
Abstract
Study Design
Protocol for the development of clinical practice guidelines following the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) standards.
Objectives
Acute SCI or intraoperative SCI (ISCI) can have devastating physical and psychological consequences for patients and their families. The treatment of SCI has dramatically evolved over the last century as a result of preclinical and clinical research that has addressed important knowledge gaps, including injury mechanisms, disease pathophysiology, medical management, and the role of surgery. In an acute setting, clinicians are faced with critical decisions on how to optimize neurological recovery in patients with SCI that include the role and timing of surgical decompression and the best strategies for hemodynamic management. The lack of consensus surrounding these treatments has prevented standardization of care across centers and has created uncertainty with respect to how to best manage patients with SCI. ISCI is a feared complication that can occur in the best of hands. Unfortunately, there are no systematic reviews or clinical practice guidelines to assist spine surgeons in the assessment and management of ISCI in adult patients undergoing spinal surgery. Given these limitations, it is the objective of this initiative to develop evidence-based recommendations that will inform the management of both SCI and ISCI. This protocol describes the rationale for developing clinical practice guidelines on (i) the timing of surgical decompression in acute SCI; (ii) the hemodynamic management of acute SCI; and (iii) the prevention, identification, and management of ISCI in patients undergoing surgery for spine-related pathology.
Methods
Systematic reviews were conducted according to PRISMA standards in order to summarize the current body of evidence and inform the guideline development process. The guideline development process followed the approach proposed by the GRADE working group. Separate multidisciplinary, international groups were created to perform the systematic reviews and formulate the guidelines. All potential conflicts of interest were vetted in advance. The sponsors exerted no influence over the editorial process or the development of the guidelines.
Results
This process resulted in both systematic reviews and clinical practice guidelines/care pathways related to the role and timing of surgery in acute SCI; the optimal hemodynamic management of acute SCI; and the prevention, diagnosis and management of ISCI.
Conclusions
The ultimate goal of this clinical practice guideline initiative was to develop evidence-based recommendations for important areas of controversy in SCI and ISCI in hopes of improving neurological outcomes, reducing morbidity, and standardizing care across settings. Throughout this process, critical knowledge gaps and future directions were also defined.
Introduction
Spinal cord injury (SCI) can be life-altering and result in significant motor, sensory and autonomic dysfunction. 1 The management of patients with SCI begins at the site of the trauma and requires careful triage by trained emergency responders. The spinal column should be promptly immobilized with the use of a backboard, rigid cervical collar, and supportive blocks in order to reduce motion of the spine and prevent further damage to the spinal cord. 2 Patients should then be immediately transferred to specialized trauma centers and started on medical therapies that reduce secondary injury and offer neuroprotection. 2 Hemodynamic management may be important in the early stages of SCI in order to optimize blood flow to tissue surrounding the primary injury that is at risk of infarction. 3 The injured spinal cord is particularly susceptible to systemic hypotension due to impaired vascular reactivity and loss of auto-regulation. The next step in the management of SCI is assessing whether a patient would benefit from surgical decompression and, if so, how quickly should it be performed. 4 Finally, individuals with SCI will require intensive rehabilitation for 12 to 18 months in order to promote neurological recovery, optimize functional status, prevent secondary complications, and provide a routine for long-term maintenance of health. 5 It is imperative to standardize care at every stage of patient management in order to enhance outcomes and improve quality of life. Less commonly, SCI can occur intraoperatively and result from any direct or indirect insult to the spinal cord during induction of anesthesia or patient positioning or as a result of surgical maneuvers or interventions. Intraoperative spinal cord injury (ISCI) is an inherent risk of any spine surgery and can have devastating physical and psychological consequences for patients and their families. Early recognition of intraoperative spinal cord dysfunction through the use of electrophysiologic techniques is essential in order to implement appropriate management strategies that can minimize neurological damage. The management of both SCI and ISCI requires significant health care resources in the form of high-level acute care as well as long-term complication management, and can place substantial financial burden on patients, families, and institutions. 6 Given the individual and societal impact of SCI, it is critical to establish recommendations in order to standardize care from the scene of the injury through to post-hospital rehabilitation.
Clinical practice guidelines (CPGs) are statements which include recommendations intended to optimize patient care that are informed by a systematic review of the literature and an assessment of the benefits and harms of alternative options.7,8 The main objectives of CPGs are to (i) synthesize and translate the highest quality of evidence into practice recommendations; (ii) optimize treatment outcomes and reduce the use of any harmful or unnecessary interventions; (iii) establish standard of care and reduce inappropriate practice variations; (iv) facilitate shared decision making among physicians, patients, and caregivers; and (v) assist policy makers in their decisions about the allocation of health care resources. 9 In contrast, CPGs are not intended to replace clinical judgement or experience, be the sole source for management decisions, influence reimbursement policies, or be used for performance measures or legal precedents.8,10,11 Quality care of patients with SCI and ISCI requires the use of CPGs that combine the highest level of evidence with clinical expertise and patient preferences. It is also imperative that CPGs are periodically reviewed for relevance and updated when new evidence emerges on benefits and harms that may impact recommendations and practice.
The treatment of SCI has drastically evolved over the last century as a result of preclinical and clinical research that have addressed important knowledge gaps, including injury mechanisms, disease pathophysiology, medical management, and the role of surgery. There have been previous CPGs, published by the American Association of Neurological Surgeons (AANS) and AO Spine, that aim to provide recommendations on key components of the management of SCI, including prehospital immobilization, the role of methylprednisolone, cardiopulmonary, and hemodynamic management, the indications for anticoagulation, the utility of magnetic resonance imaging and the timing of surgical decompression.2,3,12-17 It is recommended that CPGs are reviewed by the primary sponsor at three years to a maximum of five years following publication. Further criteria for updating a guideline include changes in (i) the evidence related to harm and benefits; (ii) outcomes which would be considered important for decision-making; (iii) ranking of current critical and important outcomes; and (iv) available interventions and resources. Given the availability of more recent research, a multidisciplinary group of clinicians agreed to update the CPGs on timing of surgical decompression and hemodynamic management of SCI. These updated CPGs will incorporate new evidence that is anticipated to be of higher quality in order to better inform current clinical practice.
Currently, there are no systematic reviews or CPGs to assist spine surgeons in the assessment and management of ISCI in adult patients undergoing spinal surgery. Based on the results of a survey of the AO Spine International community, most surgeons performing spine surgeries do not feel comfortable managing ISCI despite considerable training and experience. 18 Furthermore, 90.6% believed that CPGs for the management of ISCI would be useful and 94.4% reported being either likely or extremely likely to use such CPGs. Given this knowledge gap, there is a pressing need to summarize the existing literature and develop recommendations for the detection and management of ISCI in patients undergoing spinal surgery.
This protocol describes the rationale and proposed methodology for developing CPGs on (i) the timing of surgical decompression; (ii) the hemodynamic management; and (iii) the identification and management of ISCI in patients undergoing surgery for spine-related pathology.
Rationale and Scope
Timing of Surgical Decompression
The first section of this guideline aims to define the role and timing of surgical decompression by comparing neurological outcomes and complications between patients treated ultra-early or early vs late. Urgent surgical decompression remains one of the only treatment options for acute SCI and can help restore blood flow to the spinal cord, improve perfusion to tissue at risk, and limit secondary injury. Preclinical evidence has suggested that early surgical intervention can mitigate neural damage caused by persistent compression of the spinal cord and improve neurobehavioral outcomes.19-21 Similarly, several clinical studies have indicated that early surgical decompression may enhance neurological recovery in patients with acute SCI. 4
Across clinical studies, different time thresholds have been used to distinguish between “early” and “late” surgical decompression. The Spinal Trauma Study Group identified the first 24 hours as the most promising time window during which decompression may afford neuroprotection. 22 In 2017, a CPG was developed by AO Spine to provide evidence-based recommendations for the timing of surgical intervention in patients with SCI, using 24 hours as the cutoff to distinguish early and late decompression. 14 Based on a systematic review of the literature, a weak recommendation was formulated to suggest early surgery be offered as an option for adult SCI patients regardless of injury level. 14 For this recommendation, there was controversy among the guideline development group (GDG) about whether the neurological improvement afforded by early surgery was clinically meaningful for patients with SCI. Other limitations to this guideline included (i) insufficient evidence on the differential effectiveness and safety of early vs late surgery in subpopulations; (ii) limited evidence on the cost-effectiveness of early vs late surgery; and (iii) uncertainty surrounding the impact of early vs late surgery on functional outcomes, disability, and quality of life. Furthermore, the level of evidence in the systematic review was low or very low for the majority of findings that informed the CPG, indicating limited confidence in the estimates of effect.
Since the publication of the 2017 CPG by AO Spine, several studies have emerged that assess the impact of early vs late surgical decompression on various outcomes. Previously, the outcomes that were ranked as critical for decision making included improvement in American Spinal Cord Association (ASIA) motor score, ASIA Impairment Score (AIS) by ≥ 2 grades, functional independence measure (FIM), and spinal cord independence measure (SCIM), as well as adverse events. It is anticipated that these scores will also be considered “critical” in the updated version of the guideline and that there will only be minor changes, if any, to the ranking of outcomes. Importantly, the results of recent studies have the potential to change the strength of previous recommendations and therefore impact clinical decisions.
The 2017 CPG by AO Spine defined early surgery as decompression within 24 hours of injury and eliminated studies that evaluated the impact of “ultra-early” surgery on neurological outcomes. In a study by Wilson et al (2015), the mean time from injury to arrival at a definitive care center was 8.1 ± 25.5 hours, while the mean time to surgery was 49.4 ± 65.0 hours. Moreover, 53.3% of patients underwent surgery within 24 hours from injury, while only 34.2% reached the operating room within 12 hours. Given these findings, a recommendation for surgery within 24 hours of injury was deemed to be more feasible than proposing an even narrower time window. Not surprisingly, an increased number of stops at intermediate health centers was one of the most important predictors of delayed surgical intervention. Given that care pathways for individuals with SCI have become more streamlined in certain settings, it may be possible to intervene more expeditiously, especially if there is proof that “ultra-early” surgery is beneficial. It is therefore the endeavor of this guideline to explore different time cut-offs (e.g., <4, <8 or <12 hours) in order to establish the ideal timing of surgical intervention by considering the balance between benefits and harms, cost-effectiveness, and feasibility.
Hemodynamic Management
The second section of this guideline aims to provide recommendations on the hemodynamic management of acute SCI. A CPG for hemodynamic management is warranted because, aside from surgical decompression, augmenting the mean arterial blood pressure (MAP) is one of the only acute interventions available to clinicians to mitigate further ischemic injury to the spinal cord. Patients with SCI are often managed in an intensive care unit due to increased rates of respiratory insufficiency, cardiac dysfunction and systemic hypotension, and the need for close monitoring. 3 Systemic hypotension in this patient population may occur from a combination of hypovolemia from concomitant hemorrhage and neurogenic shock. Regardless of the cause, hypotension is likely to be deleterious to the vulnerable spinal cord and to the patient in general.
It has been proposed that reduced MAP can significantly affect the spinal cord by decreasing spinal cord perfusion, altering oxygen delivery to vulnerable tissue, and worsening secondary injury. The injured spinal cord is particularly susceptible to systemic hypotension due to impaired vascular reactivity and loss of auto-regulation. Based on a systematic review of the literature by Ryken et al (2013), volume expansion and targeted elevations in blood pressure were thought to improve neurological outcomes and reduce mortality and morbidity in individuals with SCI. 3 The findings of this review led to the development of two recommendations on the hemodynamic management of SCI by the AANS/Congress of Neurological Surgeons (CNS): (i) correct hypotension in SCI (systolic BP<90 mmHg) when possible and as soon as possible and (ii) maintain a MAP between 85 and 90 mmHg for the first 7 days following an injury. 3 There have been challenges in both the interpretation and translation of these guidelines into clinical practice, as well as suggestion that these recommendations may not be appropriate for all patients with SCI.23,24 Given this variability in implementation, revising these guidelines is warranted in order to develop recommendations that are more broadly accepted. Furthermore, since 2013, the literature on hemodynamic management of SCI has grown substantially and standards for developing CPGs have evolved.
In 2020, Evaniew et al (2020) conducted a high-quality systematic review that abided by current methodological standards in order to summarize (i) the impact of goal-directed interventions intended to optimize spinal cord perfusion on neurological recovery and adverse events; and (ii) the impact of monitoring techniques, perfusion ranges, pharmacological therapies, and duration of treatment on neurological recovery and adverse events. 25 This review identified several relevant prospective and retrospective interventional and observational studies that have been published since the development of the 2013 guidelines. 25 This study also highlighted significant limitations of previous systematic reviews on this topic; specifically, no review assessed the risk of bias of included studies or utilized the GRADE (Grading of Recommendations, Assessment, Development, and Evaluations) approach to evaluate the quality of the overall body of evidence. Furthermore, no other reviews have assessed both the impact of MAP and spinal cord perfusion pressure (SCPP) on neurological outcomes.
According to Evaniew et al (2020), the effect of augmenting MAP on neurological recovery was uncertain. 25 This conclusion was based on the results of two large cohort studies that demonstrated (i) motor scores did not differ between patient who received vasopressors and those who did not and (ii) drops in MAP were not associated with changes in ASIA motor scores.26,27 Other included studies identified MAP support as beneficial but had smaller sample sizes and lower MINORS (Methodological Index for Non-Randomized Studies) scores, indicating higher risk of bias. 25 Furthermore, low quality of evidence suggested that vasopressor support of MAP is associated with increased rates of arrhythmias, myocardial injuries, and possible posterior reversible encephalopathy syndrome. 25 These are all factors that must be considered in the approach to hemodynamic management for acute SCI, and justify revisiting the 2013 guidelines that recommended a MAP target of 85–90 mmHg for 7 days. Interestingly, SCPP may result in improved neurological outcomes based on the AIS. 25 However, evaluating SCPP via intradural catheters represents an invasive monitoring technique with the potential for cerebrospinal fluid (CSF) leak or meningitis. In developing recommendations, it is important to review the strength of evidence supporting the potential benefit of augmenting MAP or SCPP, consider the risks of each approach and evaluate the feasibility and cost-effectiveness of these treatments. A GRADE approach is required to translate this evidence into recommendations that not only incorporate the scientific literature that has become available since the last guideline was published, but also considers multi-disciplinary clinical expertise as well as the perspectives of other key stakeholders. As acute hemodynamic management of SCI is within the purview of many specialties (e.g., anesthesia, intensive care, surgery, rehab medicine), a process that engages these different disciplines is needed to develop truly relevant and applicable guidelines.
Intraoperative Spinal Cord Injury
The third section of this guideline aims to provide recommendations to assist spine surgeons in anticipating, preventing, diagnosing, and managing ISCI. Although ISCI is uncommon, it is an inherent risk to any spine surgery and can have devastating physical and psychological consequences for patients and their families.28-30 Furthermore, an ISCI can impose significant financial costs on a patient, surgeon, as well as an institution and may have severe legal repercussions. 31 This topic was identified as a key priority for guideline development by an international survey of key stakeholders. 18 ISCI results from any direct or indirect physiologic insult to the spinal cord, conus medullaris, or cauda equina during surgery, causing temporary or permanent motor, sensory, or autonomic impairment. Proposed mechanisms of ISCI include direct trauma or contusion to the spinal cord, compression of the neural elements by an epidural hematoma or abscess (typically delayed), and spinal cord ischemia secondary to systemic hypotension or from deformity reduction or correction maneuvers. 31 Furthermore, given the organization of ascending and descending tracts in the spinal cord, postoperative sensory deficits are more likely secondary to direct trauma to the dorsal columns, whereas motor deficits are more likely from spinal cord ischemia and decreased blood flow through the anterior spinal artery.32,33
The estimated incidence of ISCI is between 12 and 57 cases per million and varies depending on underlying spinal pathology, regions of involvement, surgical approach, and preoperative neurological deficits.31,34 Definitions of ISCI vary across studies and range from quadriplegia to an isolated radiculopathy. Some studies distinguish between nerve root injury and SCI, while others do not and simply report postoperative AIS or Frankel Grades. 35 There is a pressing need to standardize nomenclature for ISCI in order to better quantify the incidence of major neurological deficits, identify relevant risk factors, implement appropriate preventative strategies, and develop useful and reliable protocols for ISCI management. Furthermore, the variability in the reported incidence of ISCI may be partially attributed to heterogeneity in definitions across studies as well as differences in study design and data collection methods. 36 Unifying nomenclature and proposing a specific definition for ISCI is an important objective of the guideline development process.
Intraoperative neuromonitoring (IONM) during spine surgery can assess the integrity of the sensory and motor tracts and detect ISCI at a time when action can be taken.37,38 IONM has enabled complete resections of spinal cord tumors and more aggressive surgeries for correction of severe and rigid spinal deformities.37,39 Somatosensory evoked potentials (SSEPs) evaluate the functional integrity of sensory pathways from the peripheral nerve to the somatosensory cortex via the dorsal column-medial lemniscus; this posterior tract is more likely to be injured from direct trauma. 40 On the other hand, motor evoked potentials (MEPs) can assess the function of the anterior two thirds of the spinal cord and are useful for detecting damage secondary to spinal cord ischemia.33,37 Finally, electromyography (EMG) can be used to provide real time information about selective nerve function. 40 According to a systematic review by Fehlings et al (2010), the sensitivity of SSEPs, transcranial MEPs (tcMEPs), and EMG for detecting ISCI are 0–100%, 81–100%, and 46%, respectively, while the specificities are 27–100%, 81–100%, and 73%. 38 Based on this systematic review, there is very low evidence that SSEPs or MEPs in isolation are valid diagnostic tests for detecting ISCI during spinal surgery. 38 The diagnostic accuracy of unimodal IONM for identifying injury to the motor or sensory pathways, however, may be higher in certain populations such as intradural spinal cord tumors (SSEPs: sensitivity 94.4%, specificity 96.8%; MEPs: sensitivity 95%, specificity 98.9%). 41 Multimodal IONM (MIONM) has also gained popularity and is now often used in the operating room due to its higher sensitivity (70–100%) and specificity (52.7–100%) for detecting ISCI.38,42 While there is consensus that IONM improves outcomes in spinal deformity and oncology cases, there is still controversy with respect to the utility and cost-effectiveness of IONM in other populations such as cervical myelopathy or radiculopathy.43,44 The controversy surrounding the decision to use IONM may also stem from the fact that there is only low level of evidence to suggest that IONM reduces the rate of new or worsening neurological deficit. 38 The results of published systematic reviews should be combined in order to summarize the diagnostic accuracy of IONM and determine when these techniques should be utilized during spine surgery.
Identifying individuals who are at higher risk for ISCI is essential in order to (i) better inform patients during consent discussions, (ii) establish necessary IONM strategies, and (iii) discuss contingency plans with the surgical and anesthesia teams in the event of an IONM alert. Several studies have evaluated risk factors for ISCI in patients undergoing spine surgery for various pathologies. These factors include the presence of preoperative neurological deficits, revision or previous spinal surgery, degree of spinal deformity, surgical technique, number of operated levels, operative duration, estimated blood loss, age, gender, co-morbidities, and body mass index.29-31,39,45-47 A systematic review is required to summarize the available evidence on important risk factors for ISCI and determine which populations require closer IONM.
Although IONM allows surgeons to detect potential neurological deficits, it is the response to these alerts that influences outcomes. 38 IONM can define the nature of the injury and help the surgical team decide whether the surgery can be safely continued.37,38 There is variation across studies in terms of IONM warning criteria. Typically, a decrease in the amplitude of SSEPs or MEPs by 50% or an increase in latency by 10% are consistent with spinal cord compromise; however, thresholds of 75% to 80% for amplitude reductions have also been reported.37,48,49 Intraoperative checklists have been developed to guide the surgical team’s response to an IONM alert and often include ensuring the IONM system is functioning, confirming the change is not secondary to anesthetic agents, increasing the MAP, decreasing or removing traction weights, administrating methylprednisolone, lidocaine, fluids or warm saline, transfusing blood products and adjusting hardware, screws, and rods.33,37,48,49 Unfortunately, these checklists vary across institutions and there is no consensus in terms of how to approach a potential ISCI. Given these knowledge gaps, a further review of the literature and the development of a CPG is needed to outline strategies for responding to an IONM alert.
Purpose of the Guideline
The main objective of this guideline is to provide evidence-based recommendations on how to best manage patients with SCI and ISCI in order to improve outcomes, minimize permanent injury, and reduce mortality. Specific objectives of this guideline include (i) determine the ultimate timing of surgical decompression; (ii) define specific MAP targets and the duration of MAP augmentation therapy; and (iii) unify the definition of ISCI, define the diagnostic accuracy of IONM techniques, delineate risk factors of ISCI, and propose treatment algorithms for the management of potential ISCI.
Specific Scope of the Guideline
Patient Population
This guideline on timing of surgical decompression and hemodynamic management is to be applied in the acute phases of management in adult patients with acute SCI. The guideline on ISCI is to be used in adolescent or adult patients undergoing spine surgery for any spine-related pathology, including infection, trauma, malignancy, deformity, or degenerative disease.
Definitions
The following definitions are important to understanding the scope of all three guidelines: • • • • • • • • • • • • • • • • • • • The • A • • • • • • • • • • • • • • • • •
Specific conditions that • SCI in children or adolescents (i.e., those under 18 years of age). • ISCI in children less than 11 years of age. • Chronic SCI, defined as persistence of paralysis for ≥12 months following injury. • Patients without neurological deficit following trauma. • Cord compression due to tumor, hematoma, infection, or degenerative disease. • Inflammatory or infectious myelopathies. • ISCI secondary to compression by hematoma or abscess in the postoperative period. • ISCI in patients undergoing surgical procedures distant from the spinal column and cord (e.g., vascular surgery). • Patients with intraoperative neurological deficits attributed to intracranial pathology (e.g., stroke).
Aspects of Care Covered by Guideline
The following specific treatments or aspects of care are addressed in this guideline: • Timing of surgical decompression in patients with acute SCI. • Hemodynamic management of patients with acute SCI • Specify MAP targets and duration of therapy. • Identification and management of ISCI in patients undergoing spine surgery for any spine-related pathology, including infection, trauma, malignancy, deformity, or degenerative disease. • Standardize definitions of ISCI. • Define the diagnostic accuracy of IONM for identifying ISCI and outline specific warning criteria in terms of changes in amplitude and latency of SSEPs and MEPs. • Identify important risk factors for ISCI. • Develop treatment algorithms and evidence-based recommendations on the management of potential ISCI.
Specific treatments or • Use of methylprednisolone within 8 hours of injury as per the NASCIS 2 protocol. • Specific surgical methods for decompression or stabilization of the spine. • Role of neuroimaging in diagnosing SCI or ISCI, developing management strategies or predicting outcomes. • Utility of neural prosthetics, cell therapy, or spinal cord stimulators. • Impact of physical, speech, and respiration therapy on outcomes following SCI or ISCI. • Direct and indirect costs of SCI or ISCI. • Long-term neurological, functional, and quality of life outcomes in patients with ISCI.
Users and Settings
This guideline will facilitate shared decision-making among patients, surgeons, and other healthcare practitioners based on the best available evidence. It is intended to be used by the wide range of clinicians who provide care for patients with SCI or ISCI. Such providers include: • Pre-hospital providers (e.g., paramedics) • Emergency department physicians • In-hospital primary care physicians (e.g., internal medicine, primary care) • Critical care physicians, including subspecialists in neurocritical and trauma care • Surgeons with expertise in spinal surgery (e.g., neurosurgeons, orthopedic surgeons, trauma surgeons) • Spinal cord rehabilitation specialists (i.e., physicians with board certification in SCI Medicine) • Anesthesiologists • Other physician groups who may be consulted to care for these patients (e.g., hematologists, vascular surgeons, pain management specialists) • Allied Health Care providers • Nurses • Other stakeholders (e.g., insurers, regulators, legislative decision makers, hospital administration)
This guideline is applicable in the following settings: • Outpatient Spine Surgery Practice (to facilitate discussions with patients on the risks and benefits of the proposed surgery) • Site of Trauma and On Route to Trauma Center • Emergency Department • Operating Room • Post-Anesthesia Recovery Unit • Intensive Care Unit • Inpatient Wards
Implementation
Although the evidence-base regarding the effective implementation of CPGs is incomplete, a multipronged approach is generally recommended. Such an approach must include efforts on both a macro (i.e., internationally, nationally, major professional groups) and micro level (i.e., hospital or health care facility, individual health care providers) and must consider the availability of necessary resources (i.e., financial, human, materials) as well as patient values and preferences.
This guideline focuses on the management of SCI and is expected to inform practice based on the best available evidence. It is also expected to facilitate shared decision-making between patients and clinicians, minimize morbidity associated with acute SCI and optimize treatment outcomes. Dissemination of the guidelines will be accomplished at multiple levels: • Through influential groups and opinion leaders across stakeholder groups (The International Spinal Cord Society, AANS, American Spinal Injury Association, CNS, Academy of SCI Professionals, Canadian Spine Society, Neurocritical Care Society, Wings for Life, Craig Neilsen, Praxis, World Federation of Neurosurgical Societies, North American SCI Consortium, European Association of Neurological Societies, Christopher Reeve Foundation. etc.) • Guideline review at international meetings • Publication as a focus issue in the Global Spine Journal • Advertisement on various stakeholder websites • AO Spine Core Competency/Curriculum • Webinars to target broader audiences (consider taping any formal presentations made at professional meetings) • Submission to Emergency Care Research Institute (https://www.ecri.org/) for dissemination of these guidelines.
Summary of Contents
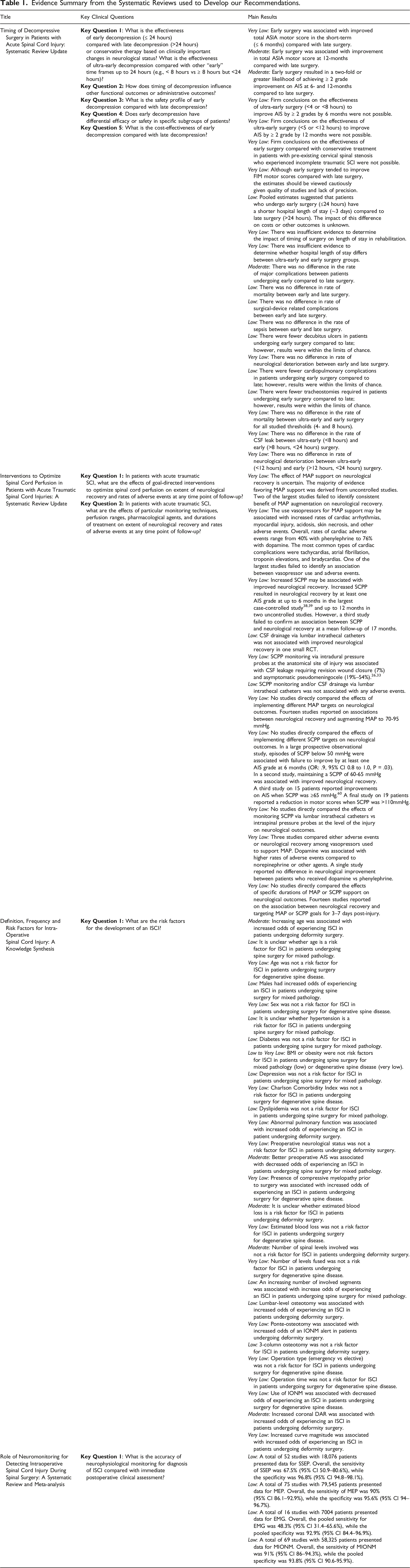
Evidence Summary from the Systematic Reviews used to Develop our Recommendations.
Timing of Surgery
Hemodynamic Management
Intraoperative Spinal Cord Injury
Footnotes
Acknowledgments
MGF is supported by the Robert Campeau Family Foundation/Dr. C.H Tator Chair in Brain and Spinal Cord Research at UHN. BKK is the Canada Research Chair in Spinal Cord Injury and the Dvorak Chair in Spinal Trauma. This Focus Issue was reviewed by the Joint Guidelines Review Committee of the American Association of Neurological Surgeons and Congress of Neurological Surgeons as well as the North American Spine Society. However, this review process does not constitute or imply endorsement of this work product by these organizations.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by the AO Foundation, AO Spine and Praxis Spinal Cord Institute. This study was jointly organized and funded by AO Foundation through the AO Spine Knowledge Forum Spinal Cord Injury (SCI) (www.aospine.org/kf-sci), a focused group of international SCI experts, and the Praxis Spinal Cord Institute (![]() ) through funding from Western Economic Diversification Canada. The funding bodies did not control or influence the editorial content of the articles or the guidelines process. Methodologic and analytic support for this work was provided by Aggregate Analytics, Inc, with funding from the AO Foundation and Praxis Spinal Cord Institute.
) through funding from Western Economic Diversification Canada. The funding bodies did not control or influence the editorial content of the articles or the guidelines process. Methodologic and analytic support for this work was provided by Aggregate Analytics, Inc, with funding from the AO Foundation and Praxis Spinal Cord Institute.