
Abstract
Study Design:
Retrospective database review.
Objectives:
The incidence and risk factors for surgical delay of multilevel spine fusion for adult spinal deformity (ASD), and the complications corresponding therewith, remain unknown. The objectives of this study are to assess the incidence and risk factors for unexpected delay of elective multilevel spinal fusions on the date of surgery as well as the postoperative complications associated with these delays.
Methods:
We conducted a retrospective review of the ACS-NSQIP database on patients undergoing elective spinal instrumentation of greater than 7 levels for ASD between the years 2005 and 2015. Preoperative risk factors for delay and postoperative complications were compared between the cohorts of patients with and without surgical delays.
Results:
Multivariate analysis of 1570 (15.6%) patients identified advanced age, male sex, American Society of Anesthesiologists (ASA) Class 4, and history of smoking as independent risk factors for delay. Patients experiencing surgical delay demonstrated longer operative times, increased intraoperative bleeding, longer hospitalizations, and significantly higher rates of postoperative complications. Patients experiencing delay demonstrated an almost 7-fold increase in mortality rate (3.4% vs 0.5%, P < .001).
Conclusions:
Delays in elective surgical care for spinal deformity are negatively related to patient outcomes. Advanced age, male sex, increased ASA class, and a history of smoking cigarettes place patients at risk for surgical delay of multilevel spinal fusion. Patients experiencing surgical delay are at higher risk for postoperative complications, including a 7-fold increase in mortality. These findings suggest that ASD surgery should be postponed in patients experiencing a delay, until modifiable risk factors can be medically optimized, and perhaps postponed indefinitely in those with nonmodifiable risk factors.
Introduction
Adult spinal deformity (ASD) represents a broad spectrum of spinal pathology encompassing scoliosis, kyphosis, degenerative spondylosis, segmental subluxation, and rotational malalignment. 1 Spinal deformity can cause debilitating pain and loss of function for affected patients, and surgical fusion for ASD has shown successful outcomes in appropriately indicated patients.2-5 Surgical advances in instrumentation and technique have led to increased utilization of multilevel instrumented fusion in treating ASD patients.6,7 The surgical management of ASD is associated with high cost and substantial resource utilization. 8 In a cost analysis of adult patients undergoing multilevel spinal fusion utilizing the Nationwide Inpatient Sample database, Sing et al 7 reported that inflation-adjusted mean hospital charges increased from $171 517 in 2004 to $303 479 in 2011. The demand for surgery to address ASD will continue to increase, as the prevalence of this condition rises in the United States,9,10 adding further strain to an already burdened health care system. In an effort to improve cost-effectiveness, identifying factors associated with increased health care spending, such as postoperative complications and longer hospital stays, has become a major focus for surgeons, hospital administrators, insurers, and health care policy makers.
Recently, several studies have sought to assess the effects associated with surgical delay in both the nonelective and elective orthopedic surgical settings.11-16 These studies found that surgical delay of elective procedures is related to increased postoperative complications, and as such, these delays result in greater hospital resource utilization and higher costs.14,15,17 Identifying the risk factors associated with experiencing an unexpected surgical delay among ASD patients scheduled for elective multilevel spinal fusion may facilitate reducing the incidence of delay and the corresponding complications and costs therewith. To our knowledge, there have been no published studies on identifying the risk factors for surgical delay in patients undergoing elective multilevel spinal fusion for ASD. Utilizing the American College of Surgeons National Surgical Quality Improvement Project (ACS-NSQIP) database, we sought to identify the incidence of and risk factors related to surgical delay in the elective multilevel fusion patient population and to evaluate the immediate postoperative outcomes in those patients experiencing postponement of their surgery. We hypothesized that patients experiencing a delay would have worse outcomes than patients without a delay.
Methods
After institutional review board approval, we queried the ACS-NSQIP database from the years 2005 through 2015 using the Current Procedural Terminology (CPT) codes 22 843 and 22 844 in order to identify all patients with ASD undergoing elective instrumented spinal arthrodesis of greater than 7 levels. These CPT codes were used to identify patients with significant multilevel spinal deformity within the ACS-NSQIP database. The ACS-NSQIP database is a national, prospectively collected database of de-identified surgical patient data variables extending up to 30 days following the index surgery obtained from participating hospitals. The database is routinely audited in order to ensure its integrity and accuracy.
Patient Demographics and Outcomes
Patients were identified as having undergone elective spinal arthrodesis of greater than 7 levels utilizing CPT codes 22 843 and 22 844, which are utilized for posterior segmental instrumentation spanning 7 to 12 and 13 or more vertebral segments, respectively. Patients were divided into 2 cohorts predicated on the presence or absence of a surgical postponement of at least 1 day from the date of the patient’s initial hospital presentation for surgery, but who still underwent surgery during the same hospitalization period. Patient demographics, surgical variables, and comorbidities were extracted from the database to identify differences between the delayed and nondelayed cohorts. Demographics analyzed included patient age, sex, body mass index (BMI), race, and American Society of Anesthesiology (ASA) classification. The medical comorbidities included were diabetes mellitus, smoking, chronic steroid use (defined as corticosteroid use within 30 days of surgery), congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), chronic renal failure requiring dialysis, and hypertension requiring treatment with medication.
The surgical variables assessed were operative time, length of hospital stay, and need for intraoperative transfusion. The complications analyzed were return to the operating room, venothrombolic event (VTE, defined as either a pulmonary embolism [PE] or deep vein thrombosis [DVT]), stroke, myocardial infarction (MI), cardiac arrest, urinary tract infection (UTI), pneumonia, ventilator time longer than 48-hours, surgical site infection (either superficial or deep), and mortality.
The delay and nondelayed cohorts were then compared to find any differences between them. Differences in demographics, surgical variables, and comorbidities between the cohorts were analyzed as potential risk factors for surgical delay. Surgical variables and complications within 30 days of the index surgery were further analyzed in order to determine a correlation with the surgical delay.
Statistical Analysis
Statistical analysis of the data was performed using the “rms” package for R (R Foundation for Statistical Computing, Vienna, Austria). The Fisher’s exact test was used to evaluate discrete variables and the Mann-Whitney U test was used to compare continuous variables except for parametric variables, which were instead compared using an unpaired Student’s t test. ASA class was also analyzed with the Mann-Whitney U test as a ranked variable. Multivariate logistic regression analysis was utilized to determine independent risk factors, with results reported as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). A P value less than .05 was considered statistically significant.
Results
A total of 10 071 patients were identified in the ACS-NSQIP database as having undergone instrumented fusion of at least 7 vertebral levels for ASD between 2005 and 2015. The rate of surgical delay within this cohort was 15.6%, comprising 1570 patients experiencing an unexpected delay of at least 1 day of their multilevel spinal fusion on the originally scheduled date of surgery. Univariate analysis yielded the following demographic characteristics as predictive of surgical delay: increased age, non-White race, decreased body mass index, male sex, elevated ASA class (ASA class 3 or 4), diabetes mellitus, steroid use, CHF, COPD, dialysis, and hypertension requiring medications (Table 1).
Univariate Analysis of Risk Factors for Surgical Delay Prior to Elective Multilevel Spine Fusiona.
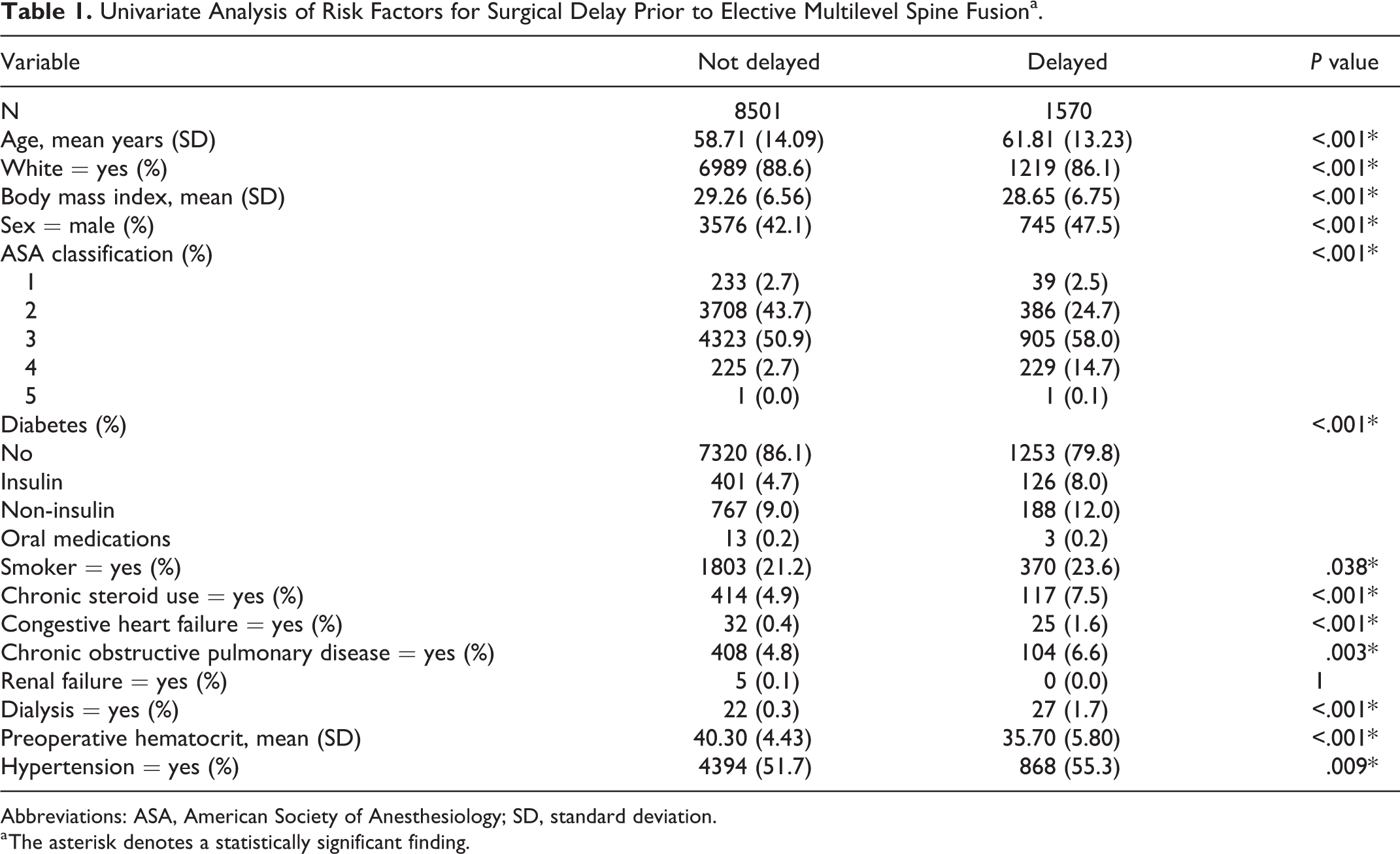
Abbreviations: ASA, American Society of Anesthesiology; SD, standard deviation.
a The asterisk denotes a statistically significant finding.
Subsequent multivariate analysis between the delayed and nondelayed cohorts identified increased age as defined by age per year (OR = 1.012, 95% CI = 1.007-1.017, P < .001), male sex (OR = 1.926, 95% CI = 1.699-2.183, P < .001), ASA class 4 (OR = 1.715, 95% CI = 1.161-2.535, P = .007), and smoking (OR = 1.437, 95% CI = 1.240-1.666, P < .001) as risk factors for surgical delay on preoperative hospital presentation. Multivariate regression also identified history of hypertension controlled on medication as being protective against delay (OR = 0.775, CI = 0.679-0.885, P < .001; Table 2).
Multivariate Analysis of Risk Factors for, or Protective Against, Surgical Delay Prior to Elective Multilevel Fusiona.
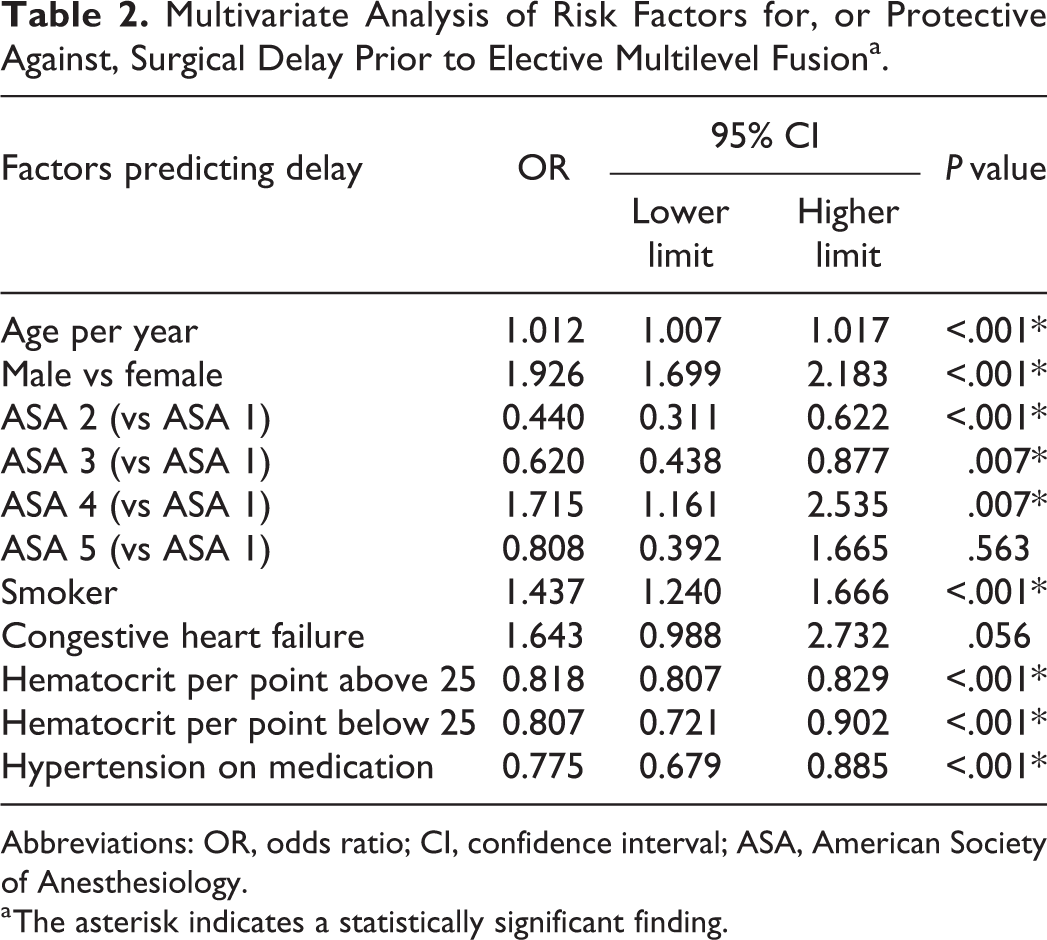
Abbreviations: OR, odds ratio; CI, confidence interval; ASA, American Society of Anesthesiology.
a The asterisk indicates a statistically significant finding.
Patients who experienced a delay of their surgery were significantly more likely to develop postoperative surgical and medical complications after undergoing multilevel fusion. The delayed cohort had a 44.4% overall complication rate compared to a 19.1% complication rate in the nondelayed cohort. When stratifying these complications as either major or minor complications, the delayed cohort demonstrated a major complication rate of 35.3% and a minor complication rate of 9.1%. In comparison, the nondelayed cohort had major and minor complication rates of 15.2% and 3.9%, respectively (Table 3). The delayed cohort had longer operative times, higher rates of operative bleeding, VTE, return to the operating room, prolonged ventilator time, UTI, pneumonia, superficial and deep wound infections, and sepsis. In addition, the total length of inpatient hospital admission was significantly longer for the delayed cohort (12.50 vs 4.83 days), and the overall mortality rates were 3.4% and 0.5% for the delayed and nondelayed cohorts, respectively (P < .001; Table 4).
Comparison of the Postoperative Complication Rates (Within 30 Days of Surgery) Between the Delayed and Nondelayed Cohorts Stratified Between Overall, Major, and Minor Complicationsa.
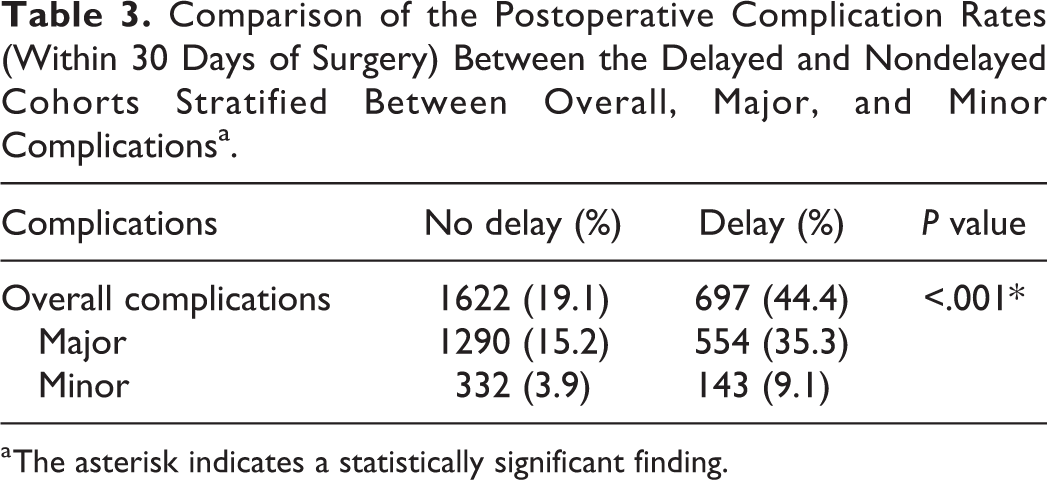
a The asterisk indicates a statistically significant finding.
Comparison of Specific Postoperative Complications (Within 30 Days of Surgery) Between Delayed and Nondelayed Cohortsa.
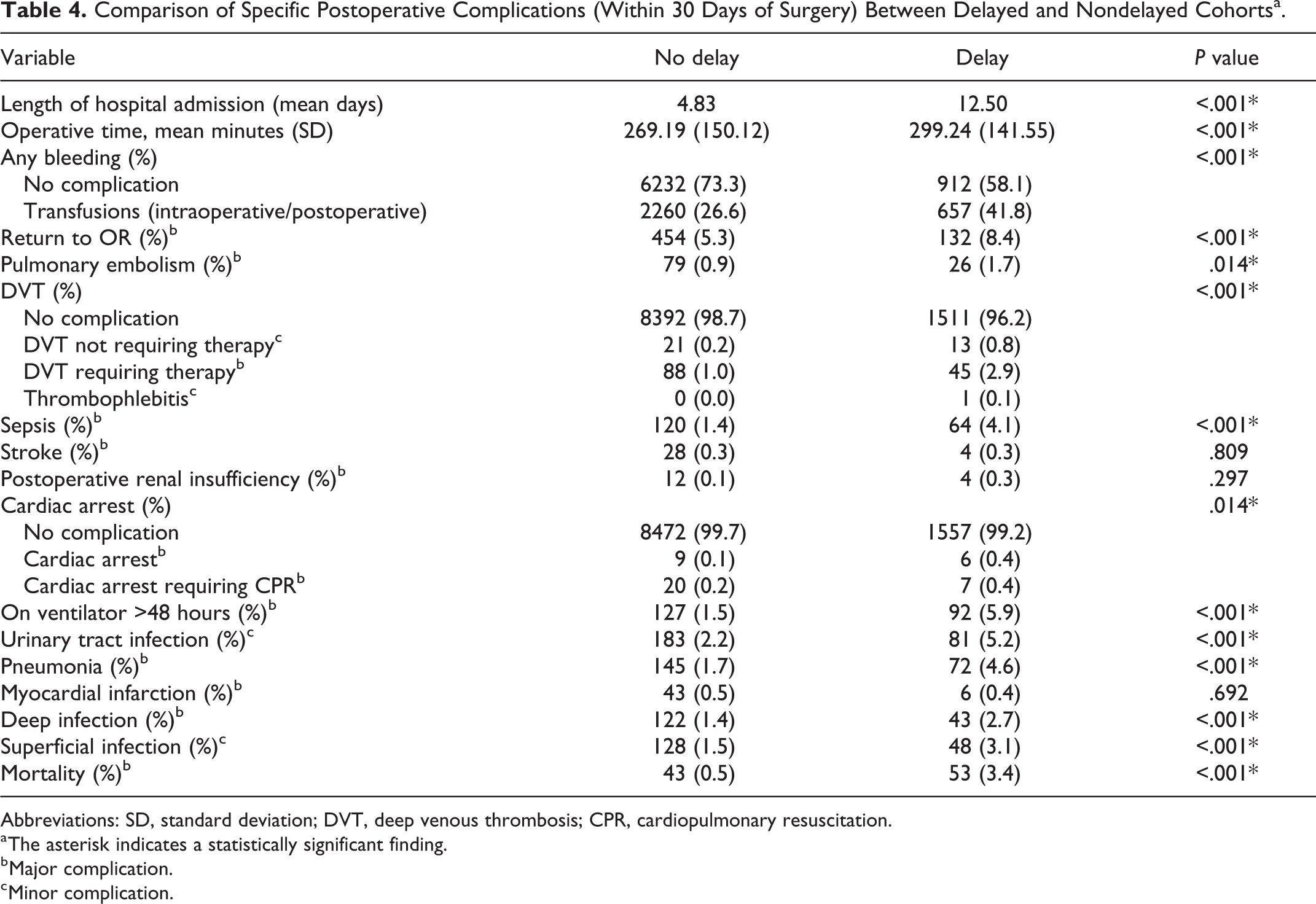
Abbreviations: SD, standard deviation; DVT, deep venous thrombosis; CPR, cardiopulmonary resuscitation.
a The asterisk indicates a statistically significant finding.
b Major complication.
c Minor complication.
Discussion
In this study, we identified the incidence of and risk factors associated with experiencing surgical delay in patients undergoing elective multilevel instrumented spinal fusion surgery for ASD. We found the incidence of delay prior to elective multilevel spinal fusion to be 15.6%, and multivariate analysis identified advanced age, male sex, ASA class 4, and a history of smoking as independent risk factors for surgical delay. The delayed cohort also experienced significantly longer operative times, prolonged ventilator times, and more lengthy hospital stays. Furthermore, we found that patients experiencing a delay had significantly higher complication rates postoperatively. Specifically, we found significantly higher rates of return to the operating room, VTE, UTI, pneumonia, superficial and deep wound infections, as well as sepsis in patients whose surgeries were delayed. Most strikingly, we found that the mortality rate in the delayed cohort was nearly 7-fold higher than in the nondelayed cohort. Although alarming, this finding further underscores the importance of recognizing the risk factors associated with surgical delay to help mitigate the risk of postoperative complication, improve patient outcomes, and reduce costs and resource burden to the healthcare system. Ultimately, we believe our findings suggest that patients who experience delay of their elective spinal deformity procedure on the day of surgery are unfit to undergo surgery at the time of delay, and either discharge with outpatient optimization must be undertaken to improve the modifiable risk factors we have identified (ie, ASA classification and smoking status), or consideration should be given to postponing the surgery indefinitely in those unable to be further optimized.
The rate of delay in this population is substantially higher than that reported for patients undergoing single-level lumbar fusion, 16 and is also much higher than the rates reported for primary total hip and total knee arthroplasty at 2.31% and 0.93%, respectively.14,15 However, the risk factors we have identified, as well as the higher complication rate in delayed patients, are similar to those reported by Wagner et al 16 in their analysis of patients undergoing single-level lumbar fusion. The authors found that male sex, ASA classes 3 and 4, and chronic steroid use are predictive for surgical delay. The authors also reported a multitude of significantly higher postoperative complications, including a 10-fold higher mortality rate, among patients experiencing a delay from the time of hospital presentation prior to undergoing a single-level lumbar fusion. 16 Elevated ASA class has also previously been reported as a risk factor for postoperative complications in spinal fusion surgery in other studies.16,18-20 Our findings suggest an association between incurring increased complications and extended operative times, which is corroborated by previous studies identifying longer operation time as predictive of developing postoperative complications.18-20 Our finding that smoking is associated with surgical delay is not surprising considering the myriad of deleterious effects smoking has on general health conditions.21,22 This association corresponds with our other findings that advanced age and an elevated ASA class, both factors which are indicative of poorer health, are also more likely to lead to a surgical delay. Consequently, our findings serve as an important step in recognizing modifiable and nonmodifiable risk factors associated with surgical delay in patients undergoing these complex surgeries.
Our multivariate analysis also demonstrated that a diagnosis of hypertension controlled on medications correlated with a reduced risk of delay. We hypothesize that this reduced risk of delay in patients undergoing treatment for hypertension may be due to a selection bias representing a segment of the patient population with greater access to health care. 23 This assertion presumes that patients diagnosed and treated for this condition, compared to affected patients who are not treated—regardless of official diagnosis—are more likely to have better management of their chronic conditions, and thereby, are less likely to experience a surgical delay.
Our findings have several limitations that are inherent to the retrospective design of the study and utilization of a multicenter database. Limitations derive from the lack of standardization in surgeon and anesthesia thresholds for initiating a delay, the length of the delay, and the exact cause of each delay within the database. Differing protocols followed at each participating hospital for addressing preoperative comorbidities and postoperative complications can potentially skew the results of this study and limit its generalizability. Although it is assumed that all the spinal deformity patients included in this study were undergoing elective multilevel fusions, it is likely that some presented with severe neurologic deficits that mandated surgery during the same hospital admission regardless of the patient’s underlying medical status. Furthermore, it is possible that some of the data is missing or incorrectly entered into the database. Finally, the postoperative complications identified in this study are restricted to those occurring within the short term, as the ACS-NSQIP database only accounts for the first 30 days following surgery. Despite these limitations, however, the ACS-NSQIP database is rigorously maintained, and as such, it is considered a “gold standard” database. It is also worth noting that the delineation between the major and minor complications was determined by the authors of the present study, which out of necessity was made in a subjective manner. Thus, we believe our findings represent an accurate assessment of the factors and complications associated with delay of multilevel fusion.
Conclusion
By analyzing a national, multicenter database comprising more than 10 000 patients, we found a 15.6% incidence of surgical delay beyond the day of hospital presentation for surgery in patients undergoing elective multilevel fusion for ASD. Patients of advanced age, male sex, ASA class 4, and a history of smoking cigarettes are at significantly greater risk for experiencing delay. Consequently, those who experience a surgical delay are more likely to develop postoperative complications, including a significantly higher risk of mortality. Our findings suggest that patients experiencing a delay prior to elective spinal fusion for ASD are medically unfit for surgery, and at a minimum, the procedure should be postponed until optimization of these risk factors can be achieved prior to any consideration of elective ASD surgery.
Footnotes
Authors’ Note
The views expressed in this article are those of the authors and do not reflect the official policy of the Department of the Navy, Department of the Army, Department of Defense, or the US government. Five authors are employees of the United States Government. This work was prepared as part of their official duties, and as such, there is no copyright to be transferred.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.