
Abstract
Study Design
Prospective observational study.
Objective
To evaluate the predictive value of the preoperative Short Form-36 survey (SF-36) scale for postoperative axial neck pain (ANP) in patients with degenerative cervical myelopathy (DCM) who underwent anterior cervical decompression and fusion (ACDF) surgery.
Methods
This study enrolled patients with DCM who underwent ACDF surgery at author’s Hospital between May 2010 and June 2016.
Results
Out of 126 eligible patients, 122 completed the 3-month follow-up and 117 completed the 1-year follow-up. The results showed that the preoperative social functioning (SF) subscale score of the SF-36 scale was significantly lower in patients with moderate-to-severe postoperative ANP than in those with no or mild postoperative ANP at both follow-up timepoints (P < .05). ACDF at C4-5 level resulted in a higher ANP rate than ACDF at C5-6 or C6-7 level, both at 3-month (P = .019) and 1-year (P = .004) follow-up. Multivariate logistic regression analysis confirmed that the preoperative social functioning subscale score was an independent risk factor for moderate-to-severe postoperative ANP at 3 months and 1 year after surgery, and preoperative NRS was an independent risk factor at 1-year follow-up. No other demographic, clinical, or radiographic factors were found to be associated with postoperative ANP severity (P < .05).
Conclusions
Preoperative social functioning subscale score of SF-36 scale might be a favorable predictive tool for postoperative ANP in DCM patients who underwent ACDF surgery.
Keywords
Introduction
Degenerative cervical myelopathy (DCM) is the most common cause of spinal cord dysfunction, especially in older population. 1 From the etiological point of view, DCM is caused by a chronic cord compression due to a number of degenerative conditions, including spondylosis, cervical disc herniation or ossification of posterior longitudinal ligament.1,2 The natural history of DCM is characterized by stepwise sensory changes, gait abnormalities and muscle weakness. 3
The mainstay of DCM treatment is decompression surgery, including both anterior and posterior approaches. 4 What needs to be emphasized is that anterior cervical decompression and fusion (ACDF) surgery does not destroy the muscles and ligaments of posterior neck, sparing the effect of surgery on axial neck pain (ANP). 5 However, ANP is still a frequently encountered postoperative complication of ACDF surgery, which can be a major cause of dissatisfaction after surgery, even in patients with excellent neurological recovery. 6
Prediction of the postoperative ANP in patients who underwent ACDF surgery has evolved from a simple imaging to a comprehensive evaluation system, but still remains an unsolved clinical problem demanding urgent solution. 7 The 11-point numerical rating scale (NRS) score was shown to directly reflect the pain situation of patients after surgery, 8 but it cannot be used as a prediction tool. On the other hand, Short Form-36 survey (SF-36) scale is currently the most widely used universal quality of life scale, consisting of 8 dimensions, which can be divided into 2 common total scores: physical component score (PCS) and mental component score (MCS). 9 The author’s previous study 5 demonstrated that the preoperative SF-36 scale score is closely correlated with chronic postoperative neck pain, but the results need to be further confirmed.
Therefore, this study aimed to evaluate the predictive value of the preoperative Short Form-36 survey (SF-36) scale for axial neck pain (ANP) in degenerative cervical myelopathy (DCM) patients who underwent ACDF surgery.
Methods
Study Design and Patients
This prospective study enrolled patients with DCM who underwent ACDF surgery at author’s Hospital between May 2010 and June 2016. Patients diagnosed with DCM (commonly confirmed both by a thorough neurological examination and radiographic findings of cervical spinal cord compression on T2-weighted magnetic resonance imaging) were eligible. While, patients who underwent trauma, previous cervical operation, more than 1 level suffered or lost follow up data were excluded. The research protocol was approved by the Institutional Review Board of author’s Hospital, and written informed consents were obtained from all patients.
Procedures
All patients completed the Short Form-36 survey (SF-36) scale before surgery. The SF-36 scale covers 8 subscales: physical functioning, role-physical, bodily pain, general health, vitality, social functioning subscale, role-emotional, and mental health in 2 common total scores: physical component score and mental component score.
Procedure for conventional ACDF surgery and fusion was performed according to the surgery standards. After esophagus, trachea and major vessels of the neck were retracted through a transverse incision, the decompression of the spinal cord and/or nerve roots has been performed. Following decompression, the intervertebral space was filled with allograft cadaveric bone or metal or polymer cage with assistance of Caspar retractor. Other than that, no other intraoperative retractions were used. Once space was filled, it was bridged with the use of a titanium plate and screws. During the operation of the patients included in this study (2010-2016), zero-profile and stand-alone internal fixations were not available in our hospital, so all patients were fixed with titanium plate and screws.
In the perioperative period, the following 2 assessment tools were selected for data collection. The 11-point numerical rating scale (NRS) was used to rate the average intensity of ANP, from 0 as no pain to 10 as worst imaginable pain. Patients were categorized into 2 groups according to NRS score for average intensity of ANP [had no or mild pain (NRS score <4) and had moderate-to-severe pain (NRS score ≥4)]. Assessment data were collected preoperatively, at 3-month follow-up and at 1-year follow-up.
Statistical Analysis
IBM SPSS Statistics 20 (IBM Corp., Armonk, NY, USA) was used to perform data analysis. Continuous data were expressed as mean ± standard deviation (SD) and compared by t test. Categorical data were expressed as n (%), and compared by the Chi-square test. Normality was assessed using the Kolmogorov-Smirnov test. The Mann-Whitney U test was used for nonparametric data. Multivariate logistic regression was used to evaluate the associations between baseline SF-36 scale scores and the moderate-to-severe postoperative ANP at 3 months and 1 year of follow-up. A P-value <.05 was considered as statistically significant.
Results
Patient Distribution at Different Follow-Up Timepoints
Among 132 eligible patients, 2 patients were excluded because of previous cervical operation, and 4 patients excluded because of trauma. Finally, 126 patients were included, with 122 patients completed the 3-month follow-up (follow-up rate: 96.8%), and 117 patients completed 1-year follow-up (follow-up rate: 92.9%) (Figure 1). Flow chart of study identification, inclusion and exclusion.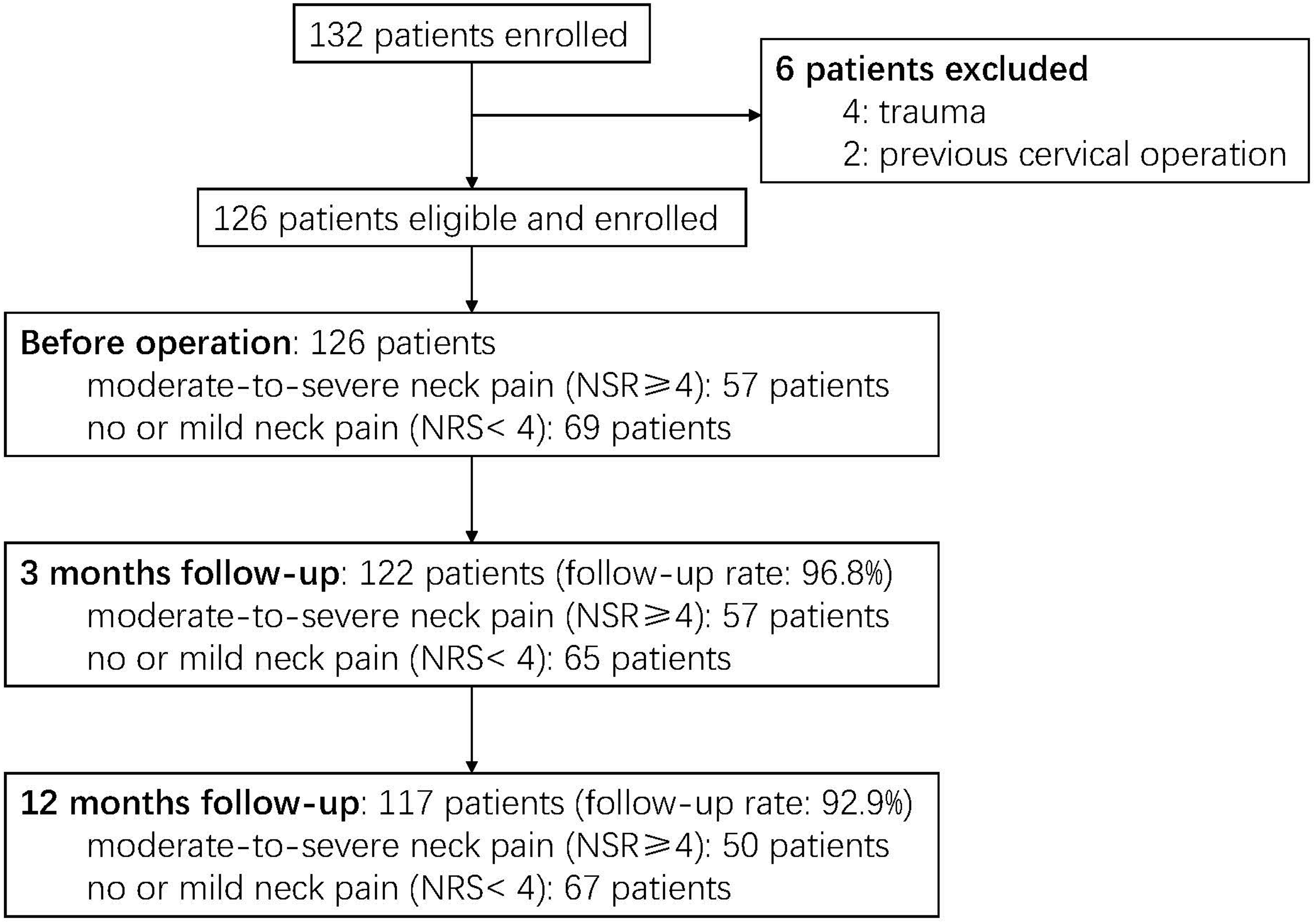
Proportion of Patients Had no or Mild Postoperative ANP and Moderate-to-Severe Postoperative ANP at Different Time Points of Follow-Up.

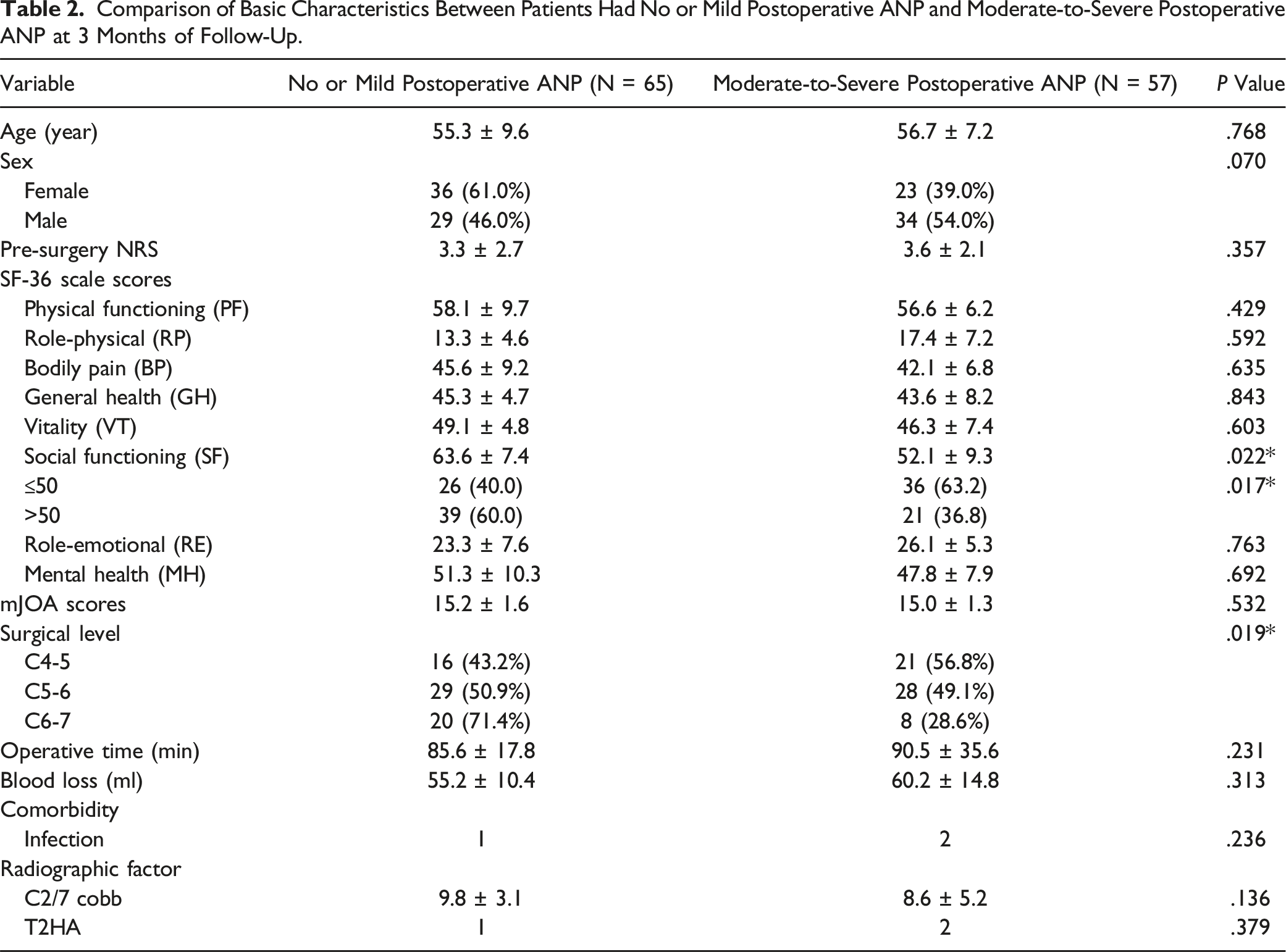
Comparison of Basic Characteristics between no or Mild and Moderate-to-Severe Postoperative ANP Groups at 3-Month Follow-Up
Comparison of Basic Characteristics Between Patients Had No or Mild Postoperative ANP and Moderate-to-Severe Postoperative ANP at 3 Months of Follow-Up.
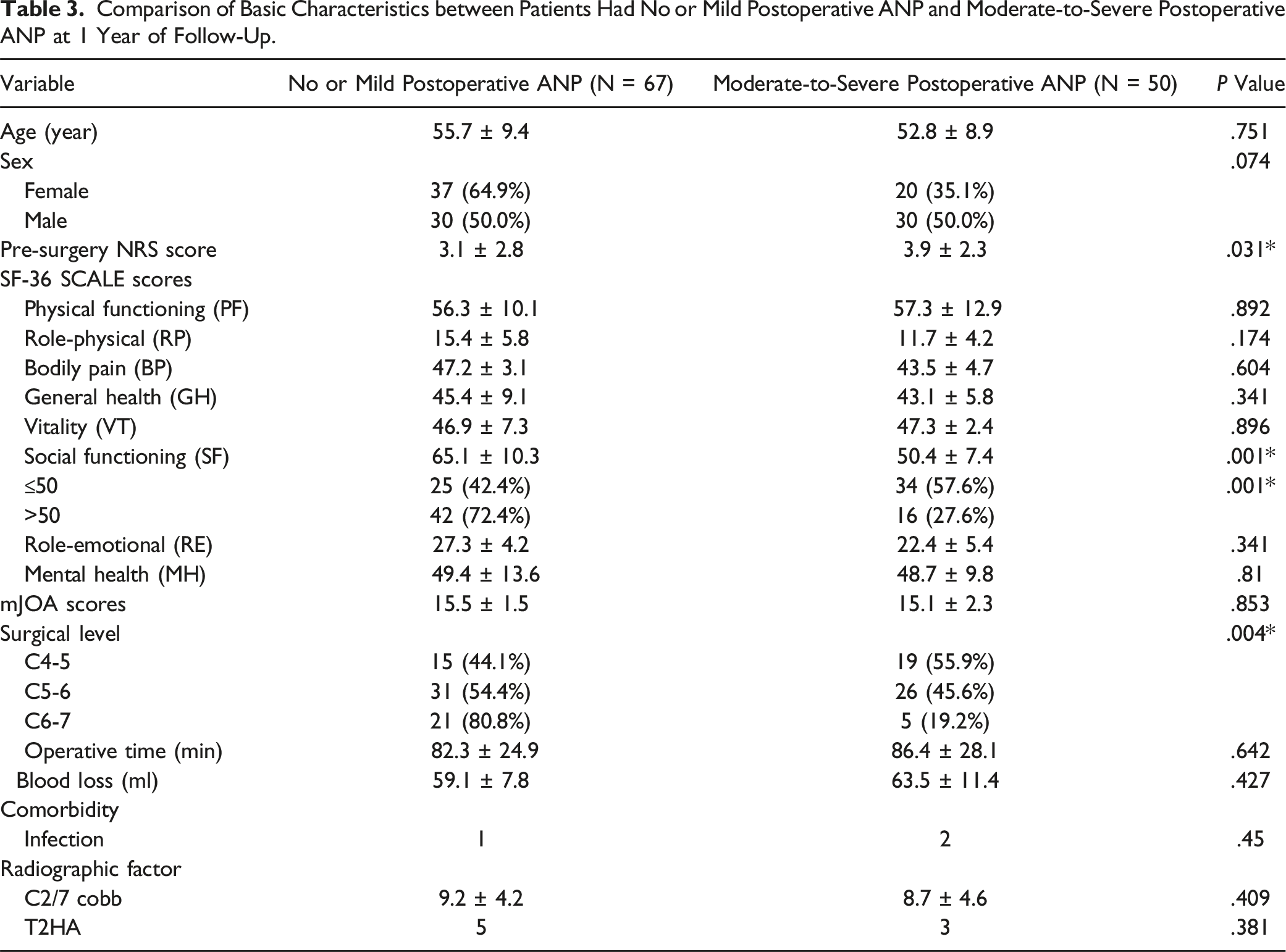
Comparison of Basic Characteristics between no or Mild and Moderate-to-Severe Postoperative ANP Groups at 1-Year Follow-Up
Comparison of Basic Characteristics between Patients Had No or Mild Postoperative ANP and Moderate-to-Severe Postoperative ANP at 1 Year of Follow-Up.
Risk Factors for Moderate-to-Severe Postoperative ANP at 3-Month and 1-Year Follow-Up
Risk Factors for Moderate-to-Severe Postoperative ANP at 3 Months of Follow-Up.
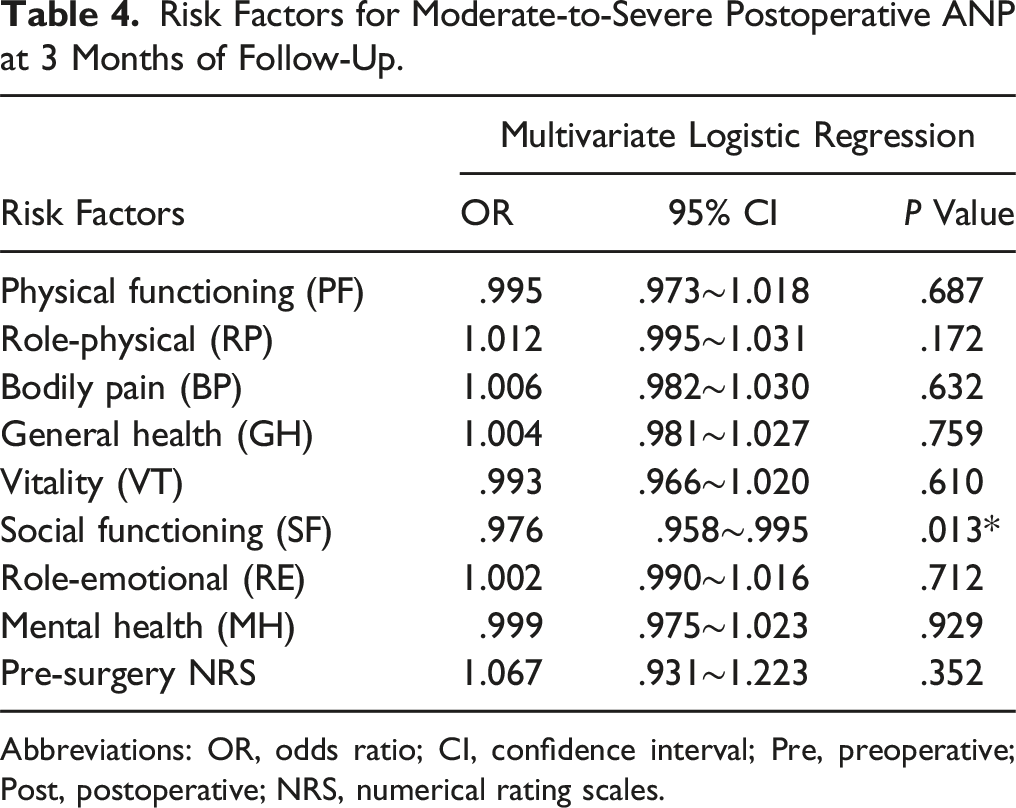
Abbreviations: OR, odds ratio; CI, confidence interval; Pre, preoperative; Post, postoperative; NRS, numerical rating scales.
Risk Factors for Moderate-to-Severe Postoperative ANP at 1 Year of Follow-Up.
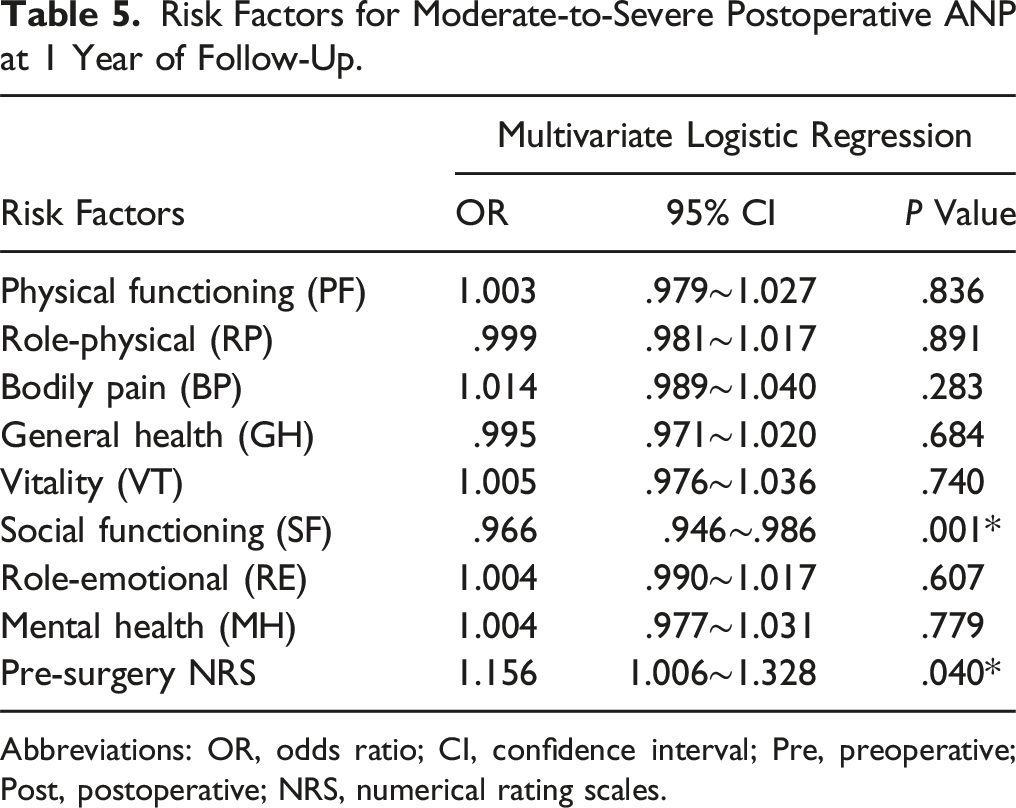
Abbreviations: OR, odds ratio; CI, confidence interval; Pre, preoperative; Post, postoperative; NRS, numerical rating scales.
Discussion
The aim of this study was to identify the predictors of moderate-to-severe postoperative ANP in patients who had anterior cervical spine surgery. Of the 126 patients who met the criteria, 122 were followed up for 3 months and 117 for 1 year. The findings revealed that patients with moderate-to-severe postoperative ANP had significantly lower scores on the social functioning subscale of the SF-36 scale before surgery than those with no or mild postoperative ANP at both follow-up periods. Multivariate logistic regression analysis verified that the score on the social functioning subscale before surgery was an independent predictor of moderate-to-severe postoperative ANP at 3 months and 1 year after surgery. Our results also indicated that the preoperative NRS score was an independent risk factor of moderate-to-severe postoperative axial neck pain in DCM patients, which is consistent with previous studies in this field. Interestingly, we discovered that patients who had ACDF at C4-5 level had a higher rate of ANP than those who had ACDF at C5-6 or C6-7 level, which suggested that the level of fusion affects the likelihood of ANP. Based on our understanding, C4-5 level is more risky than lower levels for several reasons. First, C4-5 level is near the occipital region, where many nerves and muscles are located, so any disturbance or injury to this area may result in more severe or persistent axial pain than lower levels. 10 Second, the C5 nerve root is shorter than other nerve roots. It can be more easily compressed or stretched during or after surgery, which may cause referred pain in the shoulders, upper back, and upper chest. 11 Third, C4-5 level is more prone to degeneration and kyphosis than lower levels, so ACDF at this level may need more correction and stabilization, which can increase the risk of axial pain. 12
This study suggests that patients with lower preoperative social functioning may be more prone to develop moderate-to-severe postoperative ANP after cervical spine surgery. The SF-36 is a widely used and validated instrument that measures health-related quality of life across 8 domains, including physical functioning, role limitations due to physical problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems, and mental health. The SF-36 can be summarized into 2 component scores: the Physical Component Summary (PCS) and the Mental Component Summary (MCS). The SF-36 is a good predictive tool for DCM patients who underwent cervical surgery because it captures the impact of DCM on various aspects of health and well-being, and it has been shown to have a high sensitivity and specificity to detect clinically meaningful changes in DCM patients. 13 Moreover, the SF-36 has been used in previous studies of DCM and has demonstrated good reliability and responsiveness. 14
Importantly, the SF-36 is a reliable tool for the outcome prediction of spinal diseases, as many other articles have mentioned. Oshima et al conducted a study that showed that patients with higher SF-36 MCS scores before surgery had significantly better outcomes after cervical laminoplasty for DCM, including lower neck pain and disability scores, higher physical and mental health scores and satisfaction scores. 15 A study by Ko and Choi that found that preoperative SF-36 MCS scores is a factor that can predict the prognosis of patients who underwent decompression surgery for degenerative lumbar spinal stenosis (DLSS) for at least 1 year postoperatively. 16
Compared to other outcome measures, such as mJOA, NDI, Nurick, and ODI, the SF-36 has some advantages in predicting DCM postoperative outcome. First, the SF-36 is more sensitive to changes in the patient’s condition over time and can capture improvements or declines in quality of life after surgery. Second, the SF-36 is more comprehensive and covers aspects of health that are not addressed by other measures, such as social functioning, role limitations, vitality, and mental health. Third, the SF-36 is more standardized and validated across different populations and settings, and can be compared to normative data from healthy individuals or other patient groups. At last, the SF-36 is more patient-centered and reflects the patient’s own perception of their health status, rather than the clinician’s judgment or objective tests. 17 Other available scales have their own disadvantages, such as ceiling effects, poor sensitivity to changes in mild cases, and cultural bias for mJOA scores; or susceptibility to comorbidities and psychological distress for NDI and Nurick scores. 18
In the past, efficacy evaluation of DCM surgical treatment was mainly based on the improvement degree of neurological dysfunction, like mJOA scores. Many studies have found that patients with DCM can achieve satisfactory intermediate and even long-term neurological outcomes, but still had lower quality of life due to a variety of reasons. 19 Therefore, more attention has been paid recently to the evaluation of quality of life based on patients’ subjective feelings. 20 However, the SF subscale reflects different aspects of social functioning, such as social roles, social networks, and social integration, indicating that it is a valid and reliable measure of social well-being.
Several studies already reported that a number of structural and functional brain alterations independently contribute to the neuropathology of DCM.21,22 In particular, Wang et al 23 demonstrated that DCM patients tend to have long-term functional connectivity reorganization, localized at sensorimotor, regulatory, and visual processing regions of brain. This study included DCM patients who underwent ACDF surgery that preserves the structure and function of posterior neck muscle and ligament, in order to eliminate the influence of damaged anatomical muscle-ligament structure on ANP. In addition, we excluded patients with multilevel anterior cervical surgery because it increased cervical spine rigidity and may have biased our results. This study showed that all items except social functioning subscale score in SF-36 scale remained uncorrelated with NRS score and OR values of them were all statistically insignificant, which made the predictive function of SF-36 scale appear to be monolithic. Obtained results confirm that social functioning subscale in SF-36 scale can be a noteworthy indicator of prefrontal cortex function, which was hypothesized in the previous studies.24,25 Therefore, it could be assumed that prefrontal dysfunction may be linked to surgery outcomes in DCM patients, which need to be further investigated.
Patients with DCM and low preoperative SF scores (less than 50 points) may benefit from early intervention to improve their social functioning and quality of life. At the outset, patient care coordination (PCC) may be an appropriate intervention that focuses on the individual needs, preferences, and values of the patients and their caregivers. It may involve strategies such as assessing the patient’s social history and interests, providing meaningful social activities and choices, respecting the patient’s dignity and privacy, communicating empathically, involving the patient’s family and friends, and educating and supporting the caregivers. 26 Following that, social interventions address the social determinants of health in DCM care and outcomes. They may include strategies such as providing access to equitable and affordable health care, insurance, education, and housing; enhancing patient education and awareness of DCM and its management; and improving linkages between health care systems and the communities. 27 Moreover, a multidisciplinary approach is essential for delivering personalized and comprehensive care to DCM patients, including diagnosis and monitoring by a neurologist, surgery by a neurosurgeon, rehabilitation by a physiatrist, physical therapist, and occupational therapist, pain relief by a pain specialist, and emotional support by a psychologist. 28
This study has following limitations. Firstly, single center study cannot guarantee the representativeness of enrolled patients, and multicenter investigation may improve the quality of data. Secondly, although ANP was defined as the neck pain longer than 3 months, its occurrence could be delayed, explaining the generally low NRS score at 3-month follow-up. Thirdly, the assessment of patients’ health status was limited to psychological components of SF-36 scale. Future studies should include other specific scales designed to assess physiological factors so as to conduct a more comprehensive evaluation. And finally, none of the patients in our study cohort received zero-profile or stand-alone cages for ACDF, because these types of implants were not available in our hospital at that time. Therefore, we used titanium plates and screws to fix the interbody spacers and achieve cervical stability. Zero-profile and stand-alone cages are alternative devices that have been proposed to reduce the risk of dysphagia, implant failure, and adjacent segment degeneration after ACDF. 29 However, their long-term efficacy and safety are still under investigation, which must be added and taken into consideration in future studies.
Future research should explore the mechanisms underlying the association between preoperative SF-36 MCS and postoperative axial neck pain in DCM patients, such as the role of neuroinflammation, central sensitization, and endogenous pain modulation. Future research should also evaluate the effectiveness of interventions that target the psychological aspects of pain management, such as cognitive-behavioral therapy, mindfulness-based stress reduction, and biofeedback. Clinicians should consider using the preoperative SF-36 survey scale as a screening tool to identify DCM patients who may benefit from multidisciplinary pain management programs before and after surgery.
Footnotes
Author Contributions
Rui Chen and Jiesheng Liu carried out the studies, participated in collecting data, and drafted the manuscript. Rui Chen and Jiesheng Liu performed the statistical analysis and participated in its design. Rui Chen, Jiesheng Liu and Feifei Zhou participated in acquisition, analysis, or interpretation of data and draft the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China: The mechanism of hippocampus and prefrontal cortex regulating the chronic outcome of cervical pain after cervical spine surgery (81874023).
Ethical Statement
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.