
Abstract
Study Design
Cross-sectional radioanatomic study.
Objective
To determine the feasibility of performing an anterior column realignment (ACR) using an anterior-to-psoas (ATP) approach at L1-L5.
Methods
Axial magnetic resonance images (MRI) of the L1-L5 disc levels obtained at a single institution were obtained and analyzed. The feasibility of performing an ACR was assessed using a combination of the size of the left oblique corridor (OC), the psoas morphology using the modified Moro classification, and the anterior disc edge to great vessel distance.
Results
Three hundred MRI studies obtained from 300 patients were included. All patients had a measurable left OC at the L1-L4 levels. Twenty patients (6.7%) had no measurable OC at the L4-L5 level. According to the modified Moro’s classification, a high-rising psoas was seen in 4 patients (1.3%) at the L3-L4 level and 57 patients (19.0%) at the L4-L5 level. An ALL release was considered high risk due to no measurable space between the anterior disc edge and the great vessels in 54 patients (18.0%) at the L1-L2 level, 39 patients (13.0%) at the L2-L3 level, 119 patients (39.7%) at the L3-L4 level, and 226 patients (75.3%) at the L4-L5 level.
Conclusion
ACR using an ATP approach is the most radioanatomically feasible at L2-L3. The L4-L5 level has the highest risk with regards to both the ATP approach and the ALL release for an ACR due to high rates of unmeasurable left OC and space between the anterior disc edge and the great vessels.
Introduction
Restoration of sagittal balance is an important prognostic indicator among patients undergoing surgical intervention for adult spinal deformity. 1 Depending on the severity of focal kyphotic deformity, methodologies such as three-column osteotomy and vertebrectomy have traditionally been utilized to obtain adequate deformity correction. However, these procedures have been associated with high rates of blood loss and perioperative complications.2,3 Anterior column realignment (ACR) with release of the anterior longitudinal ligament (ALL) is a more recently adopted method that was introduced as a powerful alternative for achieving adequate restoration of sagittal alignment. 4 The current literature mainly describes this procedure using a lateral transpsoas approach, which has its limitations including the need for dissection through the psoas muscle, risk of injury to the lumbar plexus, and inadequate visualization of the great vessels during ALL release.
The anterior-to-psoas (ATP) approach to the lumbar spine has been well-described as an alternative to approaching the disc space without dissecting through the psoas muscle thus decreasing the risk of injury to the lumbar plexus.5,6 Limitations of this approach have also been well-documented including higher risks of injury to the sympathetic nerves as well as to the great vessels compared to the transpsoas approach. 6 However, when performing an ACR, the ATP approach confers the benefit of direct visualization and protection of the great vessels during the ALL release. 7
A recent anatomical study proposed that an ATP approach is high risk at the L4-L5 level when there is no measurable oblique corridor (OC) or with a high riding psoas defined as grades AII, AIII, and AIV in the modified Moro’s classification. 8 Another study proposed the importance of a measurable plane between the disc space and the great vessels in avoiding vascular injury during ATP interbody fusion. 9 To our knowledge, there are no prior studies that comprehensively investigate the radioanatomical feasibility of performing an ACR using an ATP approach at the L1-L5 levels. Thus, the objective of this study was to determine the radioanatomic feasibility of performing an ACR using an ATP approach at L1-L5 by analyzing the size of the left OC, the psoas muscle morphology, and the location of the great vessels at the L1-L2, L2-L3, L3-L4, and L4-L5 disc levels.
Methods
Patient Selection
This cross-sectional radioanatomic study protocol was approved through the local institutional review board with a waiver for informed consent due to the retrospective nature of this study (Approval No. PRO00032736). Axial magnetic resonance images (MRI) of the L1-L2, L2-L3, L3-L4, and L4-L5 disc levels obtained randomly at a single institution from consecutive adult patients presenting with low back pain and/or lumbar radiculopathy were obtained and analyzed. The MRI sequences were obtained with the patient in the supine position using the Signa HDxt 1.5 T MR system (GE Medical Systems, Chicago, IL).
Exclusion criteria included incomplete imaging, MRI obtained at other institutions, any burst or compression fracture involving L1 to L5, infection or tumor of the lumbar spine, or any prior surgery to the lumbar spine, great vessel(s), or retroperitoneum.
Data Collection
Demographic data at time of surgery including age, gender, and BMI were retrospectively collected through electronic medical records. The feasibility of performing an ACR was assessed using a combination of the size of the left OC, the psoas morphology using the modified Moro classification, and the anterior disc edge to great vessel distance (Figure 1). All images were obtained at a single institution with an identical scanning protocol to ensure identical scanning thickness among all analyzed images. All measurements were obtained using GE Healthcare Centricity RIS/PACS 3.0 software (Chicago, IL, USA) by 3 reviewers to improve interobserver reliability. All reviewers obtained each measurement 3 times to improve intraobserver reliability. Interobserver and intraobserver reliabilities were assessed using intraclass correlation coefficient (ICC), where an ICC below .5 implies poor agreement, between .5 and .75 implies moderate agreement, between .75 and .90 implies good agreement, and above .90 implies excellent agreement.
10
The mean value obtained by the 3 reviewers were then reported as the final measure. All reviewers were blinded to their respective measurements as well as to patient demographics and outcomes to reduce risk of bias. Non-annotated (A) and annotated (B) example axial MRI at the L2-L3 level of a standard included patient depicting measurements of nearest anterior disc edge and the IVC (.27 cm), nearest anterior disc edge and the aorta (.18 cm), and the left OC (1.93 cm).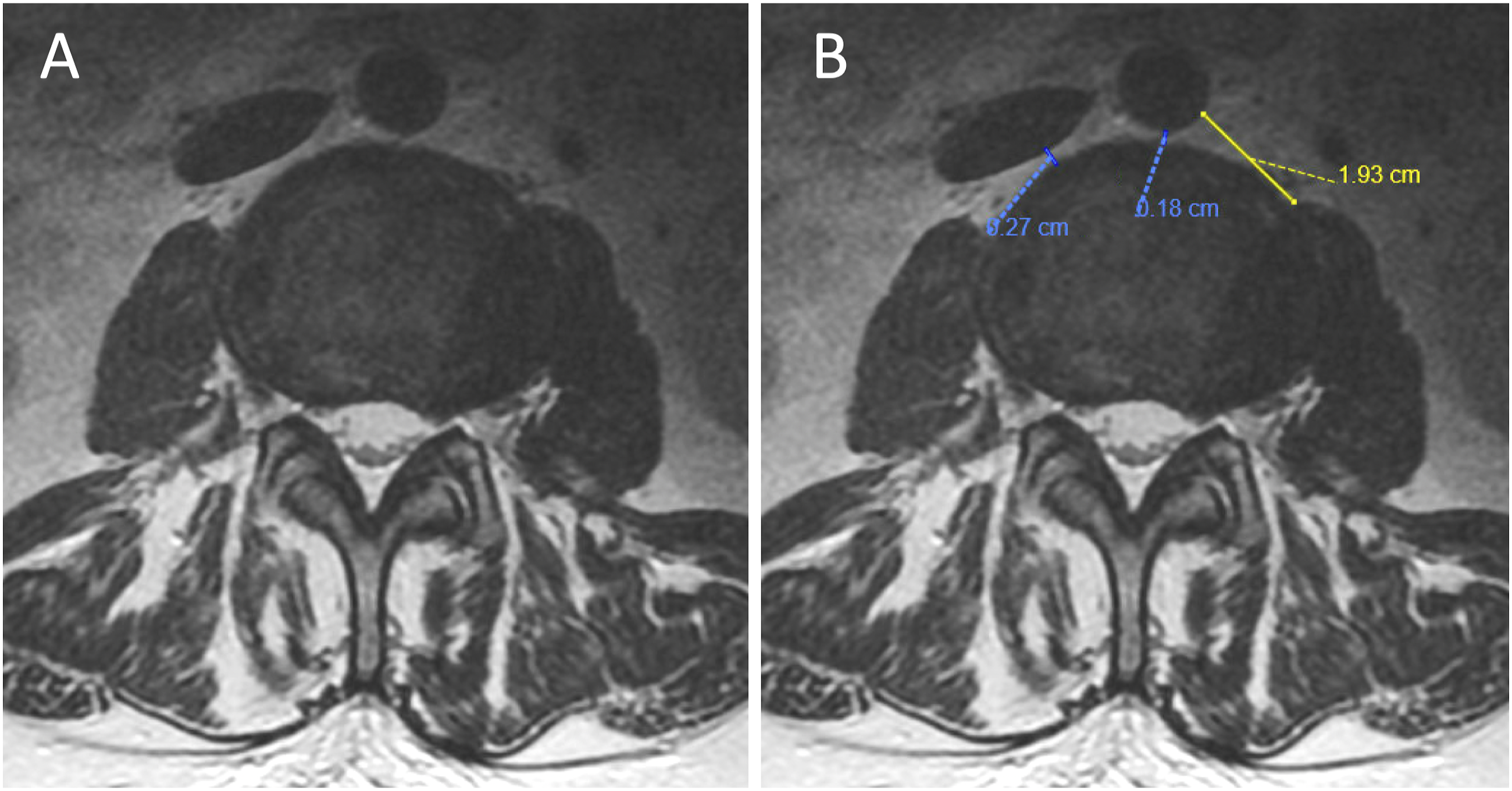
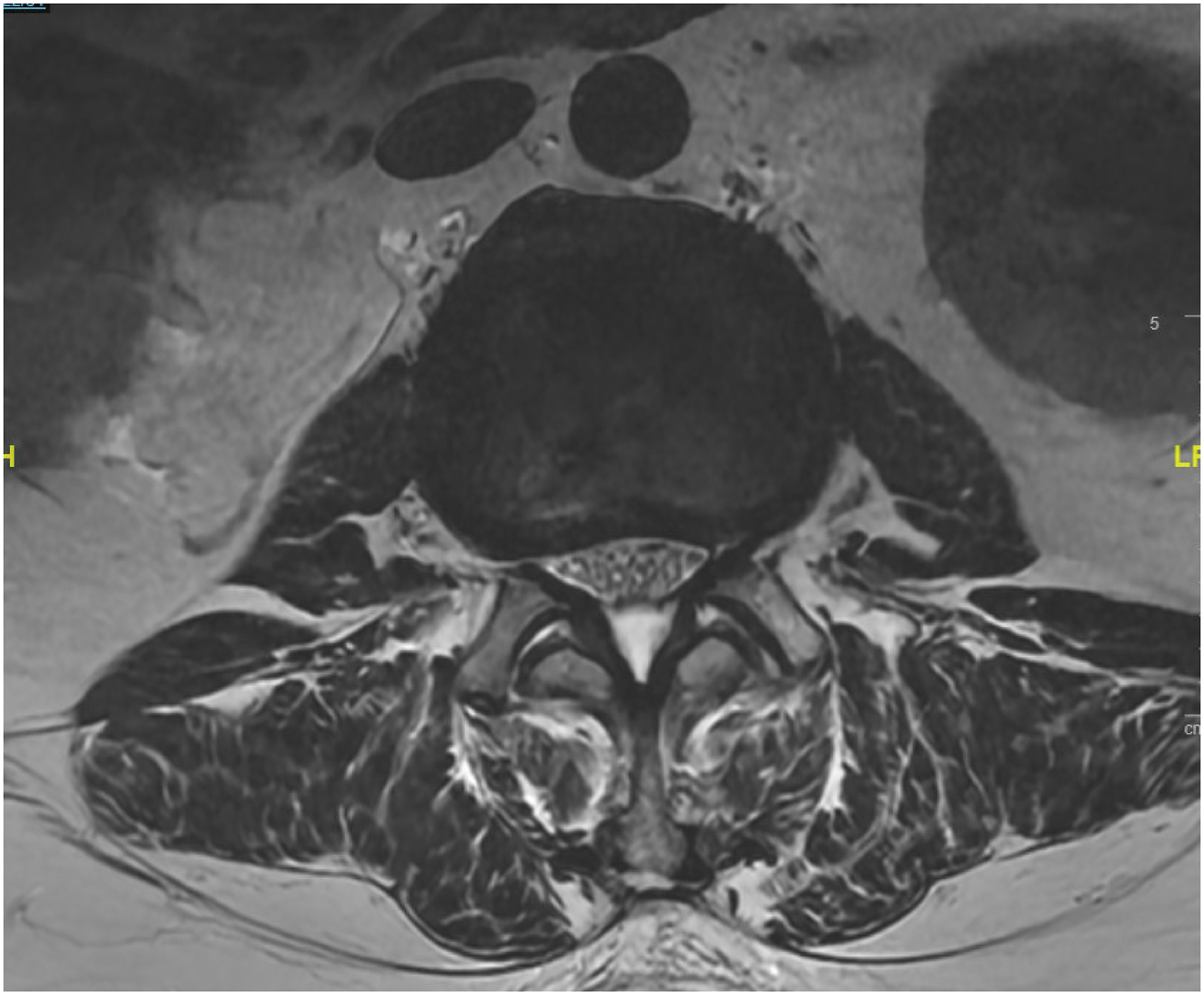
An ATP approach was considered high risk when there was no measurable OC or with the presence of a high-rising psoas (modified Moro grades AII, AIII, or AIV). (Figure 2). An anterior longitudinal ligament (ALL) release for ACR was considered high risk when there was no measurable space between the anterior disc edge and the great vessels (Figure 2). An axial MRI at the L4-L5 level of 2 separate patients where (A) represents a patient where an ATP approach was considered high risk due to both no measurable left OC and the presence of a high-rising psoas (modified Moro grade AIII) and where (B) represents a patient where an ALL release for ACR was considered high risk for vascular injury due to no measurable space or fat streak between the anterior disc edge and the nearest CIV and CIA.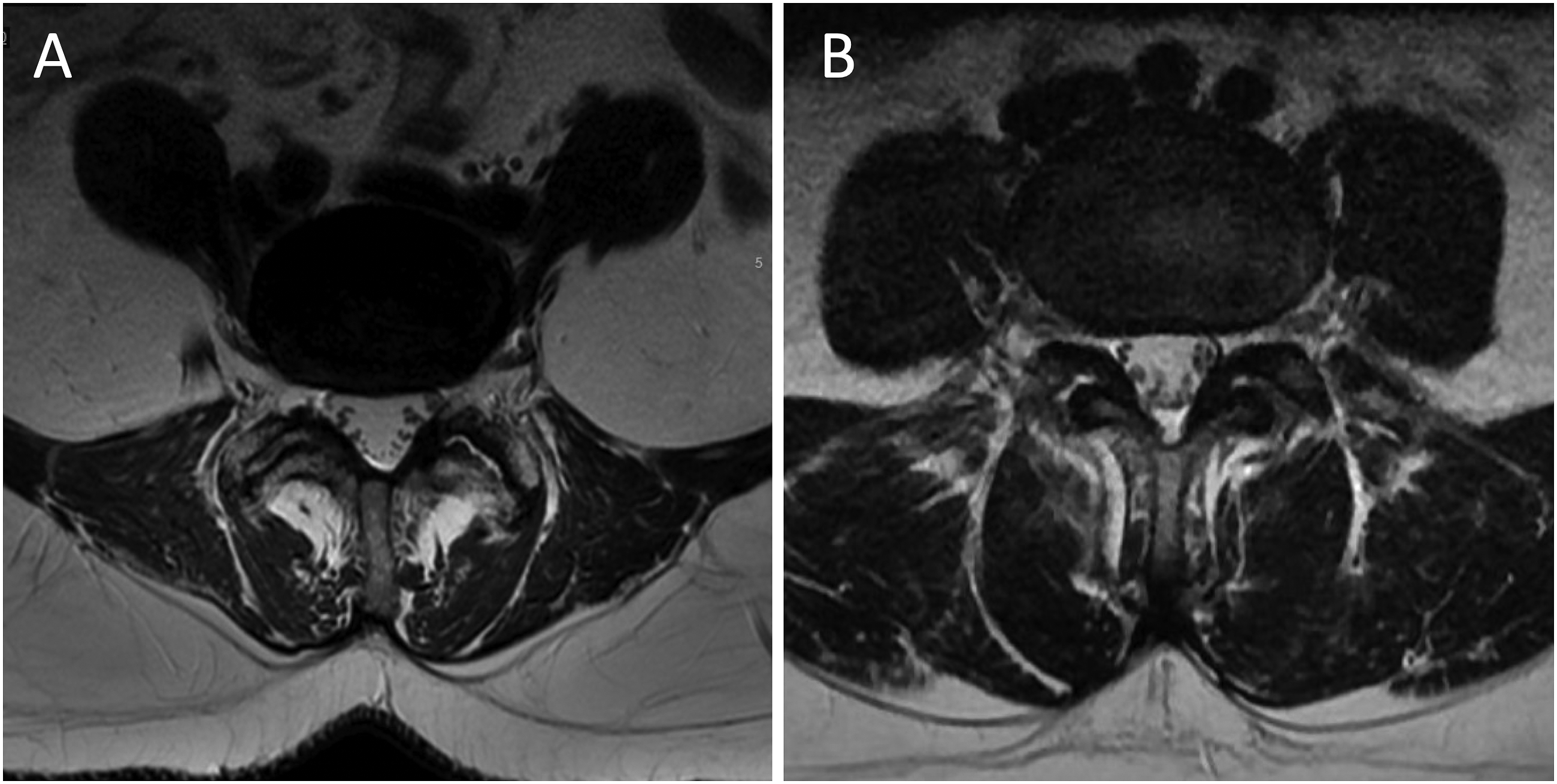
Statistical Analysis
Data analysis was performed using SPSS statistical software (Version 25.0; SPSS, Inc, Chicago, IL). Two-tailed student t-test was used to analyze continuous data and the Chi-Square or Fisher’s exact test was used to analyze categorical data. The Mann-Whitney U test was utilized for continuous variables with non-normal distribution. A P value <.05 was considered statistically significant.
Results
Demographics and Risk Characterization.
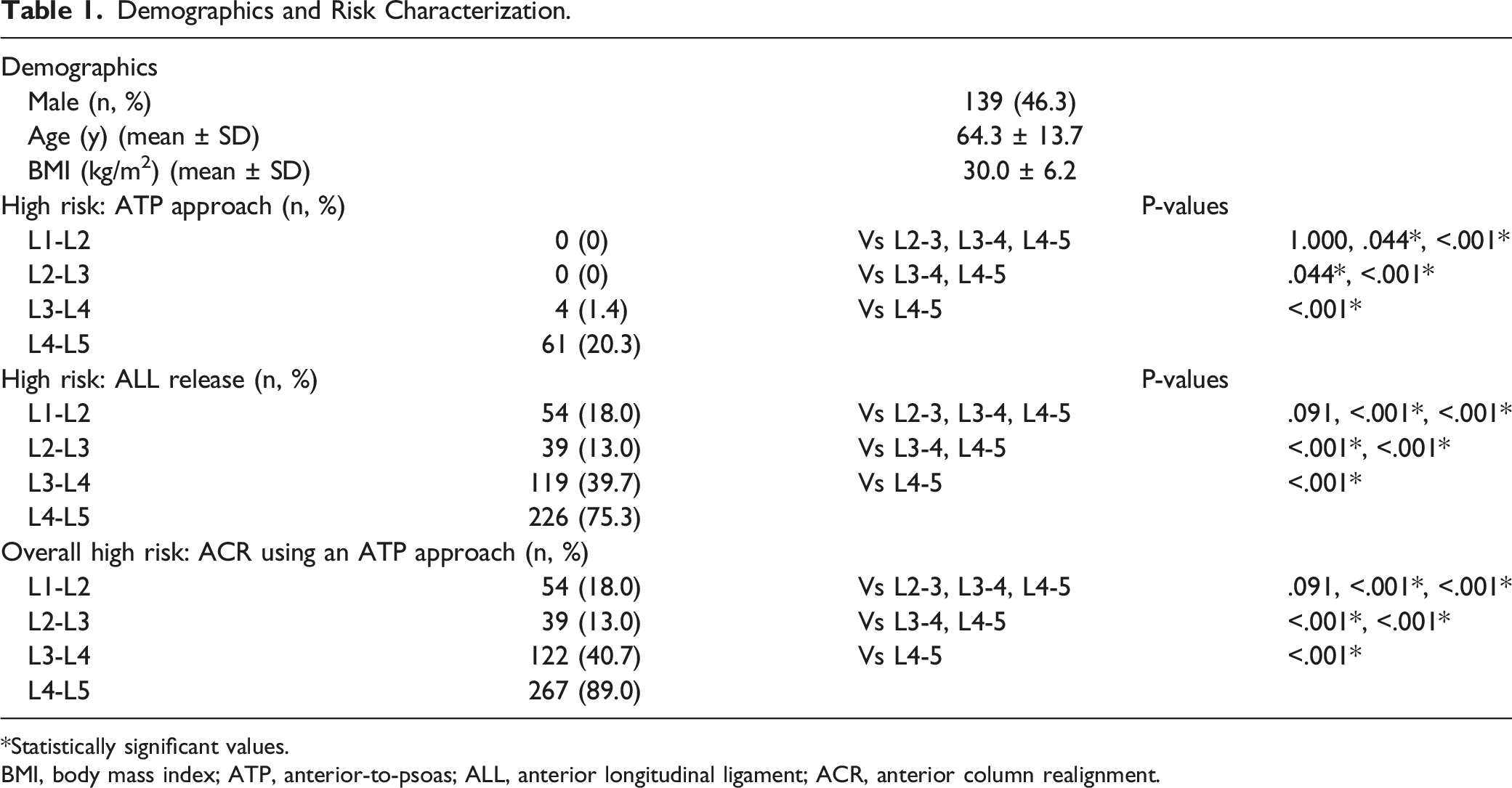
*Statistically significant values.
BMI, body mass index; ATP, anterior-to-psoas; ALL, anterior longitudinal ligament; ACR, anterior column realignment.
ATP Approach Feasibility
The mean left OC was 2.13 ± .69 cm, 1.92 ± .63 cm, 1.75 ± .61 cm, and 1.39 ± .79 cm at the L1-L2, L2-L3, L3-L4, and L4-L5 levels, respectively (Figure 3). All patients had a measurable left OC at the L1-L4 levels. Twenty patients (6.7%) had no measurable OC at the L4-L5 level. According to the modified Moro’s classification, high-rising psoas was seen in 4 patients (1.3%) at the L3-L4 level and 57 patients (19.0%) at the L4-L5 level. Since an ATP approach was considered high risk when there was either no measurable OC or with the presence of a high-rising psoas, we found that an ATP approach was feasible but with high risk in 4 patients (1.3%) at the L3-L4 level and 61 patients (20.3%) at the L4-L5 level. An ATP approach was considered feasible and low risk among all patients at the L1-L3 levels. However, partial obstruction to access the left OC from the renal vessels and/or kidney was seen in 218 patients (72.7%) at the L1-L2 level, 24 patients (8.0%) at the L2-L3 level, and 2 patients (.7%) at the L3-L4 level (Figure 4). Interobserver and intraobserver reliabilities of the OC measurements were excellent with ICC of .912 (95% CI 0.878-.948) and .965 (95% CI 0.931-.978), respectively. Mean left OC size at L1-L5. *P < .05. An axial MRI at the L2-L3 level demonstrating a left kidney partially obstructing the left OC.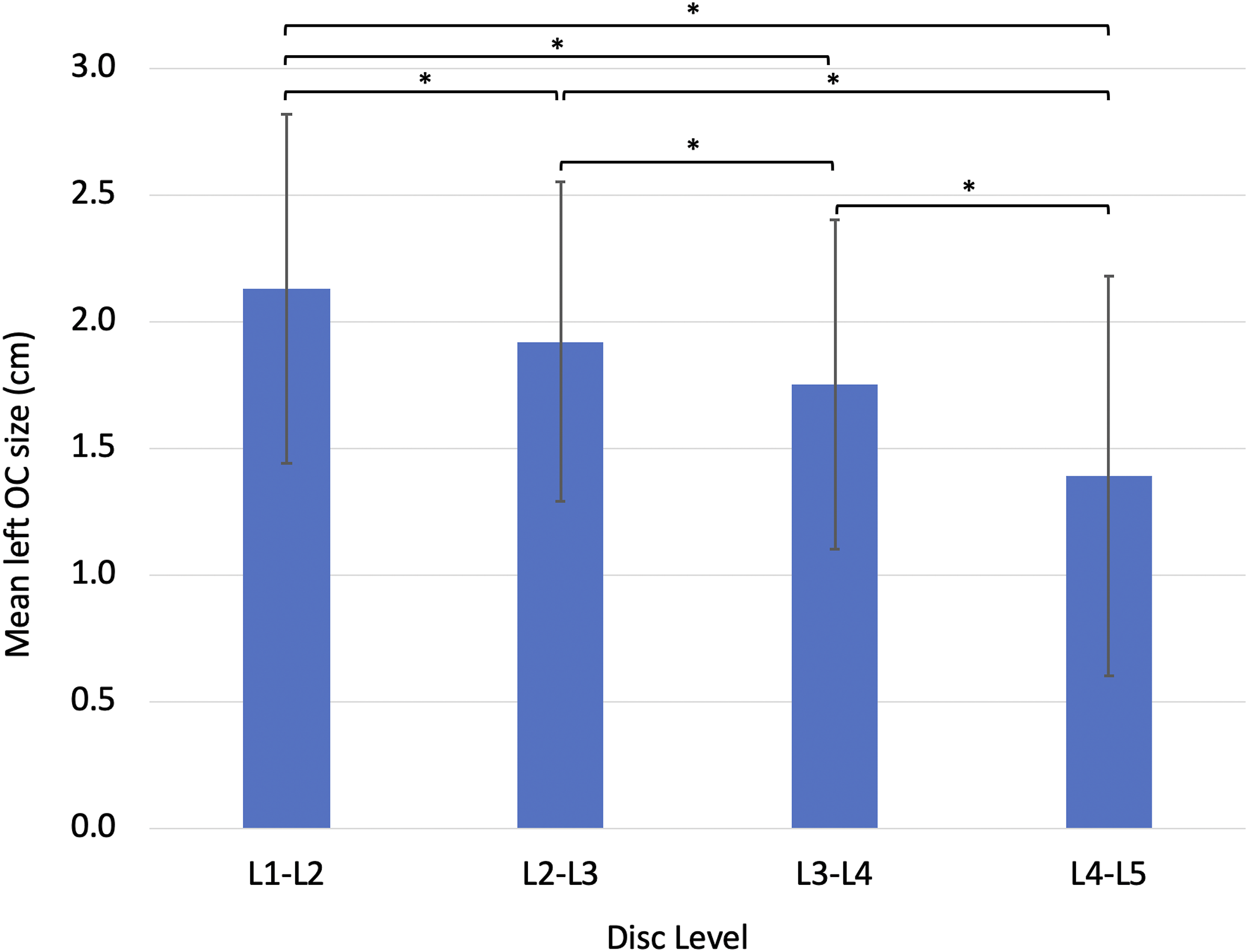
ALL Release Feasibility
The mean distance between the anterior disc edge to the closest arterial great vessel (aorta or the closest common iliac artery (CIA)) was .26 ± .22 cm, .29 ± .22 cm, .30 ± .26 cm, and .22 ± .29 cm at the L1-L2, L2-L3, L3-L4, and L4-L5 levels, respectively (Figure 5). There was no measurable space between the anterior disc edge and the aorta in 54 patients (18.0%) at L1-L2, 32 patients (10.7%) at L2-L3, and 43 patients (14.3%) at L3-L4. There was no measurable space between the anterior disc edge and the aorta or the common iliac artery (CIA) in 99 patients (33.0%) at L4-L5. Mean anterior disc edge to closest arterial great vessel (aorta or CIA) distance at L1-L5. *P < .05.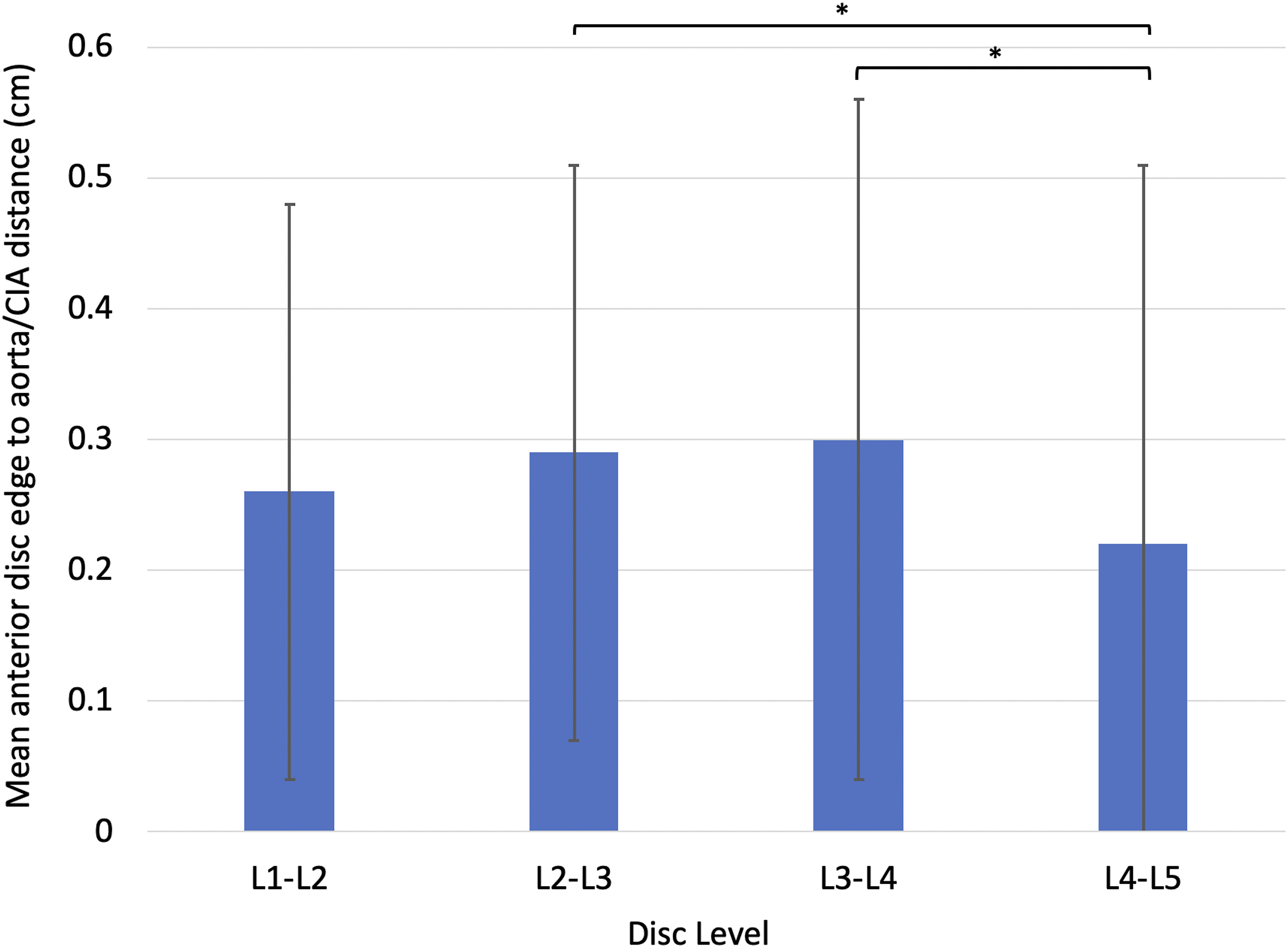
The mean distance between the anterior disc edge to the closest venous great vessel (inferior vena cava (IVC) or a common iliac vein (CIV)) was 1.36 ± .60 cm, .62 ± .53 cm, .19 ± .24 cm, and .04 ± .09 cm at the L1-L2, L2-L3, L3-L4, and L4-L5 levels, respectively (Figure 6). All patients had a measurable space between the anterior disc edge and the IVC at L1-L2. There was no measurable space between the anterior disc edge and the IVC in 10 patients (3.3%) at the L2-L3 and 104 patients (34.7%) at L3-L4. There was no measurable space between the anterior disc edge and the IVC or CIV in 216 patients (72.0%) at L4-L5. Mean anterior disc edge to closest venous great vessel (IVC or CIV) distance at L1-L5. *P < .05.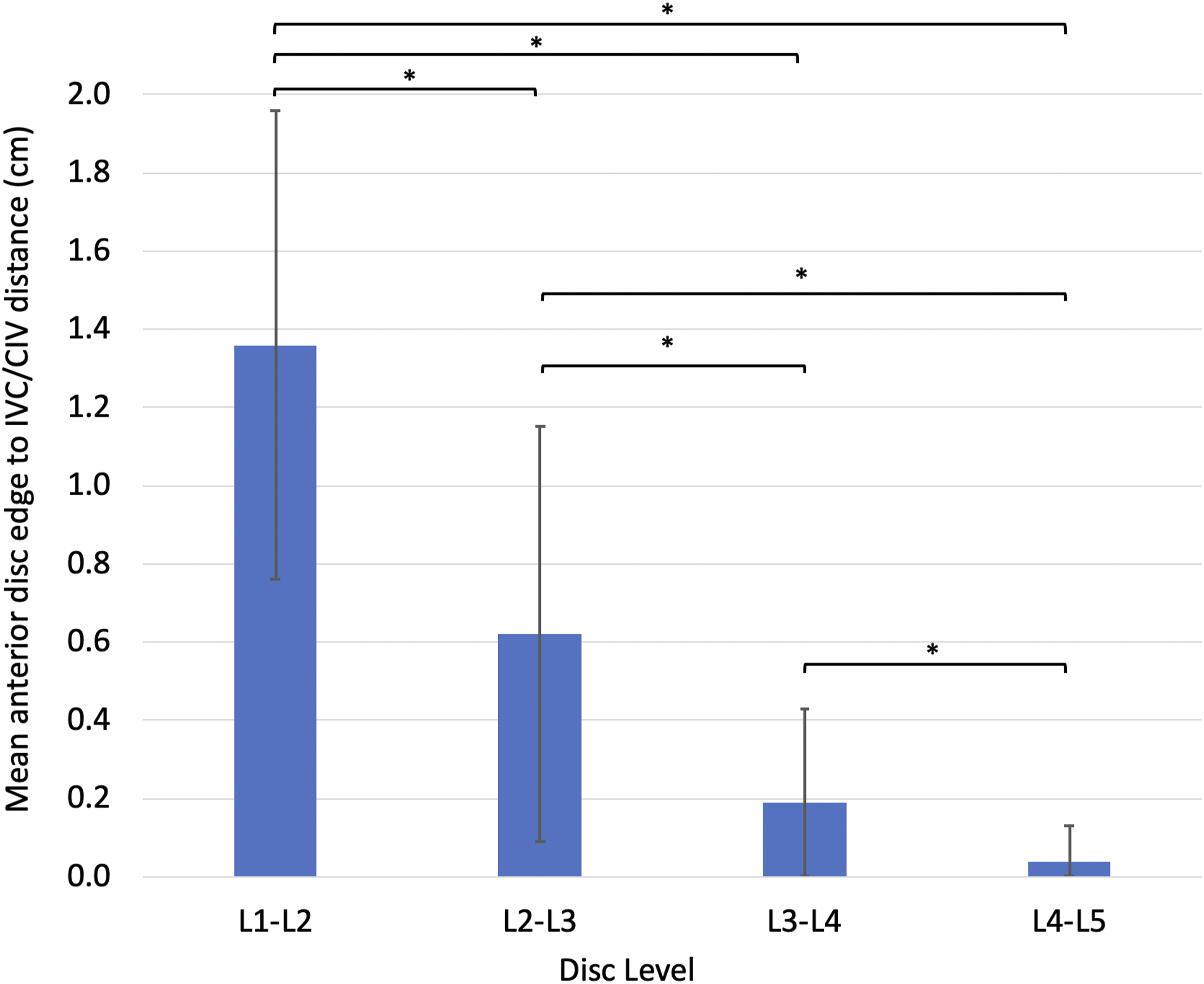
Overall, an ALL release was considered high risk due to no measurable space between the anterior disc edge and 1 or more great vessel in 54 patients (18.0%) at the L1-L2 level, 39 patients (13.0%) at the L2-L3 level, 119 patients (39.7%) at the L3-L4 level, and 226 patients (75.3%) at the L4-L5 level. A retroaortic left renal vein was seen at the L1-L2 level in 1 patient (.3%) and at the L2-L3 level in 4 patients (1.3%). There was no measurable distance between the anterior disc edge and the retroaortic left renal vein in all 5 instances (Figure 7). An axial MRI at the L2-L3 level demonstrating a retroaortic left renal vein with no measurable distance between the anterior disc edge.
Interobserver and intraobserver reliabilities for the anterior disc edge to great vessel measurements were excellent with ICC of .902 (95% CI 0.869-.932) and .947 (95% CI 0.922-.969), respectively.
ACR using an ATP Approach Feasibility
Overall, an ACR using an ATP approach was considered high risk due to either being high risk for the ATP approach and/or for the ALL release in 54 patients (18.0%) at the L1-L2 level, 39 patients (13.0%) at the L2-L3 level, 122 patients (40.7%) at the L3-L4 level, and 267 patients (89.0%) at the L4-L5 level (Table 1).
Discussion
The increasing use of the ATP approach for performing an ACR as an alternative to the lateral transpsoas approach necessitates a detailed understanding of the radioanatomic relationship of the disc spaces and the surrounding anatomy. In this study, we investigated the radioanatomic feasibility of performing an ACR using an ATP approach at L1-L5 by analyzing the size of the left OC, the psoas muscle morphology, and the location of the great vessels at the L1-L5 disc levels. We found that the L4-L5 level has the highest risk with regards to both the ATP approach and the ALL release for an ACR due to high rates of unmeasurable left OC, high-rising psoas, and unmeasurable space between the anterior disc edge and the great vessels. Although L1-L4 levels were found to be more feasible for the ATP approach and the ALL release in general, each disc level was associated with unique anatomical considerations.
The left OC was the largest at the L1-L2 level with a mean distance of 2.13 ± .69 cm, which decreased progressively to a mean distance of 1.36 ± .77 cm at the L4-L5 level. Zhang et al and Li et al also demonstrated a diminishing OC distance moving caudal from L1 to L5.11,12 Zhang et al. evaluated 40 healthy subjects of Asian descent and reported a significantly smaller mean left OC distance of 1.55 cm at L1-L2 diminishing to .86 cm at L4-L5 (P < .01). 12 Li et al. hypothesized that the decreased OC distance from L1 to L5 occurred as a result of the conical shape of the psoas muscle. 12 However, the current study confirmed that the common iliac vessels and high-rising psoas also contributed to the decreasing OC distance from L1 to L5.
Although the left OC was the largest at the L1-L2 level, partial or complete obstruction of the left OC from the renal vessels or kidney was seen in 72.7% of the patients at this level. This rate decreased to 8.0% at the L2-L3 level, and .7% at the L3-L4 level. Li et al. similarly reported a 74.5% rate of partial or complete obstruction of the left OC from the renal vessels or kidney at the L1-L2 level and 5.0% at the L2-L3 level. 12 Although the renal vessels and kidney can be safely mobilized intraoperatively, surgeons must be aware of their presence as injury to these structures have been well-described particularly when using smaller exposures with minimally invasive techniques.13–15 Our study also found a .3% and 1.3% prevalence of a retroaortic left renal vein at the L1-L2 and L2-L3 levels. Hostiuc et al similarly reported a 3% overall prevalence rate of a retroaortic left renal vein within a healthy adult population in their meta-analysis. 16 Although there are no prior reported cases of injury to this vein during spine surgery, understanding of its existence is important when performing an ACR as there was no measurable distance between the anterior disc edge and this vein in all 5 instances within our study.
Furthermore, according to the modified Moro’s classification, 1.3% and 19.0% of the patients had no measurable OC at the L3-L4 and L4-L5, respectively, due to a high-rising psoas (modified Moro AII, AIII, or AIV). These findings were similar to a previous study by Ng et al., which reported a 19.2% rate of high-rising psoas at the L4-L5 level using this criteria. 8 Our study found that although less commonly seen, this criteria may also be applicable at the L3-L4 level for a pre-operative feasibility analysis. Although previous studies considered a non-measurable OC as “inaccessible” for an ATP approach, careful retraction of the psoas muscle posteriorly and great vessels anteriorly may allow safe access to the disc.8,12,17,18 We thus classified a non-measurable OC and a high-rising psoas (modified Moro AII, AIII, or AIV) as high risk of injury to the adjacent structures during the ATP approach as opposed to being “inaccessible” or “infeasible.” Overall, our study found that an ATP approach was considered feasible among all patients at the L1-L3 levels and high risk in 1.3% of patients at the L3-L4 level and 20.3% at the L4-L5 level due to either no measurable OC or the presence of a high-rising psoas.
Our study found that the L4-L5 level had the lowest mean distance between the anterior disc edge to the closest arterial great vessel (.22 ± .29 cm) and the highest incidence of having no measurable space between the anterior disc edge and the closest arterial great vessel (33.0%). These results were similar to a prior study by Marchi et al. which also demonstrated a 33.0% rate of no measurable space between the anterior disc edge and the closest arterial great vessel at the L4-L5 level. 19 We also found that the L4-L5 level had the lowest mean distance between the anterior disc edge to the closest venous great vessel (.04 ± .09 cm) and the highest incidence of having no measurable space between the anterior disc edge and the closest venous great vessel (72.0%). Awareness of the anatomical relationship of the great vessels to the disc is particularly important to ensure proper planning for careful dissection and gentle retraction of these vessels during the ACR to decrease the likelihood of injury to these vessels.
Overall, when combining the high-risk patients for both the ATP approach and the ALL release, our study found that an ACR using an ATP approach was considered high risk in 18.0% of the patients at the L1-L2 level, 13.0% at L2-L3, 40.7% at L3-L4, and 89.0% at L4-L5. Thus, we found that an ACR using an ATP approach is the most radioanatomically feasible at the L1-L3 levels and least feasible at the L4-L5 level. These findings are similar to prior radioanatomic studies using the direct lateral approach; however, with different considerations regarding the neurovascular anatomy. In terms of the approach itself, the direct lateral approach utilizes a transpsoas corridor, which diminishes the theoretical risk of vascular injury from the exposure of the OC with an ATP approach, but inherently increases the risk of direct injury to the lumbar plexus and the psoas muscle.20,21 A study by Kepler et al. has shown that the distance between the anterior vertebral plane and the lumbar plexus diminishes from a mean of 30.8 mm at L1-L2 to 28.6 mm at L2-L3, 28.2 mm at L3-L4, and 22.1 mm at L4-L5. Furthermore, the presence of a high-rising psoas has an even higher risk of lumbar plexus injury when utilizing a direct lateral approach due to the anterior migration of the lumbar plexus. 21 In terms of the ALL release, a similar consideration regarding the adjacent vascular structures must be considered with the direct lateral approach. Mai et al. reported the presence of a clear fat plane between the anterior vertebral body and adjacent vascular structures to diminish from 80.0% and 85.5% at L1-L2 and L2-L3 to 67.2% at L3-L4 and 47.5% at L4-L5. 22 Furthermore, this fat plane is particularly important for performing an ALL release using the direct lateral approach as the great vessels are more difficult to be directly visualized and retracted when using this approach in contrast to the ATP approach. 7 Finally, from a technical standpoint, an ATP approach has its inherent disadvantage of working in an unnatural oblique orientation compared to a direct lateral approach; however, multiple studies have demonstrated equivalent fusion rates, sagittal imbalance, and implant complications between the 2 approaches.23,24 As 89.0% of the patients within our cohort was considered high risk for undergoing an ACR using an ATP approach at the L4-L5 level, an anterior lumbar interbody fusion (ALIF) may be a feasible option, particularly for these patients. Since an ALIF requires incising the ALL, this technique has been shown to achieve similar sagittal correction and lordosis compared to an ACR through a lateral technique.2,7,25 However, an ALIF is considered a more invasive procedure with a higher approach-related morbidity with longer post-operative length of stay and time to ileus recovery. 25 Furthermore, at the L4-L5 level or cephalad, the recurrent iliolumbar vein must often be safely identified, divided, and mobilized in preparation for performing a much greater retraction of the vessels when compared to an ATP approach. 25 Thus, although certain high-risk patients may benefit from an ALIF at L4-L5, careful patient selection and availability of a general or vascular surgeon is often essential.
There are several limitations in our study. First, although this procedure is typically performed in a right lateral decubitus position, all patients completed their MRI in a standard supine position, which may not accurately reflect the anatomic relationships during surgery. A study by Zhang et al., found that the left OC substantially reduced in size from a supine to a right lateral decubitus position. 11 Another study by Deukmedjian et al. found that at the L1-L2 level, the aorta moved up to 2 mm anteriorly and 6 mm to the right when transitioning from a supine to a right lateral decubitus position. 26 They also demonstrated that this movement was more significant caudally within the lumbar spine. 26 However, as suggested by Li et al., regardless of the movement in anatomic structures in relation to the patient position, awareness of the anatomy in its natural supine position is important in understanding the mobility of these structures for safe mobilization and retraction during the procedure. 12 Despite these limitations, to our knowledge, this is the largest study that evaluates the feasibility of performing an ACR using an ATP approach from L1-L5 by analyzing the size of the left OC, the psoas muscle morphology, and the location of the great vessels at the L1-L5 disc levels. Further studies demonstrating the external validity of this data may be necessary prior to its application in practice.
Conclusion
Within the lumbar spine, an ACR using an ATP approach is the most radioanatomically feasible at the L2-L3 disc level. The L4-L5 level has the highest likelihood of identifying anatomic barriers to this approach as the highest rates of unmeasurable left OC, high-rising psoas, and unmeasurable space between the anterior disc edge and the great vessels were found. The L4-L5 level has the highest risk with regards to both the ATP approach and the ALL release for an ACR due to high rates of unmeasurable left OC and space between the anterior disc edge and the great vessels. The L1-L2 level had the highest rate of left OC obstruction due to the renal vessels and/or the kidney. Due to significant anatomic variability at each level, a thorough preoperative radioanatomic assessment is recommended prior to performing this procedure.
Footnotes
Authors’ Note
The study protocol was approved through the local institutional review board with a waiver for informed consent due to the retrospective nature of this study (Approval No. PRO00032736).
Declaration of Conflicting Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Rex Marco has the following disclosures: DePuy, A Johnson & Johnson Company: Paid presenter or speaker Globus Medical: IP royalties.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by a Burroughs Welcome Fund Physician Scientist Award to the Texas A & M University Academy of Physician Scientists.