
Abstract
Study Design:
Review.
Objective:
Venothromboembolic (VTE) complications, composed of deep vein thrombosis and pulmonary embolism are commonly observed in the perioperative setting. There are approximately 500 000 postoperative VTE cases annually in the United States and orthopedic procedures contribute significantly to this incidence. Data on the use of VTE prophylaxis in elective spinal surgery is sparse. This review aims to provide an updated consensus within the literature defining the risk factors, diagnosis, and the safety profile of routine use of pharmacological prophylaxis for VTE in elective spine surgery patients.
Methods:
A comprehensive review of the literature and compilation of findings relating to current identified risk factors for VTE, diagnostic methods, and prophylactic intervention and safety in elective spine surgery.
Results:
VTE prophylaxis use is still widely contested in elective spine surgery patients. The outlined benefits of mechanical prophylaxis compared with chemical prophylaxis varies among practitioners.
Conclusion:
The benefits of any form of VTE prophylaxis continues to remain a controversial topic in the elective spine surgery setting. A specific set of guidelines for implementing prophylaxis is yet to be determined. As more risk factors for thromboembolic events are identified, the complexity surrounding intervention selection increases. The benefits of prophylaxis must also continue to be balanced against the increased risk of bleeding events and neurologic injury.
Keywords
Introduction to Deep Vein Thrombosis, Pulmonary Embolism, and Venous Thromboembolism
Venothromboembolic (VTE) complications, composed of deep vein thrombosis (DVT) and pulmonary embolism (PE) are commonly observed in the perioperative setting. There are approximately 500 000 postoperative VTE cases annually in the United States and orthopedic procedures contribute significantly to this incidence. 1 Total hip and knee arthroplasty carry the weight of this reported data, as high-quality publications examining other orthopedic procedures are lacking in number. Data on the use of VTE prophylaxis in elective spinal surgery is sparse. In the past decade, a handful of studies have analyzed the use of different VTE prophylactic agents; however, there is no consensus regarding the timing and most efficacious use of these agents.
Without prophylactic intervention, the incidence of postoperative symptomatic VTE ranges between 8% and 30% 2 -4 across all orthopedic procedures. The incidence of VTE after spine surgery specifically ranges between 0.2% and 31%. 5 -17 Traumatic spinal cord injury (SCI) patients have the highest incidence of thromboembolic events, ranging from 50% to 100% in untreated cases. 18 Due to the damaging nature of traumatic spinal cord injuries, prophylactic anticoagulation to prevent VTE is often automatically administered, even in the absence of any confounding risk factors.
However, VTE prophylaxis does not come without complications. Specific to spine surgery, the risks of bleeding secondary to VTE prophylaxis can be detrimental due to possible formation of an epidural hematoma and resultant neurologic injury. Therefore, the benefits of prophylaxis must be balanced against the increased risk of postoperative bleeding events, hematoma, and neurologic injury.
The incidence of VTE in elective spine surgery is much lower than the incidence in traumatic spine injury and the indications, or need, for VTE prophylaxis are unclear. Investigation of the efficacy, timing, and need for VTE prophylaxis after elective spinal surgery is a novel field, therefore elective spine surgery will be the focus of this review. This review aims to provide an updated consensus within the literature defining the risk factors, diagnosis, and the safety profile of routine use of pharmacological prophylaxis for VTE in elective spine surgery patients.
VTE Incidence in Spine Surgery
Differences in VTE incidence have been studied for a wide range of spinal procedures and pathologies and for this reason, it is difficult to make a definitive statement regarding the incidence of VTE in spine surgeries versus a specific procedure such as a hip arthroplasty. 19,20 The focus of this article is on elective spinal procedures, making a point to exclude trauma patients, spinal cord injuries, as well as malignancies of the spine. Few publications have exclusively examined VTE incidence in elective spinal surgery patients, however, the available literature suggests an incidence between 0.2% and 31%. 5 -8,10 -17,21,22
As many of these types of publications are international, it is imperative to note that guidelines for standard of practice regarding VTE prophylaxis in spine patients differs and thus incidence of VTE may differ. Studies of this nature are also likely retrospective designed, allowing for variation in prophylaxis protocols, imaging modalities, postoperative mobilization, and follow-up times. Because a thromboembolic event may occur after original discharge patients may seek care at a different hospital also making it more difficult to track VTE rates as well. Inconsistencies in the aforementioned categories across the literature make defining a universal protocol regarding prophylactic intervention in elective spine surgery almost impossible. It is therefore of the utmost importance for providers to be able to identify risk factors in order to best risk stratify the need for venous thromboembolic prophylaxis after elective spinal surgery.
VTE Risk Factors in Spine Surgery
VTE risk factors in patients undergoing spine surgery have been identified and stratified in the literature based on demographic variables such as age, sex, and weight as well as surgical variables such as vertebral level and surgical approach. A multitude of risk factors have been attributed to an increased risk of VTE; however, advanced age 22 -25 is the most commonly reported risk factor amongst published studies.
A 2016 retrospective study by Sebastian et al 15 looked at a total of 5405 patients from 1995 to 2012 that underwent cervical discectomy, laminectomy, corpectomy, laminoplasty, or fusion. Of these patients, they reported that 1.57% (106 patients) suffered either a DVT or PE within 30 days postoperatively and risk factors included chronic venous insufficiency, obesity, and ischemic heart disease. Consistent with the literature, they found that staged surgery had a markedly increased risk for VTE.
Staged surgeries when performed with a combined anterior-posterior approach boasted a significantly increased risk of VTE. Edwards et al 26 published a retrospective review in 2018 looking at single versus multistage posterior only spinal surgeries. Duplex ultrasound was used on the 107 total enrolled patients (26 multistage, 81 single stage) to identify patients with DVTs. They reported a DVT rate of 19% in multistage patients compared with 7% in single staged patients resulting in an 8.17 times higher risk of a DVT in multistage patients. It was mentioned that this risk difference may even be understated as the multistage group included had a lower preoperative and intraoperative VTE risk profile.
Pre- and postoperative ambulation levels have also been identified as independent risk factors for postoperative VTE. A 2015 retrospective clinical study 24 evaluated 80 patients undergoing spine surgery at a single institution. All patients were screened using ultrasonography to identify DVT in the lower extremities. They identified 20 of 80 patients (25%) with VTE and found that of all considered parameters, only preoperative walking disability and age affected VTE incidence. They suggested gait training during the early postop period in order to aid in the prevention of a thromboembolic event.
Nazareth et al 27 utilized an administrative database to identify 64 892 patients that underwent lumbar spine surgery between 2007 and 2014. They studied the rate of VTE at 1 week, 1 month, and 3 months postoperatively. Of the reported risk factors, primary coagulation disorders, extremity paralysis, and a central venous line were associated with the highest risk of VTE.
Both cervical and lumbar spine surgery present similar risk factors for postoperative VTE, however, the literature supports a slightly higher incidence associated with lumbar surgery. 27 -29 Yoshioka et al 30 published a prospective institutional study attempting to present VTE rates in spine surgery patients based on different pathologies, procedures or spinal levels. They enrolled 340 patients, excluding trauma and spinal cord injury patients, and split them into 4 groups based on procedure. A total of 90 patients with lumbar or lower thoracic degenerative disease were treated with instrumentation for spine fusion. Another group of 89 patients had cervical degenerative disease and were treated with posterior decompression or instrumentation for fusion. All patients were treated with mechanical prophylaxis only. They reported that of the 90 lumbar patients, 12 had VTE (13.3%) compared with 4 of the 89 cervical patients (4.5%). There was no comment however on the significance of this difference in the article.
Hohl et al 31 published a case-control study in 2015 including 5766 patients receiving elective thoracolumbar degenerative spine surgeries, defined as all multilevel laminectomies and all fusions, in order to establish the prevalence of venous thromboembolic events. They analyzed all approaches and noted the number of levels and excluded all trauma and infection patients. None of the included patients received pharmacologic prophylaxis; however, sequential compression devices were used routinely. The study reported an overall VTE rate of 1.5% (89/5766). More important, they found that patients undergoing fusions of 5 segments or more had a statistically significant 2.3% prevalence of VTE compared with the 1.2% prevalence in patients undergoing fusions of ≥3 segments. They reported an increasing prevalence of PE as the magnitude of surgery increased suggesting that the group with the highest risk could benefit from pharmacologic prophylaxis.
Recent studies have investigated the use of perioperative steroid administration and blood transfusions, both of which have been associated with an increased VTE risk. A 2019 retrospective database study 8 composed of 838 507 degenerative spine cases looked at readmissions secondary to VTE. They reported 3499 patients were readmitted with VTE within 30 days of discharge and 4321 patients were readmitted within 90 days of discharge. Using a multivariate logistic regression model, they found that steroid use was independently associated with a higher likelihood of readmission with VTE along with thoracolumbar surgery and an increased length of hospital stay. Horn et al 32 reported similar findings suggesting that postoperative steroid use contributes to hospital acquired conditions such as VTEs, surgical site infections, and urinary tract infections; the authors suggested caution should be taken despite the potential anti-inflammatory benefits steroids pose in the perioperative period.
Cloney et al 25 published a single institution retrospective cohort in 2018 looking at 6869 patients undergoing spine operations. Data was collected on patient demographics, surgery, hospital course, VTE rates, and epidural hematoma. Perioperative transfusions boasted a 2.25 odds ratio of patients experiencing a VTE within 30 days postoperatively and 7.38 odds ratio of experiencing an epidural hematoma. Their results identified transfusions as an independent predictor of VTE, readmission, reoperation, and symptomatic epidural hematomas. Johnson et al 33 reported similar findings as they compared thrombotic events in posterior spinal fusion patients who received transfusions versus those who did not. Of the 963 patients included in the study, 62.6% received transfusions. They reported that transfused patients had a significantly higher risk (4.6%) of thrombotic events compared with the nontransfused group (1.1%).
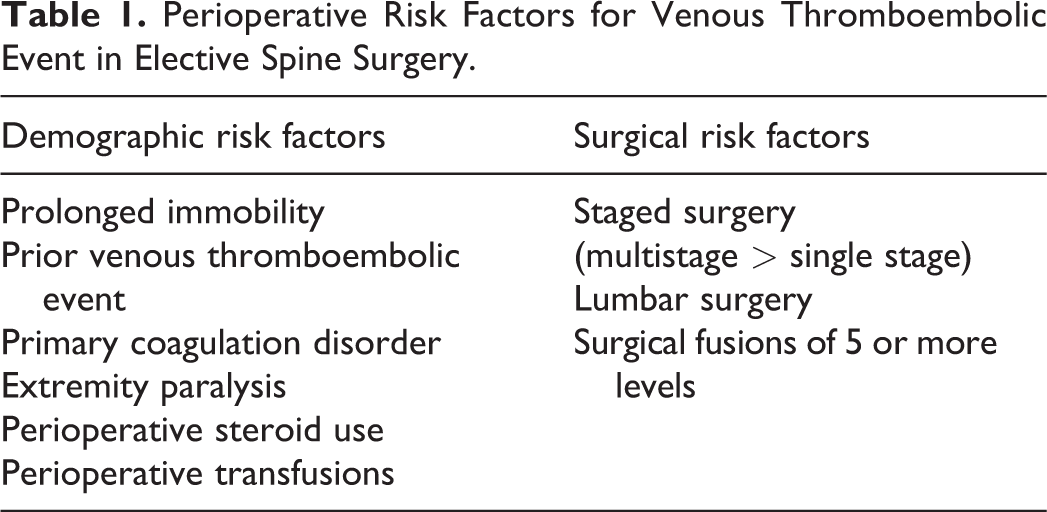
The presented risk factors (Table 1) above have been detailed throughout literature in the attempt to heighten clinical awareness in order to identify patients at greater risk for perioperative VTE complications who may require chemical VTE prophylaxis.
Perioperative Risk Factors for Venous Thromboembolic Event in Elective Spine Surgery.
Diagnosis of VTE
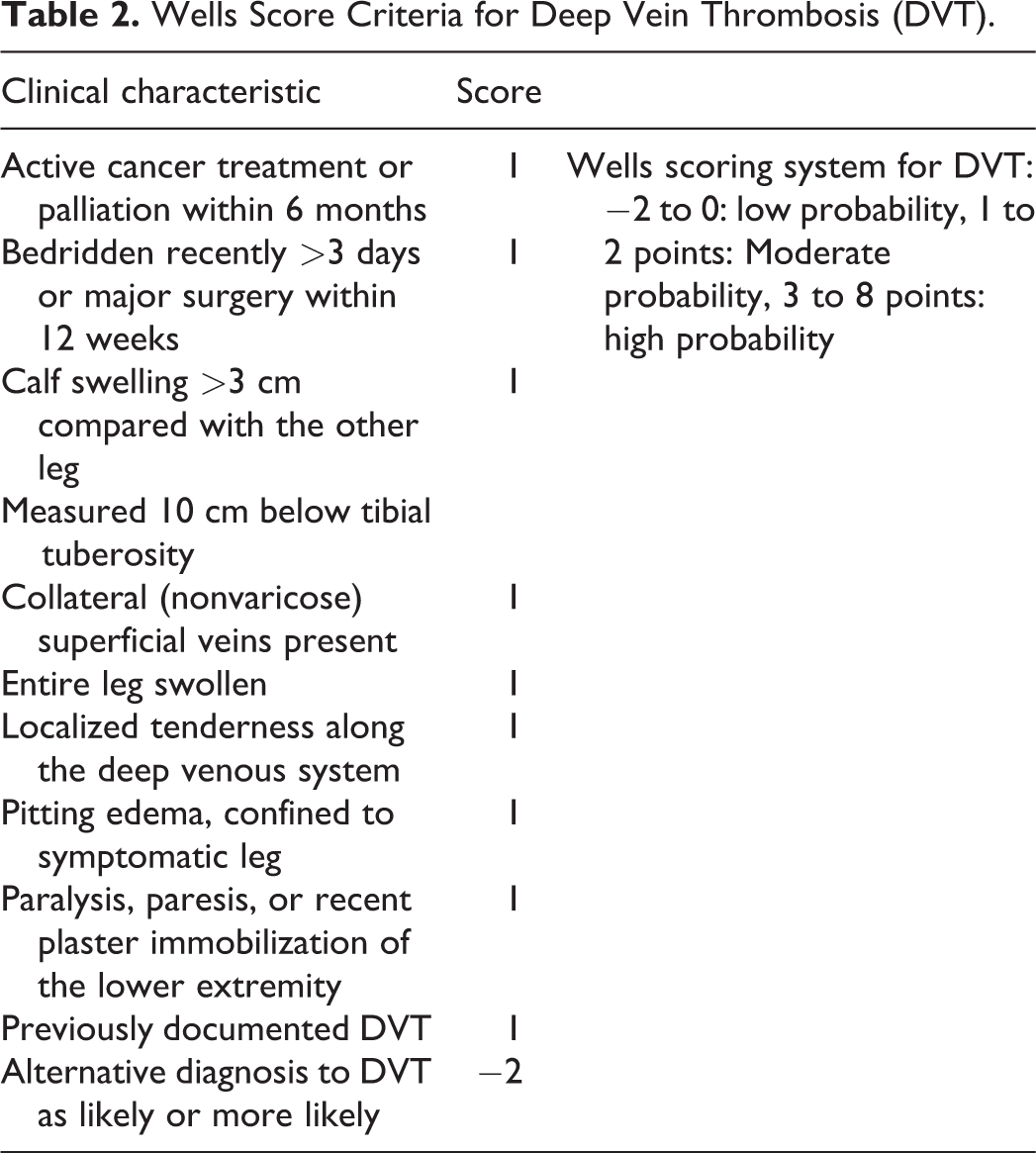
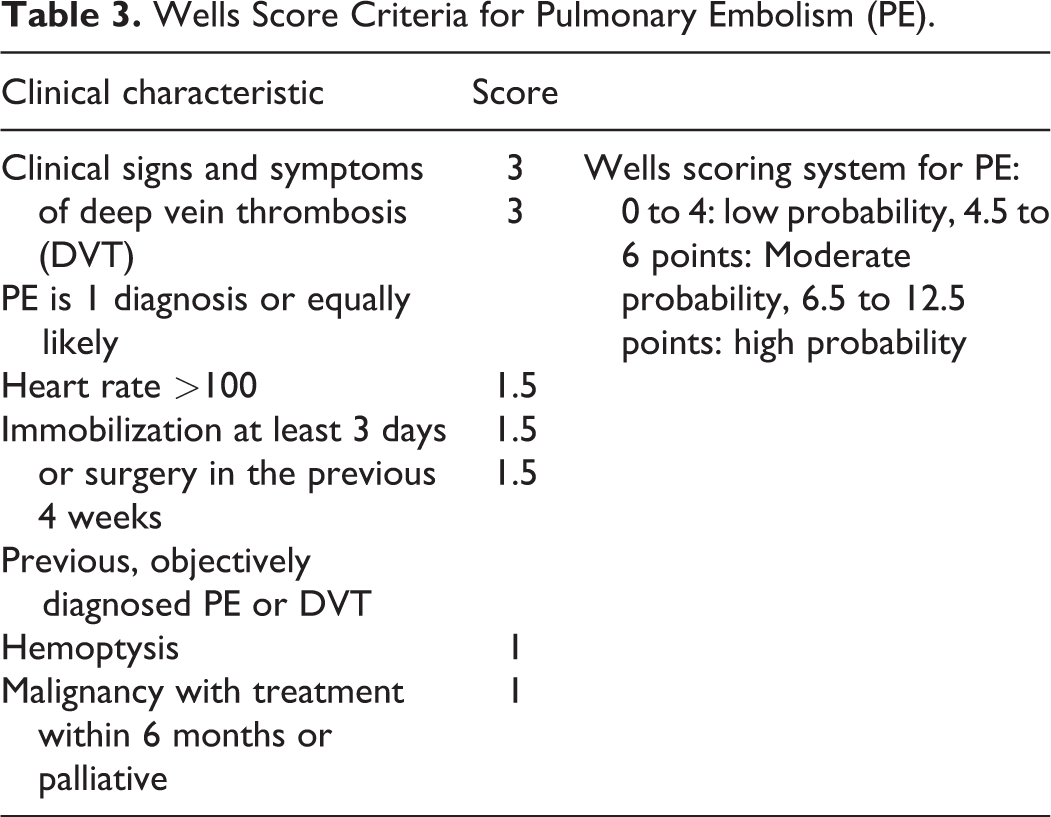
The clinical presentation and diagnosis of VTE complications postoperatively can be challenging due to vague symptomatic complaints or subtle physical exam findings. The literature stresses the importance of stratifying pretest probability for individual patients in order to determine the best imaging modality for confirmation of diagnosis. Many scoring systems have been developed for this use, including the Wells Score (Tables 2 and 3), Geneva Score, Minaiti Score, and Charlotte rule; however, the Wells Score is the most widely accepted scoring system for DVT probability. 34 The Wells Score establishes a patient as having low, intermediate, or high risk for thromboembolic events. 35
Wells Score Criteria for Deep Vein Thrombosis (DVT).
Wells Score Criteria for Pulmonary Embolism (PE).
Currently, the most common diagnostic tests for DVT is venous compression ultrasonography, which has recently replaced the more invasive contrast venography. 34 -36 This technique examines deep veins of the thigh, popliteal region and calf at approximately 2-cm intervals. 37 Studies have reported very high sensitivities and specificities for compression ultrasonography at 97% and 98%, respectively. 38 Unfortunately, however, this leaves room for overtreatment as many of the discovered DVTs are isolated and distal.
Diagnosing PEs clinically is similar to the technique used for DVTs in that scoring systems such as the Wells Score and PE rule out criteria are heavily relied on. Computed tomography (CT) pulmonary angiograms (CTPA) and V/Q scans are 2 other methods that have been used in the literature for PEs. The literature suggests that because of the low probability of PE combined with the high sensitivity of CTPA, a negative ruling eliminates the need for other testing. 39 V/Q scans were designed to replace CTPA; however, they have since become less popular as they are less available than CT. 39
D-dimer is a plasma protein produced after lysis of cross-linked fibrin by plasmin. High levels are produced at the site of thrombosis, which makes this test highly sensitive for DVTs and PEs. 40 A low D-dimer in addition to a low risk Wells Score determination should in theory be useful in ruling out the presence of DVT and PE. 41,42 It should be noted, however, that the literature describes many scenarios that can cause an elevated D-dimer, which makes this test nonspecific for DVT patients. 43 For example, Rafee et al 42 stated that both total hip arthroplasty and total knee arthroplasty, like all major surgeries, activate the fibrinolytic system, and that the elevated D-dimer in these instances cannot be differentiated from those with postoperative DVT and thus is a waste of a resource in the surgical setting.
While D-dimer is an excellent evaluative tool in certain hospitalized groups, it follows that the American Association of Orthopedic Surgeons (AAOS) has concluded that it is not a reliable screening method for DVT after surgery. 44
VTE Prevention
Through primary prevention, a multitude pharmacologic and nonpharmacologic prophylaxis methods have been accepted and are commonly used in postoperative orthopedic patients in order to prevent VTE. Preferred treatment modalities vary among clinicians and are often chosen on a case-by-case basis. The literature has not outlined the most efficacious combination of both pharmacologic and nonpharmacologic treatment options for VTE prophylaxis (Table 4). Pharmacologic options for prophylaxis include aspirin, unfractionated heparin, low-molecular-weight heparin (LMWH), vitamin K antagonists, and newer oral agents such as direct thrombin inhibitors and direct factor Xa inhibitors. Nonpharmacologic interventions include sequential compression devices (SCDs) and inferior vena cava (IVC) filters. The timing of administration of these interventions is almost as important as the intervention itself; however, research in spine-specific cases is limited. Orthopedic publications have suggested that intervention initiation between 6 and 48 hours postoperatively yields the most effective treatment with a decline in benefit after 48 hours. 45,46
Study Characteristics: VTE Prophylaxis in Spine Surgery.
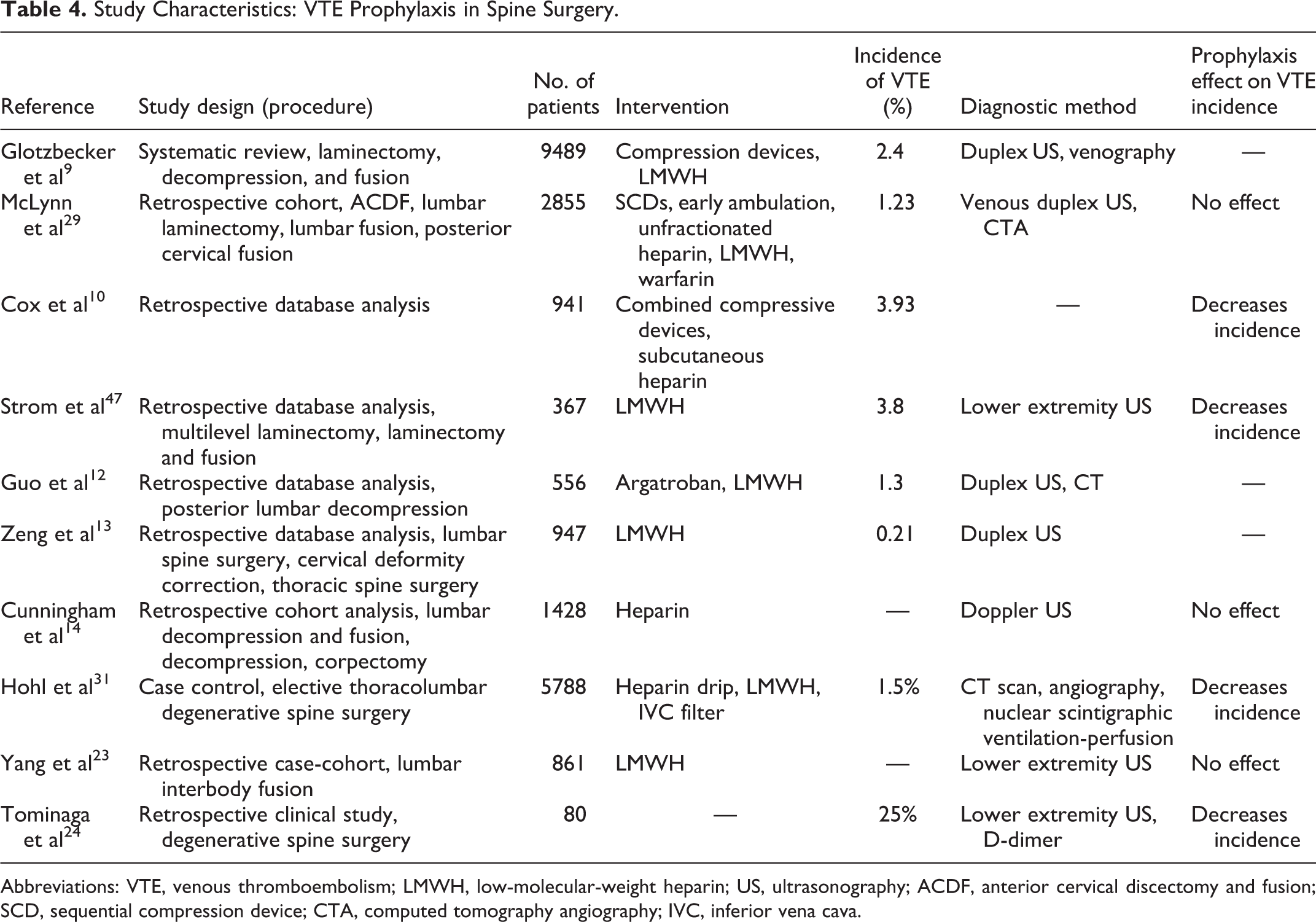
Abbreviations: VTE, venous thromboembolism; LMWH, low-molecular-weight heparin; US, ultrasonography; ACDF, anterior cervical discectomy and fusion; SCD, sequential compression device; CTA, computed tomography angiography; IVC, inferior vena cava.
Nonpharmacologic options such as mechanical compressive devices such as SCDs increase blood flow to the treated area, which in turn decreases the concentration of local coagulation factors and promotes local lymphatic drainage. 48 The draw to these mechanical modalities stems from the potential to avoid bleeding complications that result from the chemical prophylaxis mentioned above. The North American Spine Society (NASS) antithrombotic evidence-based guidelines recommends mechanical compression in the lower extremities in elective spine surgery in order to reduce complications. 49 IVC filters are endovascular devices functioning to prevent thrombi from traveling within the vasculature. Various older studies have been published demonstrating IVC filters yielding a direct reduction in VTE incidence in patients following spine surgery in concordance with chemical chemoprophylaxis making it a useful modality in prevention. 40,50 It is important to note that the most recent American College of Chest Physicians (ACCP) guidelines do not recommend a filter as primary prevention alone in patients with an increased bleeding risk. 51
The literature has thus far been inconclusive as to the best combination for preventing thromboembolic events. A 2009 systematic review by Glotzbecker et al 9 compiled data from 25 eligible articles to report on the incidence of thromboembolic disease in postoperative spine patients. Of the 9485 reported patients, they reported a DVT risk ranging from 0.3% to 31% with an overall rate of 2.1%. The study included compression devices, chemical anticoagulants, IVC filters, chemical anticoagulants, and no prophylaxis. They concluded that it is reasonable to use compression stockings as well as other compression devices to reduce the risk of DVT after spine surgery. However, because the overall risk is quite low to begin with, there is insufficient evidence to speak about the efficiency of chemical prophylaxis to reduce the risk of DVT.
Strom et al 47 published a 5-year retrospective study composed of patients undergoing both cervical and lumbar decompressive laminectomies from 2007 to 2011. The primary goal of this study was to assess the safety of LMWH when started 24 to 36 hours after degenerative spine surgery. They explained that this specific patient group was chosen because of the lack of VTE data on patients with an exposed thecal sac. Of the 367 patients included, 14 had thromboembolic complications. Comparing VTE rates of patients receiving LMWH and literature collected rates for patients receiving unfractionated heparin, this article describes LMWH as a better and more predictable prophylactic agent between the 2 and LMWH combined with mechanical prophylaxis is more effective than one alone. None of the 367 patients experienced an epidural hematoma, however, with a 0.7% hemorrhage rate, they concluded that a 24- to 36- hour delay of administration may allow sufficient hemostasis while also allowing the early prophylactic benefits. The study had an average 3-year follow-up; however, it was limited by the lack of a control group. It is for this reason that much of the literature is still inconclusive, and a prospective, controlled study is still needed.
Timing of administration has been proposed in the literature as one aspect of care that may be just as important as the method of prophylaxis itself. Cox et al 10 performed a study reporting on institutional practices for VTE prophylaxis by looking at VTE rates before and after a protocol change. They included 941 patients who underwent spine surgery in the preprotocol group. Of which, 25 had DVT, 6 had PE, and 6 had postoperative epidural hematoma. The new protocol consisted of 5000 U heparin administered subcutaneously 3 times daily, with the first dose given immediately postoperatively, compared with the old protocol of provider-dependent prophylaxis administration at least 24 hours after operation. This group included 992 patients, 10 had DVT, 5 had PE, and 4 had epidural hematoma. The reduction in DVT was found to be statistically significant allowing this group to conclude that an early aggressive utilization of heparin 5000 U in the early postoperative period after spine surgery decreases VTE incidence without increasing morbidity.
A 2019 time-to-event analyses of lower extremity VTE in lumbar spine surgery patients recorded Ultrasound findings preoperatively, and on postoperative weeks 1, 2, 4, 8, and 12. 22 Of the 1620 total patients included, 382 had a VTE. Their most notable finding was that VTE formation is the highest in the first postoperative week. The literature has reported different cutoffs for the most efficient time to intervention; however, all have mentioned that earlier prophylaxis administration leads to a decreased incidence of VTE compared with a later administration.
Prophylaxis Complications
The major risk of chemoprophylaxis unique to spine surgery is epidural hematoma and potential neurologic decline. In a comprehensive review of the literature, epidural hematoma rates in spine surgery patients range from 0.2% to 0.9% 14,52 making the choice to use anticoagulation therapy a carefully thought out decision by medical providers. Epidural hematomas present clinically as increasing pain with the potential to progress rapidly to neurological deterioration. A 2006 study 52 out of Korea reported a hematoma rate of 0.24% out of 3720 spine patients undergoing a multitude of spinal operations. They reported anticoagulation therapy as one factor that increased the risk of postoperative hematoma. It is important to mention, however, that this study included tumor patients, which could influence the epidural hematoma rate as these patients with highly vascularized tumors were more vulnerable. 52
With regard to complications associated with chemical VTE prophylaxis, McLynn et al 29 retrospectively studied 2855 patients, of whom 56.3% received heparin VTE prophylaxis and found no significant association between pharmacologic prophylaxis and incidence of VTE. They did, however, report that the incidence of postoperative bleeding was significantly greater in patients receiving prophylaxis versus no prophylaxis. 29 In total, 11 patients had postoperative bleeding or hematoma (0.4%), 10 of these patients were receiving prophylaxis (0.62%) and the remaining 1 patient was not (0.08%). Cunningham et al 14 published similar results in a 2011 retrospective cohort analysis comprised of 3870 patients that underwent elective spine surgery. A total of 1428 patients received prophylaxis in the form of 5000 U heparin. There were 103 coded hematomas; however, only 16 were identified as spinal epidural hematomas. Of the 16 cases, 7 received preoperative chemoprophylaxis and there was no significant difference in the incidence of epidural hematoma between treatment groups.
The most recent ACCP guidelines 53 for patients undergoing elective spine surgery who do not have any additional VTE risk factors discussed above, do not recommend routine use of VTE chemoprophylaxis. For patients who do have identifiable risk factors such as advanced age, history or VTE, and staged surgery, they recommend that one of the following: low-dose unfractionated heparin, LMWH, intermittent pneumatic compressions, or SCDs. They concluded that high-risk groups, including those with multiple risk factors should use a combination or chemoprophylaxis and mechanical prophylaxis; however, a specific combination was not mentioned. 53 Duration of treatment guidelines for elective spine patients specifically has not been released by the ACCP at this time.
The most recent NASS guidelines 22 recommend initiation of mechanical prophylaxis just prior to or at the beginning of elective spine surgery and continue until the patient is fully ambulatory. The guidelines state that chemical prophylaxis is safe to initiate the day of elective spine surgery and that an ideal duration has yet to be decided. AAOS is yet to release spine specific recommendations for VTE prophylaxis.
Future Directions
Invasive testing for VTE can easily be avoided using the above-described techniques. However, more research is needed to confirm a highly sensitive and highly specific test for screening. In general, more research is needed to establish procedure specific guidelines for prophylaxis in spine surgery. This may entail outlining and assessing risk factors, including demographic and surgical variables in order to develop a risk-stratification score for elective spine surgery patients. This score may help indicate which patients may or may not benefit from any form of prophylaxis. Patients with a previous history of DVT, PE, and VTE are at highest risk for a reoccurrence. In addition, more work is needed to determine the efficacy and differences among the many available prophylactic interventions. Future studies will then need to utilize a standardized regimen in order to determine efficacy in elective spine surgery patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.