
Abstract
Study Design
Retrospective Cohort Study.
Objective
Venous thromboembolic events (VTE) and post-operative epidural hematoma (EDH) are significant complications after spine surgery. Guidelines for chemoprophylaxis are controversial and variability amongst surgeons remains. The objective of this study was to establish the incidence of clinical VTE and EDH at our institution and evaluate the association of chemoprophylaxis with clinical VTE and EDH.
Methods
We conducted a retrospective cohort study of patients undergoing spine surgery at a high-volume tertiary care center in Seattle, WA between January 2016 and December 2019. The Premier Health Care Database and Agency for Healthcare Research and Quality (AHRQ) patient indicators PSI-9 (Perioperative hemorrhage and hematoma) and PSI-12(Perioperative PE or DVT) were used to identify patients experiencing VTE and/or post-operative EDH. The primary outcome was the incidence of clinical VTE and EDH in post-operative spine patients. Secondary outcomes included the association of chemoprophylaxis with clinical VTE and EDH.
Results
From 2016 to 2019, 4587 patients underwent spine surgery, totaling 4764 hospital stays. The incidence of clinical VTE was .21% (10/4764) and the incidence of EDH was .10% (5/4764). Most hemorrhages occurred prior to the initiation of chemoprophylaxis. One patient with EDH received chemoprophylaxis prior to hemorrhage.
Conclusions
The rate of post-operative clinical VTE and EDH in spine surgery is low. Despite early initiation of chemoprophylaxis after major spine surgery we did not appreciate a high rate of EDH. We attribute our low rate of clinical VTE to multimodal prophylaxis with SCDs, early mobilization and chemoprophylaxis on post-operative day 1.
Introduction
Venous thromboembolic events (VTE) and post-operative epidural hematoma (EDH) are feared complications of spine surgery and represent major contributors of perioperative morbidity and mortality. The management of thrombotic and hemorrhagic risk is complex due to a heterogeneous patient population, diverse spinal pathologies, and different surgical techniques. Further complicating these considerations is the lack of consistent data defining risk factors for VTE, uncertainties in VTE detection and the safety of chemoprophylaxis, which leads to highly variable institutional practices.1,2 The reported incidence of VTE surrounding spine surgery ranges between .3% and 31%.3-10 The incidence of actual postoperative spinal hemorrhage appears to be relatively low and depends on the type of procedure with acute spinal EDH reported between 0% and .7%.11,12 In clinical practice, surgeons are forced to weigh the benefit of chemoprophylaxis for VTE prevention against the risk of symptomatic postoperative bleeding.
Standard approaches for VTE prophylaxis in the perioperative setting for surgical patients include an emphasis on early mobilization, mechanical modalities and chemoprophylaxis. While guidelines for chemoprophylaxis are well established after trauma surgery and joint arthroplasty, similar guidelines for spinal procedures remain controversial.13,14 In 2009, the North American Spine Society introduced specialty specific clinical guidelines on antithrombotic therapy, 15 and although comprehensive, these guidelines highlighted the lack of high quality studies, resulting in a lack of consensus regarding perioperative chemoprophylaxis.16-18 There remains a paucity of well-controlled single- or multi-center trials defining comprehensive inclusion and exclusion criteria for both VTE and post-operative EDH. In 2020, the AO Spine Anticoagulation Global Survey emphasized that more robust data is needed to establish recommendations for anticoagulation management. 1
Due to the lack of consensus in perioperative anticoagulation management in spine surgery, we sought to identify the actual incidence of perioperative clinical VTE and post-operative EDH using a large volume single tertiary institution with high specificity prospective data collection capability. Our institution favors early multimodal prophylaxis with sequential compression devices (SCD), early mobilization and chemoprophylaxis on post-operative day 1. The secondary aim of the study was to perform a comprehensive retrospective analysis of any association of the use of chemoprophylaxis with clinical VTE and post-operative EDH.
Methods
Study Design and Patient Selection
This is a retrospective cohort study of a prospectively collected database of patients who received spine surgery requiring inpatient care at a high-volume tertiary care center in Seattle, WA between January 2016 and December 2019, level of evidence III. The study used the Premier Health Care Database and Agency for Healthcare Research and Quality (AHRQ) indicators. AHRQ Patient Safety Indicators (PSI)-9(Perioperative hemorrhage and hematoma) and 12(Perioperative PE or DVT) were used to identify all patients experiencing VTE and/or post-operative EDH. All safety data had been entered by dedicated Patient Quality and Safety staff and had been verified for clinical accuracy in an iterative prospectively collected fashion. The study protocol was reviewed and approved by the Institutional Review Board (#2020000515). A waiver of consent and HIPAA authorization was obtained based on meeting criteria of 45 CFR 46.116(f)(3) and 45 CFR 164.512(i)(2)(ii). Patients over 18 years of age who underwent spine surgery were included. Surgical procedures were identified as cervical, thoracolumbar or lumbosacral. ICD-10 procedure codes were used to identify patients who underwent spine fusion or instrumentation vs decompression alone. All types of spine surgical approaches were included, such as anterior, posterior, lateral and combined approaches. A complete list of AHRQ exclusion criteria can be found at www.qualityindicators.ahrq.gov. Patients were excluded if they were younger than 18 years old, had a present on admission diagnosis of pulmonary embolism (PE), proximal deep vein thrombosis, hemorrhage, or hematoma, pregnancy, ICD-10 diagnosis for coagulation disorder, receiving extracorporeal membrane oxygenation (ECMO), or acute traumatic brain or spinal cord injury on admission.
A total of 4764 hospital stays with surgery meeting inclusion criteria were captured by our database, of which 17 triggered PSI-9 and PSI-12 quality indicators. These 17 charts were then manually reviewed by two independent authors (A.M.M/S. F) to determine eligibility criteria, the use and timing of chemoprophylaxis and its relationship to clinical VTE or hemorrhage. Cases in question were adjudicated by a formal Neurosurgical review panel. Two of these cases were excluded after formal review and 15 charts were included in the formal analysis.
Primary Outcome
The primary outcome was to establish the clinical incidence of VTE and EDH in post-operative spine patients. Secondary outcomes included the association of chemoprophylaxis with clinical VTE and EDH. Predictors of clinical VTE and EDH were analyzed using demographics, comorbidities, length of stay (LOS), and peri-operative characteristics.
Statistical Analysis
The incidence of a perioperative clinical VTE or EDH was calculated as the number of events meeting our operational definition divided by the total number of cases meeting the eligibility criteria for this study. Demographics, medical history, LOS, procedural ICD-10 codes, and prior medications including anticoagulants were obtained from the electronic medical record.
Definitions
VTE was defined as the clinical diagnosis of deep vein thrombosis (DVT) and/or PE. Patients did not undergo routine elective surveillance screening post-operatively. DVTs were diagnosed based on clinical symptoms, such as lower extremity pain or swelling, and verified by venous duplex ultrasonography. PEs were diagnosed by spiral chest CT scans, nuclear ventilation-perfusion scintigraphy, and pulmonary angiography, all used either individually or in concert as needed. Relevant symptoms consisted of shortness of breath, hypoxia, pleuritic chest pain, and tachycardia. EDH was defined as symptomatic bleeding in the epidural space causing acute neurologic deficit and/or unplanned return to the operating room for evacuation. For patients who experienced a clinical VTE or EDH, the timing of the first dose of chemoprophylaxis and the drug used in relation to when the VTE or hematoma was recognized was assessed. Occurrences of clinical VTE and EDH met inclusion criteria for PSI-12 and PSI-9 respectively.
Institutional VTE Prophylaxis
At our institution, post-operative spine patients routinely receive mechanical prophylaxis with SCD and emphasis on earliest possible ambulation when not clinically contraindicated. Additionally, our protocol is to start chemoprophylaxis on post-operative day 1, 24 hours after surgery. In rare cases, the clinical provider or surgeon may withhold chemoprophylaxis based on clinical judgement. Our institution favors low molecular weight heparin, enoxaparin for all surgical patients. For patients with creatinine clearance (Cl) > 30 mL/min enoxaparin 40 mg subcutaneous daily was given. For patients with a CI < 30 mL/min the dose was adjusted to enoxaparin 30 mg subcutaneous daily or unfractionated heparin 5000 mg every 8 hours. For obese patients with BMI >40 the protocol was adjusted to 40 mg low molecular weight heparin subcutaneous twice daily.
Results
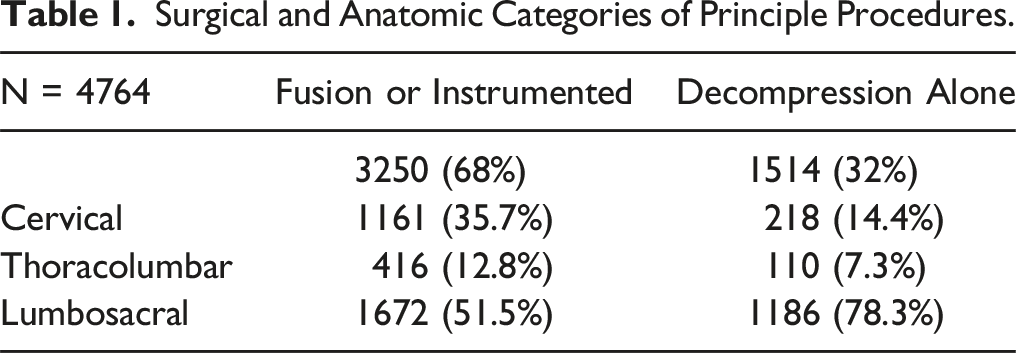
Surgical and Anatomic Categories of Principle Procedures.
Demographics, Age a .
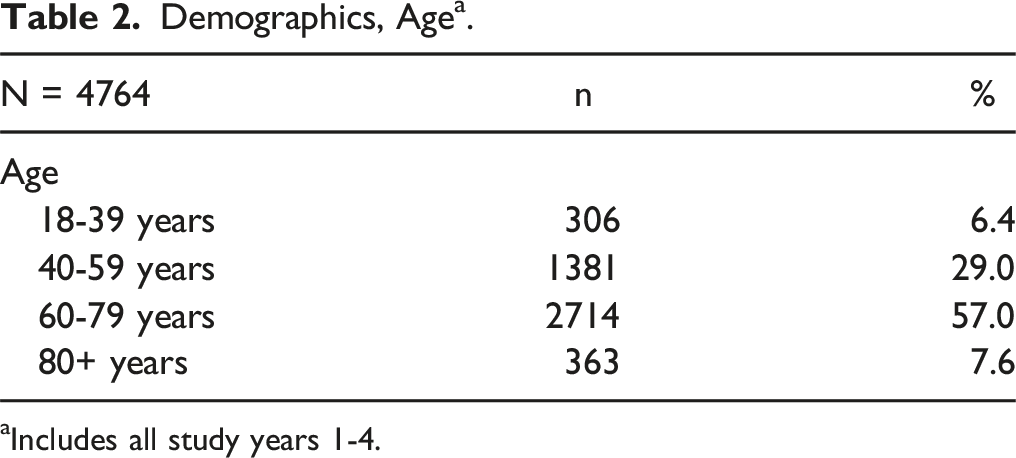
aIncludes all study years 1-4.
Demographics, Gender, Race, Ethnicity. a
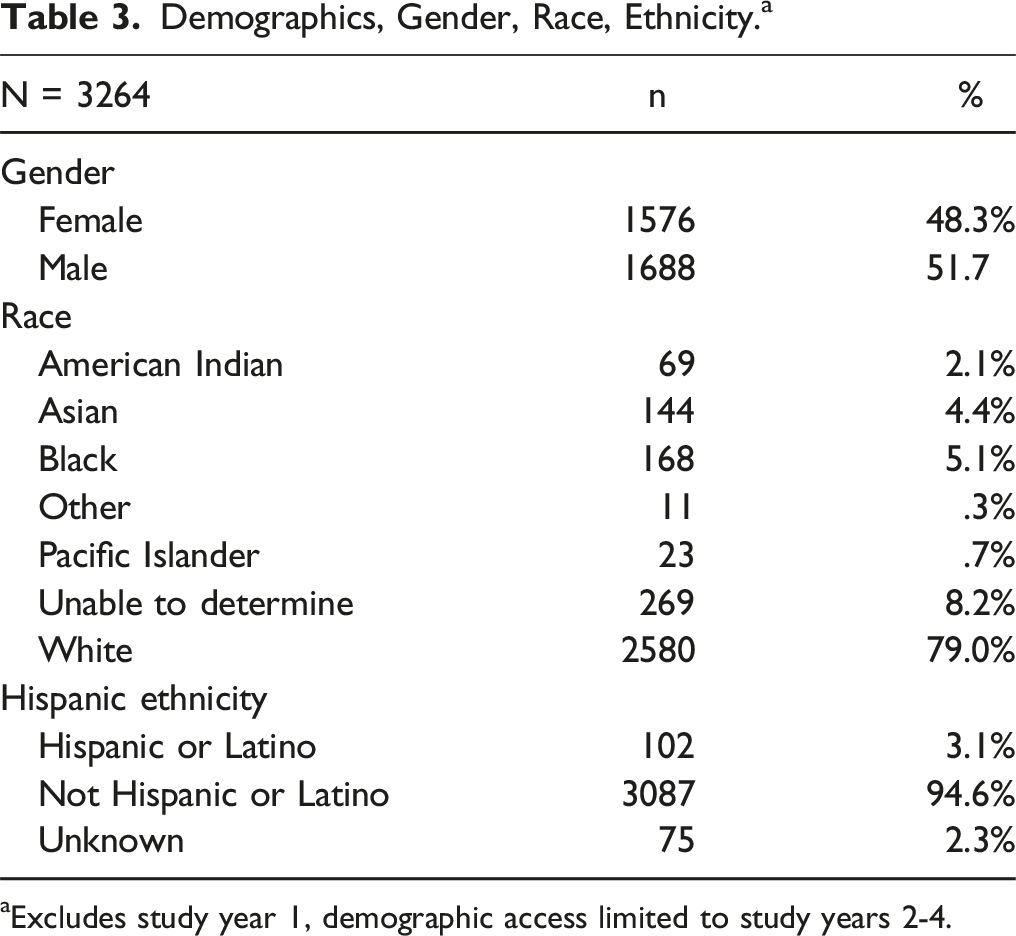
aExcludes study year 1, demographic access limited to study years 2-4.
Population Medical History. a
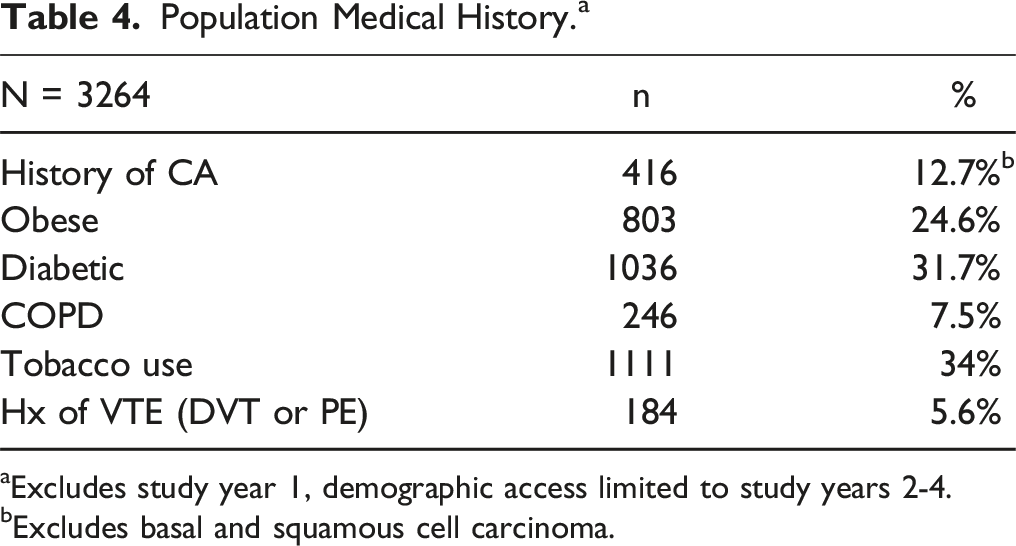
aExcludes study year 1, demographic access limited to study years 2-4.
bExcludes basal and squamous cell carcinoma.
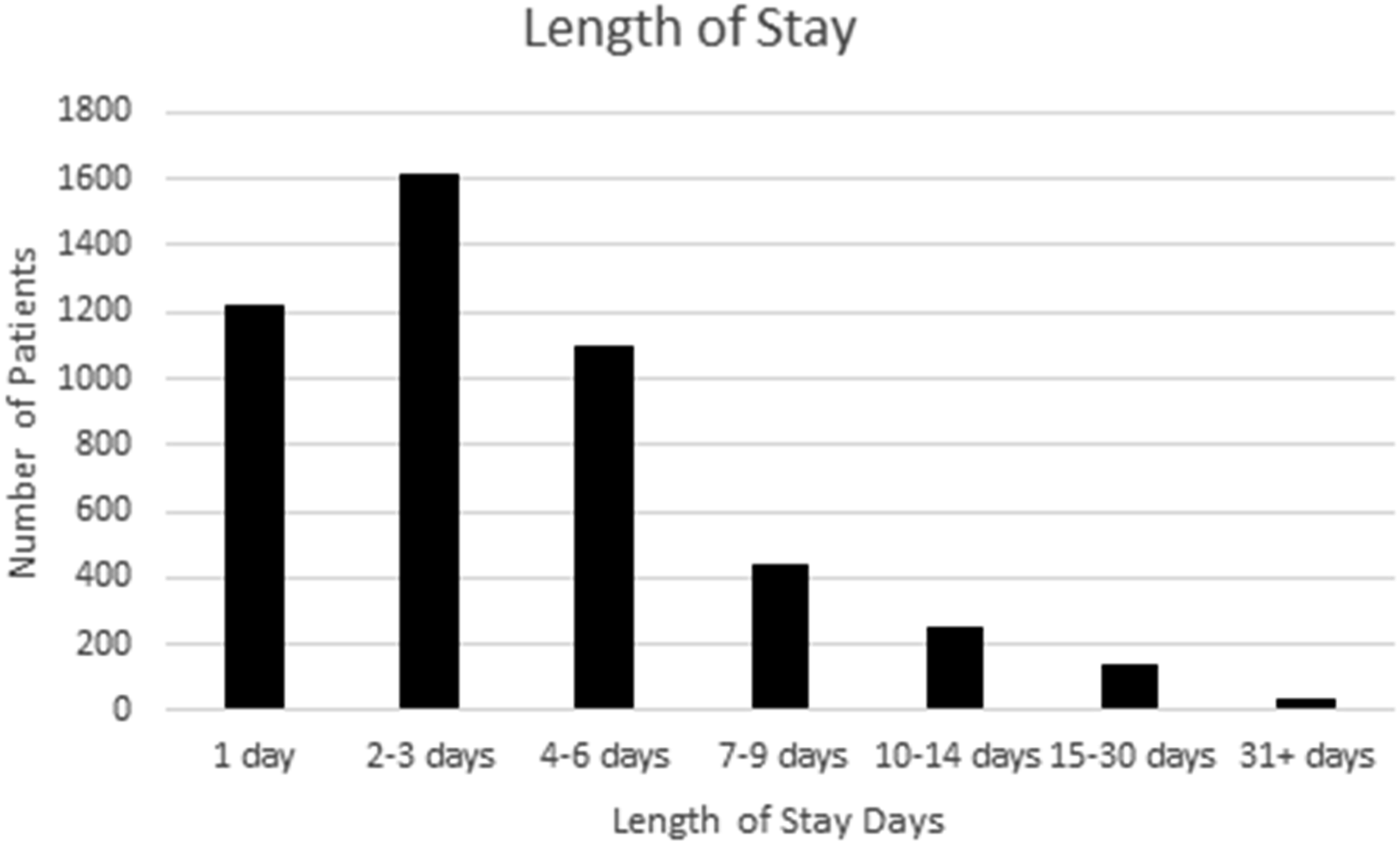
Length of stay.
Study Results.

Events by Surgical Categories.

Discussion
Study Results Alongside National Comparative Rates for Version 2019 of Agency for Healthcare Research and Quality (AHRQ) Quality Indicators, National Benchmark Data. 23
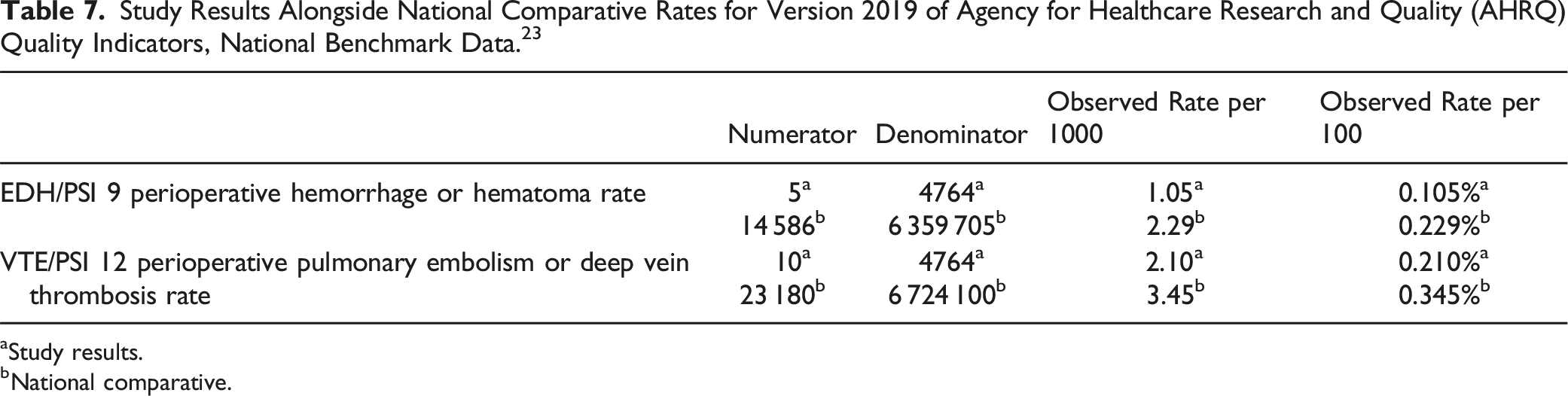
aStudy results.
bNational comparative.
Clinically significant EDH can have devastating neurologic effects. In only one of the 5 patients could we identify a temporal relationship between chemoprophylaxis and EDH. This patient had a dural tear in the operating room and was started on chemoprophylaxis on post-operative day 1. The patient subsequently had a drop in hemoglobin and hematocrit within 24 hours of starting chemoprophylaxis. Imaging revealed post-operative EDH and the patient went urgently to the operating room for evacuation of an EDH. Fortunately, the patient did not suffer permanent neurologic injury. Intra-operative dural tear has been identified as an independent risk factor for EDH. 19 Additional reported clinical risk factors include increased age, obesity (BMI >35), peri-operative transfusion and multilevel surgery (>2 levels). 19
Of note, 3 of the 5 patients identified with EDH were not on chemoprophylaxis at the time of hemorrhage. Of these 3 patients, one had epidural bleeding after fiducial marker placement without clinical deterioration. The patient proceeded to surgery the following day and had an uneventful hospital course. A second patient identified in our cohort had a polyetheretherketone (PEEK) intervertebral cage dislocation causing bilateral lower extremity weakness requiring take back to the operating room for repair. Intra-operatively an EDH was identified and evacuated. The third patient had extensive multifocal epidural abscesses who underwent a C5-C6 ACDF and L3-L5 laminectomy and had a protracted course related to the management of the systemic infection. On post-operative day 20 a repeat MRI of the lumbar spinal revealed a fluid collection in the laminotomy defect and surgical tract. Fortunately, there was no associated clinical decompensation, and the patient subsequently did not return to the operating room.
Although we used a large national database to identify our subjects, further detailed manual chart review allowed us to specifically identify the temporal association between EDH and chemoprophylaxis. We believe this granular data strengthens our argument that the perceived relationship between chemoprophylaxis and postoperative hemorrhage is overestimated. Most post-operative imaging will have evidence of some fluid accumulation, such as a seroma formation, in the surgical field and to mitigate this, post-operative drains are often left for longer periods of time in the surgical exposure sites. Our search identified 5 cases of EDH, however after manual chart review only 2 cases met our prespecified definition of EDH and there was only 1 case where chemoprophylaxis was given prior to identification of EDH. Two of the 5 patients returned to the operating room, making our true rate of symptomatic EDH closer to .04% (2/4764).
Interestingly, most patients (80%) were receiving chemoprophylaxis when clinical VTE was identified. Factors specific to VTE in spine patients include limited mobility due to post-operative pain or weakness, pre-existing disability and underlying comorbidities. 3 On manual chart review, 2 of the of 8 patients who developed clinical VTE were retrospectively found to have had a propensity for a hypercoagulable state. One patient had a history of unprovoked DVT and was on anticoagulation prior to surgery. This patient developed a contralateral clinical DVT on post-operative day 5. A second patient had a history of PE 2 years prior to surgery who was off anticoagulation prior to surgery and developed a clinical DVT and PE post operatively.
Surgery itself is known to promote the body’s natural clotting cascade causing a transient prothrombotic state.21,22 Two patients who developed DVT while not on chemoprophylaxis had hyperacute clinical VTE, presenting less than 24 hours post operatively. One patient developed hypoxia 6 hours post operatively and was found to have a PE. A second patient had a DVT found on post-operative day 1 prior to the initiation of chemoprophylaxis.
The rate of clinical VTE after spine surgery is also associated with the type of procedure. Similar to Schairer et al, 10 our fusion and instrumentation procedures had a much higher risk of clinical VTE compared with decompression alone (Table 6). Schairer also noted prolonged prone positioning and longer spinal fusions to have higher rates of clinical VTE. 10 Specific to elective spinal surgeries, Hohl et al 5 found a higher risk of clinical VTE with patients undergoing fusions of >5 segments. Patients undergoing longer and more complex surgeries should be considered at increased risk for post operative clinical VTE.
Implementation of early multimodal prophylaxis including chemoprophylaxis has been shown to be safe and effective. 3 Cox et al compared the rate of clinical VTE in almost 1000 post-operative spine patients 2 years pre and post implementation of an early and aggressive multimodal prophylaxis protocol that included chemoprophylaxis on post-operative day 1. They found a decrease in the rate of clinical VTE after protocol implementation (DVT 1%, PE .5%) compared to pre-protocol rates of DVT 2.7% and PE .6%. 3 In addition, there was not a statistically significant increase in the rate of EDH (.6% pre-protocol and .4% post protocol). Furthermore, in a meta-analysis of 4383 patients, Sansone et al 2 found the use of pharmacologic prophylaxis significantly reduced the prevalence of symptomatic and asymptomatic VTE relative to either mechanical prophylaxis or no prophylaxis. We believe our rate of clinical VTE was below the reported national range due to our early use of chemoprophylaxis, in combination with mechanical prophylaxis as well as mobilization protocol.
Our study has obvious limitations, chief of which is the likely underreporting of VTE and EDH events. Our institution serves as a regional referral center and many patients travel long distances for surgery. Patients may have presented to their local hospital or primary care physician with clinical PE and/or DVT after being discharged from our institution without reporting the event to us despite a comprehensive follow-up system. One large cohort that followed patients for 90 days observed that 40% of clinical VTE were diagnosed after discharge from the hospital, with a median time of 9 days. 10 Our average LOS was 4.3 days (LOS decompression alone median: 2 days; LOS fusion median: 3 days), therefore it is plausible that more patients experienced clinical VTEs in outside facilities. We did not contact all 4764 patients to verify a subsequent clinical VTE, so our data may underreport the true prevalence of clinical VTE. Likewise, we did not screen for asymptomatic extremity DVTs and the prevalence of .21% therefore could be an underestimation. However, the importance of subclinical events is not well established. 24 Retrospective cohort studies are also potentially more prone to bias than a prospective cohort study, however, when studying an outcome as rare as PE, DVT and EDH, a well-designed retrospective study can provide valuable information regarding the relationship between an exposure and a specific outcome. The data reported to the national data base clearing house was however, collected and vetted in a prospective fashion and any VTE or EDH event known to our practitioners would have been entered, even if a patient did not get readmitted.
Finally, we did not sub-differentiate various clinical spine pathologies such as oncologic, infectious, and traumatic indications and surgical approaches and the invasiveness of the underlying surgery performed. Acute traumatic spinal cord injury was excluded based on our database. Our VTE prevention protocol was, however, applied universally for all patients regardless of their indication or type of surgery performed. Most importantly the outcome variables investigated were universally applicable to all conditions and then specifically scrutinized as to possibly associated underlying risk factors.
A strength of our study is the large number of patients treated at a single institution with a very consistent general and specific treatment algorithm and a robust data collection methodology. In fact, this is one of the largest studies of its kind reported on this subject in the field of spine surgery, which remains contentious even in recent guidelines recommendation efforts. Clinical implications from our study are as follows: while the overall incidence of clinical VTE remains relatively low, considering its serious adverse clinical implications, multimodal prophylaxis efforts in patients receiving major spine surgery seem to clearly benefit from inclusion of early chemoprophylaxis protocol, modifiable based on individual patient factors. In addition, the risk of EDH formation appears to be very low despite initiation of early chemoprophylaxis and does not seem to be affected by use of chemoprophylactic agents.
Conclusion
Although, the timing and use of perioperative chemoprophylaxis is controversial given the lack of consensus, this review of almost 5000 patients adds to the growing body of literature that chemoprophylaxis after spine surgery is safe. Our institution favors early multimodal prophylaxis with SCDs, early mobilization and chemoprophylaxis on post-operative day 1. Despite early chemoprophylaxis, we did not appreciate elevated rates of EDH. Undoubtedly, the debate about efficacy and safety of chemotherapeutic agents will continue, but in absence of further data, we find our approach towards early initiation of chemoprophylaxis following major spine surgery to be a safe approach.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.