
Abstract
Study Design
Retrospective cohort study.
Objectives
This study aimed to (1) evaluate for any temporal trends in the rates of VTE, deep venous thrombosis (DVT), pulmonary embolism (PE), and mortality from 2011 to 2020 and (2) identify the predictors of VTE following lumbar fusion surgery.
Methods
Annual incidences of 30-day VTE, DVT, PE, and mortality were calculated for each of the operation year groups from 2011 to 2020. Multivariable Poisson regression was utilized to test the association between operation year and primary outcomes, as well as to identify significant predictors of VTE.
Results
A total of 121,205 patients were included. There were no statistically significant differences in VTE, DVT, PE, or mortality rates among the operation year groups. Multivariable regression analysis revealed that compared to 2011, operation year 2019 was associated with significantly lower rates of DVT. Age, BMI, prolonged operation time, prolonged length of stay, non-home discharge, anterior fusion, smoking status, functional dependence, and chronic steroid use were identified as independent predictors of VTE following lumbar fusion. Female sex, Hispanic ethnicity, and outpatient surgery setting were identified as protective factors from VTE in this cohort.
Conclusions
Rates of VTE after lumbar fusion have remained mostly unchanged between 2011 and 2020. Older age, higher BMI, longer operation time, prolonged length of stay, non-home discharge, anterior fusion, smoking, functional dependence, and steroid use were independent predictors of VTE after lumbar fusion, while female sex, Hispanic ethnicity, and outpatient surgery were the protective factors.
Keywords
Introduction
Venous thromboembolic events (VTEs), including pulmonary emboli (PE) and deep venous thrombosis, are amongst the most feared but preventable post-operative complications of orthopaedic surgery. 1 While there are clinical guidelines that patients undergoing total joint arthroplasty and hip fractures should receive antithrombic prophylaxis postoperatively for at least 10-14 days, the recommendations for chemoprophylaxis in spinal surgery are less clear. 2
Thromboembolic prophylaxis is seldom used in spine surgery due to possibility of epidural hematomas (EDHs). Surgeons, therefore, must balance the risk of DVT/PE against this catastrophic complication. As a result, anticoagulation is often delayed for a period of time based on surgeons’ personal experience until the postoperative bleeding risk is perceived to be sufficiently low. 2
This variability in thromboembolic prophylaxis practice seems to be the result of a glaring lack of published data. It has been found that the incidence of postoperative thromboembolic disease in spinal patients can range from .3% to 31%. However, these estimates are based on relatively small studies in heterogenous populations with different spine surgeries using various detection methods. 3
From 1998 to 2014, the utilization rate for spinal fusions has nearly doubled from 74 to 139 cases per 100,000 persons, with lumbar fusion being the primary driver of this trend. 4 In a report published in 2014, spinal fusions accounted for the highest aggregate hospitals costs ($12.8 billion in 2011) of any surgical procedure performed in U.S. hospitals. 5 Because of the high volume and cost of lumbar fusions, it is crucial to assess postoperative complications in these patients. 6 Despite increasing surgeon experience and more advanced techniques, complications rates, however, have remained relatively stable over time. 4
Furthermore, current literature regarding the incidence, trend, and predictors of VTE after lumbar fusion is severely limited.4,7 Previous database studies on VTE events after spine surgery have focused on general trends among all surgery types rather than analyzing for time-dependent trends in incidence rates and risk factors particular to lumbar fusion. Therefore, this study aimed to (1) evaluate for any temporal trends in the rates of VTE, DVT, PE, and mortality from 2011 to 2020 and (2) identify the predictors of VTE following lumbar fusion surgery.
Methods
This retrospective cohort study utilized the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database. Informed consent and Institutional Review Board approval were not required for this study as it utilized a publicly available, de-identified national surgical database, and no direct patient involvement occurred. Adult patients who underwent primary lumbar fusion from 2011 to 2020 were identified using Current Procedural Terminology (CPT) codes 22612, 22630, 22633, and 22558. Anterior fusion (22558) was examined as a distinct variable due to the inherent VTE risk associated with manipulation of the great vessels. 8 Exclusion criteria included cervical or thoracic fusion, arthroplasty, non-elective cases, emergency cases, deformity procedures, operative levels of 6 levels or greater (to exclude deformity cases with elevated risks of VTE),9,10 osteotomy, revision surgery, malignancy, preoperative sepsis, wound infection, unexpected weight loss, and missing demographic or perioperative variables. In addition, patients were excluded for any primary International Classification of Diseases diagnosis codes indicating trauma, tumor, or infection.
Patient demographics and perioperative variables were extracted from the NSQIP database, including age, sex, race, ethnicity, BMI, operation time, surgery setting (inpatient vs outpatient), length of hospital stay after surgery (LOS), location of discharge disposition (home vs non-home), and anterior fusion. Non-home discharge disposition included discharge to rehabilitation center or non-home skilled care facility. Comorbidities extracted from the database included diabetes mellitus, current smoking status, dyspnea, functional dependence, chronic obstructive pulmonary disease (COPD), congestive heart failure (CHF), hypertension requiring medications, dialysis, chronic steroid use, bleeding disorder, wound class, and American Society of Anesthesiologists (ASA) class. Wound class variable was binarized into class ≥2 vs <2 (wound class greater than 1 implies a degree of contamination and/or infection), and ASA class variable was binarized into class ≥3 vs <3, consistent with common reporting methods used in prior literature.11-15
The primary outcomes of interest included 30-day incidences of VTE, DVT, PE, and mortality. In the NSQIP database, DVT is defined as a new diagnosis of a blood clot or thrombus within the superficial or deep venous system which has been confirmed by duplex ultrasonography, venogram, or computed tomography scan. PE is defined as a new diagnosis of a blood clot in a pulmonary artery causing partial or complete obstruction of the lung vasculature confirmed by ventilation-perfusion scan. The incidence of VTE was calculated by the occurrence of a DVT and/or PE in the same patient.
Baseline Patient Characteristics by Operation Year.
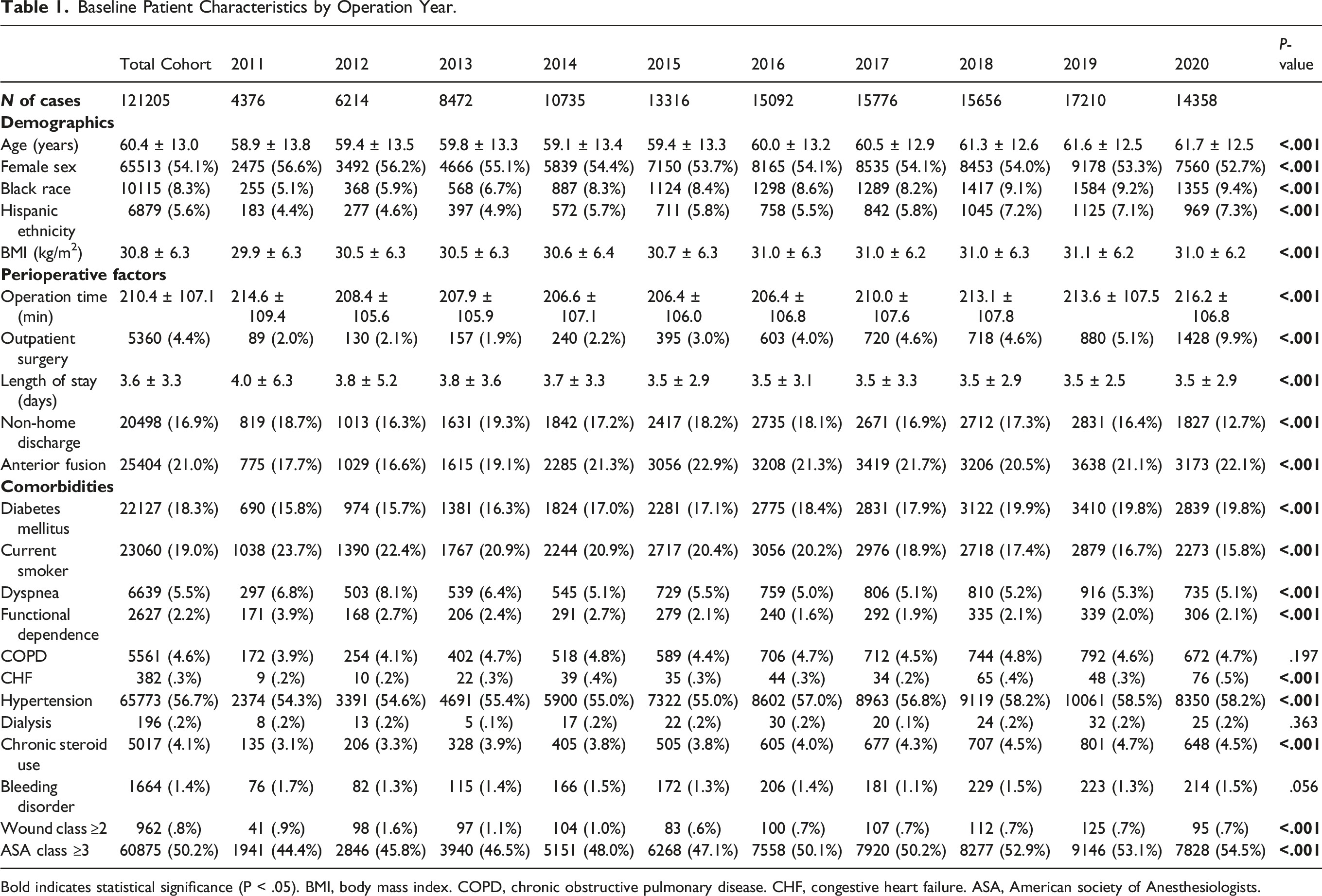
Bold indicates statistical significance (P < .05). BMI, body mass index. COPD, chronic obstructive pulmonary disease. CHF, congestive heart failure. ASA, American society of Anesthesiologists.
Results
A total of 121,205 patients were included with the following distribution of operation years: 4376 (3.6%) patients in 2011, 6214 (5.1%) patients in 2012, 8472 (7.0%) patients in 2013, 10,735 (8.9%) patients in 2014, 13,316 (11.0%) patients in 2015, 15,092 (12.5%) patients in 2016, 15,776 (13.0%) patients in 2017, 15,656 (12.9%) patients in 2018, 17,210 (14.2%) patients in 2019, and 14,358 (11.8%) patients in 2020 (Table 1). The mean age of the total study population was 60.4 ± 13.0 years, and the mean BMI was 30.8 ± 6.3 kg/m2. The total cohort included 65,513 (54.1%) females, 10,115 (8.3%) patients of Black race, and 6879 (5.7%) patients of Hispanic ethnicity. 5360 (4.4%) cases were performed in the outpatient setting, and 20,498 (16.9%) patients were discharged to a non-home destination. 25,404 (21.0%) cases involved an anterior lumbar fusion.
Patient demographics, perioperative variables, and comorbidities were compared among operation year groups to assess for baseline differences. Proportions and means which significantly differed among operation year cohorts included age, sex, race, ethnicity, BMI, mean operation time, outpatient surgery setting, LOS, non-home discharge, anterior fusion, diabetes mellitus, current smoking status, dyspnea, functional status, CHF, hypertension, steroid use, wound class, and ASA class (P < .05) (Table 1).
Incidence of Venous Thromboembolism and Mortality for Lumbar Fusion by Operation Year.

VTE, venous thromboembolism. DVT, deep venous thrombosis. PE, pulmonary embolism.
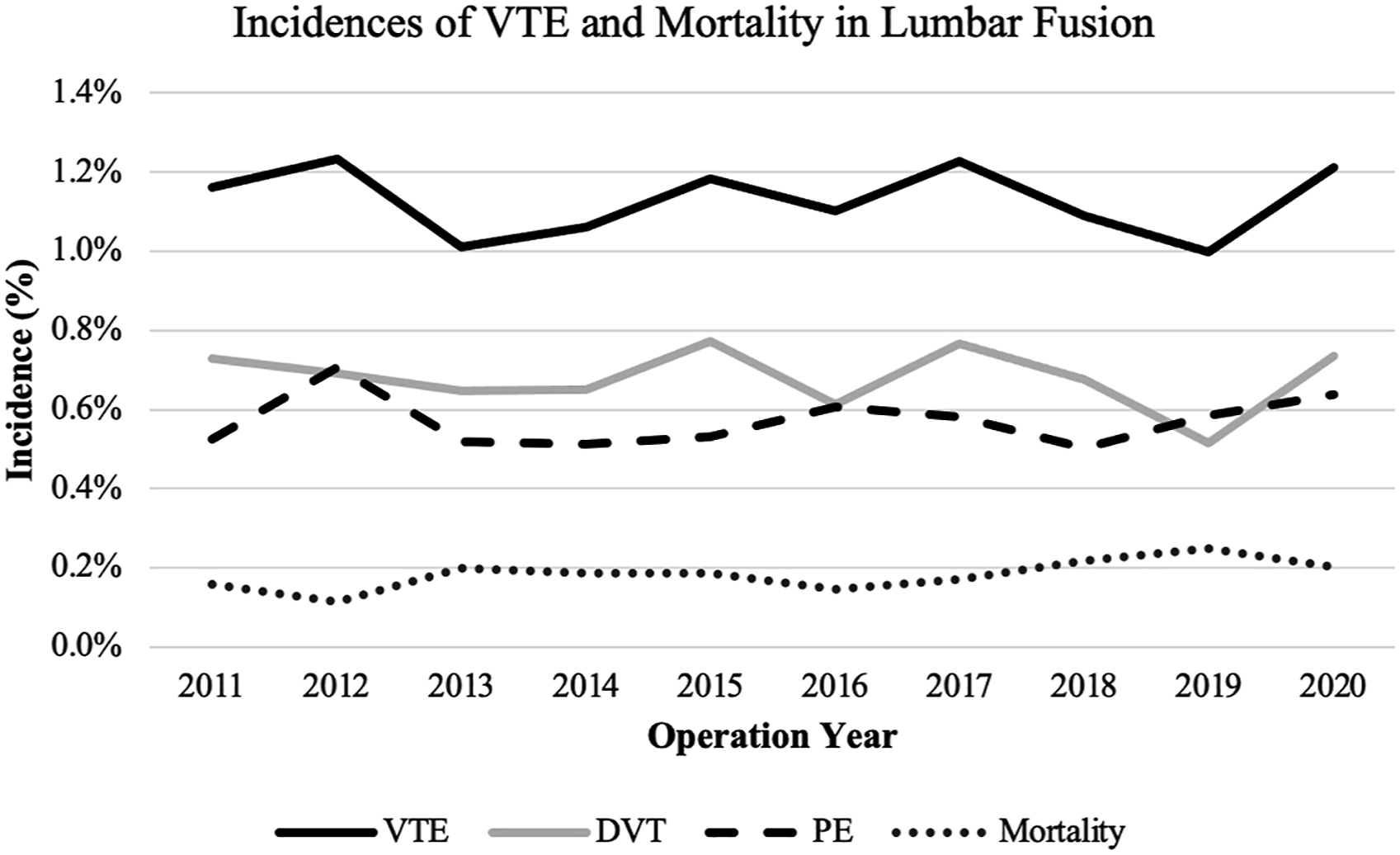
Incidences of VTE and mortality in lumbar fusion
Adjusted Multivariate Regression Analysis of VTE and Mortality.
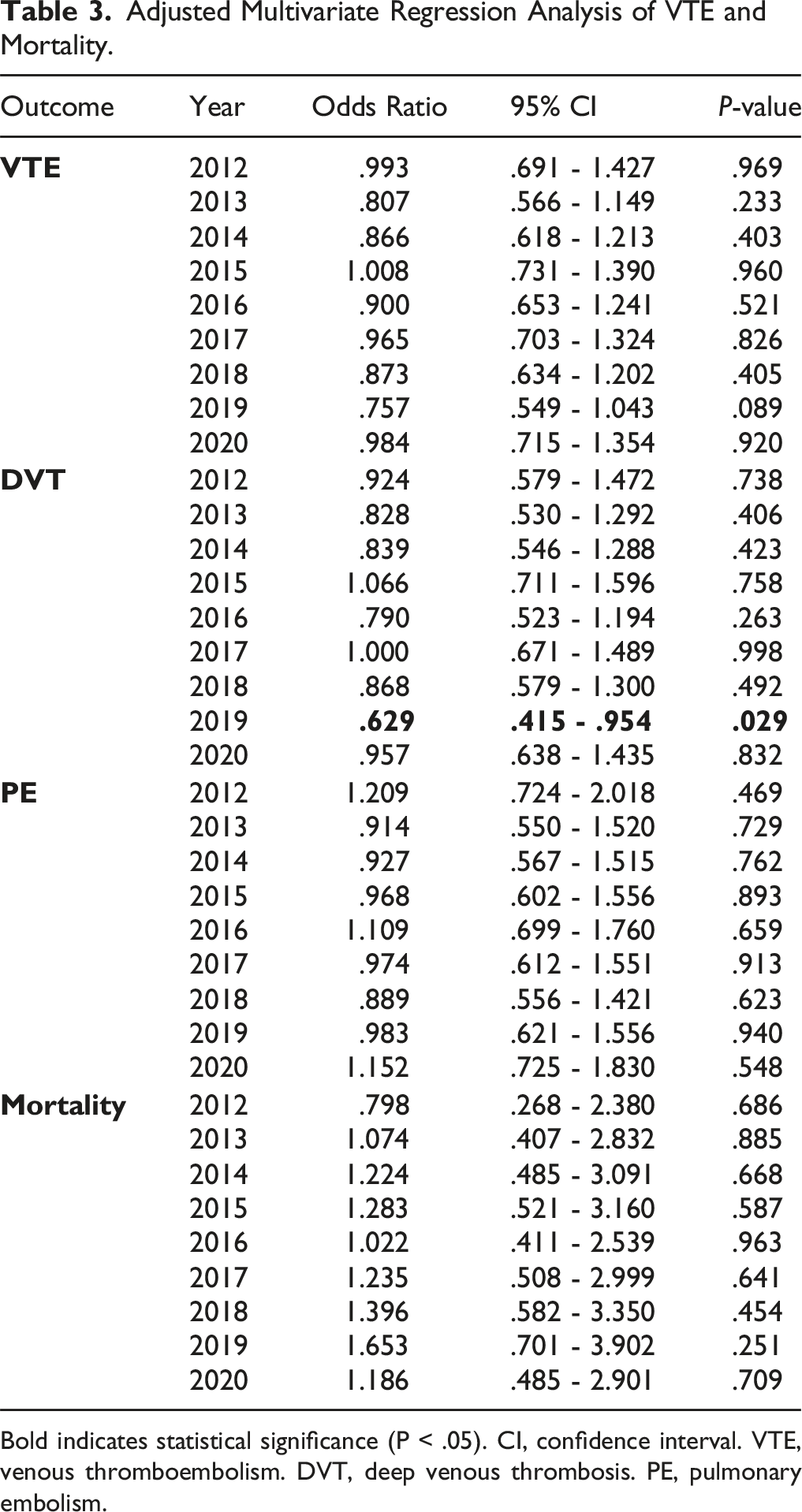
Bold indicates statistical significance (P < .05). CI, confidence interval. VTE, venous thromboembolism. DVT, deep venous thrombosis. PE, pulmonary embolism.
Predictors of VTE following Lumbar Fusion.
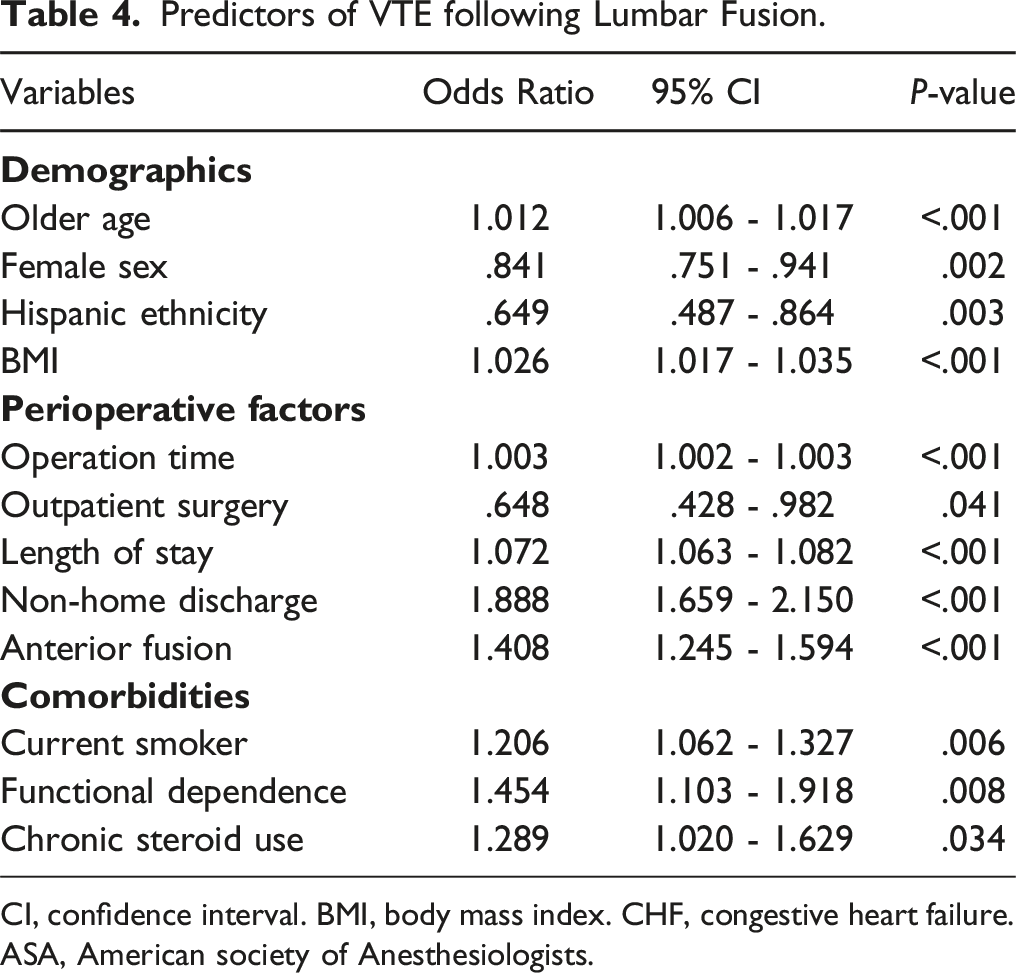
CI, confidence interval. BMI, body mass index. CHF, congestive heart failure. ASA, American society of Anesthesiologists.
Discussion
The current study aimed to evaluate for any temporal trends in the incidence rates of VTE and mortality following lumbar fusion, as well as to identify the predictors of VTE after lumbar fusion. Our analysis revealed that the rates of VTE and mortality have remained mostly unchanged between 2011 and 2020. In addition, older age, higher BMI, prolonged operation time, prolonged LOS, non-home discharge disposition, anterior fusion, smoking, functional dependence, and steroid use were independent predictors of VTE after lumbar fusion, while female sex, Hispanic ethnicity, and outpatient surgery were the protective factors.
Historically, the incidence of VTE after spinal surgery has been reported to range from .3% to 31%, reflecting the variability of patient populations studied, presentation of symptoms, diagnostic methodology, and post-operative care. 17 It has been found that patients diagnosed with a VTE have been hospitalized approximately 10 days longer than those without. Hospital costs doubled for patients who had undergone lumbar fusion with VTE from approximately $25,000 to over $50,000, likely due to increased hospitalization, diagnostic tests, and treatment. To add, mortality in lumbar fusion patients increases 40-fold with a PE. 3 Thus, VTEs are a notable source of morbidity, mortality, and increased healthcare utilization that requires attention from the spine community.
Our analysis reveals overall incidence rates of 1.1%, .7%, .6%, and .2% for VTE, DVT, and PE, respectively, after lumbar fusion between 2011 and 2020. This is consistent with that of current literature which reports VTE rates ranging from .2% to 4.3%.7,18,19 From 2002 to 2009 using the Nationwide Inpatient Sample (NIS) database, Fineberg et al reported a VTE rate after lumbar spine surgery to be .49% with incidences of DVT .34% and PE .18%. 3 Furthermore, Nazareth et al reported a VTE incidence rate of 2.57% after lumbar spine surgery using the 2007 to 2014 Humana private insurance PearlDiver database. 7 Although these rates are relatively low, a distinction must be made in the literature between fusions and less invasive lumbar procedures, including isolated laminectomy and discectomy, since they have been shown to have lower postoperative VTE incidences compared with fusion procedures. 7 This difference is likely attributable to the fact that fusion requires increased exposure, greater blood loss, immobilization, and postoperative hospitalization.3,20-23
Within the last decade and since the latest North American Spine Society (NASS) guidelines in 2009, our rates of VTE and mortality in lumbar fusions have not significantly declined. This is in contrary to total knee arthroplasties which have seen a significant reduction in DVTs, PEs, and VTEs from 2008 to 2016. 24 While spine surgeons must weigh the .2% to .9% epidural hematoma rates, this lack of improvement despite the continual advancements in surgical skills, techniques, and technology highlights the need for higher quality data and more efficacious patient specific guidelines for VTE prophylaxis to address this life threatening complication. 18
The 2009 NASS guidelines recommend initiating mechanical prophylaxis for patients undergoing elective spine surgery. 25 Guidelines state that chemical prophylaxis is safe to initiate the day of elective spine surgery. Meanwhile, the most American College of Chest Physicians (ACCP) guidelines do not recommend routine use of VTE chemoprophylaxis for elective spine surgery. 18 For patients with identifiable risk factors and high-risk groups, it is recommended for at least 1 type of DVT prophylaxis or a combination of chemoprophylaxis and mechanical prophylaxis, respectively. Unfortunately, none of these recommendations provide a duration for these treatment guidelines.18,25
Within our analysis of risk factors, we found that older age, higher BMI, operation time, LOS, non-home discharge, anterior fusion, smoking status, functional dependence, and steroid use were independent predictors of VTE following lumbar fusion. This aligns with prior reports that have highlighted age, obesity, smoking status, functional status, LOS, and operation time as risk factors of VTE.4,7,26-28 In particular, our finding that chronic steroid use increases VTE risk aligns with a recent 2019 retrospective database study composed of 838,507 degenerative spine cases where they published that steroid use was independently associated with a higher likelihood of readmission with VTE. 18 Our finding corroborates the notion that providers should be mindful of the harmful effects of steroid usage despite the potential anti-inflammatory benefits they pose in the perioperative period.
While modifiable clinical and surgical risk factors such as obesity, smoking, functional status, and operation time have been previously identified, this is the first lumbar study to assess LOS as a predictive factor vs outcome measure for VTE events.4,7,28 This may be attributed to the fact that longer hospitalization time may predispose patients to stay in bed for prolonged periods, increasing the risk for VTE. 26 In addition, patients with increased LOS may be prone to more comorbidities and other VTE risk factors. Nevertheless, daily and efficacious inpatient physical therapy should play a vital role in the postoperative period to increase ambulatory status.
To our knowledge, our study is the first to demonstrate outpatient lumbar fusion surgery as protective for VTE risk. This could be due to the earlier mobilization status, shorter operation times, and less likelihood of diagnosing especially asymptomatic VTE postoperatively. 29 Also, these patients likely have greater preoperative functional status and fewer comorbidities, decreasing VTE risk. Contrary to previous studies, female sex was a protective factor for VTE risk.7,26 Our results reinforce that all genders should be encouraged to ambulate as soon as possible safely after surgery.
Anterior approach to lumbar fusion has been previously identified as a risk factor for VTE, 30 and our results help to confirm this association. In a propensity-matched analysis of 1147 patients undergoing lumbar fusion, Cloney et al noted that anterior approach surgery caused an increase in VTE rate by 7.2%. 8 This association between anterior lumbar fusion and heightened VTE risk can be explained by the need to manipulate and compress major abdominal vessels during surgery, predisposing to both arterial thrombosis and VTE. 31 Therefore, utilization of an anterior approach may be an important factor when considering the risks of VTE in a patient undergoing lumbar fusion. Some patients undergoing anterior lumbar fusion may be candidates for VTE chemoprophylaxis, especially in the setting of intraoperative vascular injury. 32
Despite the large study population, limitations of this study should be recognized. There are variables associated with a patient’s risk of VTE that are not captured in NSQIP.24,27 The overall rate of VTE may be understated since it has been reported that up to 40% of VTE cases are diagnosed at hospitals separate from the institution the surgery was performed. 33 Not all patients are screened for VTE, so our incidence represents patients who were symptomatic and determined to have VTEs. We were unable to identify which patients in our cohort received thromboprophylaxis during the perioperative period. Furthermore, NSQIP is limited to 30-day postoperative VTEs. While studies have shown that highest risk of VTE is within the first week, ACCP suggests that patients are at an increased risk of VTE for up to 90 days.7,24 Despite these limitations, this study is, to the best of the authors’ knowledge, the most recent and comprehensive nationwide evaluation of temporal trends in VTE rates after lumbar fusion surgery.
Conclusion
The current study revealed that the rates of VTE after lumbar fusion have not improved between 2011 and 2020. In addition, older age, higher BMI, longer operation time, prolonged length of stay, non-home discharge, smoking, functional dependence, and steroid use were independent predictors of VTE after lumbar fusion, while female sex, Hispanic ethnicity, and outpatient surgery were the protective factors. To the authors’ knowledge, this analysis provides the most recent and comprehensive nationwide evaluation of temporal trends in VTE rates after lumbar fusion surgery. Further research is needed to establish patient and/or procedure specific guidelines, which include demographic and surgical risk factors, for VTE prophylaxis in spine surgery.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.