
Abstract
Study Design
This is a retrospective case-control study.
Objectives
The objectives of this study are to identify (1) risk factors for delayed ambulation following adult spinal deformity (ASD) surgery and (2) complications associated with delayed ambulation.
Methods
One-hundred and ninety-one patients with ASD who underwent posterior-only fusion (≥5 levels, LIV pelvis) were reviewed. Patients who ambulated with physical therapy (PT) on POD2 or later (LateAmb, n = 49) were propensity matched 1:1 to patients who ambulated on POD0-1 (NmlAmb, n = 49) based on the extent of fusion and surgical invasiveness score (ASD-S). Risk factors, as well as inpatient medical complications were compared. Logistic regressions were used to identify risk factors for late ambulation.
Results
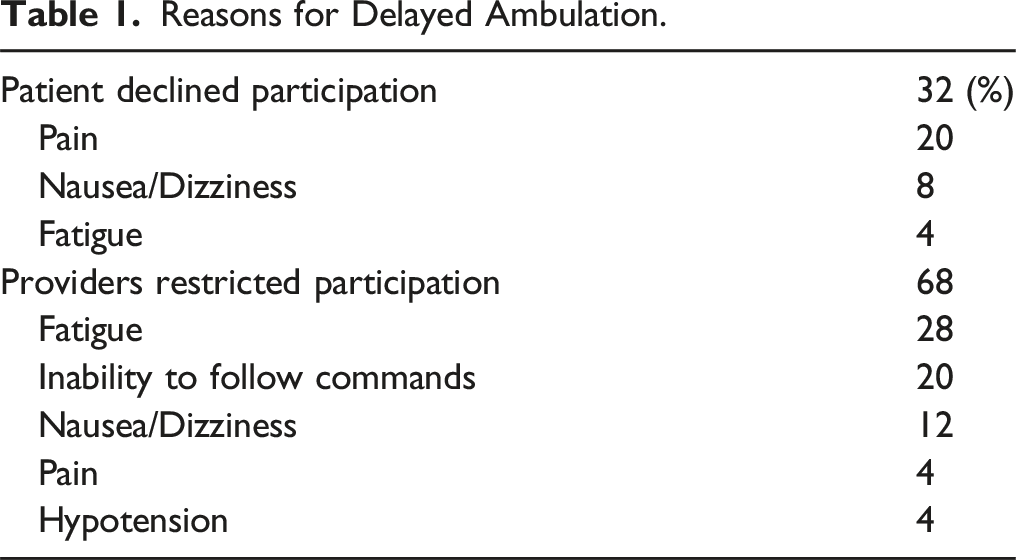
Of the patients who did not ambulate on POD0-1, 32% declined participation secondary to pain or dizziness/fatigue, while 68% were restricted from participation by PT/nursing due to fatigue, inability to follow commands, nausea/dizziness, pain, or hypotension. Logistic regression showed that intraoperative estimated blood loss (EBL) >2L (OR = 5.57 [1.51-20.55], P = .010) was independently associated with an increased risk of delayed ambulation, with a 1.25 times higher risk for every 250 mL increase in EBL (P = .014). Modified 5-Item Frailty Index (mFI-5) was also independently associated with delayed ambulation (OR = 2.53 [1.14-5.63], P = .023). LateAmb demonstrated a higher hospital LOS (8.4 ± 4.0 vs 6.2 ± 2.6, P < .001). The LateAmb group trended toward an increase in medical complications on POD3+ (14.3% vs 26.5%, P = .210).
Conclusions
EBL demonstrates a dose-response relationship with risk for delayed ambulation. Delayed ambulation increases LOS and may impact medical complications.
Introduction
Surgical correction of symptomatic patients with adult spinal deformity (ASD) is effective in improving spine-related health quality. 1 However, complications after surgical correction of large deformities can be devastating to patient recovery.2,3 To reduce complications, various preoperative, intraoperative, and postoperative factors have been identified as potential risk factors for adverse medical and surgical events.2,4-6 However, many of these risk factors, such as age, medical comorbidities, and extent of surgery, are not modifiable, creating a ceiling effect on the extent to which pre- and postoperative protocols can impact complication rates.
Delayed postoperative ambulation is a potentially modifiable risk factor that has been implicated as a contributor to adverse outcomes in the spine literature,7-10 general orthopaedic literature,11,12 and general surgical literature.12,13 In the spine literature specifically, delayed ambulation has been linked to an increased risk of medical complications, an increased likelihood of non-home discharge, increased postoperative length of stay (LOS), and worse patient-reported outcomes.7-10,14 Though the impacts of delayed ambulation are well described, there has been limited investigation into why certain patients mobilize later than others. 15
We hypothesize that delayed ambulation is a multi-factorial phenomenon, impacted by preoperative comorbidities, surgical invasiveness, patient motivation, as well as institutional rehabilitation practices. However, a better understanding of these factors may provide modifiable targets for intervention to help patients mobilize more quickly after surgery, decreasing the risks associated with convalescence.7,10,16,17 Thus, the purpose of this study is to (1) identify preoperative, intraoperative, and postoperative risk factors for delayed ambulation and (2) assess the impact of delayed ambulation on inpatient complications.
Materials and Methods
Study Design
Institutional Review Board approval was attained prior to the initiation of this study (Hospital for Special Surgery, IRB #22014-357) and informed consent was obtained for all patients. We performed a single-center retrospective review of adult patients (≥50 years old) who underwent ASD surgery at our institution between January 2013 and December 2019. Inclusion criteria was posterior-only lumbar fusion of ≥5 vertebral levels to the pelvis. Patients with deformity from trauma, infection, or cancer were excluded from the analysis.
To investigate the impact of delayed ambulation on postoperative outcomes, patients were split into 2 groups based on whether they ambulated with physical therapy (PT) on postoperative day (POD) 1 or sooner vs POD2 or after. Those who ambulated on POD1 (Normal Ambulation Group [NmlAmb]) were propensity matched 1:1 with patients who ambulated on POD2 or later (Late Ambulation Group [LateAmb]) based on the number of levels fused and an ASD-specific surgical invasiveness score developed by Neuman et al (ASD-S). 18 All patients received a loading dose of 10-20 mg/kg and a maintenance dose of 1-2 mg/kg/hr of tranexamic acid (TXA), with exact dosing depending on anesthesiologist preference. All durotomies were primarily repaired and patients were permitted to work with PT on POD1 without restrictions. While our institution does not employ formal enhanced recovery after surgery (ERAS) protocols, the tenets of these protocols are emphasized at our institution, including physical therapy on postoperative day 1 or sooner, multimodal analgesia, and early feeding.
Statistical Analysis
Reasons for Delayed Ambulation.
Results
Risk Factors for Delayed Ambulation
Risk Factors for Delayed Ambulation.
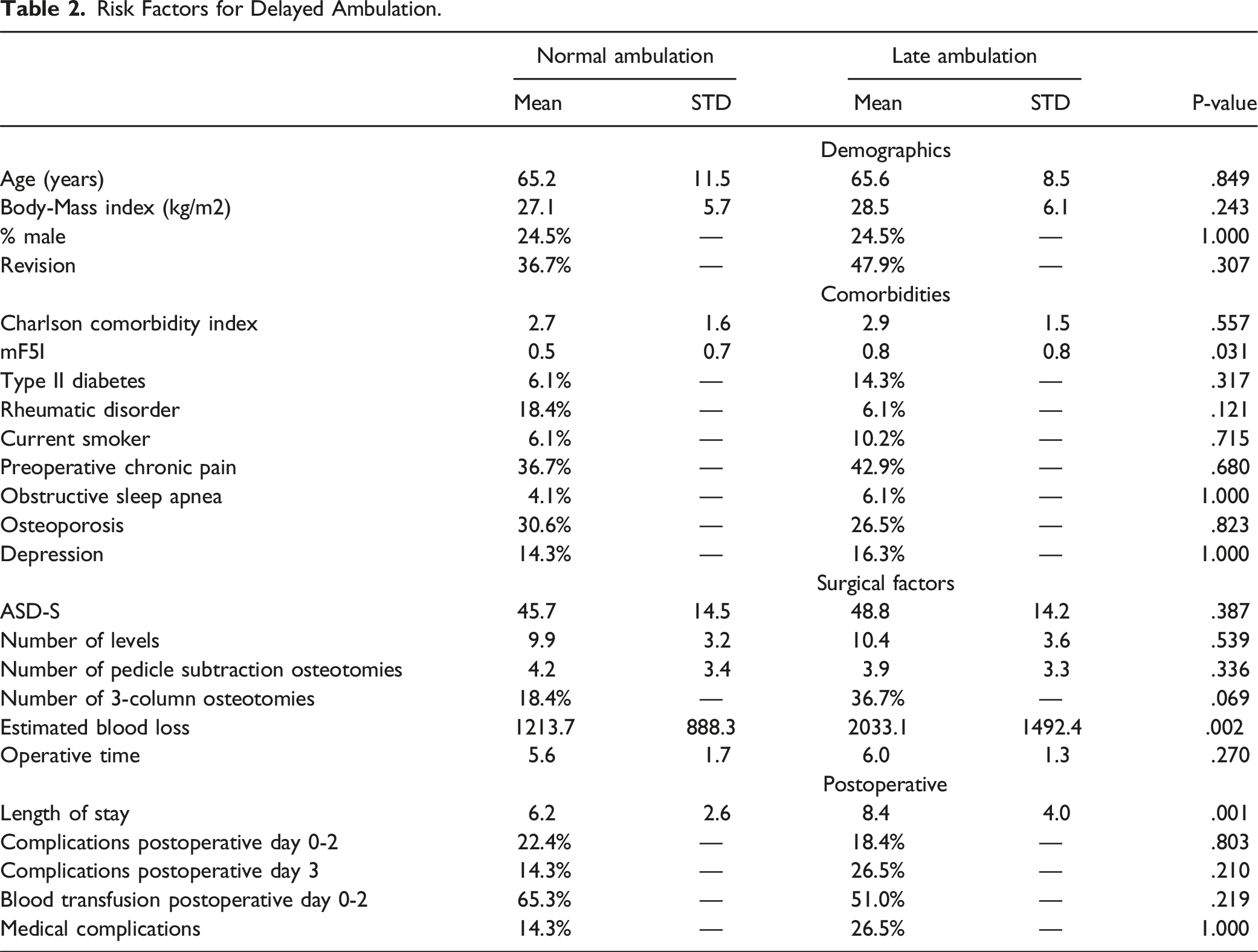
Backwards stepwise logistic regression was performed by inputting all the potential risk factors listed in Table 2 (ie, all factors listed except for excluding medical complications POD3 or later and length of stay). Logistic regression showed that EBL >2L (OR = 5.57 [1.51-20.55], P = .010) was independently associated with an increased risk of delayed ambulation, with 1.25 times increased odds for every 250 mL increase in EBL (P = .014). mFI-5 was also independently associated with delayed ambulation (OR = 2.53 [1.14-5.63], P = .023).
Reasons for Delayed Ambulation
Among the patients who did not ambulate on POD0-1, 32% declined participation secondary to pain, nausea/dizziness, or fatigue (Table 1). The remaining 68% of patients who did not ambulate on POD0-1 were restricted from participation by PT or nursing due to fatigue, inability to follow commands, nausea/dizziness, pain, or hypotension (Table 1). Combining patients who declined participation and those who were restricted from participating in PT, fatigue was the reason for delayed ambulation with PT in 32% of patients, pain in 24%, and nausea/dizziness in 20%. While differences in the proportion of patients with neurologic complications between the groups could impact early ambulation, there were no differences in neurologic complications between the groups.
Impact of Delayed Ambulation
LateAmb was associated with an increased hospital LOS (8.4 ± 4.0 vs 6.2 ± 2.6, P < .001). While there were no differences in medical complications between the groups on POD0-2 (22.4% vs 18.4%, P = .803), the LateAmb group trended toward increased medical complications on POD3+ (26.5% vs 14.3%, P = .210). There were no trends towards specific medical complications, such as DVTs/PEs, ileus, or failure to void.
Clinical vignettes comparing an early and delayed ambulator are shown in Figure 1. Clinical vignettes comparing early and delayed ambulators. The early ambulator shown in Panel 1 was a 65 year-old female with adult idiopathic scoliosis. She underwent a T2-pelvis posterior spinal fusion with osteotomies from L1-L4 and bilateral iliac fixation. Her intraoperative EBL was 900cc. She ambulated well on POD1 (15’) and POD2 (20’), and rapidly increased her ambulation thereafter. The delayed ambulator shown in Panel 2 was a 57 year-old female fixed thoracolumbar kyphosis and lateral listhesis from L1-5. She underwent a T2-pelvis posterior spinal fusion with Ponte osteotomies from T12 to L4 and bilateral iliac fixation. Her intraoperative EBL was 1800cc. She ambulated on POD2 (4’) and made slow ambulatory progress on POD3 (6’) and POD4 (6’) due to nausea and pain. Due to multiple failed trials of void, she required Foley catheter re-insertion and was discharged with a Foley in place.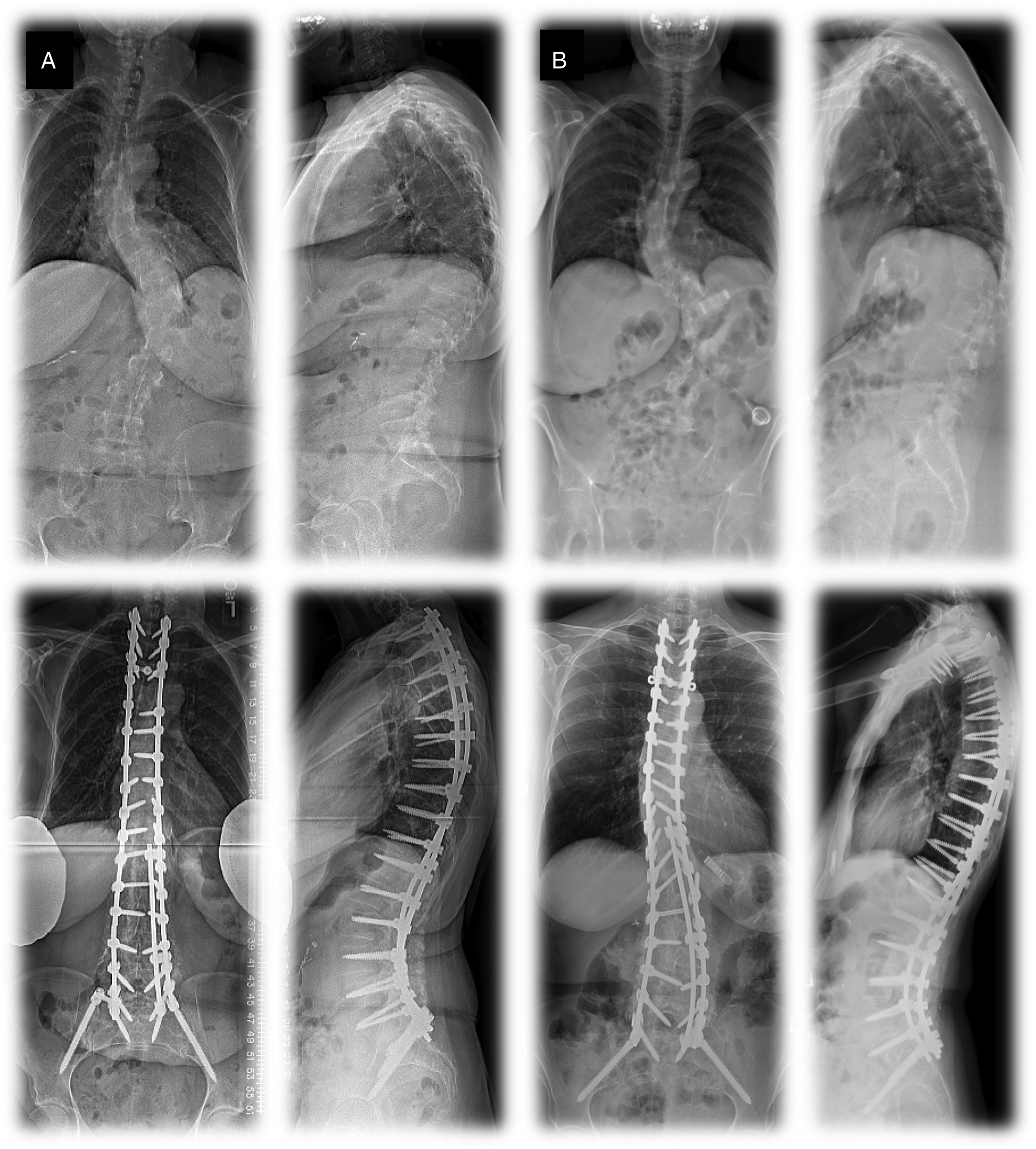
Discussion
In the current study, we assessed the reasons and risk factors for delayed ambulation, as well as the impact of delayed ambulation, following surgical correction of ASD. We identified preoperative frailty and intraoperative EBL as risk factors for delayed ambulation, with EBL >2L being associated with a 5.6 times higher risk of delayed ambulation. Furthermore, there was a dose-response relationship between EBL and risk of delayed ambulation, in which every 250cc increase in EBL was associated a 1.25 times higher risk of delayed ambulation. While most LateAmb patients were restricted from participation by nursing or PT, approximately one-third declined to participate with PT on POD1 despite being medically and physically appropriate for PT as assessed by the therapists and nursing staff. Delayed ambulation was associated with a higher length of stay and demonstrated a trend towards an increased risk of medical complications on POD3 and greater, but not before.
Importantly, the current study highlights the major reasons for failure to ambulate on POD0-1: fatigue, pain, and nausea/dizziness. While inability to follow commands and hypotension (which accounted for 24% of late ambulators) are difficult to modify, fatigue, pain, and nausea/dizziness represent actionable targets for improvement. It is possible that better use of multi-modal protocols for pain and nausea management may decrease these symptoms and subsequently impact early mobilization. Additionally, it is an interesting finding that 68% of late ambulators failed to ambulate on POD0-1 due to restrictions imposed by nursing and PT. Based on these findings, it is important to develop and implement standardized rapid ambulation protocols that prioritize ambulation on POD0-1. Protocols must be designed to decrease the impact of subjective provider judgement on who is appropriate for PT. This could be comprised of criteria that include patient-specific vital signs, labs, urine output, or number of hours after surgery that indicate appropriateness for PT. Physical therapists should be educated on the impact of early ambulation, focusing time on patients early after surgery vs those who are nearing discharge. If a patient declines to participate, then the therapist could visit the patient at a later time when pain is better controlled or the patient is feeling more motivated. Finally, surgeons must educate patients pre-operatively on the importance of early ambulation, turning them into active agents in their own recovery. While these changes may require new allocation of resources to therapy departments, the strong connection between early mobilization, reduced length of stay, and decreased medical complications7-13 should more than offset this cost.
We have also identified potential factors that ultimately lead to delayed ambulation: frailty and blood loss. We hypothesize there is likely a link between EBL, postoperative fatigue, hypotension, and inability to mobilize POD0-1. Blood loss, while often accepted as an inevitable aspect of ASD surgery, is an important area for optimization. Use of standardized protocols to limit blood loss, such as intraoperative tranexamic acid (TXA) and blood reinfusion, are important aspects of a multi-level protocol to limit the risk of delayed ambulation. 19 In a recent double-blind, placebo-controlled, randomized study by He et al, the use of IV TXA was associated with a decreased time to ambulation in patients undergoing transforaminal posterior lumbar interbody fusion. Furthermore, in the surgical oncology literature, increased intraoperative blood loss was associated with higher levels of postoperative fatigue and lower levels of activity. 20 Frailty was an additional factor independently associated with delayed ambulation. Frailty, as defined by the Modified 5-Item Frailty Index (mFI-5), is composed of non-independent functional status, type II diabetes, chronic obstructive pulmonary disease, congestive heart failure within 30 days, and hypertension requiring medication. In a general sense, these patients have less overall physiologic “reserve” and may be more susceptible to the side effects of heavy blood losses during surgery. Unfortunately, given that frailty is difficult to modify in the short term, optimization of chronic conditions is the most effective way to treat this condition preoperatively and minimize its impact on postoperative outcomes. These patients may also require extra motivation to participate in physical therapy and may require additional physical therapy sessions to offset their baseline low reserve.
The impact of delayed ambulation on the risk of adverse events following spine or other musculoskeletal surgery has been well-described.7-13 Adogwa et al. found that late ambulators were at an increased risk for the development of pneumonia after spine surgery, as well as were more likely to develop at least 1 medical complication postoperatively. 7 Additionally, early ambulators averaged a shorter postoperative LOS and were more likely to be discharged home as opposed to an inpatient rehabilitation center. Similarly, Huang et al 10 found an increased risk of postoperative urinary retention and ileus, as well as an increased risk of at least 1 medical complication among delayed ambulators.7-9 Finally, Nielsen et al 8 and Qvarfordh et al 8 found that early ambulation may increase patient satisfaction and decrease opiate use, 14 respectively.
While the drivers of delayed ambulation are multifactorial, interventional studies have demonstrated that targeted efforts to increased early mobilization can decrease time to ambulation and improve outcomes. For example, Kim et al. compared the impact of ERAS pathways in patients undergoing surgical correction of ASD to historical controls and found a decreased hospital LOS by nearly 3 days among early ambulators. 19 Similarly, Yuan et al 21 compared the impact of newly implemented ERAS pathways to historical matched controls in patients undergoing ASD surgery, reporting that earlier ambulation was associated with decreased LOS, shorter times to drain and urinary catheter removal, decreased 90-day readmission, earlier return of bowel function, and a decreased risk of urinary retention and surgical site infection. The common theme is that both studies implemented tenants of ERAS theories: multimodal analgesia, multidisciplinary input and interventions, and quality review once protocols were initiated.
This investigation had several limitations. First, while we matched for surgical invasiveness and surgical levels, it is impossible to capture the intricacies of each surgery. Therefore, there may have been differences in individualized surgeries that were not accounted for in the match, serving as unknown confounders. Additionally, given the high number of patients who were restricted from participation in PT (as opposed to being unable to participate), it is possible that factors like EBL and frailty influenced providers’ willingness to allow patients to ambulate, rather than EBL and frailty independently decreasing the probability of early ambulation. Pre-defined thresholds on the time from surgery to first PT participation, patient-specific vital signs for PT, and repeat visits for patients who are not initially participating may help offset the impact of subjectivity in provider judgement. Preoperative patient-reported outcomes, which may influence whether patients ambulate early, were not assessed as a risk factor or protective factor for timing of ambulation postoperatively. Finally, given the single-institution design, we did not have sufficient power to detect statistical differences in certain aspects of our analysis, such as the risk of medical complications, despite relatively large absolute differences.
Conclusions
Preoperative frailty and increased blood loss are independently associated with delayed ambulation after ASD surgery. These may manifest as downstream symptoms that limit patients from early mobilization. While most patients are restricted by providers from participation in physical therapy, one-third of patients decline to participate despite being deemed appropriate. Delays in ambulation are associated with an increased LOS and trends towards a higher risk of medical complications. These findings suggest that delayed ambulation and its associated adverse impacts may be avoided by educating patients and therapists on the importance of early ambulation, instituting therapy protocols that minimize the impact of subjective provider judgement, encouraging repeat early PT visits for frail or high-EBL patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.