
Abstract
Study Design
Retrospective study of prospectively collected data.
Objective
To determine if patients undergoing spinal deformity surgery with pelvic fixation are at an increased risk of morbidity.
Methods
The American College of Surgeons National Surgical Quality Improvement Program is a large multicenter clinical registry that prospectively collects preoperative risk factors, intraoperative variables, and 30-day postoperative morbidity and mortality outcomes from ~400 hospitals nationwide. Current Procedural Terminology codes were used to query the database between 2010 and 2014 for adults who underwent fusion for spinal deformity. Patients were separated into groups of those with and without pelvic fixation. Univariate analysis and multivariate logistic regression were used to analyze the effect of pelvic fixation on the incidence of postoperative morbidity and other surgical outcomes.
Results
Multivariate analysis showed that pelvic fixation was a significant predictor of overall morbidity (odds ratio [OR] = 2.3, 95% confidence interval [CI]: 1.7 to 3.1, p = 0.0002), intra- or postoperative blood transfusion (OR = 2.3, 95% CI: 1.7 to 3.1 p < 0.0001), extended operative time (OR = 4.7, 95% CI: 3.1 to 7.0 p < 0.0001), and length of stay > 5 days (OR = 2.1, 95% CI 1.5 to 2.8, p < 0.0001) in patients undergoing fusion for spinal deformity. However, fusion to the pelvis did not lead to additional risk for other complications, including wound complications (p = 0.3191).
Conclusion
Adult patients undergoing spinal deformity surgery with pelvic fixation were not susceptible to increased morbidity beyond increased blood loss, greater operative time, and extended length of stay.
Introduction
Adult spinal deformity (ASD) is a challenging spinal disorder due to its complex presentation and treatment. 1 –3 Surgical treatment is most commonly spinal fusion, though the surgeon must take into account several factors that vary by patient and deformity characteristics. 4,5 Particularly challenging is the extension of long fusions to L5–S1 for several reasons. Long fusion constructs to this area, which are often necessary for correction of both sagittal and coronal plane deformities, have a high rate of pseudarthrosis. The large lever arms and cantilever forces created by long constructs produce high mechanical stress at the construct's base. Furthermore, the sacrum and the S1 and S2 pedicles in particular are quite cancellous and potentially osteoporotic in the elderly ASD patient. When these risks are present, pelvic fixation may be indicated to improve the stability of the construct base and maintain the surgical correction of deformity until fusion is achieved. 6 –8
Given the increasing incidence of spinal deformity in the United States, 1 –3 understanding the potential complications of surgical intervention is important. In particular, pelvic fixation has not been well studied. Previous studies generally do not adequately assess the additional risk pelvic fixation adds to spinal fusion surgery. In the recent literature, pelvic fixation has been associated with higher infection rates, longer operating times, longer length of stay, and higher rate of blood loss. However, these studies were small, single-center studies. 9 –11 Furthermore, these studies considered pediatric patients with neuromuscular scoliosis, not ASD. Other studies on pelvic fixation have considered the differences in complications between different techniques for extension to the pelvis. 12 –14 Others have been noncomparative investigations, focusing solely on outcomes. 15 –17
To our knowledge, no study has used a large, multi-institutional database to describe the risk profile for pelvic fixation in patients who undergo fusion for ASD. In this study, the ACS-NSQIP database was used to investigate the effect of pelvic fixation adjunct to spinal deformity surgery on 30-day morbidity and mortality in adults.
Materials and Methods
Data Source
The ACS-NSQIP was originally created as a quality improvement initiative for the Veteran's Administration (VA) health system in 1994. It has since expanded to the private sector after its initial success in the VA system. 18,19 Details of the ACS-NSQIP (www.acsnsqip.org) have been described before, and its use has been well established in the surgical literature. It is a validated outcomes registry that allows assessment of 30-day risk-adjusted surgical morbidity and mortality to provide feedback to participating hospitals. 20
The database consists of more than 150 preoperative, intraoperative, and 30-day postoperative variables that are collected prospectively from the medical records and operative reports among other sources by on-site surgical clinical reviewers. Data is gathered through the entirety of the 30-day postoperative period, including patients discharged within this period or treated on an outpatient basis. 20
Data Collection
The ACS-NSQIP database from 2010 to 2014 was used in this study. Adult patients (≥18 years) undergoing spinal fusion for deformity were identified based on Current Procedural Terminology (CPT) codes 22802, 22804, 22810, and 22812. CPT codes 22843, 22844, 22846, or 22847 were included to capture long, multilevel fusions (Table 1). Patients undergoing pelvic fixation in addition to fusion were identified using CPT code 22848. To reduce the risk of confounding variables, we excluded cases with missing preoperative data; emergency cases; patients with a wound class of 2 (clean wound but within the respiratory, alimentary, genital, or urinary tracts), 3 (contaminated), or 4 (infected); patients with an open wound on their body, current sepsis, current pneumonia, or prior surgeries within 30 days; cases requiring cardiopulmonary resuscitation prior to surgery; patients undergoing a nonelective procedure; and cases with diagnoses of cervical spine trauma or injury or neoplasm of the spine.
CPT code definitions
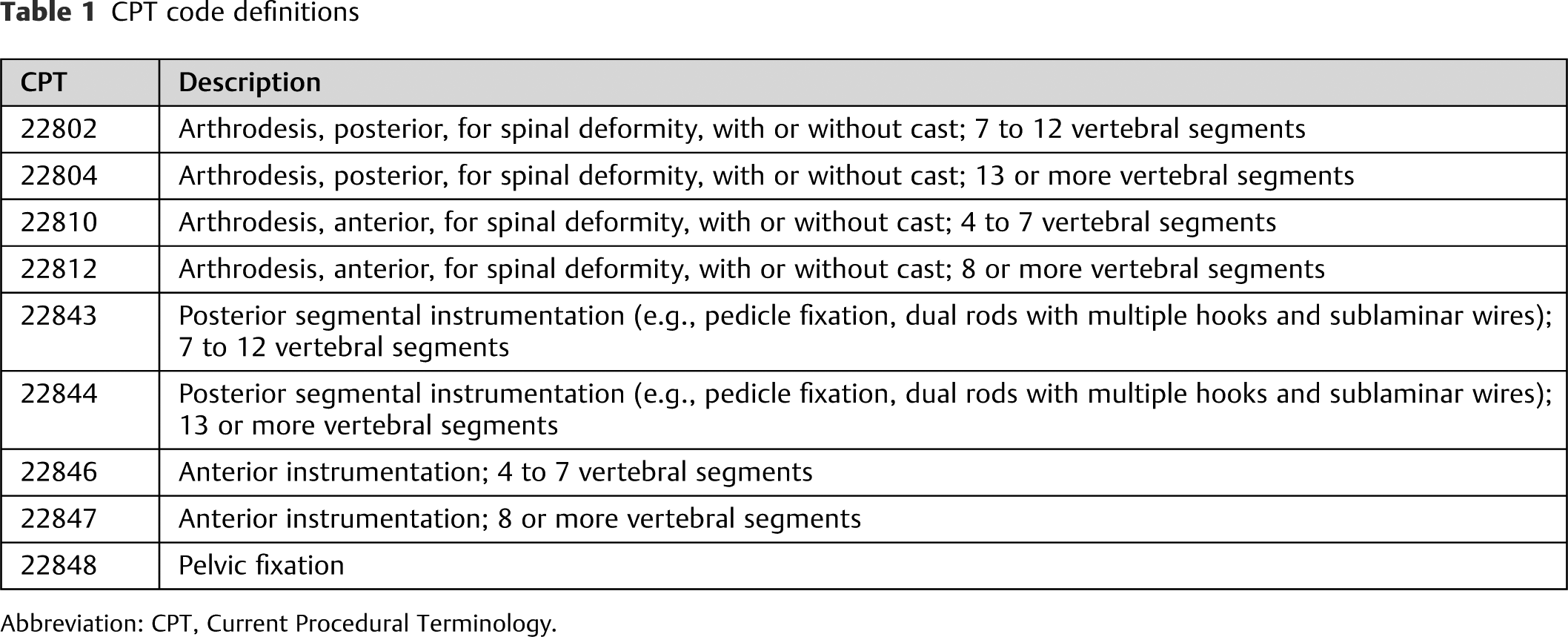
Abbreviation: CPT, Current Procedural Terminology.
Propensity-Score Matching
Propensity-score matching allowed for reduction of the risk of selection bias within this population. This reduction was particularly important as the pool of patients with pelvic fixation was small (n = 415) and the number of patients without pelvic fixation was much larger (n = 3,233). Propensity scores were assigned to patients in each cohort (with or without pelvic fixation) based on several preoperative factors including patient demographics, operative information (primary posterior versus primary anterior approach, osteotomy, bone graft, intervertebral device insertion, and total relative value units [RVUs]), and preoperative comorbidities. The process of matching was 1:1 and performed by selecting one patient from the pelvic fixation cohort and matching the patient with one in the non–pelvic fixation cohort with the closest propensity score. Comparisons for postoperative morbidity and mortality were conducted only on the matched cohorts. Propensity-score matching has been well described in the literature. 21 –25 Matching was performed using R Software (Vienna, Austria, http://www.R-project.org/) package “MatchIt.” 26
Variable Definitions
Several comorbidities were grouped into the following categories: pulmonary, renal, cardiac, and peripheral vascular disease and neuromuscular injury. Pulmonary comorbidity included a history of severe chronic obstructive pulmonary disease or ventilator dependence during the 48 hours preceding surgery. Renal comorbidity included dialysis or acute renal failure. Cardiac comorbidity included a history of congestive heart failure within 30 days before admission or hypertension requiring medication. Obesity was defined as a body mass index ≥ 30, per World Health Organization guidelines. Patients were characterized as smokers by the ACS-NSQIP if they had smoked cigarettes in the year prior to admission for surgery. Using the list of CPT codes described in the work by Martin et al, 27 patients were categorized according to the type of surgical procedure performed.
This study's definition of morbidity included all ACS-NSQIP-defined complications, including the need for an intra- or postoperative blood transfusion. The scope of this study extended further to mortality, return to operating room, unplanned reoperation, unplanned readmission, extended operative time (>4 hours), and extended length of hospital stay (>5 days).
Statistical Analysis
Descriptive and comparative statistics of demographics, comorbidities, operative details, and postoperative complications were analyzed for all patients. In the univariate analysis, categorical variables were assessed using Pearson chi-square or Fisher exact test where appropriate. Continuous variables were examined using one-way analysis of variance test. Preoperative variables with a p < 0.2 in the univariate analysis were carried forward into the multivariate analysis, as has been demonstrated in previous studies. 28 This specific selection criterion was used to consider as many potential risk factors as possible without compromising the validity of regression models. Stepwise multivariate logistic regression analysis was used to determine the independent risk factors for each postoperative complication based on this criterion. A p value < 0.05 was considered significant; 95% confidence intervals (CIs) are reported for each odds ratio (OR) and can be interpreted as being 95% certain the true odds ratio falls between this range. SAS software (Version 9.3, SAS Institute, Inc., Cary, North Carolina, United States) was used for all statistical analyses.
Results
In the unmatched cohorts, patients with pelvic fixation were more likely to be female (p = 0.0002) and be between the ages of 61 and 70 years (p < 0.0001). They were less likely to be of Black or African American race (p = 0.0103), to have American Society of Anesthesiologists (ASA) score ≥ 3 (p < 0.0001), and to smoke (p < 0.0001). They had higher total RVUs (p < 0.0001; Table 2). Additionally, the pelvic fixation cohort was more likely to have cardiac comorbidity (p = 0.0287; Table 3).
Demographics and clinical characteristics
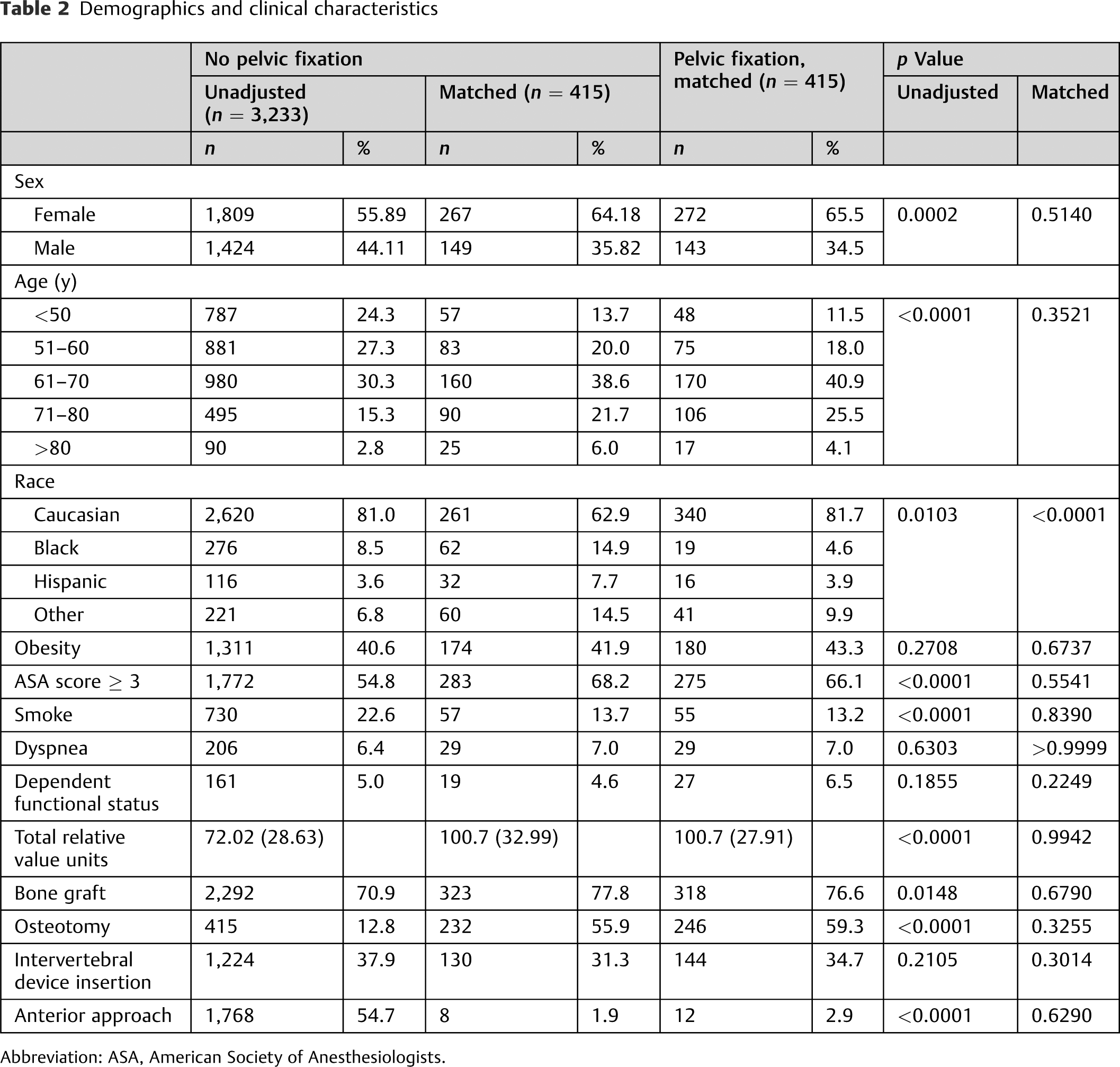
Abbreviation: ASA, American Society of Anesthesiologists.
Preoperative comorbidities
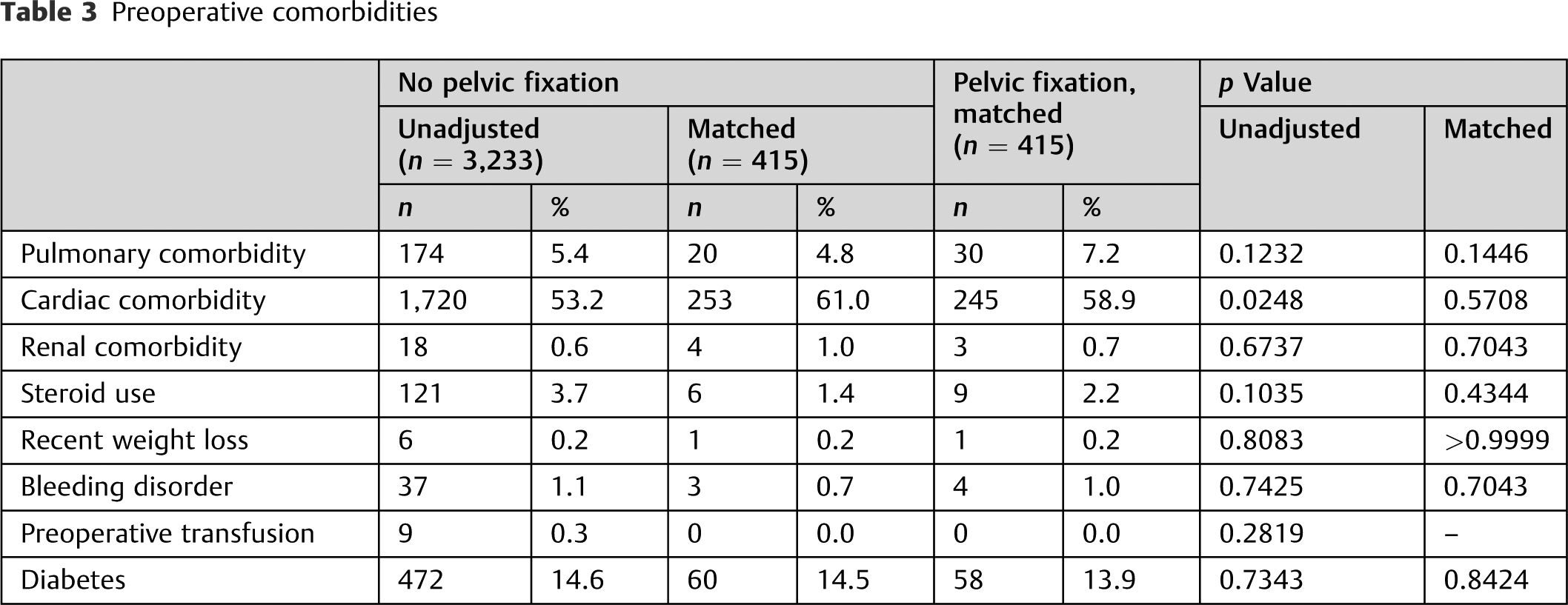
After propensity matching, there were no significant differences in patient demographics or preoperative comorbidities between the two cohorts (Tables 2 and 3), except for race (p < 0.0001).
Univariate Analysis
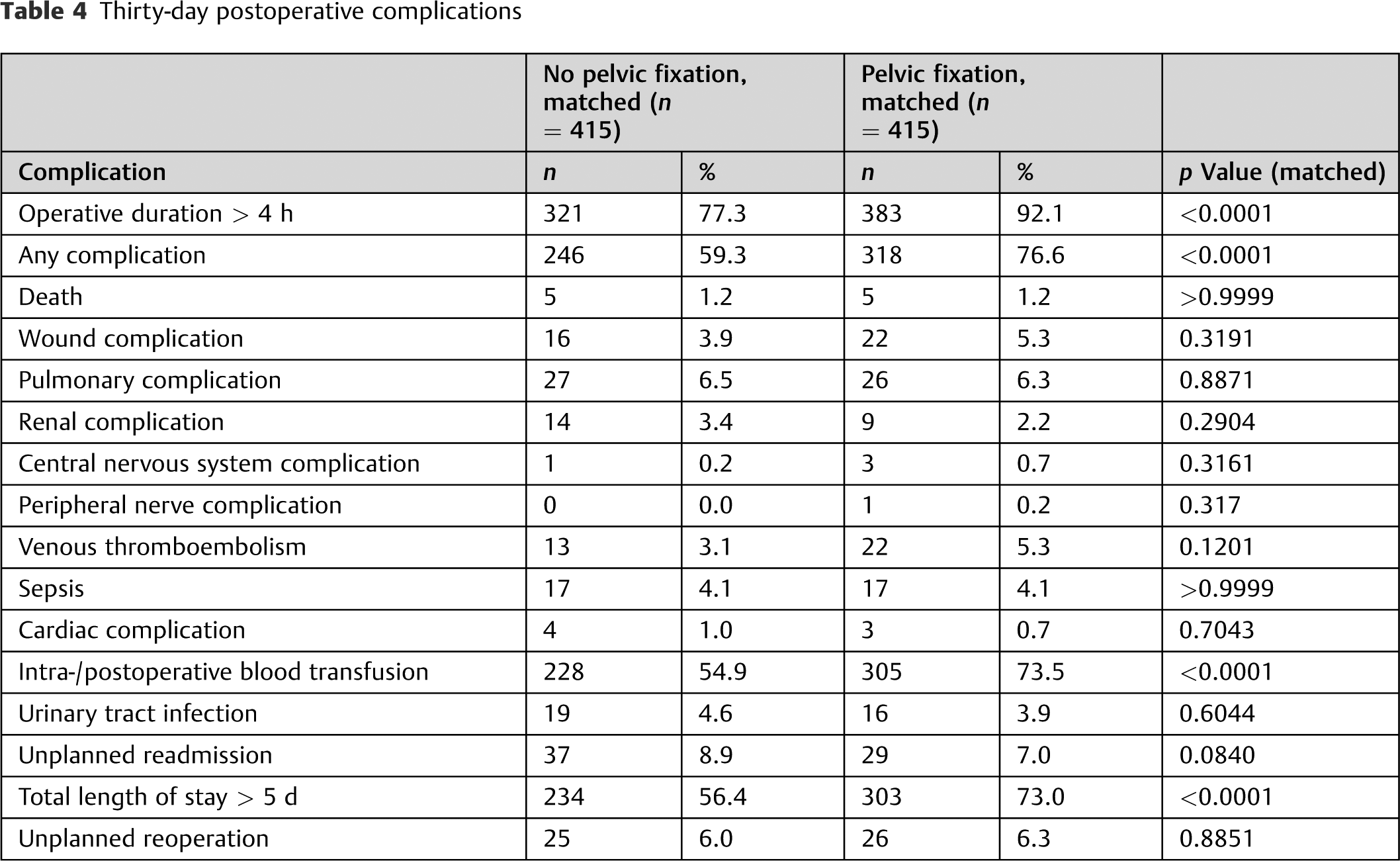
Pelvic fixation was associated with greater overall morbidity (p < 0.0001), higher rate of intra-and postoperative transfusion (p < 0.0001), higher likelihood for operative time > 4 hours (p < 0.0001), and extended length of stay > 5 days (p < 0.0001). Importantly, the pelvic fixation cohort had no additional risk for wound complications (p = 0.3191). All other complications studied showed no statistical difference as well (Table 4).
Thirty-day postoperative complications
Multivariate Analysis
The multivariate analysis showed that pelvic fixation was a significant predictor of overall morbidity (OR = 2.3, 95% CI: 1.7 to 3.1, p = 0.0002), intra- or postoperative blood transfusion (OR = 2.3, 95% CI: 1.7 to 3.1, p < 0.0001), extended operative time (OR = 4.7, 95% CI: 3.1 to 7.0, p < 0.0001), and length of stay > 5 days (OR = 2.1, 95% CI 1.5 to 2.8, p < 0.0001) in patients undergoing fusion for spinal deformity (Table 5).
Adjusted ORs for selected outcomes for pelvic fixation (n = 832)
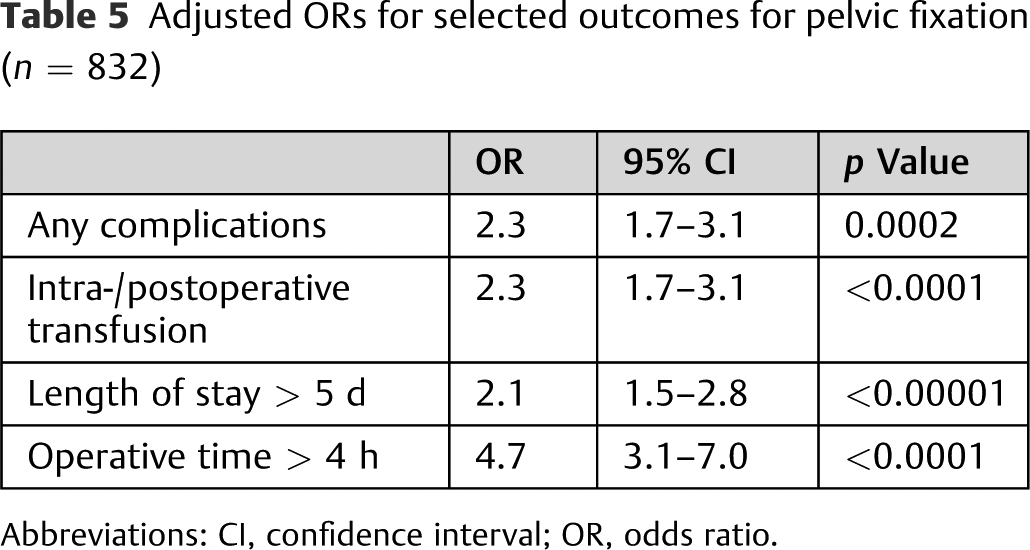
Abbreviations: CI, confidence interval; OR, odds ratio.
Discussion
This investigation presents a comparative analysis on 830 patients undergoing spinal fusion for ASD, divided into propensity-matched cohorts based on the additional procedure of pelvic fixation. Few studies have directly evaluated the differences in short-term complication rates between patients with ASD who underwent spinal fusion with and without pelvic fixation, and to our knowledge, none have been performed using a large national database such as the ACS-NSQIP. The present study revealed that intraoperative or postoperative transfusion, operative time, and length of stay were significantly greater in the pelvic fixation cohort (Table 5). However, no other complications were found to be statistically different between the two cohorts (Table 4).
A major finding of this analysis was that pelvic fixation itself did not increase the incidence of wound complications (superficial and deep surgical site infections, organ space infection, and wound dehiscence, p = 0.3191; Table 4). In the unmatched cohort comparison, patients with pelvic fixation were older (63.4 versus 58.4 years, p < 0.0001). Previously, age has been shown to be a significant risk factor for wound complications in several studies focused on spinal fusion (Table 2). 29,30,31 Patients having pelvic fixation were also more likely to have ASA class of ≥ 3 (66.1 versus 54.8%, p < 0.0001; Table 2). Higher ASA score has also been correlated with an increased risk of wound complications in spinal fusion surgeries. 32 When adjusted for risk factors, there was no longer any statistical difference in the wound complications between the two cohorts, indicating that patient-related factors may have played a more significant role than pelvic fixation.
Based on the multivariate analysis, pelvic fixation was an independent risk factor (OR = 2.3, p < 0.0001) for intra- or postoperative transfusion (Table 5). These findings were consistent with previous studies. 10,11 Overall, 73.5% of patients having pelvic fixation required blood transfusion compared with 54.9% of patients not having pelvic fixation who required transfusion, which was statistically significant (p < 0.0001; Table 4). Ramo et al concluded that the addition of pelvic fixation to spinal fusion surgery caused additional complications simply because pelvic fixation was a proxy for increased operative time. 9 However, on multivariate analysis, pelvic fixation was found to be a risk factor independent of operative time for intra- or postoperative transfusion.
The literature has shown increased blood transfusion to be associated with increased postsurgical morbidity and mortality. 33 –37 These studies have been unable to conclude if the high complication rate was a product of preoperative anemia or the transfusion itself. Dunne et al concluded that preoperative anemia was the risk factor and that blood transfusion was simply correlated to peri- or postoperative anemia. 34 However, Schwarzkopf et al hypothesized that blood transfusions have modulatory effects on the immune system of recipients leading to greater infection rates. 36 Furthermore, a recent meta-analysis between programs with liberal versus restrictive blood transfusion programs in Europe showed that a restrictive transfusion protocol led to decreased hospital mortality and postoperative infections, 38 adding weight to the thought that transfusions may have deleterious effects on patient outcome. A better understanding of pelvic fixation as a risk factor for blood transfusion may lead to the implementation of interventions designed to control excessive bleeding. Additionally, more stringent patient blood management programs, such as those that are in place in Europe, may have value in this regard. 39
Another major finding was that pelvic fixation was an independent risk factor for extended operative time (>4 hours; OR = 4.7, p < 0.0001; Table 5). This finding is natural, because extending instrumentation to the pelvis was likely performed with long fusion constructs and the fixation itself was an additional procedure. 6 –8 Nonetheless, it is important to be mindful of extensive operative time when risk-stratifying patients with ASD. Operative time is particularly important because it is correlated to higher morbidity, particularly infection, in spinal fusion surgeries. 40,41 Tang et al hypothesized that direct contact with the sterile field, airborne contamination from traffic, and loss of sterile technique become more likely with extended operative time. 40 Dalstrom et al conducted a study in a simulated operating room environment and found a significant correlation between the length of time that the sterile tray was exposed to the air and the contamination rate of the instruments. 42 Additionally, studies in general and vascular surgery and neurosurgery studies showed that operative time increased the likelihood of venous thromboembolism. 43 –46 In fact, venous thromboembolism had a higher incidence in the pelvic fixation cohort in our analysis (5.3 versus 3.1%) but was not statistically significant (p = 0.1201).
Finally, the greater length of stay with patients undergoing pelvic fixation is a more complex finding that may be attributed to several causes. Greater operative times and higher rates of transfusion are independent predictors for greater length of stay as shown by Basques et al in spinal fusion. 47 Possible reasons for extended hospitalization may also include the generally higher overall rates of complication (76.6 versus 59.3%, p < 0.0001), compared with the cohort without pelvic fixation.
There were several limitations to this study. Different techniques for pelvic fixation exist and are associated with different complication rates. 12 –14 Because this study was performed using CPT codes, only the general procedure was accounted for, so it was not possible to determine the effect of specific techniques used. Furthermore, patients were matched by total relative value units to account for case mix, fusion approach, and additional operative features such as pedicle subtraction osteotomy. Notably, matching by additional characteristics was not feasible given the handicap of working with CPT codes. For example, matching was not conducted to ensure nonsignificant differences in the number of patients who had posterior-only approaches versus those who had an adjunct anterior or lateral interbody fusion in conjunction with posterior fusion. Additionally, in multivariate analysis, the interaction effects between variables were not considered or adjusted for.
The ACS-NSQIP database itself poses several additional limitations. First, information was not captured on the severity of the deformity being treated. For example, no radiographic parameters were captured that would indicate the degree of deformity in the sagittal or coronal plane. However, this issue was addressed by isolating only the cohort of patients who underwent fusions that were greater than four levels with anterior approach and greater than six levels with posterior approach. Furthermore, patients with and without pelvic fixation were propensity-matched with anterior versus posterior approach, total RVUs, and use of pedicle subtraction osteotomy to ensure both cohorts were similar with respect to complexity of the deformity surgery. Additionally, the specific long-term outcomes relevant to spinal fusion such as pseudarthrosis and loss of correction are not captured by the ACS-NSQIP database. This lack of data did not allow us to study the efficacy of pelvic fixation in preventing these complications, although several previous studies have already demonstrated that pelvic fixation does indeed lead to decreased pseudarthrosis rates. 47 Instead, the ACS-NSQIP database only allowed us to understand the short-term morbidity risk of pelvic fixation adjunct to fusion. These limitations are inherent to retrospective analysis conducted on data collected without the specific research question in mind.
The ACS-NSQIP database is also not representative of all U.S. hospitals, because academic medical centers are overrepresented in the database. 48,49 Academic medical centers are significantly different from community hospitals in terms of dedication to using the latest research to improve outcomes and the general profile of patients seen. Furthermore, variations or errors in coding of procedures, comorbidities, and complications may naturally be present and cannot be accounted for. Additionally, creating binary values of “yes” or “no” for comorbidities such as diabetes or chronic obstructive pulmonary disease that have a range of presentation and progression does not fully capture the true profile of that particular patient. Finally, the observation period for morbidity, mortality, and other surgical outcomes was limited to 30 days after surgery. Thus, longer-term complications were not captured, leading to potential underestimation of the risk profile for these surgical procedures.
Despite these limitations, this study was one of the largest examining pelvic fixation as part of spinal deformity surgery in adults. Pelvic fixation was found to increase the risk for overall postoperative morbidity, intra- or postoperative blood transfusion, extended operative time, and extended length of hospitalization. However, there was no increase in any other complications examined. Thus, its use should be encouraged for situations in which it may augment the correction of deformity and reduce rates of pseudarthrosis and implant failure. Future studies should consider the impact of pelvic fixation on complications beyond the 30-day period captured by the ACS-NSQIP.
Footnotes
Disclosures
Parth Kothari: none
Sulaiman Somani: none
Nathan J. Lee: none
Javier Z. Guzman: none
Dante M. Leven: none
Branko Skovrlj: none
Jeremy Steinberger: none
Jun Kim: none
Samuel K. Cho: Consultant (Stryker); Research support (Zimmer)
Note
This study was qualified as exempt by the Mount Sinai Hospital Institutional Review Board.