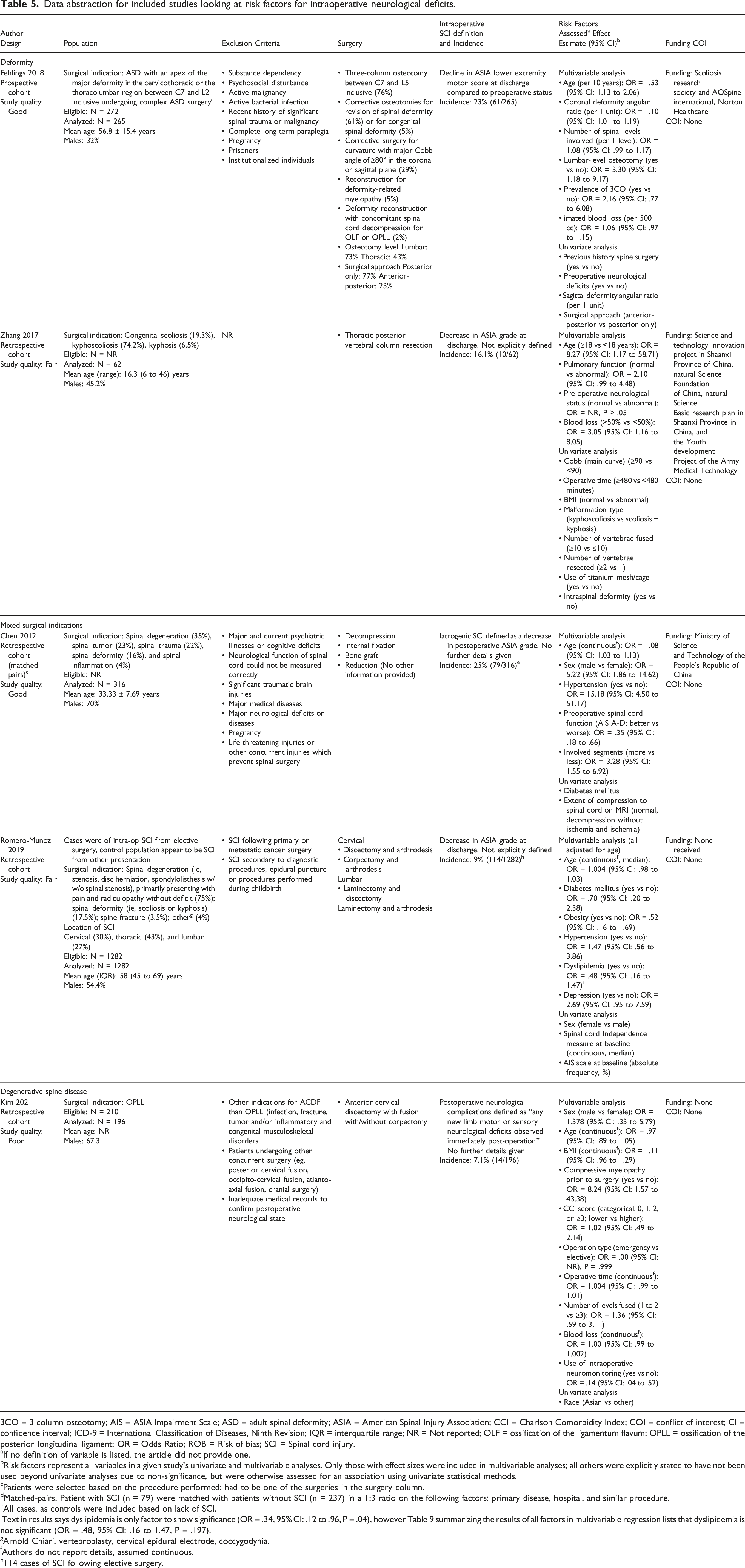
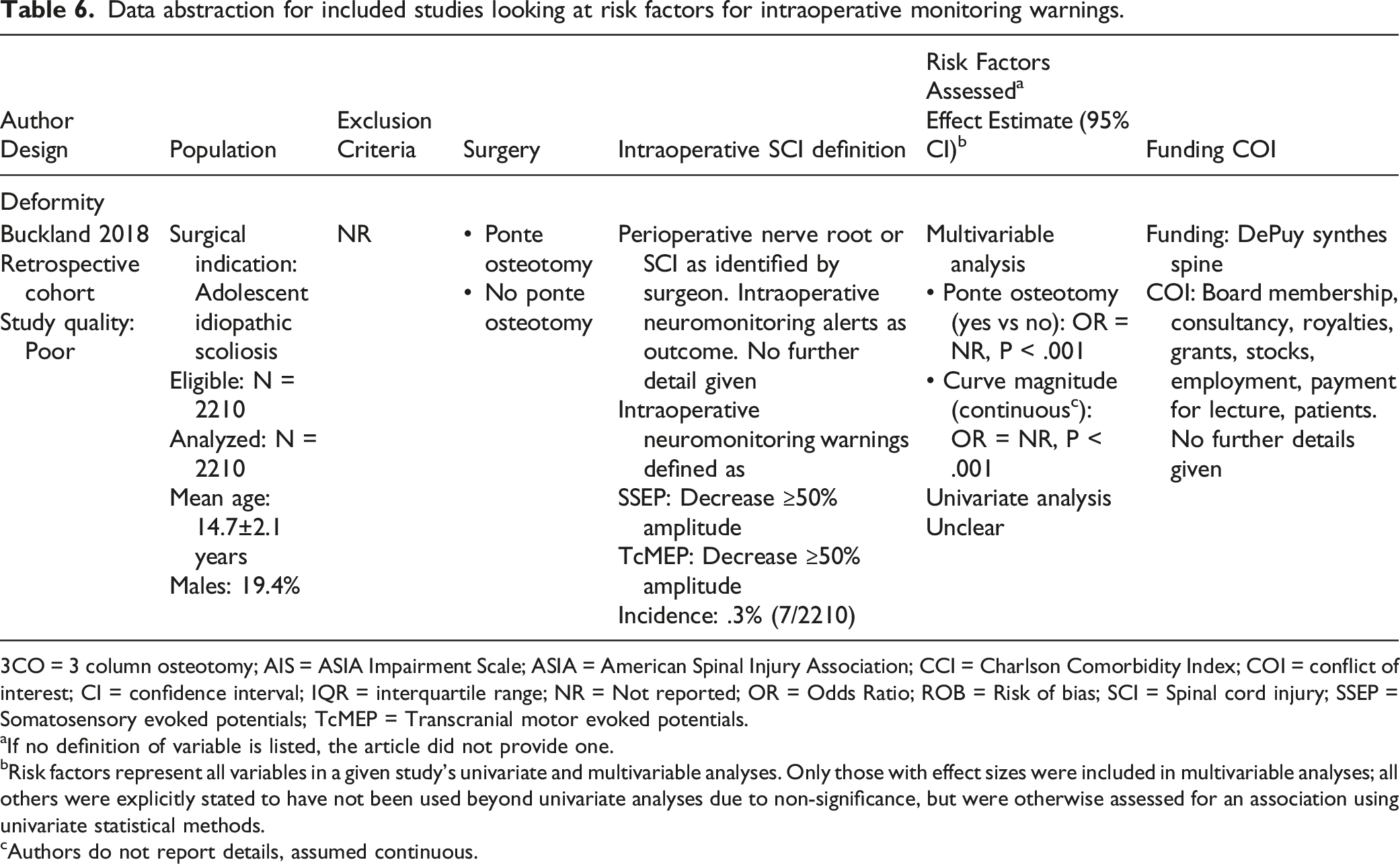
was also considered in the literature analysis, as recommended by the GDG. Data abstraction from these studies is summarized in Tables 5 and 6. Literature search and study selection flow diagram for the systematic review on risk factors of ISCI. Data abstraction for included studies looking at risk factors for intraoperative neurological deficits. 3CO = 3 column osteotomy; AIS = ASIA Impairment Scale; ASD = adult spinal deformity; ASIA = American Spinal Injury Association; CCI = Charlson Comorbidity Index; COI = conflict of interest; CI = confidence interval; ICD-9 = International Classification of Diseases, Ninth Revision; IQR = interquartile range; NR = Not reported; OLF = ossification of the ligamentum flavum; OPLL = ossification of the posterior longitudinal ligament; OR = Odds Ratio; ROB = Risk of bias; SCI = Spinal cord injury. aIf no definition of variable is listed, the article did not provide one. bRisk factors represent all variables in a given study’s univariate and multivariable analyses. Only those with effect sizes were included in multivariable analyses; all others were explicitly stated to have not been used beyond univariate analyses due to non-significance, but were otherwise assessed for an association using univariate statistical methods. cPatients were selected based on the procedure performed: had to be one of the surgeries in the surgery column. dMatched-pairs. Patient with SCI (n = 79) were matched with patients without SCI (n = 237) in a 1:3 ratio on the following factors: primary disease, hospital, and similar procedure. eAll cases, as controls were included based on lack of SCI. iText in results says dyslipidemia is only factor to show significance (OR = .34, 95% CI: .12 to .96, P = .04), however Table 9 summarizing the results of all factors in multivariable regression lists that dyslipidemia is not significant (OR = .48, 95% CI: .16 to 1.47, P = .197). gArnold Chiari, vertebroplasty, cervical epidural electrode, coccygodynia. fAuthors do not report details, assumed continuous. h114 cases of SCI following elective surgery. Data abstraction for included studies looking at risk factors for intraoperative monitoring warnings. 3CO = 3 column osteotomy; AIS = ASIA Impairment Scale; ASIA = American Spinal Injury Association; CCI = Charlson Comorbidity Index; COI = conflict of interest; CI = confidence interval; IQR = interquartile range; NR = Not reported; OR = Odds Ratio; ROB = Risk of bias; SCI = Spinal cord injury; SSEP = Somatosensory evoked potentials; TcMEP = Transcranial motor evoked potentials. aIf no definition of variable is listed, the article did not provide one. bRisk factors represent all variables in a given study’s univariate and multivariable analyses. Only those with effect sizes were included in multivariable analyses; all others were explicitly stated to have not been used beyond univariate analyses due to non-significance, but were otherwise assessed for an association using univariate statistical methods. cAuthors do not report details, assumed continuous.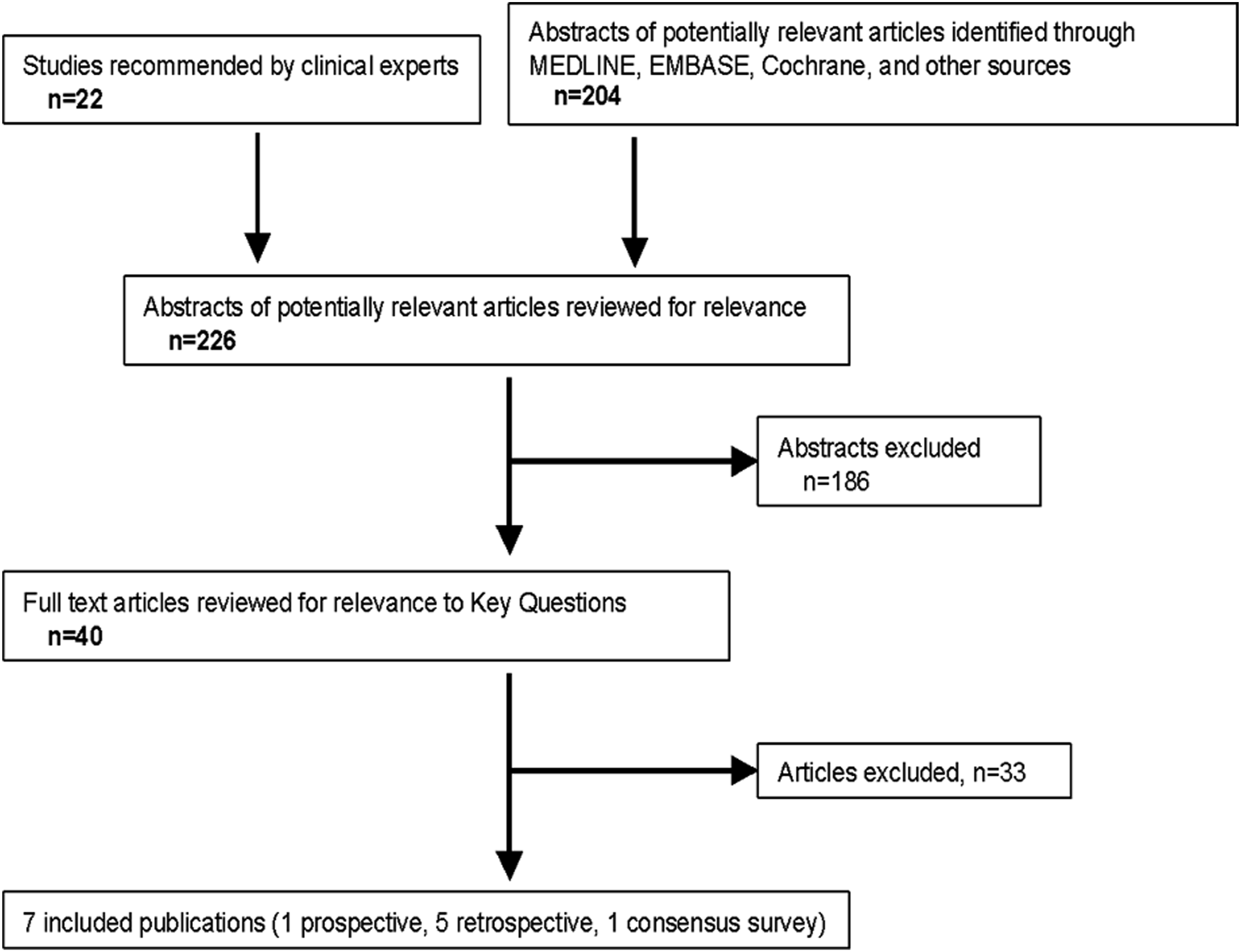
Demographic, clinical, surgical, and radiographic factors potentially associated with intra-operative SCI in studies that conducted multivariable analyses. a
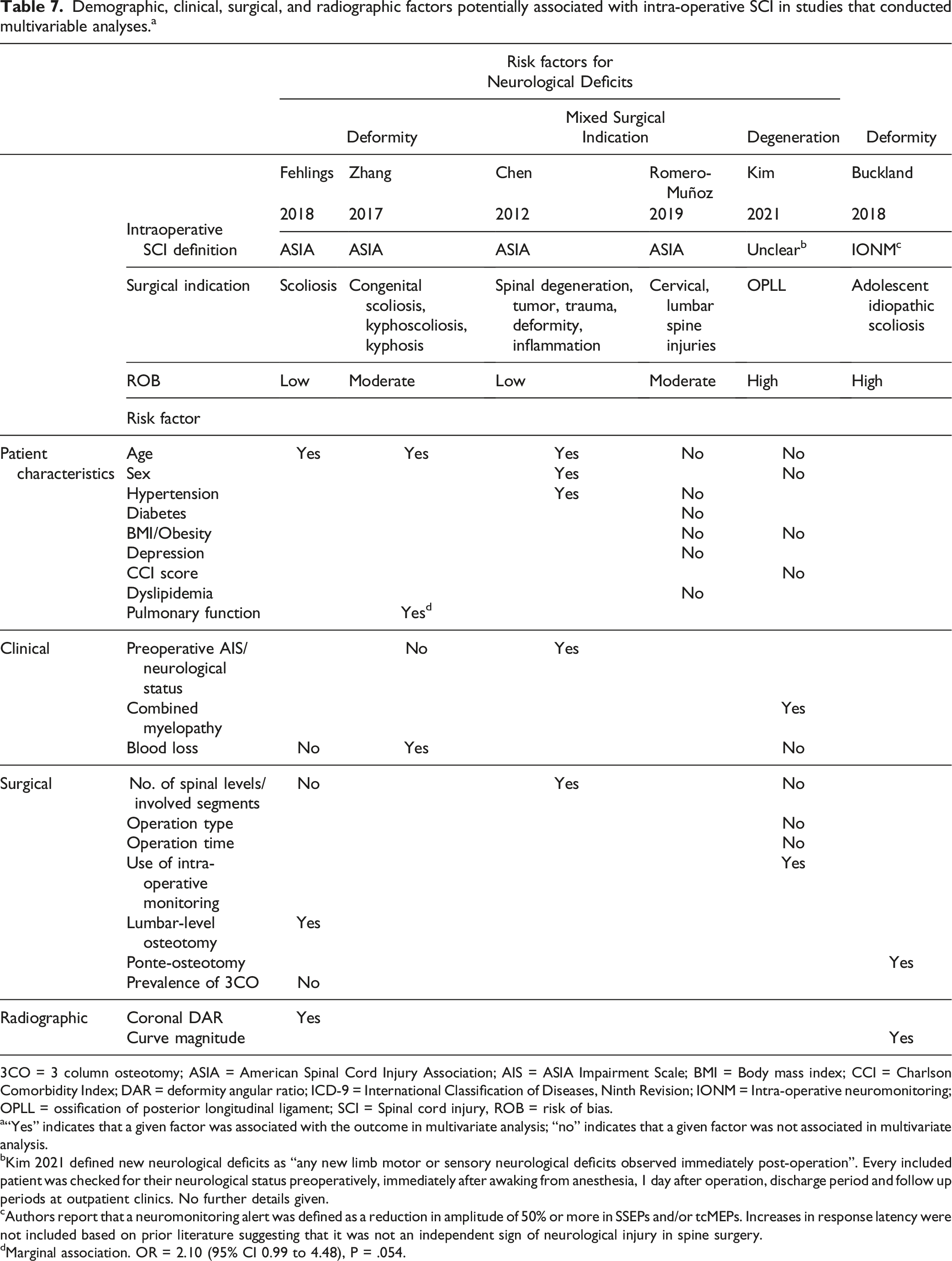
3CO = 3 column osteotomy; ASIA = American Spinal Cord Injury Association; AIS = ASIA Impairment Scale; BMI = Body mass index; CCI = Charlson Comorbidity Index; DAR = deformity angular ratio; ICD-9 = International Classification of Diseases, Ninth Revision; IONM = Intra-operative neuromonitoring; OPLL = ossification of posterior longitudinal ligament; SCI = Spinal cord injury, ROB = risk of bias.
a“Yes” indicates that a given factor was associated with the outcome in multivariate analysis; “no” indicates that a given factor was not associated in multivariate analysis.
bKim 2021 defined new neurological deficits as “any new limb motor or sensory neurological deficits observed immediately post-operation”. Every included patient was checked for their neurological status preoperatively, immediately after awaking from anesthesia, 1 day after operation, discharge period and follow up periods at outpatient clinics. No further details given.
cAuthors report that a neuromonitoring alert was defined as a reduction in amplitude of 50% or more in SSEPs and/or tcMEPs. Increases in response latency were not included based on prior literature suggesting that it was not an independent sign of neurological injury in spine surgery.
dMarginal association. OR = 2.10 (95% CI 0.99 to 4.48), P = .054.
All demographic, clinical, surgical, and radiographic factors explored/evaluated as prognostic factors for intraoperative SCI in univariate analyses. a
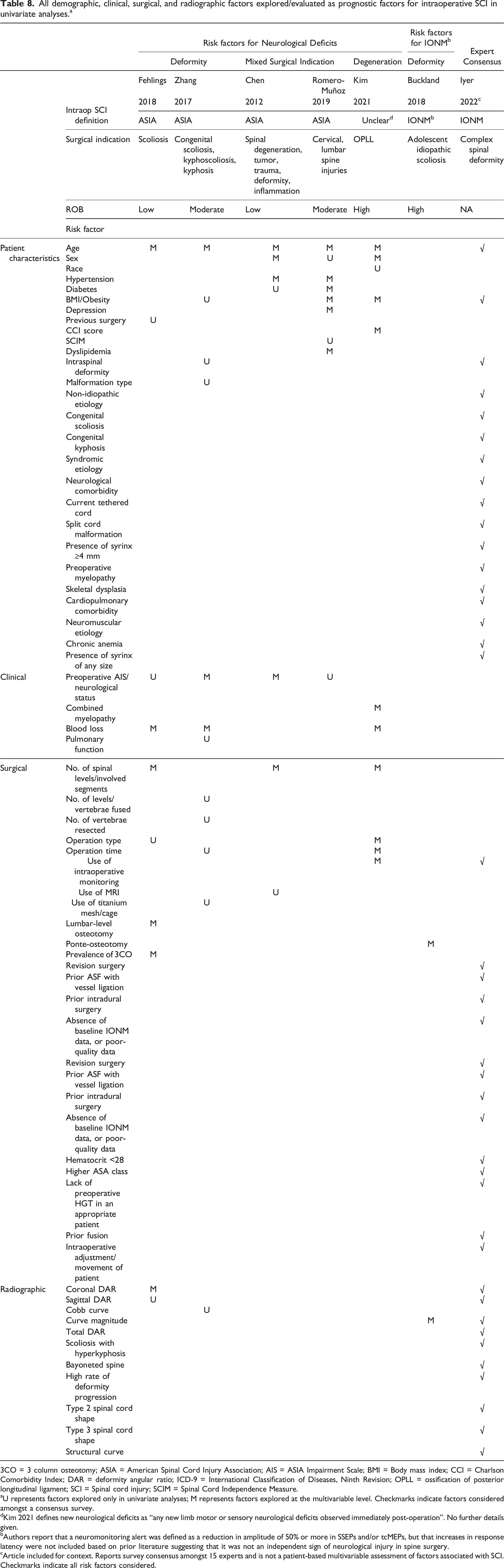
3CO = 3 column osteotomy; ASIA = American Spinal Cord Injury Association; AIS = ASIA Impairment Scale; BMI = Body mass index; CCI = Charlson Comorbidity Index; DAR = deformity angular ratio; ICD-9 = International Classification of Diseases, Ninth Revision; OPLL = ossification of posterior longitudinal ligament; SCI = Spinal cord injury; SCIM = Spinal Cord Independence Measure.
aU represents factors explored only in univariate analyses; M represents factors explored at the multivariable level. Checkmarks indicate factors considered amongst a consensus survey.
dKim 2021 defines new neurological deficits as “any new limb motor or sensory neurological deficits observed immediately post-operation”. No further details given.
bAuthors report that a neuromonitoring alert was defined as a reduction in amplitude of 50% or more in SSEPs and/or tcMEPs, but that increases in response latency were not included based on prior literature suggesting that it was not an independent sign of neurological injury in spine surgery.
cArticle included for context. Reports survey consensus amongst 15 experts and is not a patient-based multivariable assessment of factors associated with SCI. Checkmarks indicate all risk factors considered.
Summary of Effect Estimates for Risk Factors for Intra-operative SCI in Studies Using Multivariable Analysis.
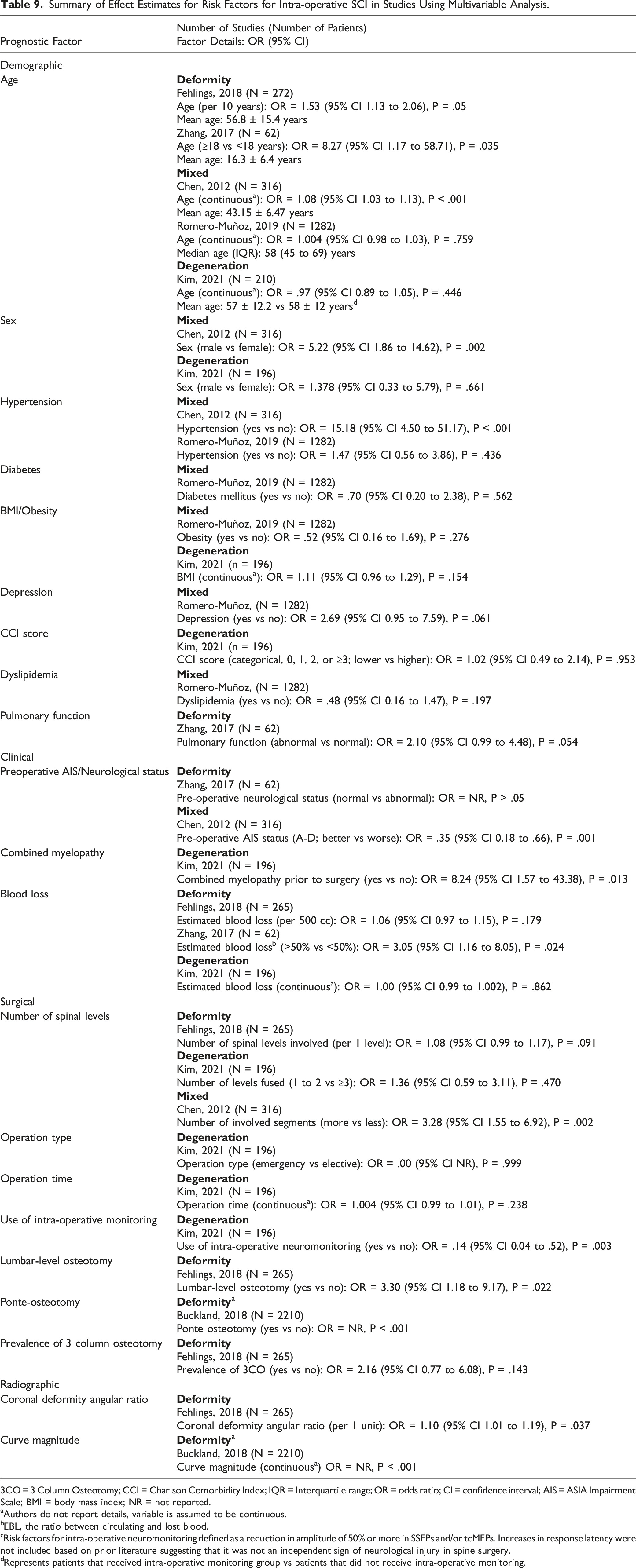
3CO = 3 Column Osteotomy; CCI = Charlson Comorbidity Index; IQR = Interquartile range; OR = odds ratio; CI = confidence interval; AIS = ASIA Impairment Scale; BMI = body mass index; NR = not reported.
aAuthors do not report details, variable is assumed to be continuous.
bEBL, the ratio between circulating and lost blood.
cRisk factors for intra-operative neuromonitoring defined as a reduction in amplitude of 50% or more in SSEPs and/or tcMEPs. Increases in response latency were not included based on prior literature suggesting that it was not an independent sign of neurological injury in spine surgery.
dRepresents patients that received intra-operative monitoring group vs patients that did not receive intra-operative monitoring.
Three patient population groups were identified in the included studies: those with deformity, those with various indications for spine surgery, and those with degenerative disease.
Evidence for the risk factors for neurological deficits in patients with deformities was derived from one good-quality, prospective cohort (Fehlings 2018, N = 265) 11 on scoliosis in adults, and one fair-quality, retrospective cohort (Zhang 2017, N = 62) 23 in patients with congenital scoliosis (19%), kyphoscoliosis (74%), and kyphosis (7%). Another poor-quality retrospective cohort (N = 2210) (Buckland 2018) 24 described risk factors for IONM alerts in adolescent patients with idiopathic scoliosis.
Studies in patients with surgery for deformity found an increased risk of ISCI with older age, higher blood loss, surgical technique related factors like the requirement for osteotomy, and radiographic factors including coronal deformity angular ratio (DAR) and curve magnitude. For patients with “mixed” indications, one good-quality, retrospective cohort (N = 316) (Chen 2012) 19 reported on patients with spinal degeneration (35%), tumor (23%), trauma (22%), deformity (16%), and inflammation (4%), while one fair-quality retrospective cohort (N = 1282) (Romero-Munoz 2019) 21 reported on patients with spinal degeneration (75%), deformity (18%), fractures (4%), or other rare injuries (4%). In this latter study, authors did not describe the group to which patients with ISCI were compared to. It appears that patients receiving elective surgery who experienced ISCI were compared to those with other causes of SCI. Studies enrolling patients undergoing spine surgery for a variety of indications found that older age, male sex, hypertension, depression, and a higher number of operative spinal levels were associated with ISCI.
Strength of evidence (SOE) table assessing risk factors for intra-operative SCI in prognostic studies.
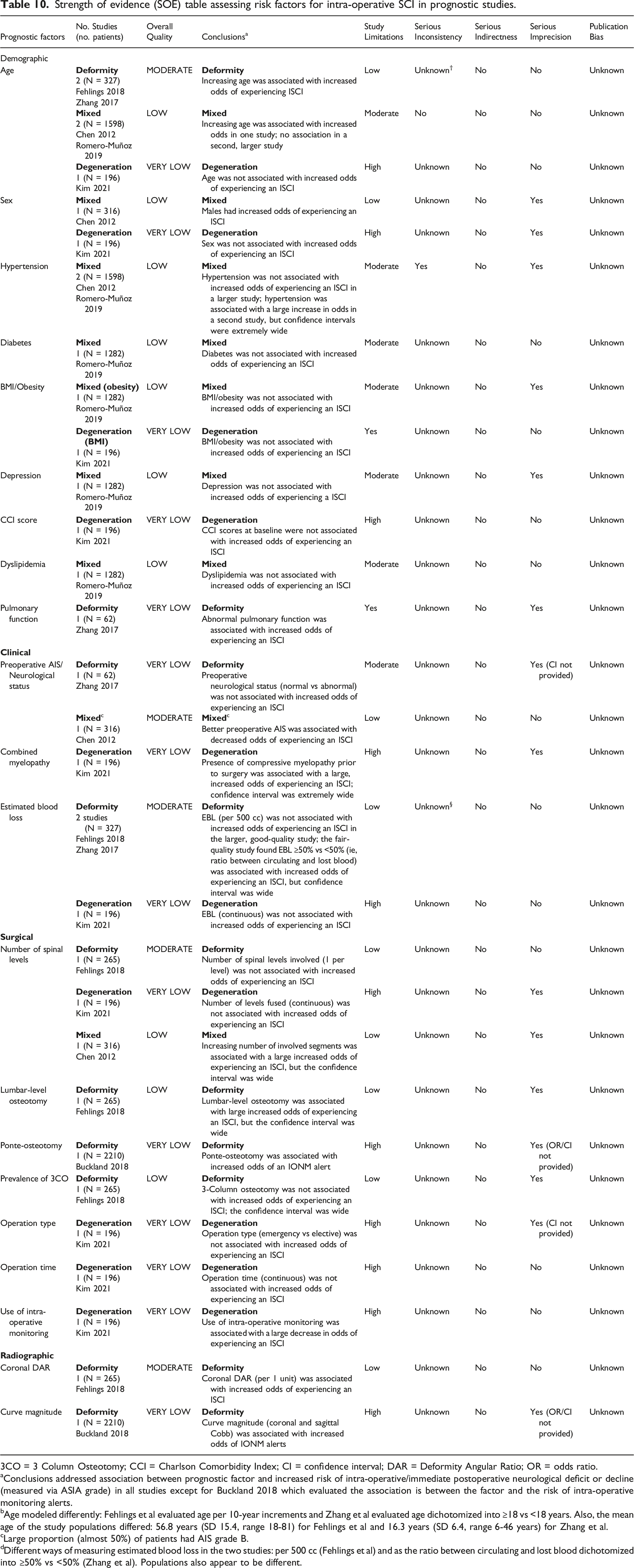
3CO = 3 Column Osteotomy; CCI = Charlson Comorbidity Index; CI = confidence interval; DAR = Deformity Angular Ratio; OR = odds ratio.
aConclusions addressed association between prognostic factor and increased risk of intra-operative/immediate postoperative neurological deficit or decline (measured via ASIA grade) in all studies except for Buckland 2018 which evaluated the association is between the factor and the risk of intra-operative monitoring alerts.
bAge modeled differently: Fehlings et al evaluated age per 10-year increments and Zhang et al evaluated age dichotomized into ≥18 vs <18 years. Also, the mean age of the study populations differed: 56.8 years (SD 15.4, range 18-81) for Fehlings et al and 16.3 years (SD 6.4, range 6-46 years) for Zhang et al.
cLarge proportion (almost 50%) of patients had AIS grade B.
dDifferent ways of measuring estimated blood loss in the two studies: per 500 cc (Fehlings et al) and as the ratio between circulating and lost blood dichotomized into ≥50% vs <50% (Zhang et al). Populations also appear to be different.
Patient Specific Risk Factors for ISCI
Five studies reported on age as a risk factor for ISCI (Fehlings 2018, 11 Romero Munoz 2019, 21 Zhang 2017, 23 Chen 2012, 19 Kim 2021 20 ). Four studies reported increased risk of ISCI with increased age (Fehlings 2018, 11 Romero Munoz 2019, 21 Zhang 2018, 23 Chen 2012 19 ). Two of these studies reported this as a significant association (Zhang 2017, 23 Chen 2012 19 ), while in the other two studies the association was not significant (Fehlings 2018, 11 Romero Munoz 2019 21 ). In one study, a slightly decreased risk of ISCI was associated with increased age (OR = .97), which was not significant (P > .05) (Kim 2021 20 ). Male sex was associated with increased risk of ISCI in two studies. The association was significant in one study, while not significant in the other (Chen 2012, 19 Kim 20 ). Hypertension was associated with a significantly increased risk of ISCI in one study, and a non-significantly increased risk of ISCI in another study (Chen 2012, 19 Romero Munoz 2019 21 ). Diabetes Mellitus was associated with a non-significant decreased risk of ISCI in one study (Romero Munoz 2019 21 ). Obesity was associated with an increased but non-significant risk of ISCI in one study (Romero Munoz 2019 21 ). Another study reported a non-significant increased risk of ISCI with increasing body mass index (BMI) (Kim 20 ). Clinical depression was associated with a non-significant increased risk of ISCI (Romero Munoz 2019 21 ). CCI was also associated with a non-significant increased risk of ISCI (Kim 20 ). Dyslipidemia has a non-significant association with decreased risk of ISCI in one study (Romero Munoz 2019 21 ). Worse pulmonary function was reported to have increased risk of ISCI in one study that was non-significant (Zhang 2017 23 ).
Clinical Risk Factors for ISCI
Pre-operative neurological status was reported as a risk factor in two studies (Chen 2012, 19 Zhang 2017 23 ). In one study, a better pre-operative neurological status was associated with a significantly decreased risk of ISCI (Chen 2012 19 ). In a second study, the association was not significant, although it was associated with a decreased risk (Zhang 2017 23 ). Combined myelopathy was associated with a significantly increased risk of ISCI in one study (Kim 2021 20 ).
Blood loss was associated with an increased risk of ISCI in two studies (Fehlings 2018, 11 Zhang 2017 23 ). The association was significant in one study, and non-significant in the other (Zhang 2017, 23 Fehlings 2018 11 ). In a third study, blood loss had equivocal (OR = 1) association with ISCI that was not significant (Kim 2021 20 ).
Surgical Risk Factors for ISCI
A higher number of spinal levels was associated with increased risk of ISCI in two studies and with a decreased risk in one study. The increased risk was significant in one study and non-significant in the second study. The decreased risk was non-significant (Fehlings 2018, 11 Kim 2021, 20 Chen 2012 19 ). Increasing operation time was associated with increased risk of ISCI, however this was not significant (Kim 2021 20 ). Lumbar level osteotomy was associated with a significantly increased risk of ISCI. In the same study, prevalence of three level osteotomy had a non-significant increased risk of ISCI (Fehlings 2018 11 ). In another study, ponte-osteotomy was associated with a significant increased risk of ISCI (Buckland 2018 24 ). Use of IONM was associated with a significant decreased risk of ISCI in one study (Kim 2021 20 )
Radiological Risk Factors ISCI
One study (Fehlings 2018) 11 on patients with scoliosis reported a greater odds of postoperative neurological deficit per 1 unit increase of coronal deformity angular ratio (DAR). One study (Buckland 2018) 24 in patients with adolescent scoliosis found a significant positive association between spinal curve magnitude and IONM alerts but did not report an effect estimate.
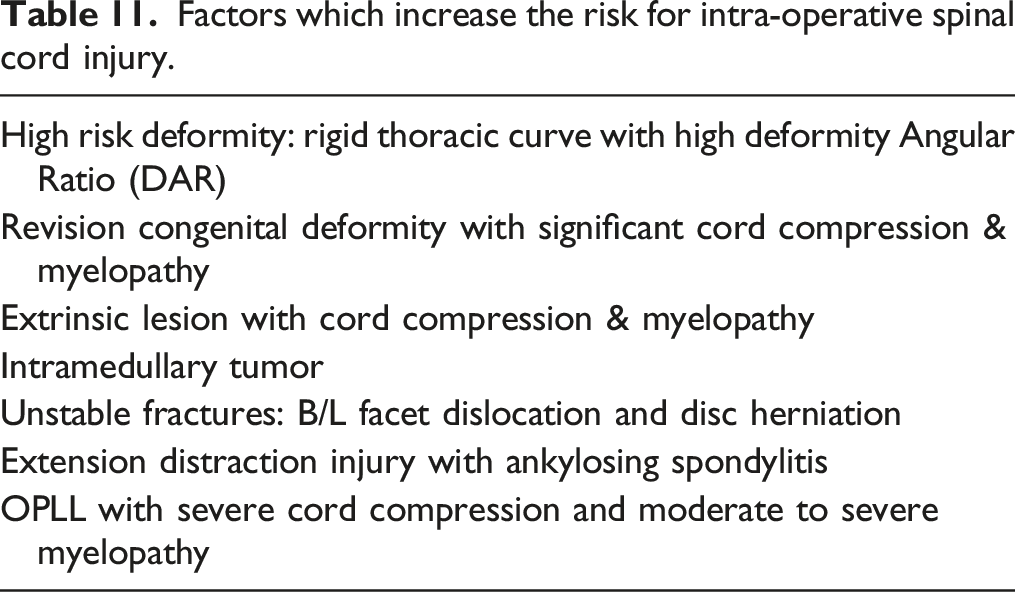
In addition to risk factors identified in the systematic review, the GDG proposed seven characteristics of high-risk patients for ISCI. These included rigid thoracic curve with high deformity angular ratio, revision congenital deformity with significant cord compression and myelopathy, extrinsic intradural or extradural lesion with cord compression and myelopathy, intramedullary tumor, unstable fractures (bilateral facet dislocation and disc herniation, extension distraction injury with ankylosing spondylitis, ossification of posterior longitudinal ligament (OPLL) with severe cord compression, and moderate to severe myelopathy. These risk factors were thoroughly discussed and voted upon by the GDG. Eventually, these risk factors were accepted as high risk after a unanimous vote according to the Delphi Process.
Quality (Strength) of Evidence
The overall quality (strength) of evidence for risk factors for ISCI based on multivariate analyses was low or very low for most factors across surgical conditions (Table 10). Increased odds for ISCI varied by surgical indication/population (eg, deformity). In patients undergoing surgery for spinal deformity, there was moderate evidence of increased odds for ISCI in patients with increasing age and increasing coronal DAR. There was moderate evidence that estimated blood loss and the number of spinal levels were not associated with increased odds of ISCI in the same population. There was moderate evidence that better preoperative AIS was associated with decreased odds of ISCI in a mixed population.
Consensus Summary of Risk Factors for Intraoperative Spinal Cord Injury
Factors which increase the risk for intra-operative spinal cord injury.
Discussion
The study of ISCI has been limited to date. Consequently, prior to this Focus issue, a paucity of evidence exists to guide clinicians in the decision-making surrounding patients who sustain an ISCI. This article has sought to identify the definition, frequency, risk factors, and management of ISCI through a scoping and systematic review of the existing literature.
Definition of ISCI
To define ISCI a scoping review was conducted in which studies were reviewed and divided into two groups based on whether they focused on deformity or tumor surgery. Three studies by Lenke et al, 12 Fehlings et al 11 and Kato et al 10 were centered around outcomes after adult deformity surgery. These outcomes were reported with respect to LEMS, where a major decline was defined as a loss of more than 5 points, as this correlated to a deficit in 3 or more myotomes for 90% of the major decline group. 10 The aforementioned deficits were assessed at various time points postoperatively and therefore represent outcomes as a result of surgery rather than the natural history of the disease. The ASIA assessment is based on scoring of each key myotome from 0-5 on the MRC scale. The LEMS is the sum of all myotomes in the lower extremities bilaterally – this has been shown to correlate with ambulatory ability. 11
Within tumor-based surgery, six studies provided definitions of ISCI. Each of these studies aimed to demonstrate the role of IONM in spinal cord tumor resection surgery. The definition of ISCI varied from a decrease in McCormick grade, MRC grade or neuromonitoring signal changes, with periods of assessment ranging from immediately postoperatively to outpatient follow up. The McCormick grade defines a patient’s neurological impairment based on motor and sensory symptoms and functional status. This was used by Harel, 13 Korn 15 and Sala 17 to define ISCI resulting from spinal tumor resection surgery. Overall, the definition “a new or worsening neurological deficit attributable to spinal cord dysfunction during spine surgery that is diagnosed intra-operatively via neurophysiologic monitoring or immediately post-operatively based on clinical assessment” settled on for the purposes of this review is based on a combination of the studies included in this review and GDG recommendations. This definition encompasses both the role of IONM and the clinical impact on the patient. The true impact of an ISCI is dependent on how the SCI affects the patient clinically; therefore, while the definition of ISCI relates to changes in neuromonitoring, further investigation is required to determine how IONM signals translate to clinical findings. Additionally, the review identified the most commonly used threshold for IONM indicative of ISCI as loss of 50% or more signal on IONM. The above-mentioned definition was reviewed by the GDG in the context of evidence collected from the scoping review. Changes were proposed and voted upon, in accordance with the Delphi Process. The use of wake-up test to detect ISCI was added to the definition as it was proposed that IONM is not readily available across the globe. This change was upheld after the voting process.
Based on the knowledge synthesis and a Delphi-based approach with the GDG, the following definition of Intraoperative Spinal Cord Injury was proposed: “a new or worsening neurological deficit attributable to spinal cord dysfunction during spine surgery that is diagnosed intra-operatively via neurophysiologic monitoring or via wake-up test, or immediately post-operatively based on clinical assessment”.
Frequency of ISCI
The frequency of ISCI varied across pathology and spinal level, as seen in Table 3. The data from this review suggested that the frequency of ISCI may be greater in tumor surgery with a range of 0-61% and persistent deficits up to 27%. 16 Of the 13 studies reporting on tumor surgery and IONM, one reported exclusively on extradural tumors (frequency of 1.97% with post-operative deficits), three on intradural extramedullary tumors (up to 16.5% with post-operative deficits), five on intramedullary tumors (up to 71.4% with ISCI) and the remainder on tumors in varied locations. This higher frequency of ISCI could be due in part to pre-existing deficits resulting from tumors within or abutting the cord.23,25,26
Risk Factors of ISCI
The most commonly reported risk factors identified in this systematic review included older age, male sex, hypertension, pre-operative neurological status, blood loss, higher BMI, and number of spinal levels operated on. Older age, male sex, hypertension, combined myelopathy, blood loss, ponte-osteotomy, DAR, and curve magnitude were identified as factors with a statistically significant increased risk of ISCI. A better pre-operative neurological status and use of IONM were identified as factors associated with a significantly decreased risk of ISCI.
One of the most commonly cited risk factors was a decreased preoperative neurological status that can be considered evidence of preoperative spinal cord dysfunction. 21 This can be attributed to the fact that a damaged cord is considered more vulnerable (or potentially “with less reserve”) to further insult. 19 Furthermore, it is possible that tumors result in intrinsic cord damage and that patients undergoing surgical resection may have more deficits preoperatively. These preoperative deficits may therefore increase the risk of ISCI as the spinal cord may be more susceptible to ischemia (on top of the obvious fact that the surgical approach often requires dissection through parts of the spinal cord that may be unaffected preoperatively).
The frequency of deficits differed by spinal level, with the lumbar spine representing the greatest frequency of ISCI. Some literature has suggested that the sparse blood supply in the thoracolumbar region may contribute to the relatively increased risk of ischemia and subsequent increased frequency of ISCI in this region. 26 Importantly, while the lumbar region has the highest reported frequency of ISCI, studies have identified a potential for injury to the cord during surgery at all spinal levels. Additionally, while injury at a lumbar spinal level may not, in the strictest definition, mean injury to the lumbar spinal cord but rather to the cauda equina (ie, nerve root injury), for the purpose of this review, it was considered as ISCI as the etiology of the injury was still iatrogenic during spine surgery.
Several mechanisms have been suggested to describe the etiology of ISCI. Studies have proposed that injury is the result of direct mechanical trauma to the cord or from spinal cord ischemia.27,28 Mechanical trauma can result from the placement of instrumentation or compression from surrounding structures such as the ligamentum flavum or the intervertebral disc. Vitale et al also discussed the implications of ischemia on ISCI and demonstrated that those with cardiopulmonary comorbidities were more likely to sustain ISCI as detected by IONM. This finding was not reported by the studies assessed in our scoping review – however, blood loss was described as a risk factor for ISCI in two studies and may potentially be a surrogate for cord perfusion. 28 Additionally, Zhang et al showed that pulmonary function had an increased risk of ISCI (although not significant). 23
Older age was also reported as a risk factor for ISCI, presumably due to both the increased likelihood of postoperative complications and because of decreased neural tissue resilience with age. 19 Depression and CCI were associated with an increased, but non-significant, risk of ISCI. Hypertension showed a positive association with ISCI in one study but not another. As such, while this scoping review has identified several risk factors of ISCI, there was not enough evidence to establish the association between patients, surgical and disease characteristics, and risk of ISCI. Further, it is not feasible to interpret age and co-morbidities in isolation as risk factors of ISCI, as these factors are related to each other. In future studies, authors could evaluate the association of frailty and risk of ISCI, as frailty index includes age as well as co-morbidities and can serve as a more comprehensive parameter.
Importantly, Kim et al reported a significant negative association between ISCI and the use of IONM (OR .14, P = .003). 20 Specifically, this finding indicates that when IONM was used during surgery, the risk of ISCI was significantly decreased. Use of IONM is a modifiable factor unlike many other factors such as age and co-morbidities. IONM can detect ISCI in real time during surgery, which can notify the surgical team to take actions to minimize or even reverse the deficit when still possible. 23
The curve magnitude and DAR ratios were identified as high-risk factors for ISCI. More significant deformity can result in kinking or stretching of the cord and alter its hemodynamic supply. 23 These surgeries are naturally associated with a higher risk of ISCI due to direct manipulation of the neural elements, acute change in spinal canal alignment, the use of extensive spinal instrumentation and vascular insufficiency from stretch of the anterior spinal artery or over-shortening of the spinal column.1,2,13 Male sex was also shown to be a risk factor by three of the included studies. Chen et al attributed this to a potential protective effect of estrogen and progesterone in female patients. 19 Not all studies, however, reported a statistically significant association between sex and ISCI.
There are several limitations to this knowledge synthesis. Firstly, the majority of the studies available on this topic were rated as low quality. As there was previously no single definition, method, or criteria to define ISCI, there is variation in the reported frequency and risk factors of ISCI. Further, it is possible that not all included studies documented neurological score preoperatively using standard grading methods. There are also several strengths to our review. It is the first comprehensive and systematic knowledge synthesis that evaluates the frequency and risk factors of ISCI and provides a uniform definition. The methods used to conduct the knowledge synthesis were rigorous and abided by current standards. Additionally, the quality of the studies included was ascertained and reported. Specifically, the definition was thoroughly reviewed, debated, and voted upon by the GDG after the scoping review, and was formed after a unanimous vote, following the Delphi Process.
In summary, a comprehensive definition of ISCI was provided using the evidence gathered in this knowledge synthesis and input from GDG. This standardization of nomenclature for ISCI will enable future studies to better quantify the incidence of major neurological deficits, identify relevant risk factors and assess treatment protocols for ISCI management. Furthermore, by combining the results on risk factors with the frequency data, and recommendations by GDG, this review identified a subset of patients at “higher risk” for ISCI. These patients include older patients, those with high grade tumors causing compression, severe rigid deformity requiring multiple osteotomies, or structural pathologies causing myelopathy (eg, OPLL) and those undergoing revision surgery.
While, in theory, the risk of ISCI can never be eliminated, there can be strategies developed to mitigate and minimize it. This further raises the question of the role of IONM, management strategies in the event of loss on IONM, and a potential care pathway to mitigate the adverse event.
Conclusion
After a comprehensive mixed-methods knowledge synthesis and expert opinion input using the Delphi Method, a consensus-based definition for ISCI was developed. It has been identified that most studies have reported that a decrease of 50% or more on IONM parameter can be considered indicative of ISCI. Additionally, several clinical, surgical, and radiological risk factors for ISCI have been identified. The results synthesized in this manuscript will supplement clinicians’ knowledge of the frequency and risk factors for ISCI in order to inform decision making regarding prevention and management strategies. A uniform, consensus-based definition of ISCI will also aid in optimizing future research on this topic. Additionally, this review further raises the question of the role of IONM, management strategies in the event of an IONM alert, and a potential care pathway to manage ISCI.
Supplemental Material
Supplemental Material - Definition, Frequency and Risk Factors for Intra-Operative Spinal Cord Injury: A Knowledge Synthesis
Supplemental Material for Definition, Frequency and Risk Factors for Intra-Operative Spinal Cord Injury: A Knowledge Synthesis by Michael G. Fehlings, Ayesha Quddusi, Andrea C. Skelly, Erika D. Brodt, Ali Moghaddamjou, Anahita Malvea, Nader Hejrati, Nisaharan Srikandarajah, Mohammed Ali Alvi, Shay Stabler-Morris, Joseph R. Dettori, Lindsay A. Tetreault, Nathan Evaniew and Brian K. Kwon in Global Spine Journal
Footnotes
Acknowledgments
MGF is supported by the Robert Campeau Family Foundation/Dr. C.H. Tator Chair in Brain and Spinal Cord Research at UHN. BKK is the Tier I Canada Research Chair in Spinal Cord Injury and the Dvorak Chair in Spinal Trauma. NH acknowledges support by the Research Fund of the University of Basel for Excellent Junior Researchers. The authors wish to thank the following for contributions to this work: Shelby Kantner (literature search). This Focus Issue was reviewed by the Joint Guidelines Review Committee of the American Association of Neurological Surgeons and Congress of Neurological Surgeons as well as the North American Spine Society. However, this review process does not constitute or imply endorsement of this work product by these organizations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by the AO Foundation, AO Spine and Praxis Spinal Cord Institute. This work was supported by the jointly organized and funded by AO Foundation through the AO Spine Knowledge Forum Spinal Cord Injury (SCI) (www.aospine.org/kf-sci), a focused group of international SCI experts, and the Praxis Spinal Cord Institute (![]() ) through funding from Western Economic Diversification Canada. The funding bodies did not control or influence the editorial content of the articles or the guidelines process. Methodologic and analytic support for this work was provided by Aggregate Analytics, Inc, with funding from the AO Foundation and Praxis Spinal Cord Institute.
) through funding from Western Economic Diversification Canada. The funding bodies did not control or influence the editorial content of the articles or the guidelines process. Methodologic and analytic support for this work was provided by Aggregate Analytics, Inc, with funding from the AO Foundation and Praxis Spinal Cord Institute.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.