
Abstract
Study Design
A single centre retrospective review.
Objective
Recent studies have suggested that distal lordosis (L4-S1, DL) remains constant across all pelvic incidence (PI) subgroups, whilst proximal lordosis (L1-L4, PL) varies. We sought to investigate the impact of post-operative DL on adjacent segment disease (ASD) requiring reoperation in patients undergoing lumbar fusion for degenerative conditions.
Methods
Patients undergoing 1-3 level lumbar fusion with the two senior authors between 2007-16 were included. Demographic and radiographic data were recorded. Univariate, multivariate binary logistic regression, and Kaplan Meier survivorship analyses were performed.
Results
335 patients were included in the final analysis. Most had single (67%) or two (31%) level fusions. The mean follow-up was 64-month. Fifty-seven patients (17%) underwent reoperation for ASD at an average of 78-month post-operatively (R group). The R group had a significantly lower mean post-operative DL (27.3 vs 31.1 deg, P < .001) and mean PI (55.5 vs 59.2 deg, P < .05). On univariate analysis, patients with a post-operative DL of <35 deg had higher odds of reoperation for ASD than those with a post-operative DL of ≥35 deg (OR 2.7, P = .016). In the multivariate model, post-operative DL, low/average PI, and spondylolisthesis were all significantly associated with reoperation for ASD.
Conclusion
This study provides preliminary support to an association between post-operative distal lumbar lordosis and risk of reoperation for ASD in patients undergoing fusions for degenerative conditions. Further multicentre prospective study is needed to independently confirm this association and identify the impact of restoration of physiological distal lumbar lordosis on long term patient outcomes.
Keywords
Introduction
The utilisation of lumbar spinal fusion for degenerative conditions and associated costs have increased markedly over the past two decades. 1 Whilst most patients experience an improvement in pain and disability, a subset of patients experience delayed symptom recurrence due to symptomatic adjacent segment degeneration. The aetiology of this adjacent segment disease (ASD) is controversial but is most commonly believed to be a consequence of increased biomechanical strain accelerating the natural degenerative process at the level above or below a rigid lumbar arthrodesis.2,3
The reported prevalence of ASD varies widely based on whether/which radiographic and/or clinical criteria are used. Long term follow-up Magnetic Resonance Imaging (MRI) has demonstrated radiographic development of adjacent segment stenosis in over two-thirds of patients following lumbar fusion. 4 A recent meta-analysis reported an ASD rate of 17.2% across 22 studies using a combination of radiographic and clinical criteria. 5 Reported reoperation rates for symptomatic ASD range from 9.9%–22.2% at 10 years with an approximate annual incidence of 2.5%/year.2,4
A broad number of risk factors for ASD have been variably reported and refuted including age, body mass index, number of levels fused, decompression at the level adjacent to a fusion, violation of the superior facet, pre-existing superior facet and/or disc degeneration, floating fusions, pelvic incidence and lumbar sagittal alignment.2,4-8 Of these, only preservation of the superior segment facet complex and lumbar sagittal alignment represent intra-operatively modifiable factors once the decision to perform a lumbar fusion has already been made.
The importance of lumbar sagittal alignment has been well established in patients undergoing long fusions for adult spinal deformity. 9 These studies have typically focused on aligning global lumbar lordosis with pelvic incidence, a marker of individualised spinopelvic morphology (PI-LL mismatch). Whilst PI-LL mismatch has also been linked to patient outcomes in short fusions for degenerative conditions,10-14 it represents a more challenging alignment parameter to target when surgery is limited to only one-two level fusions of the distal lumbar spine.
More recently, segmental lumbar lordosis has been shown to be linked with spinopelvic morphology with distal (L4-S1) lumbar lordosis remaining constant across pelvic incidence subgroups whilst proximal (L1-4) lordosis varies. 15 Restoration of this distal lumbar lordosis (DL) has been linked with achieving overall alignment targets in adult spinal deformity patients. 16 We sought to investigate whether restoration of distal lordosis was linked to the risk of reoperation for ASD in patients having short fusions for degenerative conditions in the distal lumbar spine. The primary objective of this study was to determine whether there was an association between post-operative distal lordosis and reoperation for ASD. The secondary objectives of the study were to determine whether pelvic incidence and restoration of the physiological 35-degree distal lordosis reported by Pesenti et al 15 influenced the risk of reoperation for ASD.
Methods
Patient Selection
A retrospective review of patients undergoing lumbar fusion with the two senior authors at our institution between 2007-16 was performed. Adult patients having contiguous 1-3 level lumbar posterolateral and/or interbody fusions for spondylolisthesis or other degenerative conditions were included. Patients with a history of prior thoracic or lumbar spine surgery, or underlying spinal tumours were excluded. Patients were followed up at 6-week, 6-month, and then yearly from 1-year post-surgery. Ethics approval was obtained for the University Health Network Research & Ethics Board (#19-6278). Informed consent was waived for this study.
Data Collection
Patient demographic data, surgical data and reoperation data were collected from an existing database. Radiographic parameters including pelvic incidence, segmental lumbar lordosis and adjacent disc characteristics were measured on standing pre-operative and first post-operative radiographs by authors 1-6. Verification of recorded radiographic parameters were performed in a portion of the cohort by authors 1 and 2. Definitions and measurement techniques are provided in Figure 1. Patients were divided into ASD reoperation (R) or no ASD reoperation (NR) groups and categorised into subgroups based on pelvic incidence (low <45 deg; average 45-60 deg; high >60 deg) and post-operative distal lordosis (<35 deg; ≥35 deg).
15
Final follow-up was defined at the date of the last review with radiograph in the NR group and the date of revision surgery for ASD in the R group. Measurement of radiographic spinal parameters Pelvic incidence: angle between a line drawn from the mid-point of the femoral heads to the midpoint of the sacral endplate and a line perpendicular to the sacral endplate Distal lumbar lordosis: angle between the L4 superior endplate and the sacral endplate.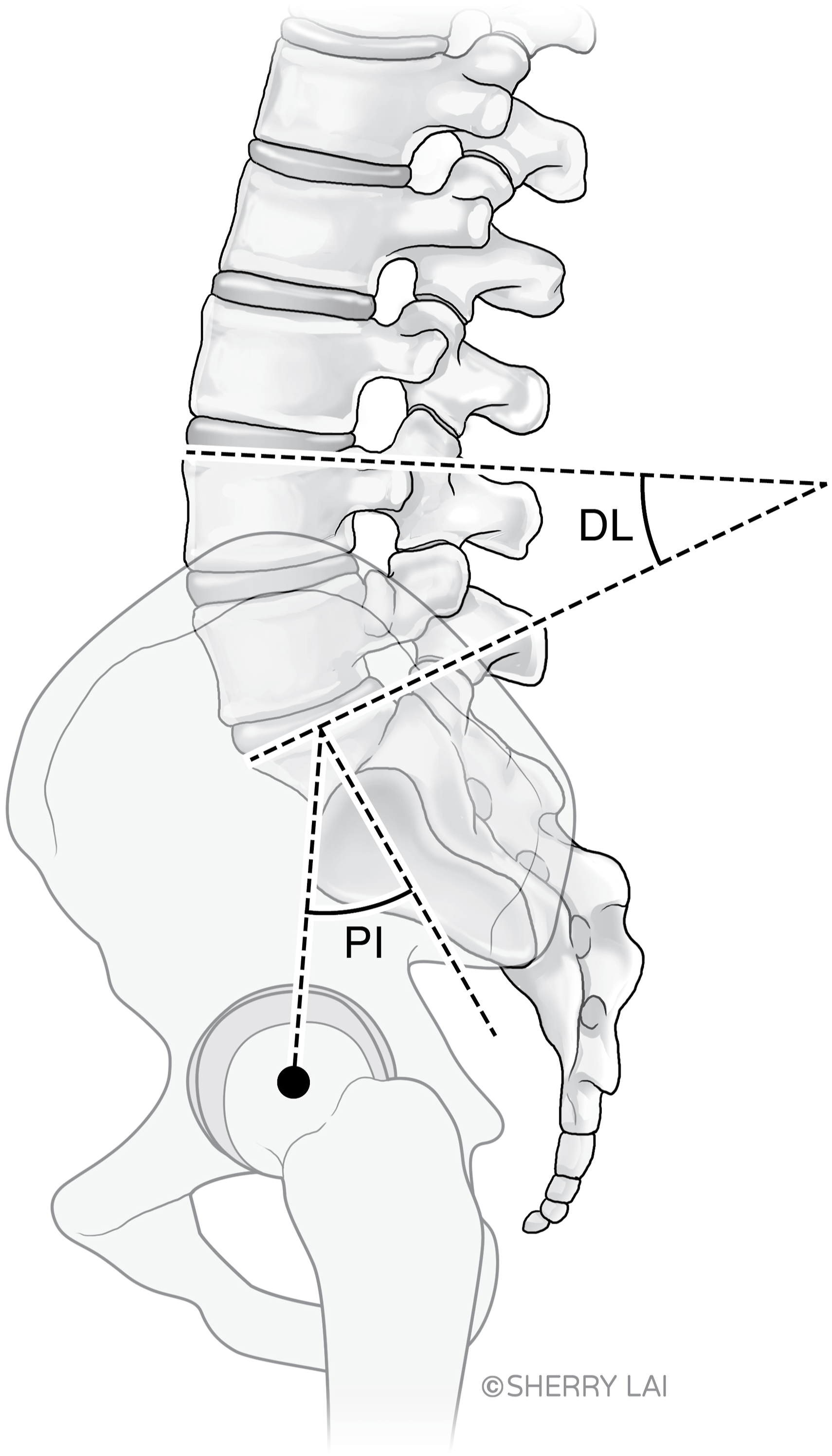
Statistical Analysis
Statistical analysis was performed using SPSS software Version 28 (IBM Corporation, Armonk, NY). Univariate analysis was performed using Pearson Chi square for categorical variables and univariate binary logistic regression analysis for continuous variables. Multivariate binary logistic regression analyses were then performed to identify factors associated with the risk of reoperation for ASD. Final multivariate model section was optimised using Bayesian and Akaike Information Criterion as well as through assessment of Receiver Operating Characteristic curves. Finally, a Kaplan-Meier analysis was performed to assess the reoperation free survival of various subgroups delineated in the regression analysis. Significance was set at a P value of .05.
Results
Between 2007-16, 341 patients had short lumbar fusions performed by the senior authors. Of these, 335 met the inclusion criteria and were included in the final analysis. Six of these patients were excluded from the study. This was due to the presence of prior thoracic scoliosis surgery in 3 patients, an underlying tumour in 2 patients, and a history of prior lumbar spine surgery in 1 patient. The mean age of patients in the cohort was 56.4 years and there was a slight female predominance (M:F 1:1.2). The majority of patients had surgery for a symptomatic spondylolisthesis (70%) with the remainder having other degenerative conditions such as isolated foraminal stenosis or degenerative disc disease. Most patients were treated with a single level fusion (67%) or two-level fusion (31%). Of the five patients treated with a 3-level fusion, 4/5 had fusion from L4-Pelvis and the remaining patient had an L3-S1 fusion. The fusion incorporated the distal lumbar spine (L4/5 and/or L5/S1 segment) in 327/335 (98%) patients. The remaining 2% had single level fusion at the L3/4 level.
Cohort Characteristics.
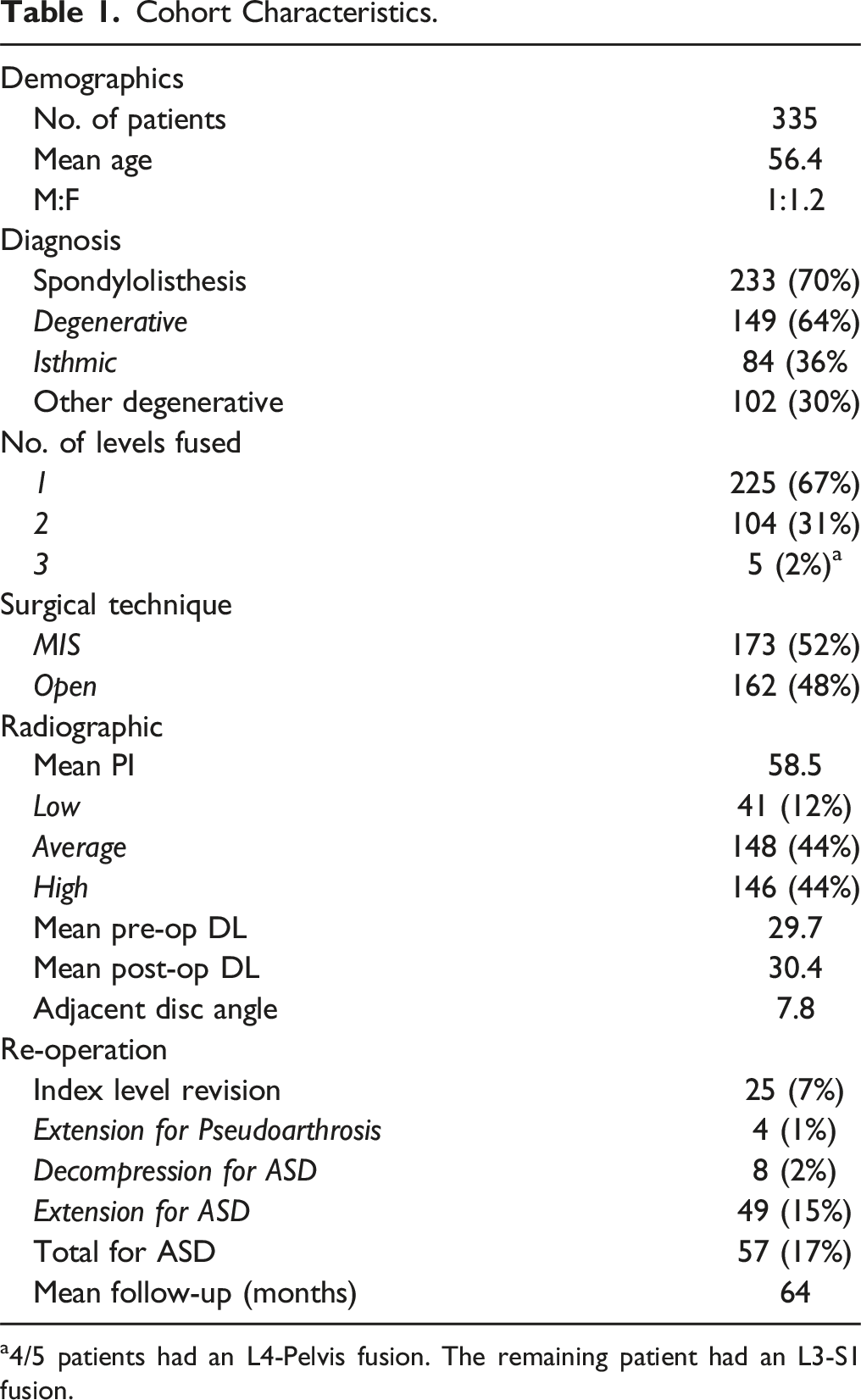
a4/5 patients had an L4-Pelvis fusion. The remaining patient had an L3-S1 fusion.
ASD Reoperation and No.
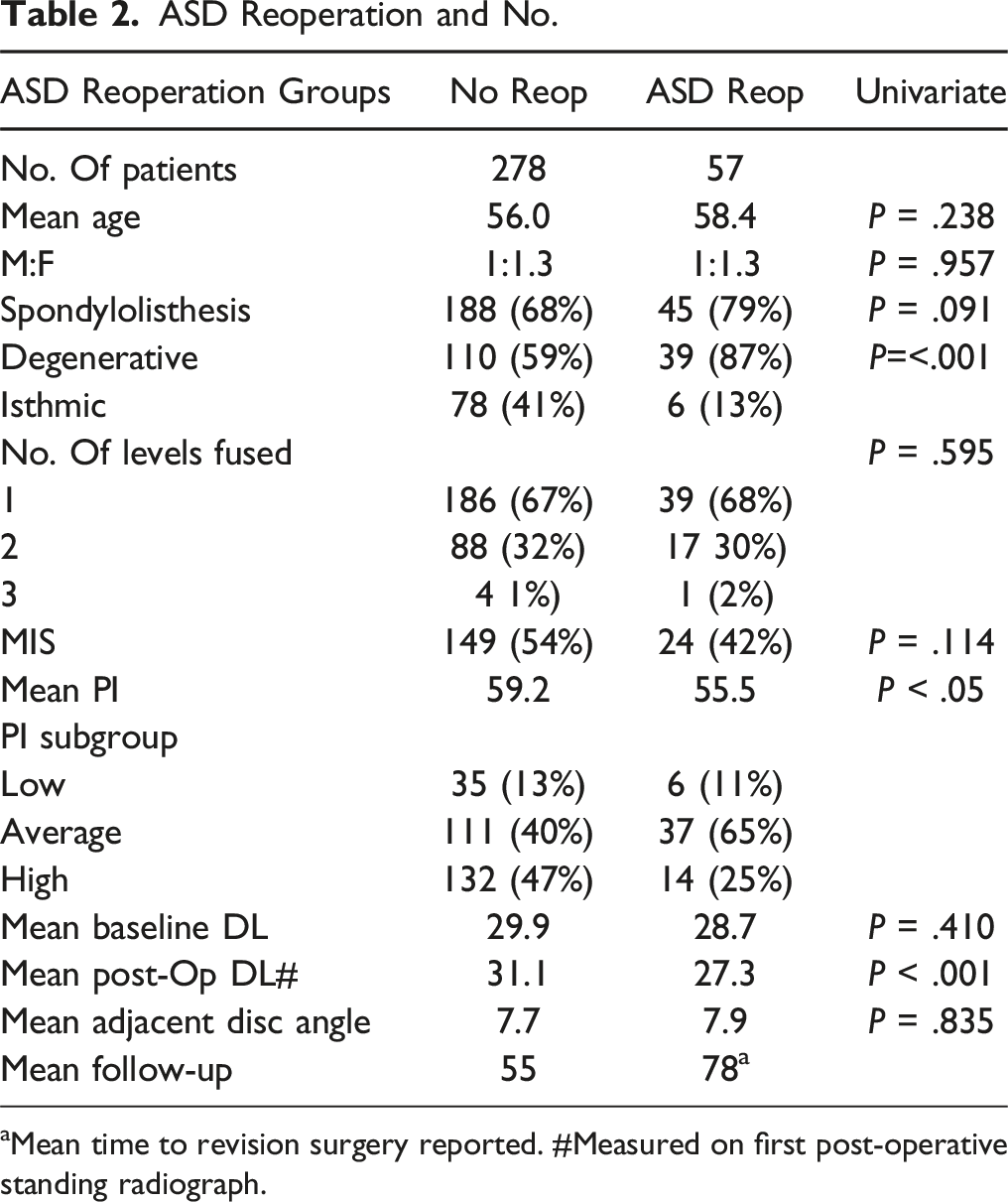
aMean time to revision surgery reported. #Measured on first post-operative standing radiograph.
On univariate analysis, there was no significant difference between the R and NR groups on the basis of age, sex, underlying diagnosis, single vs multi-level fusion, surgical technique, baseline distal lordosis or adjacent disc angle. The R group had a significantly lower mean post-operative distal lordosis (27.3 vs 31.1 deg, P < .001) and mean pelvic incidence (55.5 vs 59.2 deg, P < .05) than the NR group. Patients with a post-operative distal lordosis of <35 deg had higher odds of reoperation for ASD than those with a post-operative distal lordosis of ≥35 deg (OR 2.7, 95% CI 1.2-6.0, P = .016). The mean post-operative follow-up was longer in the R group (110 vs 55 months).
After categorisation of patients based on PI subgroup, 76% of patients in the R subgroup and 53% of patients in the NR subgroup were found to have a low or average PI. Patients with a low or average PI were found to have higher odds of reoperation for ASD than those with a high PI (OR 2.8, 95% CI 1.4-5.3, P = .001). When these PI and DL subgroups were combined, the highest ASD reoperation rate was seen in those patients with a low or average PI and post-operative distal lordosis <35 deg (reoperation rate 24%, Figure 2). ASD reoperation by combined PI-DL subgroup.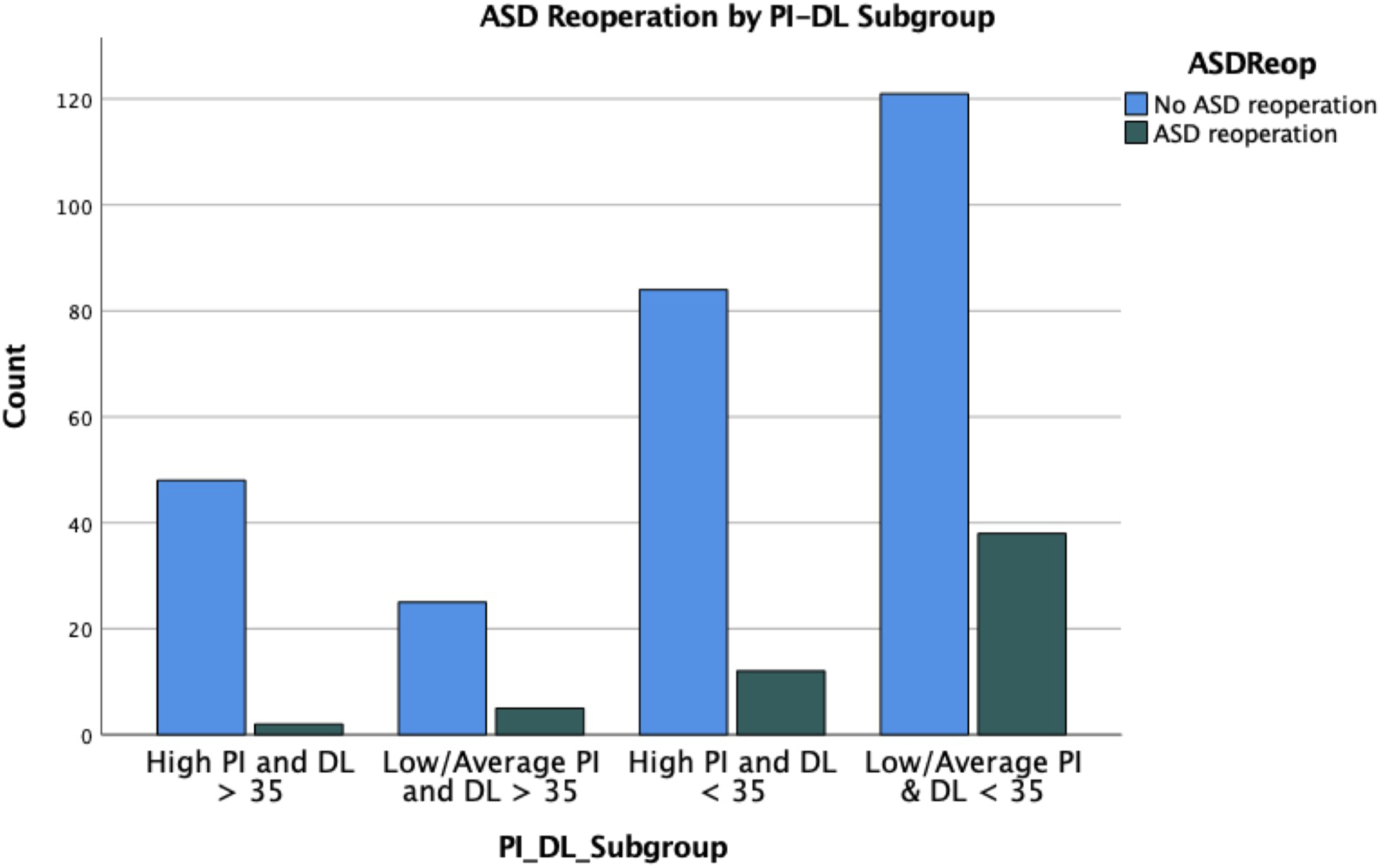
Optimum multivariate model fit was obtained when age, PI (low/average vs high), post-operative distal lordosis, single vs multi-level fusion, and underlying diagnosis (spondylolisthesis vs other) were included (AUC .71). In this multivariate model, post-operative distal lordosis, low/average PI, and spondylolisthesis were associated with reoperation for ASD. Each degree increase in post-operative distal lordosis afforded odds reduction against ASD reoperation (OR .89, 95% CI 0.90-.98, P = .006). A low/average PI increased the odds of ASD reoperation (OR 3.0, 95% CI 1.5-6.0, P = .002). The presence of a spondylolisthesis increased the odds of ASD reoperation (OR 2.3, 95% CI 1.1-4.8, P = .023). When the patients with a spondylolisthesis were divided into isthmic or degenerative subgroups, there was a significant association between the presence of a degenerative spondylolisthesis and the odds of ASD reoperation (P < .001, OR 4.6, 95% CI 1.9-11.4).
When ASD reoperation was investigated in a time dependent manner with a Kaplan-Meier analysis, there was a trend towards a longer reoperation free survival in the post-operative distal lordosis ≥35 deg subgroup that did not reach statistical significance (median estimated ASD reoperation free survival 149 vs 136 months, P = .076). When PI and DL subgroups were combined, there was a significantly shorter estimated median reoperation free survival in the subgroup with a low/average PI and DL <35 deg (115 vs 137-159 months, P = .029; Figure 3). Kaplan Meier ASD reoperation free survival curves for distal lordosis and combined pelvic incidence and distal lordosis subgroups.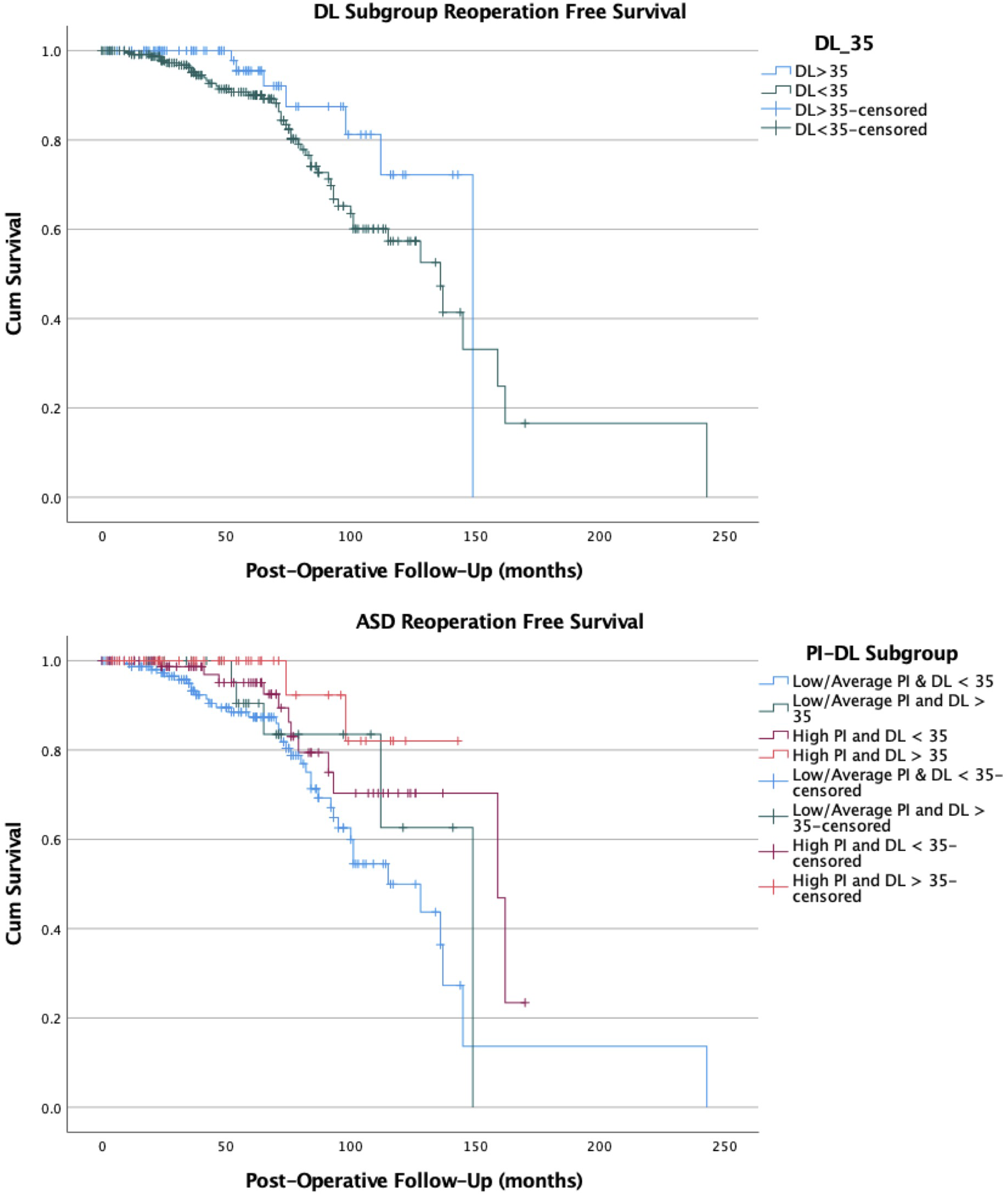
Discussion
Reoperation for symptomatic adjacent segment disease is an important cause of delayed morbidity after short lumbar fusion for degenerative conditions. The incidence of reoperation for ASD was 17% in this series at a mean follow-up period of just over 5 years. Whilst a variety of risk factors have been reported in the literature, few are modifiable and none have consistently been shown to be associated with the risk of reoperation for ASD. Previous investigation into surgical factors contributing to ASD reoperation risk have highlighted proximal facet violation, performing a decompression adjacent to a fusion and lumbar sagittal alignment as potential modifiable factors contributing to ASD reoperation risk.2,4-8
It is well established that the lumbar sagittal profile is related to pelvic incidence, a metric of individualised spinopelvic morphology. 18 Until recently, most analysis of lumbar sagittal alignment has focused on the discrepancy between global lumbar lordosis and pelvic incidence (PI-LL mismatch).8-12,19 This provides a reasonable alignment metric in patients undergoing long multilevel spinal deformity surgery but is more difficult to optimise in patients undergoing short lumbar fusions for degenerative conditions. Pesenti et al 15 (2018) reported that in asymptomatic adult patients, proximal (L1-L4) lordosis varies across PI subgroups whilst distal (L4-S1) lordosis remains constant at approximately 35 °. We sought to investigate whether restoration of 35 degrees of distal lumbar lordosis was associated with the risk of reoperation for ASD in patients undergoing short lumbar fusions for degenerative conditions
In this series, both pelvic incidence and post-operative distal lordosis were associated with the risk of reoperation for ASD on both univariate and multivariate analysis. In patients with a post-operative DL of <35°, the odds of reoperation for ASD were increased by 2.7-fold when compared to those patients with a post-operative DL of ≥35°. This association appeared to be relative to the amount of post-operative DL, with a larger odds of ASD reoperation seen in those patients with <25 degrees of post-operative DL (OR2.9, 95% CI 1.5-5.4, P < .001) and a trend towards a lower odds of ASD reoperation in those with a post-operative DL of >40° (OR0.3, 95% CI 0.1-1.1, P = .061) (Figure 4). (A) NR group patient with post-operative distal lordosis of 37 degrees. (B) Post-operative R group patient with post-operative distal lordosis of 21 degrees. Progressive, symptomatic degenerative changes in L3/4 and L2/3 discs leading to eventual extension of fusion to L2.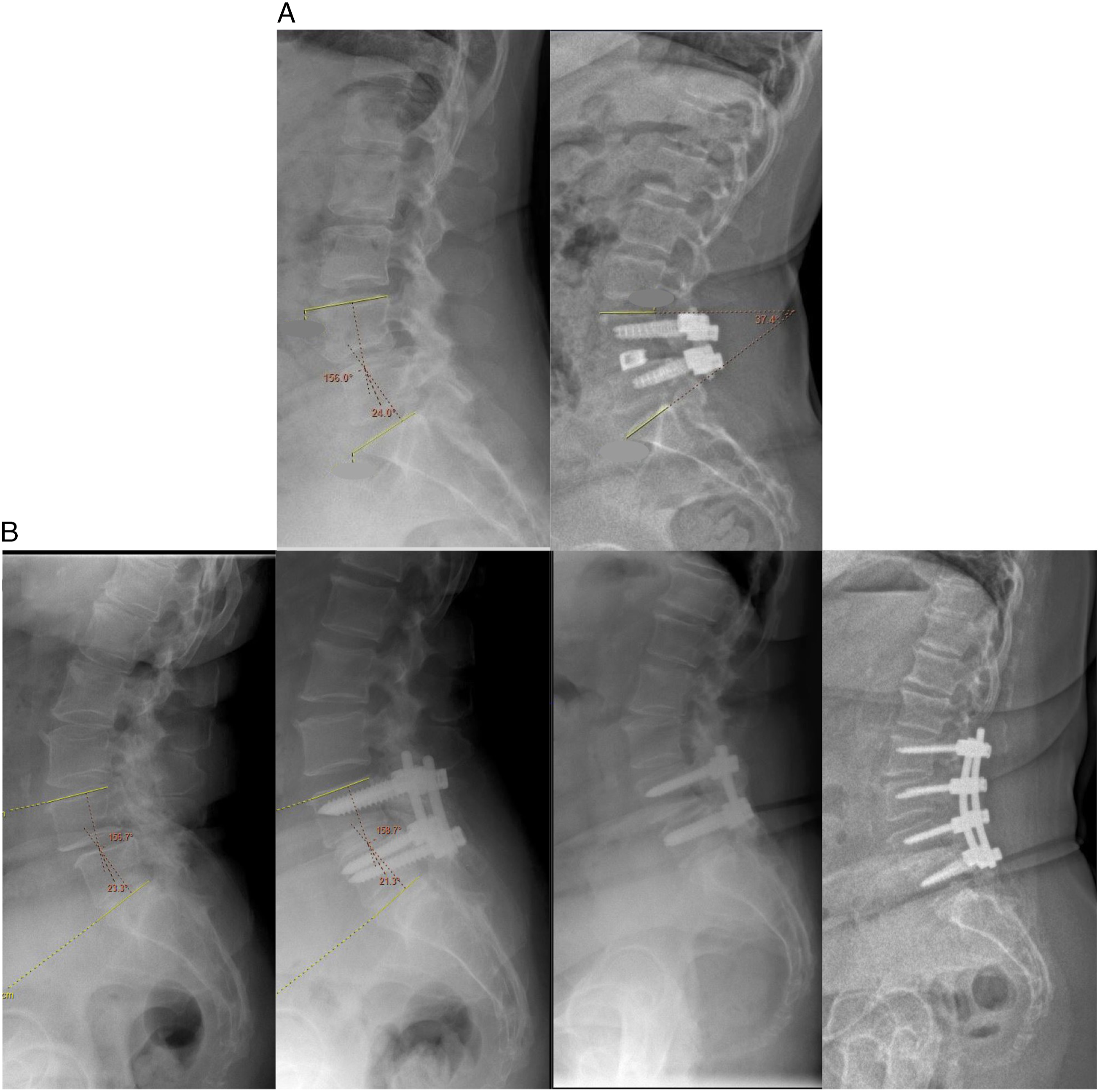
An ASD reoperation odds increase was also seen in patients with a low or average pelvic incidence when compared to those with a high PI. The highest odds of ASD reoperation were seen in patients with an average PI and post-operative distal lordosis <35 deg (OR 3.1, 95% CI 1.7-5.3, P < .001). Based on these data and the findings of Pesenti et al (2018) 15 and Umehara et al (2000), 3 we postulate that patients with a high PI may be able to compensate for loss of distal lumbar lordosis through their inherent proximal lordosis in a manner that does not significantly increase the biomechanical strain on the adjacent levels. Comparatively, patients with a low/average PI and distal lumbar hypolordosis may experience increased biomechanical strain at the adjacent level due to their lack of natural lordosis in the proximal lumbar spine. In this series, a post-operative distal lordosis of ≥35° was more likely to be achieved in patients who had a higher baseline distal lordosis (39 vs 27°, P < .001) and a higher pelvic incidence (64 vs 57°, P < .001).
Approximately 70% of the patients in this cohort had a spondylolisthesis at the operated level. In 64% of these patients, this was a degenerative spondylolisthesis, whilst the remaining 36%, had an isthmic spondylolisthesis. The presence of a spondylolisthesis was associated with an increased odds of ASD reoperation on multivariate analysis and subdivision of these patients into isthmic and degenerative subgroups demonstrated a significantly increased odds of ASD reoperation in patients with degenerative spondylolisthesis (P < .001, OR 4.6, 95% CI 1.9-11.4).
Further statistical analysis demonstrated significant differences between patients in these two subgroups. Patients with degenerative spondylolisthesis were older (mean age 63.7 vs 45.9, P < .001), had a lower pelvic incidence (mean PI 59.7 vs 64.2°, P = .005), had a lower baseline DL (26.5 vs 34.7°, P < .001), and a lower post-operative DL (27.6 vs 35.2°, P < .001). These demographic differences demonstrate the underlying heterogeneity of these two patient populations that has been established in the literature. 20 Whilst both degenerative and isthmic spondylolisthesis patients have been shown to have a higher mean PI than the average population, patients with an isthmic spondylolisthesis have a higher pelvic incidence and consequently, a greater proximal lumbar lordosis than patients with a degenerative spondylolisthesis .20-23 In this study populations, 35/39 (90%) of the degenerative and 5/6 (83%) of the isthmic spondylolisthesis patients that required reoperation for ASD had a post-operative DL <35°, suggesting that loss of distal lumbar lordosis represents a risk factor for ASD across both cohorts.
There is growing evidence in the literature to support the notion that the restoration of physiologically distributed lordosis improves patient outcome. Bari et al 24 (2021) reported that maldistribution of lordosis was associated with an increased rate of revision surgery and poor radiographic outcome in parameters such as pelvic tilt and PI-LL mismatch that have previously been linked to clinical outcomes. Similarly, Zheng et al 25 (2020) reported an increased incidence of observed ASD in patients with an abnormal lordosis distribution index (distal lordosis/total lumbar lordosis) following L4-S1 fusion. Pesenti et al 16 (2021), suggested that restoration of distal lumbar lordosis is also critical in optimising correction in patients with adult spinal deformity. The quantified, simple radiographic metric examined in the current study (distal lordosis of 35°) is advantageous in that it is simpler to assess and easier to target when performing 1 or 2 level fusions in the distal lumbar spine than the global lumbar parameters studied by previous authors.
Many studies have examined the choice of surgical technique in patients with a degenerative lumbar spondylolisthesis (DLS).26-28 Whilst it is becoming clearer that not all patients with DLS require fusion, there is ongoing uncertainty with regards to the characteristics of patients that benefit from the addition of fusion to decompression alone. 29 Recently, Mohanty et al 14 (2023) reported a benefit in patient reported outcomes to decompression and fusion over decompression alone in DLS patients with sagittal malalignment (PI-LL mismatch). In the current study, patients with a degenerative spondylolisthesis were more susceptible to ASD requiring reoperation when post-operative distal lordosis was lower than physiologically reported values. DLS patients with sagittal malalignment may hence benefit from not only the addition of fusion, but moreover from a fusion technique that allows restoration of physiological distal lordosis.
In our study, the mean post-operative DL was slightly lower than the mean pre-operative DL in the R group (28.7 vs 27.3°) and correction of distal lordosis from a pre-operative value of <35° to a post-operative value of ≥35° was only achieved in approximately 10% of patients. Further study is required to determine whether advances in surgical techniques and implant design will facilitate achievement of this distal lordosis target from a posterior approach in a broader range of patients.
This study has a number of limitations beyond its retrospective, single-center nature. Reoperation for ASD is a complex metric that is influenced by individual patient and surgeon attitudes in addition to the risk factors described above. It is difficult to measure the contribution of these psychosocial factors on the decision for reoperation. The mean time to revision in the R group was longer than the mean follow-up in the NR group (78 vs 55 months). This is in part due to our definition of time to revision as the time between the index surgery to the adjacent level surgery (rather than the time from index surgery to the date that a decision was to proceed with adjacent level surgery). Due to a transition of electronic medical record systems, the date of decision to proceed with ASD reoperation was not available for many patients, allowing the wait time from ASD reoperation decision to ASD reoperation surgery (often 12 months) to prolong the “mean time to revision”.
There are known associations between some of the radiographic variables collected that may confound the statistical analysis. Adjustment for this potential collinearity requires larger, multicenter data sets. In our study, there was only limited assessment of pre-existing adjacent level degenerative changes as not all patients had pre-operative CT and/or MRI images available for review. However, it is the practice of both senior authors to include existing degenerative segments in their fusions. Use of a cross sectional imaging with an established grading system for segmental degenerative changes may facilitate control for existing adjacent segment degenerative changes in future studies. The measurement of radiographic parameters has an inherent interobserver variability and parameters may differ at various post-operative time points, eg, early post-operative distal lordosis may not be indicative of final post-operative distal lordosis due to interbody device settling or subsidence. Further, the outcome of this study was revision for ASD. There were likely patients with symptomatic ASD that chose not to have revision surgery during the period studied. Finally, it was assumed on the basis of prior literature that reoperation is associated with increased patient morbidity, however, patient reported outcome measures were not assessed in this study. 30
Conclusion
This study supports the association between post-operative distal lumbar lordosis and the risk of reoperation for adjacent segment degeneration. This risk was amplified in patients with a low/average pelvic incidence undergoing fusion for degenerative spondylolisthesis. Further multicenter prospective study is needed to independently confirm this association and identify the impact of restoration of physiological distal lumbar lordosis on long term patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.