
Abstract
Study Design
Retrospective Cohort Study.
Objective
Restoration of lordosis in lumbar fusion reduces low back pain, decreases adjacent segment degeneration, and improves postoperative outcomes. However, the potential effects of changes in segmental lordosis on adjacent-level and global lordosis remain less understood. This study aims to examine the relationships between segmental (SL), adjacent-level, and global lumbar lordosis following L5-S1 Anterior Lumbar Interbody Fusion (ALIF).
Methods
80 consecutive patients who underwent single-level L5-S1 ALIF were divided into 3 groups based on the degree of change (∆) in index-level segmental lordosis: <5° (n = 23), 5°-10° (n = 29), >10° (n = 28). Radiographic parameters measured included global lumbar, segmental, and adjacent level lordosis, sacral slope, pelvic tilt, pelvic incidence, and PI-LL mismatch.
Results
Patients with ∆SL 5°-10° or ∆SL >10° both showed significant increases in global lumbar lordosis from preoperative to final follow-up. However, patients with ∆SL >10° showed statistically significant losses in adjacent level lordosis at both immediate postoperative and final follow-up compared to preoperative. When comparing patients with ∆SL >10° to those with ∆SL 5-10°, there were no significant differences in global lumbar lordosis at final follow-up, due to significantly greater losses of adjacent level lordosis in these patients.
Conclusion
The degree of compensatory loss of lordosis at the adjacent level L4-L5 correlated with the extent of segmental lordosis creation at the index L5-S1 level. This may suggest that the L4 to S1 segment acts as a “harmonious unit,” able to accommodate only a certain amount of lordosis and further increases in segmental lordosis may be mitigated by loss of adjacent-level lordosis.
Keywords
Introduction
Ever since Capenar described the first anterior approach spinal procedure for the treatment of spondylolisthesis in 1932, there have been robust advances which have allowed for Anterior Lumbar Interbody Fusion (ALIF) to become a well-accepted surgical technique used to treat a wide range of lumbar diseases such as spondylolisthesis, recurrent disc herniation, degenerative disc disease, foraminal stenosis, and sagittal imbalance.1-4 Over the years, the rate of ALIF procedures have rapidly increased with trends showing over 49,000 procedures between 2007 and 2014 with an average increase of 24.07% annually during this period. 5 This increase may be attributed to studies which have shown that ALIF procedures provide greater restoration of lordosis and foraminal height compared to other surgical approaches while also having low reoperation rates and avoiding violation of paraspinal muscles.1,3,6-9
In a recent retrospective study of 147 patients undergoing fusion by Sembreno et al, ALIFs were shown to have a statistically greater increases in segmental lordosis at 3.8° compared to posterior spinal fusions, lateral lumbar interbody fusion (LLIF), and transforaminal lumbar interbody fusion (TLIF). 10 ALIF procedures may be superior to other surgical approaches in improving segmental lordosis due to greater anterior column distraction as a result of releasing the anterior longitudinal ligament and the ability to place large footprint interbody cages.11-13 While the current literature has shown the relationship between ALIFs and improvements in segmental lordosis, there is little to no evidence outlining the connection between changes in segmental lordosis and its effect on global and adjacent segment lordosis.
Optimizing sagittal parameters is vital to maintaining adequate posture, reducing postoperative complications such as adjacent segment disease, and has also been reported to improve low back pain.14-16 A systematic review and meta-analysis of 13 studies by Chun et al reports a strong association between low back pain and loss of lumbar lordotic curvature. 16 The goal of the present study was to evaluate how changes in segmental lordosis may impact overall global lumbar and adjacent segment level lordosis following ALIF at L5-S1.
Material and Methods
A retrospective cohort study was performed of consecutive patients who underwent single-level ALIF with or without percutaneous instrumentation between 2004 and 2019 for a diagnosis of degenerative disc disease with disc space collapse and secondary foraminal stenosis or spondylolisthesis by a single spine surgeon. Informed consent was obtained, and this study received IRB approval (ORA #18072901). Cases were identified based on CPT code 22558 for anterior lumbar interbody fusion. A thorough review of the cohorts’ medical and radiographic records was performed to confirm the surgical procedures. Patients older than the age of 18, with obtainable operative and radiographic reports, that received a single-level ALIF at L5-S1 with minimum of 6 months follow-up were included in this study. Patients who received an ALIF at any other level, direct posterior decompression surgery, or any prior posterior fusion were excluded. All ALIFs were performed with anterior cages with integrated screws for fixation spanning the index level. None of the cases in this study were performed specifically to address complex spinal deformity. Nineteen patients (23.8%) in the cohort received supplemental percutaneous posterior instrumentation for the indication of isthmic spondylolisthesis. Seventy-six (95%) of the cohort received PEEK cages and 4 (5%) received titanium cages. Biologic graft used in the cohort included bone morphogenic proteins (BMP) (Medtronic, Memphis) (45/80 patients), Osteocel (Nuvasive, San Diego) (23/80 patients), Cancellous chips (8/80 patients), Autograft (4/80 patients). Patients were evaluated preoperatively, immediately postoperative (<4 weeks follow-up), and at final postoperative follow up. All patients presented with collapsed L5-S1 discs with secondary reduction in foraminal dimensions. The surgical goals in all cases were to increase posterior disc height to provide indirect decompression and restore L5-S1 lordosis. Interbody cages were selected with the goal of increasing posterior disc height by 2-4 mm and the lordotic angle of the cage was then selected based on achieving restoration of normal L5-S1 lordosis of approximately 16-24°.15,17,18 In the setting of isthmic spondylolisthesis, percutaneous posterior instrumentation was used to provide greater stability and additional fixation at L5-S1. Pre-op PI-LL mismatch was calculated routinely and when required an attempt was made to establish this within published normal values. It should be noted that in the patient cohort the mean pre-op PI-LL mismatch value was 2.13°.
Radiographic Analysis
Three orthopedic spine surgery fellows independently reviewed all standing anteroposterior (AP) and lateral radiographs taken preoperatively, immediate postoperatively, and at final follow up. All 3 readers independently assessed all images, and after a short training period, intra- and interobserver reliability was deemed to be good to excellent (intraclass coefficient constant [ICC] > .80). ICC cutoffs were established as .50 for poor reliability, .51 to .74 for moderate, .75 to .89 for good, and .90 for excellent. 19 Each radiograph was measured for Global Lordosis across the lumbar spine, operative level Segmental Lordosis, Sacral Slope, Pelvic Tilt, and Pelvic Incidence. Global Lumbar Lordosis was measured from the superior endplate of L1 to the superior endplate of S1. L5-S1 Segmental Lordosis was measured from the superior endplate of L5 to the superior endplate of S1. Sacral slope was measured as the angle between a horizontal reference line and the superior sacral end plate. Pelvic tilt was measured as the angle between a vertical reference line and a line from the midpoint of the sacral end plate to the center of the femoral heads. Pelvic incidence is described as an angle formed by a line drawn from the center of the femoral heads to the midpoint of the sacral end plate and a line perpendicular to the midpoint of the sacral end plate. Pelvic incidence – lumbar lordosis (PI-LL) mismatch was calculated as the difference of pelvic incidence and lumbar lordosis.
Statistical Analysis
Statistical analysis was performed using STATA version 15.1 (StataCorp, College Station, TX). Continuous baseline variables were reported as mean ± standard deviation (SD). Baseline patient demographics and operative characteristics were compared using independent t-tests and chi-square analysis for continuous and categorical variables, respectively. Multivariate linear and logistic regressions were performed to analyze the relationship between various cage angles and radiographic outcomes. Multivariate regressions controlled for age, sex, BMI, smoking status, uncomplicated diabetes, use of percutaneous posterior instrumentation, ASA score, and surgical level. Scatter plots and Pearson correlation coefficients were used for analysis of quantitative relationships. A P-value of <.05 was used to determine statistical significance.
Results
Demographics by Changes in Segmental Lordosis.
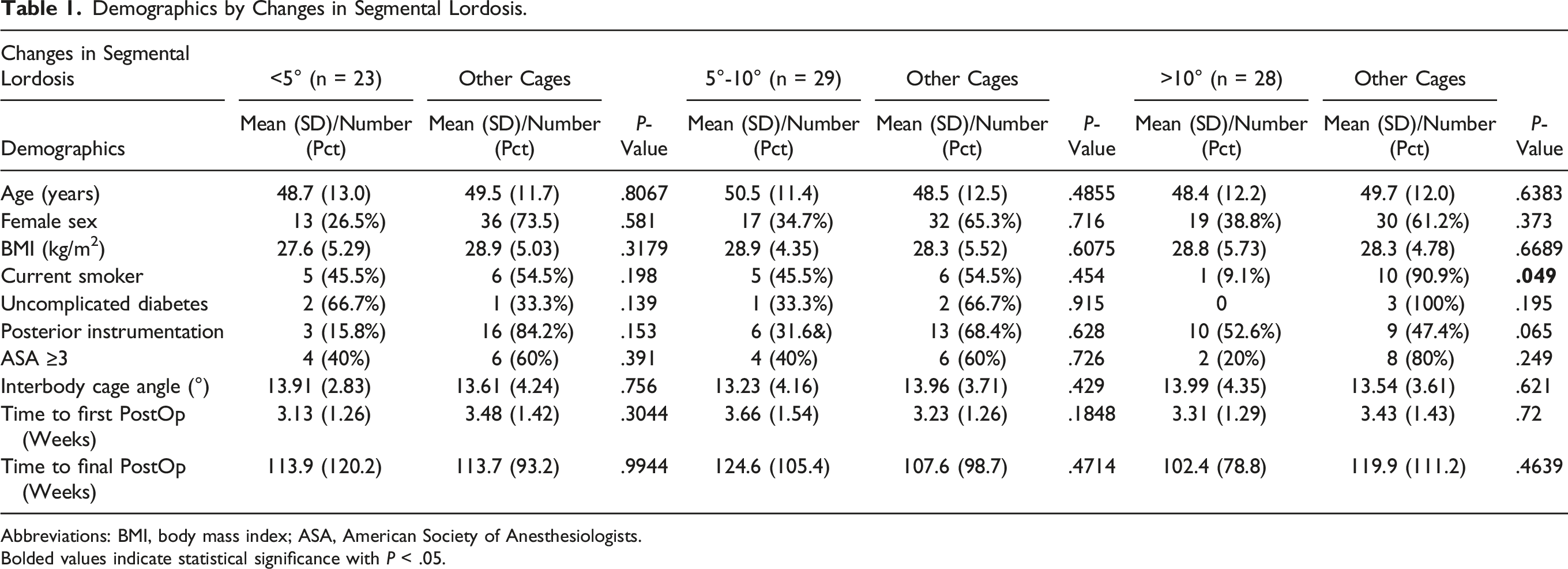
Abbreviations: BMI, body mass index; ASA, American Society of Anesthesiologists.
Bolded values indicate statistical significance with P < .05.
When evaluating the changes in lordosis measurements following L5-S1 ALIF, patients with changes in segmental lordosis <5° showed no significant differences in global, or adjacent segment level (L4-L5) lordosis, sacral slope, pelvic tilt, pelvic incidence, or PI-LL mismatch from preoperative to both immediate postoperative and final follow-up. Following L5-S1 ALIF, patients with a change in segmental lordosis of 5°-10° showed significant increases in index level lordosis at immediate postoperative follow up compared to preoperatively (P = <.001). However, compared to preoperative measurements, these patients experienced no significant changes in global lordosis likely a result of a decrease in adjacent segment level (L4-L5) lordosis (2.1° loss; P = .0048) at the immediate postoperative period. At final follow-up, patients with a change in segmental lordosis 5°-10° showed statistically significant increases in both index level (P = <.001) and global lordosis (3.7° increase; P = .0427). Further, patients with a change in segmental lordosis 5°-10° showed no significant difference in adjacent level L4-L5 lordosis, sacral slope, pelvic tilt, or pelvic incidence at final follow-up.
Effect of ALIF on Sagittal and Spinopelvic Parameters by Changes in Segmental Lordosis.
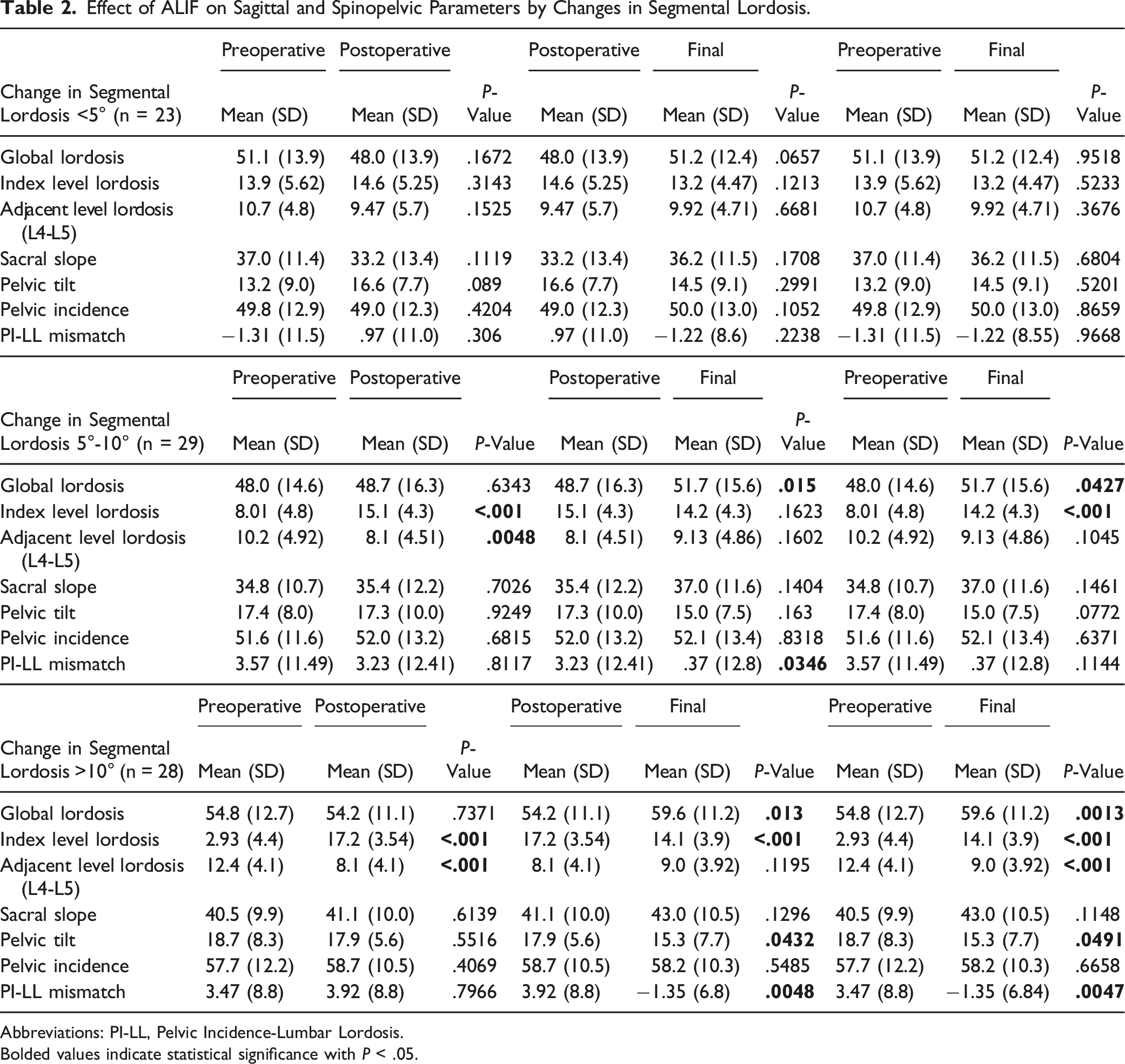
Abbreviations: PI-LL, Pelvic Incidence-Lumbar Lordosis.
Bolded values indicate statistical significance with P < .05.
Effect of Changes in Segmental Lordosis on Sagittal and Spinopelvic Parameters.
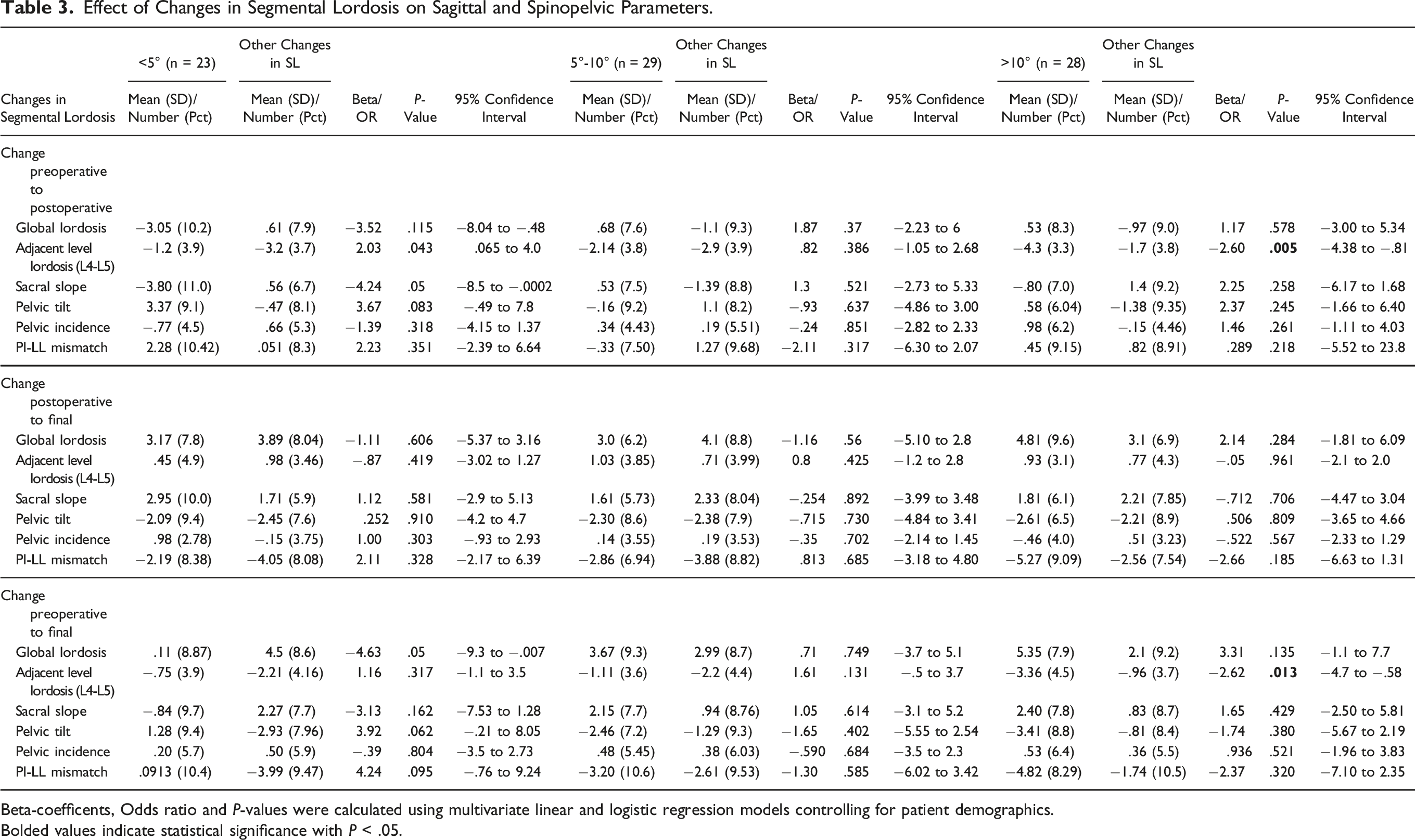
Beta-coefficents, Odds ratio and P-values were calculated using multivariate linear and logistic regression models controlling for patient demographics.
Bolded values indicate statistical significance with P < .05.
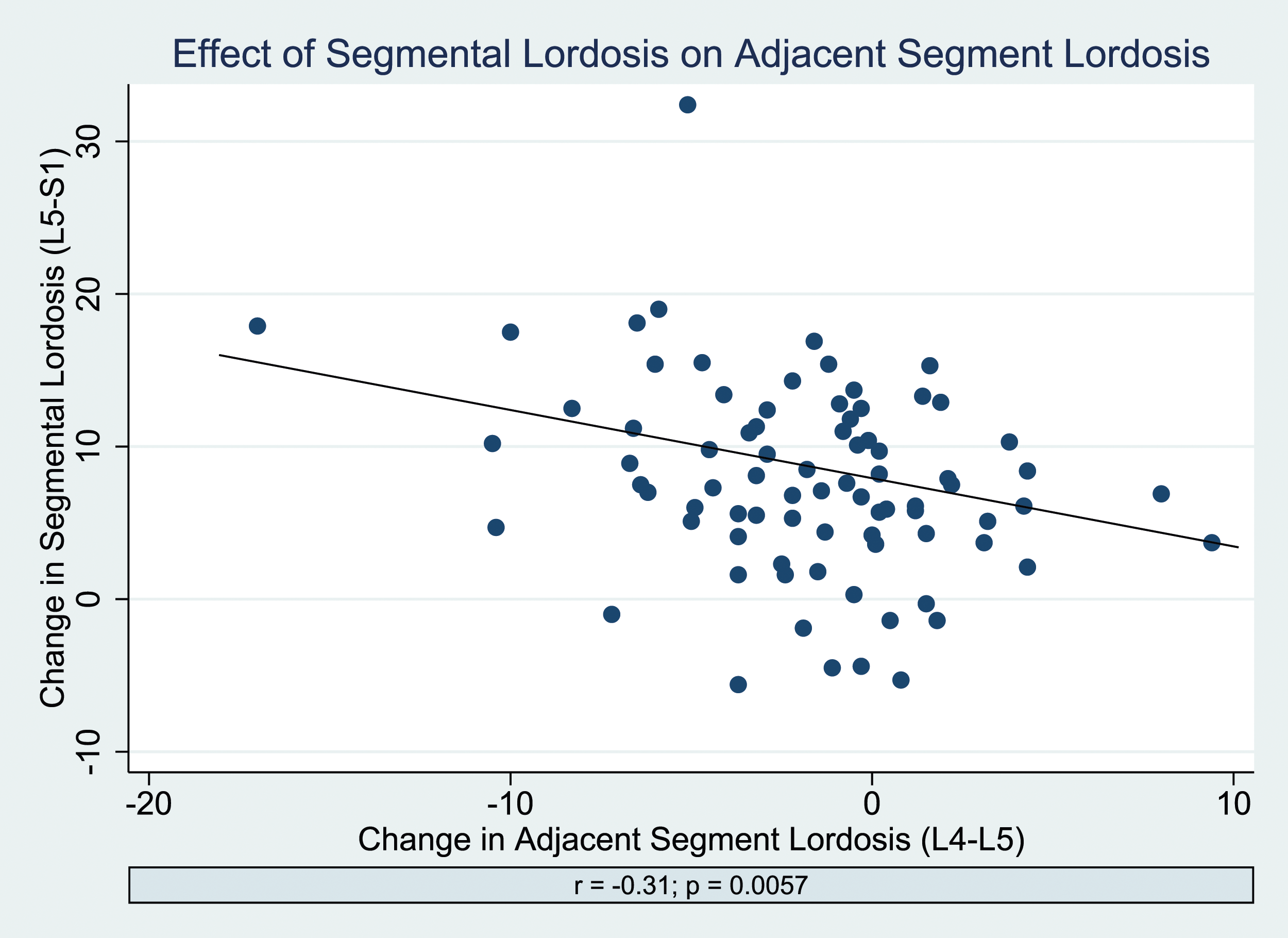
A scatter plot showing the correlation between changes in index segmental lordosis at L5-S1 and adjacent segment lordosis at L4-L5.
Discussion
Appropriately corrected sagittal alignment has been consistently associated with better postoperative clinical outcomes following lumbar fusion procedures.14-16,20,21 While the current body of literature shows significant improvements in index level segmental lordosis following ALIF surgery, the relationship between changes in segmental lordosis on global lumbar and adjacent segment level lordosis remains unclear.3,8,13 Our aim was to assess these sagittal parameters in patients who underwent L5-S1 ALIF.
In this study, we examined how various changes in index level segmental lordosis impacted the overall global lumbar lordosis as well as the lordosis at the adjacent segment level (L4-L5). Our results indicate that patients with changes in segmental lordosis of <5° had no significant changes in global or adjacent segmental lordosis at either immediate or final postoperative compared to preoperative evaluations. Meanwhile, patients with changes in segmental lordosis 5°-10° or >10° demonstrated significant improvements in index level segmental lordosis at both immediate and final postoperative follow-up as well as significant increases in global lumbar lordosis at final follow up compared to preoperative.
Previously, a retrospective cohort study by Afathi et al reported a statistically significant improvement in segmental lordosis by 4.02° following 1 or two-level standalone ALIF or LLIF procedures, but no changes in overall global lordosis. 22 This finding is consistent with the our results demonstrating lack of improvement in global lumbar lordosis when segmental lordosis is not maximized to at least 5° increase compared to preoperative measurements.
While both changes in segmental lordosis 5°-10° or >10° demonstrated significant improvements in global lumbar lordosis at final follow-up, patients with changes in segmental lordosis >10° showed significant decreases in adjacent segmental lordosis (L4-L5) at final follow up compared to preoperative. When comparing between all 3 groups, patients with changes in segmental lordosis >10° showed significantly greater losses in adjacent segmental lordosis (L4-L5) at both immediate postop and final follow up compared to both other groups with changes in segmental lordosis <10°. The degree of compensatory loss of lordosis at L4-L5 correlated with the extent of lordosis creation at the index L5-S1 level as shown in Figure 1. These findings may suggest that the L4 to S1 segment acts as a “harmonious unit,” able to accommodate only a certain amount of lordosis and further increases in segmental lordosis may be mitigated by loss of adjacent segment lordosis. This finding is further supported by other studies in the literature which have also reported an association between increased segmental lordosis following ALIF surgery leading to decreases in adjacent segment lordosis.10,13 For instance, in a large multicenter retrospective study of 474 patients undergoing interbody fusion for degenerative lumbar pathology by O’Connor et al, ALIF/LLIF patients experienced significantly greater increases in segmental lordosis compared to TLIF/PLIF patients, but had significantly greater losses of adjacent segment lordosis. 13
In addition to significant improvements in global lumbar lordosis, we did find greater segmental lordosis to be associated with significant improvement in PI-LL mismatch. Specifically, change in segmental lordosis of 5-10° trended towards a significant decrease in PI-LL mismatch when comparing final measurements (P = .1144). Moreover, change in lordosis of >10° demonstrated significant decrease in PI-LL mismatch when comparing both preoperative and postoperative measurements to final radiographs. The importance of congruency in PI and LL has been well established in the spinal deformity literature, with mismatch >10° associated with greater risk of adjacent segment disease and/or revision surgery, and improvements in PI-LL mismatch associated with higher likelihood of achieving clinical improvements in health-related quality of life outcomes.23-27 Interestingly, in a study of asymptomatic patients, the mean PI-LL mismatch was found to be −5.4° ± 10.7°, a value much lower than the commonly cited <10° difference threshold for spinal deformity. In our study, we found segmental lordosis change >10° to result in a final PI-LL mismatch of −1.35 (Table 2), much closer to the physiologic range found in asymptomatic patients. 25 Despite this, the influence of PI-LL mismatch on clinical outcomes in short segment lumbar fusions remains less clear, with literature available that argues for and against an association of PI-LL mismatch with improved PROMs.28,29
While our study evaluated the effect of changes in segmental lordosis on global and adjacent level lordosis, the effectiveness of ALIF in restoring more physiologic sagittal alignment has been well established. In a study by Ahlquist et al ALIF and LLIF were both found to significantly improve segmental lordosis, lumbar lordosis, anterior disc height, posterior disc height, and foraminal height. 30 Moreover, they found ALIF to be the most effect surgical approach in maximizing segmental lordosis. However, these authors did not evaluate the relationship between segmental lordosis creation and its impact on global lumbar or adjacent segment lordosis. The present study’s findings show that while ALIF can be used to achieve greater restoration and correction of segmental lordosis, there is a reciprocal loss of adjacent segment lordosis observed after >10° of correction. Thus, our study demonstrates cases with more advanced degrees of correction with L5-S1 ALIF may come at the expense of adjacent segment lordosis at L4-5. The long-term effect of these adjacent segment changes is a source for future investigation.
Despite providing novel evidence on the relationship between the changes in segmental lordosis on global and adjacent level lordosis, this study is not without limitations. As with all studies that are retrospective in design, our study may be subject to potential selection biases. Further, due to the nature of this radiographic study, sagittal parameters were not correlated with long term clinical outcomes. However, since surgeons still depend on intraoperative radiographs to assess for adequate restoration of sagittal alignment and improve foraminal dimensions, there is value in understanding the relationship of segmental lordosis creation on sagittal balance.
The findings of this study are strengthened by a follow-up time of over 2 years on average as well as strict inclusion criteria with high internal validity as our cohort examined L5-S1 ALIF procedures without any prior fusions or direct posterior decompression procedures. Furthermore, this study aimed to illustrate a relationship between changes in segmental lordosis and its effect on global lumbar and adjacent level lordosis that has not been directly described before in the current body of literature.
Conclusion
When analyzing the effects of changes in segmental lordosis on sagittal alignment after L5-S1 ALIF, the degree of compensatory loss of lordosis at the adjacent level L4-L5 significantly correlated with the extent of segmental lordosis creation at the index L5-S1 level. These findings may suggest that the L4 to S1 segment acts as a “harmonious unit,” able to accommodate only a certain amount of lordosis and further increases in segmental lordosis may be mitigated by loss of adjacent segment lordosis.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.