
Abstract
Study Design
Retrospective case-control study.
Objectives
To evaluate postoperative outcomes of single-level cervical disc arthroplasty (CDA) in patients with osteopenia and compare these results with a matched cohort of normal bone mineral density (BMD).
Methods
Patients who had undergone single-level CDA were collected and screened. Included patients were divided into the osteopenia group and the normal group. 38 eligible patients with osteopenia were included in the final analysis. Subsequently, a 1:1 match was utilized. Clinical, radiographic data, and complications were recorded. Appropriate statistical methods were applied to conduct analysis using SPSS version 24.0.
Results
The mean follow-up time was 30.5 ± 27.3 months. The osteopenia group achieved satisfactory clinical outcomes, with no significant intergroup differences. Additionally, there were no significant differences between groups in any of the radiological parameters, either in cervical alignment or segmental height, or range of motion. The radiological incidence rate of adjacent segmental degeneration and heterotopic ossification (HO) was comparable in both groups, respectively, with a similar composition of ROM-limiting HO. However, the osteopenia group had a tendency of more implant subsidence (2.7% vs 15.2%). The logistic regression analysis showed the osteopenia group had a significantly higher incidence rate of anterior bone loss (ABL) (OR = 5.37, 95% CI: 1.50 - 19.22).
Conclusions
Single-level CDA for patients with osteopenia achieved similar satisfactory clinical outcomes compared with the normal BMD group. Meanwhile, the osteopenia group maintained adequate sagittal balance and segmental height. Based on this observation, this option may be feasible for selected patients with osteopenia.
Introduction
Cervical degenerative disease is a chronic, progressive, and age-related condition encountered in clinical practice.1,2 Cross-sectional data demonstrated that cervical spine degeneration frequently occurs among asymptomatic volunteers, with a prevalence rate of up to 80%. 3 More importantly, neck pain, the most common symptom of cervical degenerative disease, has become 1 of the most significant contributors to the global health burden. 2 Over the last 2 decades, cervical disc arthroplasty (CDA) has emerged as a viable motion-preserving option for refractory cervical degenerative disease. 4 Several prospective randomized US Investigational Device Exemption studies have repeatedly demonstrated the effectiveness and safety of CDA at the 1 or 2 levels.5-8 In addition to fewer specific complications of fusion, such as pseudarthrosis and loosened screws, CDA was proven to have substantial advantages in reducing the rate of adjacent-segment disease.6-9
Currently, the patient selection remains a topic of debate for CDA. The indications and contraindications varied in different regions. 10 However, osteoporosis was unanimously listed as an exclusion criterion in the published IDE trials for CDA.5,7,8,10 The presence of osteoporosis presents significant challenges to spine surgeons due to numerous complications associated with low bone mineral density (BMD), such as prosthesis loosening, pseudarthrosis, and graft subsidence.11,12 Nevertheless, there was a paucity of data on CDA patients with osteopenia. The extent to which BMD influences the postoperative outcomes of CDA patients remains uncertain. Notably, as the population ages, an increasing number of patients with osteopenia or osteoporosis are offered spine surgery as treatment. 13 Overall, it is estimated that osteoporosis and osteopenia affected 54% of adults over the age of 50 in the United States. 14 Previous research revealed a 29.7%-46.7% rate of osteopenia in patients aged 50 years undergoing spine surgery. 15 The number of patients who require CDA will rise, and the prevalence of osteopenia in patients with cervical degenerative disease will increase synchronously. Therefore, in the current study, CDA patients with osteopenia at our center were analyzed and compared to those with normal BMD. This is the first study to address cervical degenerative disease with varying levels of BMD treated by CDA specifically to our knowledge.
Methods
Study Population
This retrospective matched cohort study used data from consecutive patients who had undergone single-level CDA with the Prestige LP disc (Medtronic Sofamor Danek, Memphis, TN) in a single-center between 2008 and 2021 (Figure 1). A waiver of informed consent was granted to participants due to the observational nature of our study, which was approved by the local ethics committee (WCH20190946). All procedures were performed by the same senior spine surgeon. In this series, surgical indications for CDA included single-level cervical degenerative disease between C3-C7 in patients with radiculopathy and/or myelopathy that were refractory to ≥6 weeks of conservative non-operative interventions. The diagnosis of cervical degenerative disease was based on clinical features, physical examinations, and imaging outcomes. Exclusion criteria included cervical anatomical deformity, prior cervical spine surgery, segmental instability (defined by translation on flexion-extension radiographs of >3.5 mm or >20° angular motion), presence of motion <2°, ossification of the posterior longitudinal ligament, severe facet arthritis, fracture, infection, tumor, and osteoporosis. Flow-chart selection for the included participants.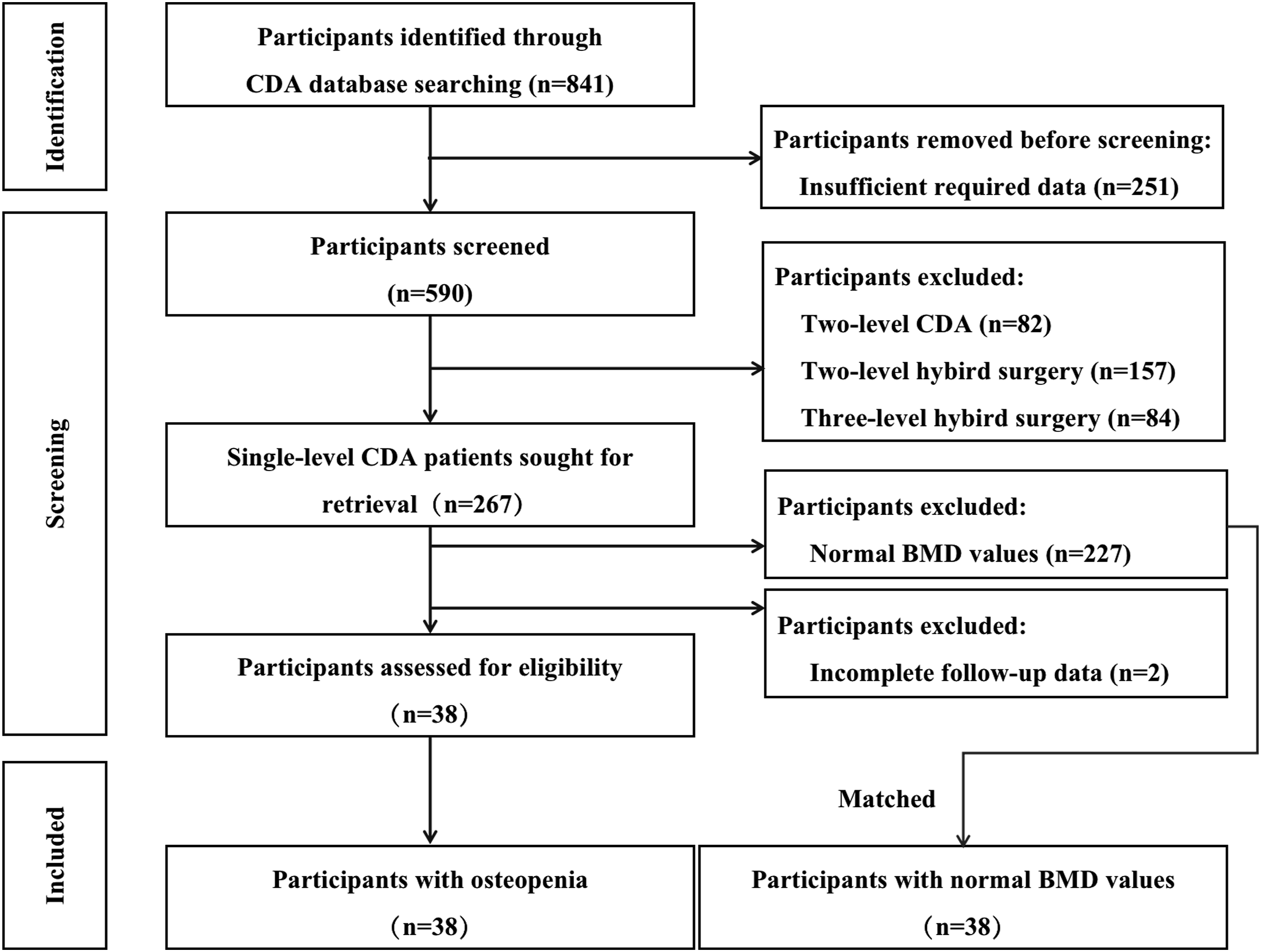
According to the World Health Organization (WHO) classification criteria, patients were classified into the normal and osteopenia groups based on the bone mineral density (BMD) T-scores on preoperative routine dual-energy X-ray absorptiometry (DEXA) scans. Specifically, the T-scores of posterior-anterior lumbar spine and femoral neck were measured in our study. Test results were based on the lower T-score of the femoral neck or L1-L5: T-score >−1 was considered normal. Osteopenia was defined as a T-score between −1.0 and −2.5 and osteoporosis as a T-score ≤−2.5. 16 In total, 15.0% (40/267) patients were classified as having osteopenia. Each patient with osteopenia was matched with a patient with normal BMD based on gender, follow-up time (±5 months), and arthroplasty level. The normal BMD group participants were sorted using a random computer-assisted generator and then selected from top to bottom to avoid selection bias.
Outcome Assessment
The clinical and radiological outcomes of preoperative, immediate postoperative, and last follow-up were retrospectively reviewed. Patient-reported scores, including the Japanese Orthopaedic Association (JOA) score for neurological function, the Neck Disability Index (NDI) for neck function, and the Visual Analog Scale (VAS) for neck and arm pain, were applied to evaluate clinical outcomes. The VAS outcome represents the mean score of both the patient’s arm and neck pain.
Radiological measurements were assessed via plain radiographs and CT scans. The parameters comprised cervical alignment, disc height, FSU height, and range of motion (ROM). Cervical alignment was assessed by using cervical lordosis, disc angle, C2-7 sagittal vertical axis (SVA), and T1 slope as described previously in the literature17-19 (Figure 2). If TS is obscured by disturbance, C7 slope was converted to a T1 slope using the formula: T1 slope = (C7 slope + .54)/0.88.
17
C2-7 ROM and segmental ROM of the index level were measured on dynamic lateral flexion/extension radiographs. The disc height was calculated as the anterior and posterior disc heights average. The anterior FSU height was defined as the distance from the highest portion of the upper end-plate of the cephalad vertebra to the lowest portion of the lower end-plate of the caudal vertebra in the anterior FSU. The posterior FSU height was measured in a similar way. Measurement techniques for cervical sagittal alignments. (Left) Cervical lordosis and C2-7 sagittal vertical axis. (Right) Disc angle of the arthroplasty level and T1 slope.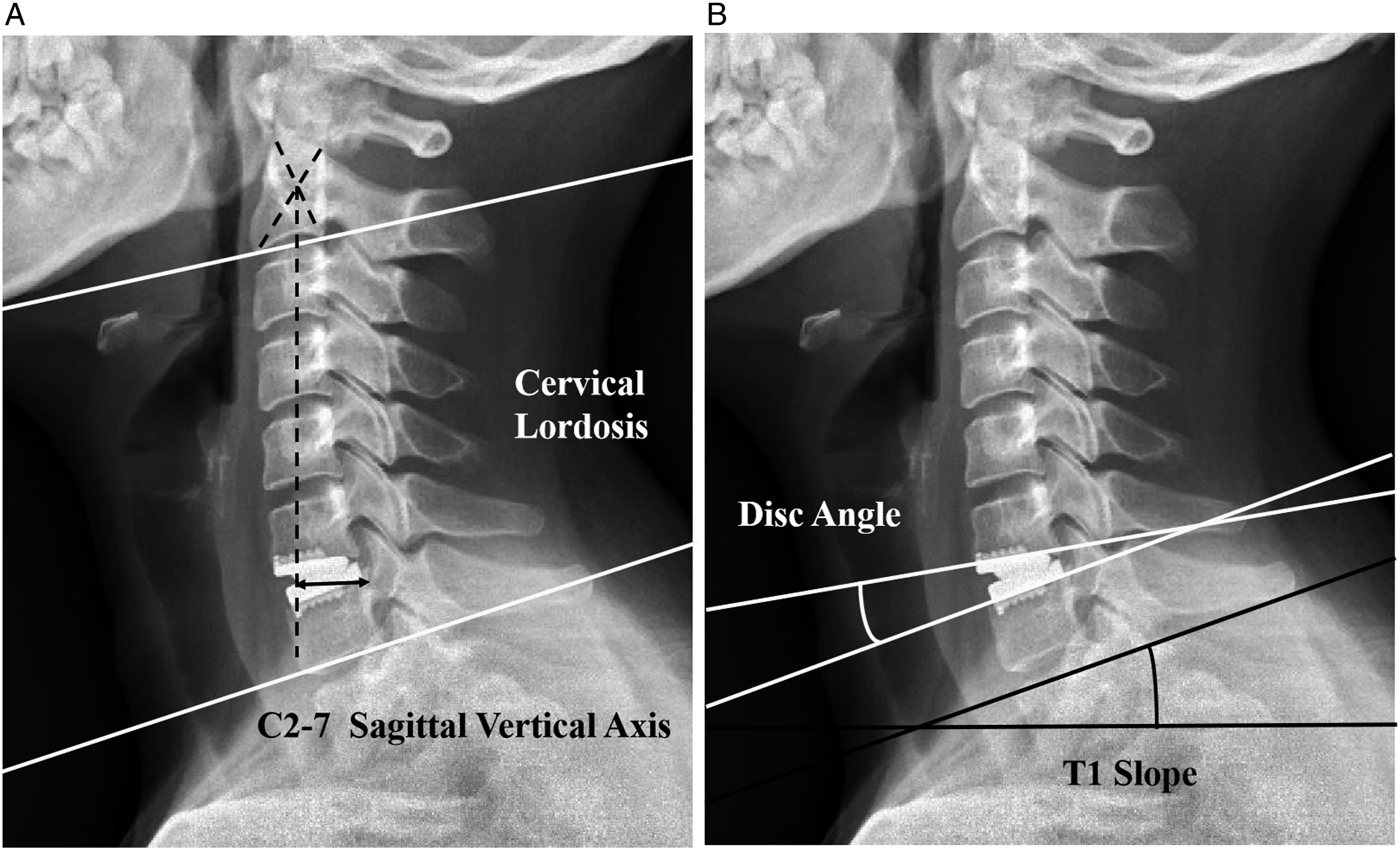
Complications
Several BMD-related complications were evaluated independently by 2 spine surgeons using a picture archiving and communication system, including implant subsidence, anterior bone loss (ABL), heterotopic ossification (HO), and adjacent segmental degeneration (ASD). Implant subsidence was defined as a reduction of >5° in the angle between the prosthetic endplate and the posterior vertebral line or a reduction of more than 2 mm in prosthesis-to-vertebral height at follow-ups.
20
ABL was defined as a combined standard of the endplate length reduction and implant subsidence at follow-ups (Figure 3).
20
It was featured as non-progressive early peri-prosthetic vertebral bone loss commencing within 6 months after surgery at the arthroplasty level. HO was identified via static and dynamic X-rays based on McAfee’s classification (Grade I-IV).
21
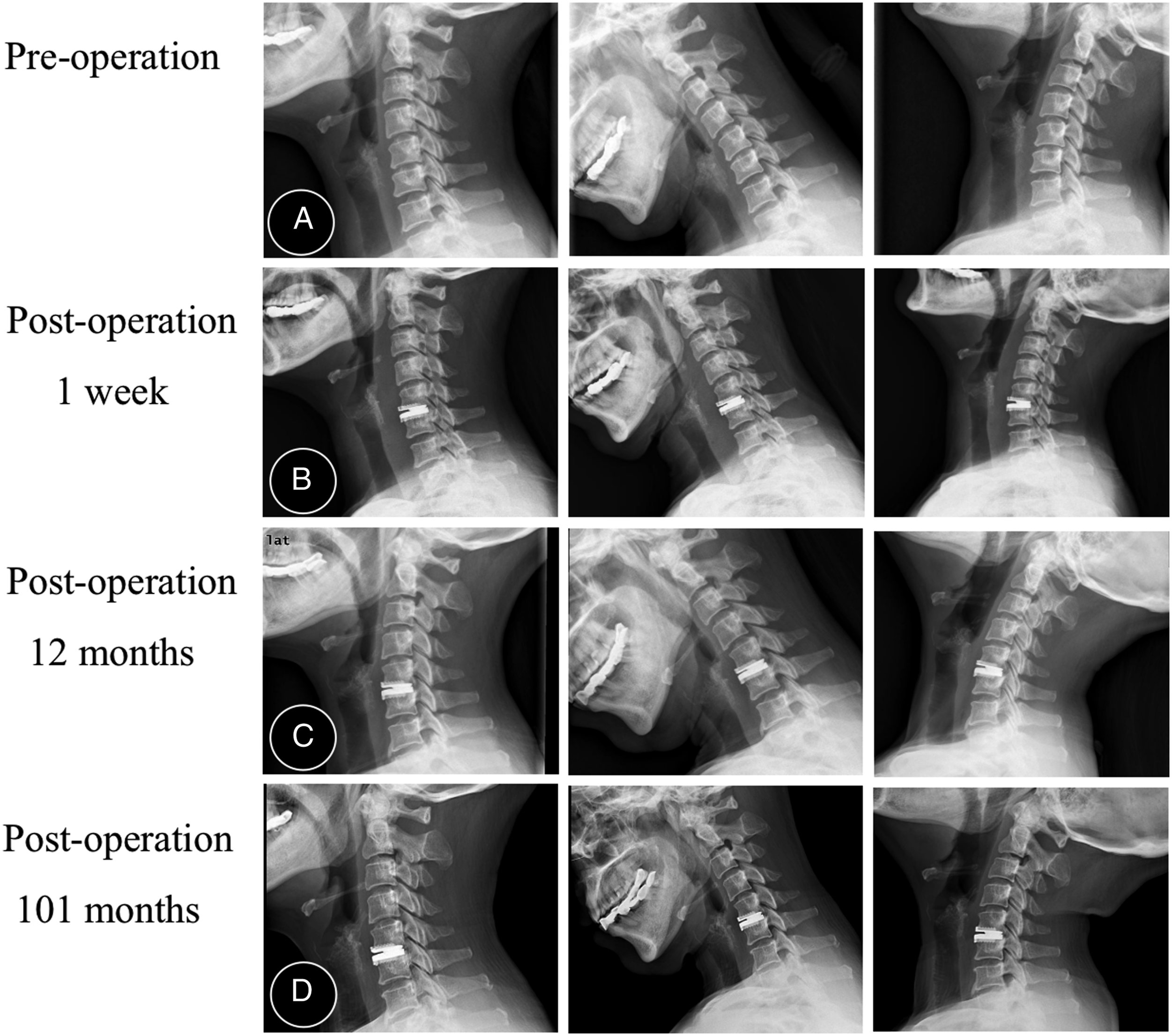
ASD was determined from radiographs using the presence of at least 1 of the following: a new anterior or an enlarging osteophyte formation, narrowing of the disc space, or an abnormal increase of segmental mobility when compared to the preoperative radiographs (Figure 4).
22
CT scans during the follow-up period were used for the final decision when ambiguity or discrepancy. The Ethics committee was fully aware of this provision and approved the study protocol, considering the potential benefits and risks involved. Measurement techniques for anterior bone loss. (A, B) Immediate and 6-month postoperative lateral radiographs: P and P′ are the length of the prostheses. A and A′ are subchondral endplate length. ABL% = (P/A)/(P′/A′)×100%. Classification of ABL: mild (ABL%≤5%), moderate (ABL% = 6%–10%), and severe (ABL% >10% with and without implant subsidence). (C) The 40-month postoperative lateral radiograph: severe ABL with implant subsidence. A typical case. A 50-year-old woman was treated with C5/6 CDA. The T value was less than −1.0 at pre-operation. (A) C5/6 shows segmental degeneration, including decreased mobility and narrowing of the disc space. (B-D) Radiographs at postoperative 1 week, 12 months, and 101 months show a disc angle of 5.5° at the arthroplasty level and no evidence of anterior bone loss, implant subsidence, or adjacent segmental degeneration.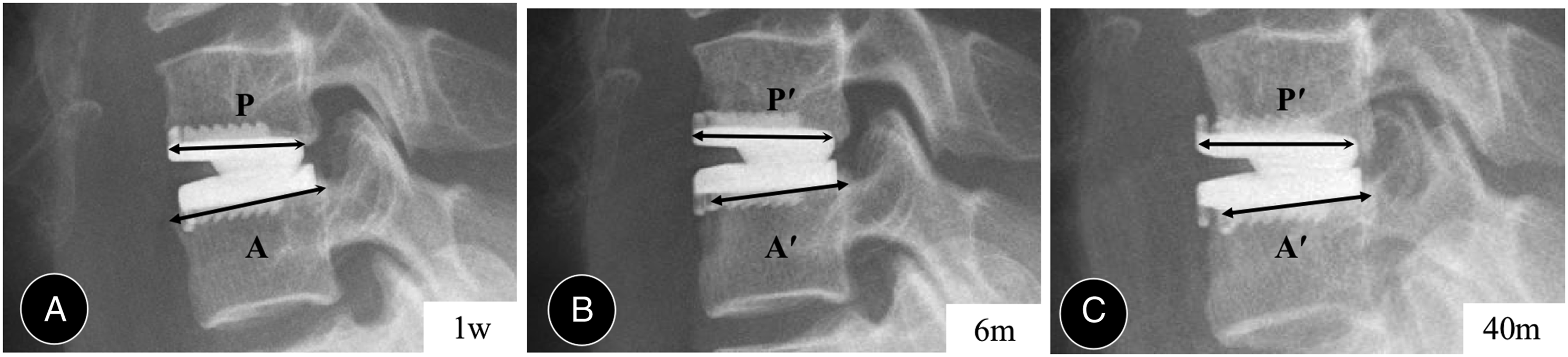
Statistics
Statistical analysis was performed using SPSS version 24.0 (SPSS, Chicago, IL, USA). Parameters were described as mean ± SD, median (interquartile range), and proportion. Fisher’s exact test and Chi-square test were applied for categorical data. Shapiro-Wilks test was used to determine normality. Comparisons of normally distributed continuous variables were made using an independent t test and Paired t test. In contrast, Mann-Whitney and Wilcoxon signed-rank tests compared non-normally distributed data. The threshold for statistical significance was set at P ˂ .05.
Results
Patient Characteristics
Baseline Demographic Characteristics.
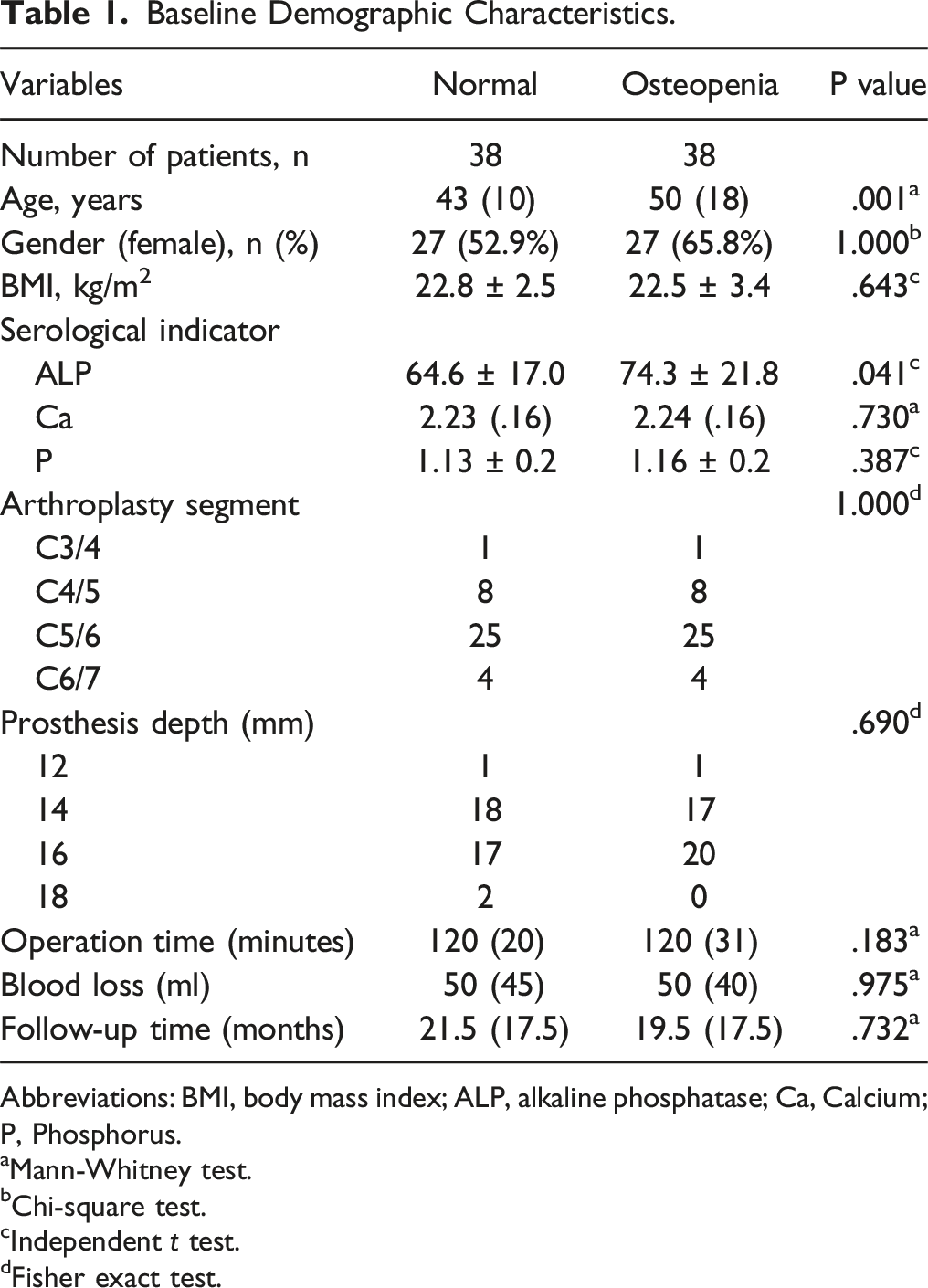
Abbreviations: BMI, body mass index; ALP, alkaline phosphatase; Ca, Calcium; P, Phosphorus.
aMann-Whitney test.
bChi-square test.
cIndependent t test.
dFisher exact test.
Clinical Outcomes
Clinical Outcomes.
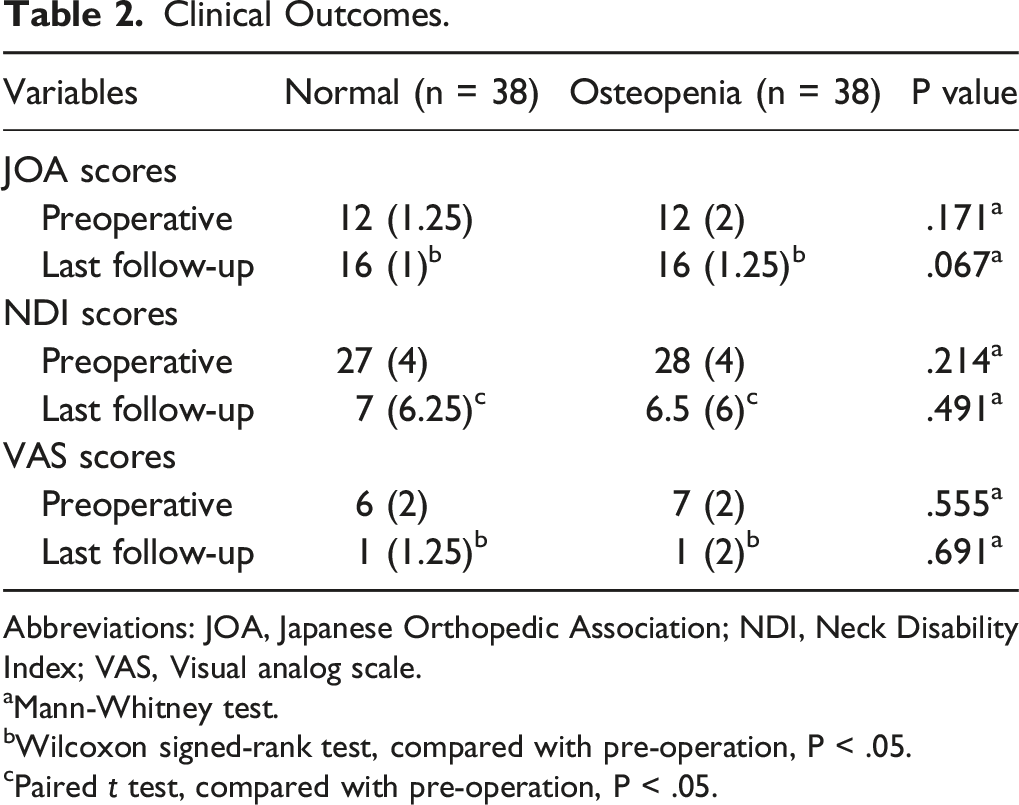
Abbreviations: JOA, Japanese Orthopedic Association; NDI, Neck Disability Index; VAS, Visual analog scale.
aMann-Whitney test.
bWilcoxon signed-rank test, compared with pre-operation, P < .05.
cPaired t test, compared with pre-operation, P < .05.
Radiological Outcomes
Radiographical Outcomes.
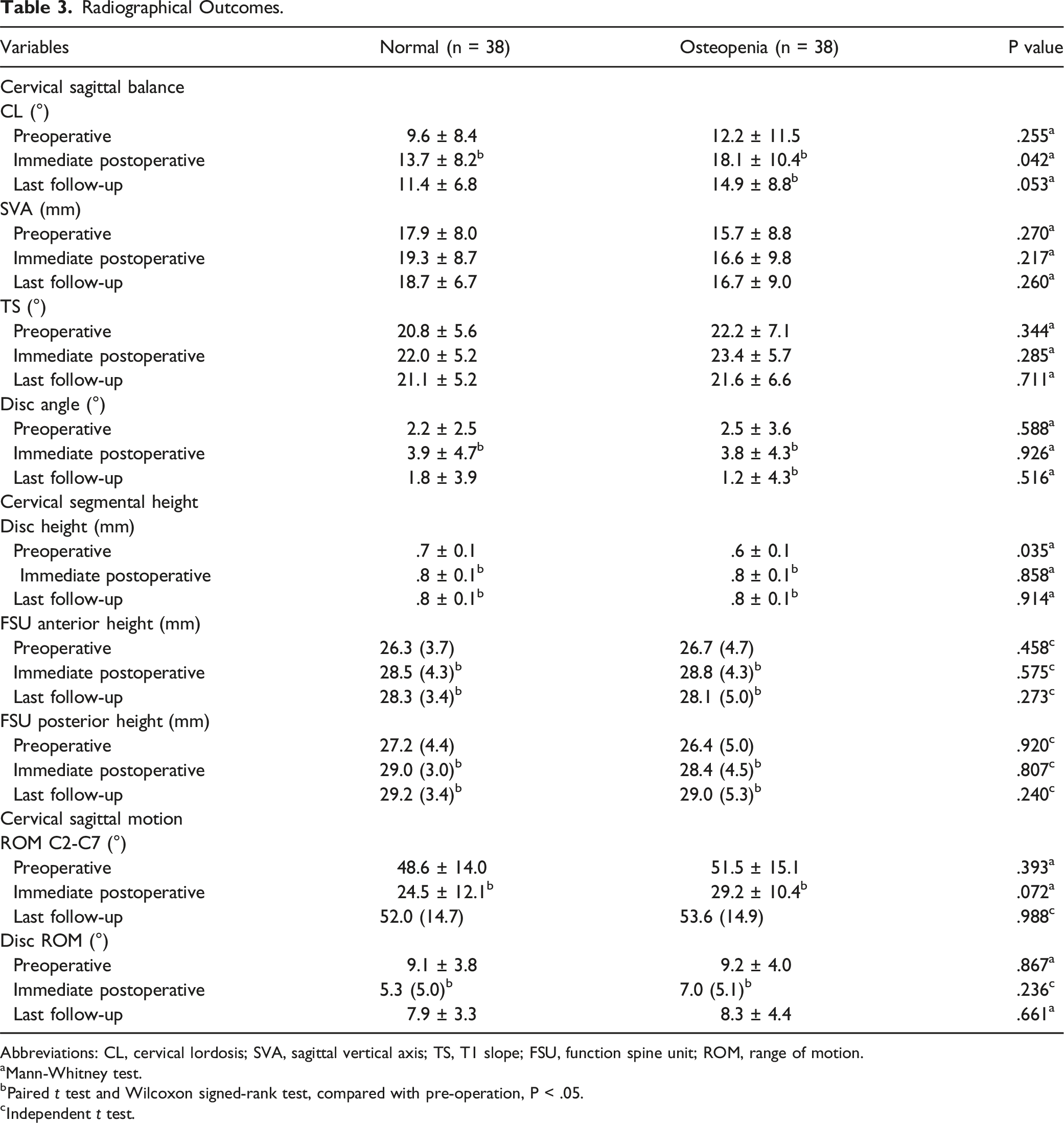
Abbreviations: CL, cervical lordosis; SVA, sagittal vertical axis; TS, T1 slope; FSU, function spine unit; ROM, range of motion.
aMann-Whitney test.
bPaired t test and Wilcoxon signed-rank test, compared with pre-operation, P < .05.
cIndependent t test.
Complications
Comparison of Postoperative BMD-Related Complications.
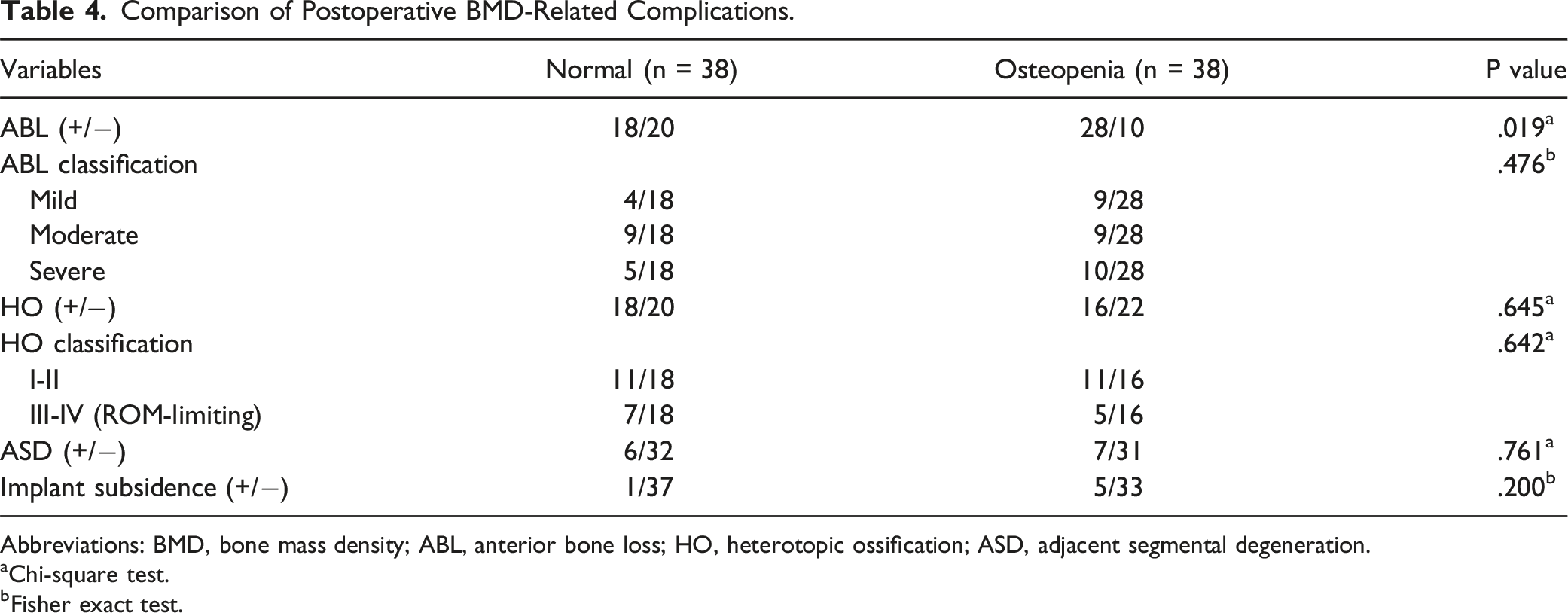
Abbreviations: BMD, bone mass density; ABL, anterior bone loss; HO, heterotopic ossification; ASD, adjacent segmental degeneration.
aChi-square test.
bFisher exact test.
Logistic Regression Analysis Outcomes for ABL.
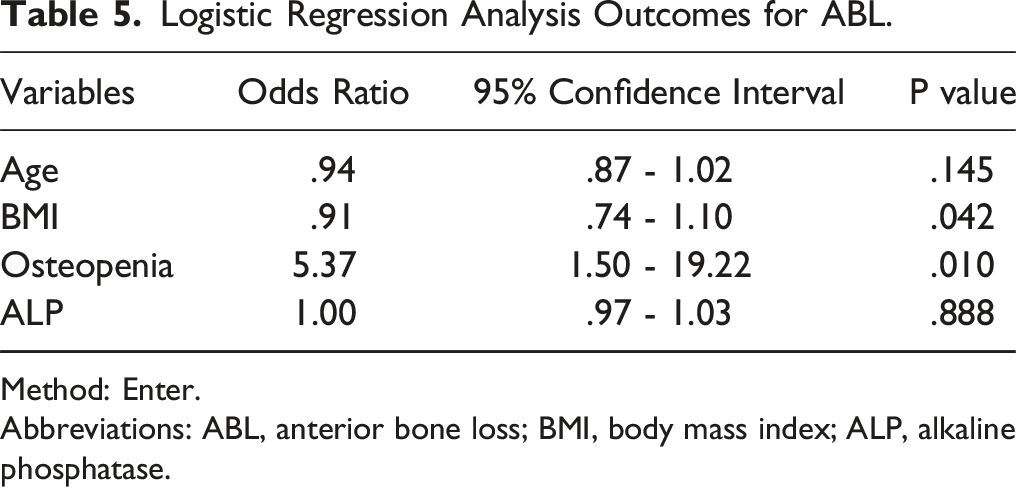
Method: Enter.
Abbreviations: ABL, anterior bone loss; BMI, body mass index; ALP, alkaline phosphatase.
Discussion
Aging populations have increased dramatically in recent decades due to advances in medicine, economies, and technology. 2 Consequently, the burden of degenerative spinal disorders, including cervical degenerative disease and osteopenia, among the elderly will increase.2,3,14,15 As a potent motion-preserving modality in the treatment of cervical degenerative disease, CDA has more limited indications, with most surgeons opposing the use of CDA in patients with osteoporosis.5,7,8 However, whether CDA should be performed on patients with osteopenia but not meet the diagnosis of osteoporosis is debatable. In a retrospective review of hybrid surgery incorporating CDA and ACDF, osteopenia was considered a general contraindication, 23 but the possibility of individual CDA for patients with osteopenia was insufficient in their study. On the contrary, Nunley et al provided a report in 3 US FDA-IDE trials of CDA that 15.4% (28/182) of enrolled patients had osteopenia comorbidities, 24 indicating that osteopenia may not be a contraindication for CDA.
In a further step, this retrospective matched cohort study of CDA, for the first time, focused on patients with osteopenia and specifically compared these patients to those with normal BMD in a 1:1 control ratio. NDI, VAS, and JOA scores improved significantly in both groups compared with the preoperative stage, without statistically significant differences. The present results demonstrated that CDA with Prestige-LP can yield satisfactory clinical outcomes irrespective of whether the patients have osteopenia, implying that BMD may not directly impact the clinical results in CDA. Our findings are consistent with previous studies that neurological improvement after CDA is primarily dependent on complete decompression and stability reconstruction of the cervical spine.1,6,9,18 Similarly, Rong et al, in their retrospective cohort study of 24 patients with osteoporosis undergoing single-level ACDF, demonstrated that the overall clinical benefit of ACDF was satisfactory in 95.8% of patients with osteoporosis at the final observation. 25
The effect of preoperative BMD on changes in cervical curvature and mobility after CDA has not been previously reported. In this study, osteopenia did not significantly alter SVA and T1 slope in CDA, and similar results were observed in ROM of C2-C7 and the arthroplasty level. In contrast, the value of disc angle in the osteopenia group at the last observation was significantly lower than the preoperative value. Surprisingly, there was a greater improvement in overall cervical lordosis in the osteopenia group compared to the normal group. This finding is more likely to be explained by the potential bias due to the sample size. Although CDA has been demonstrated to improve and maintain cervical sagittal alignment to some extent, 26 patients with preoperative kyphosis are considered poor CDA candidates.10,26 Moreover, CDA tends to develop kyphosis when the anterior column lacks support compared with ACDF. 19 Hence, fusion instead of CDA was performed in cases of kyphosis with comorbid osteopenia at our center, which may have resulted in selection bias.
Pathologically, osteoporosis and osteopenia are severe forms of decreased BMD, concomitant with deficient trabecular bone structure and reduced mechanical strength. 27 Several prior biomechanical studies have demonstrated that bone density is strongly related to the yield load and stiffness of the cervical endplate.27,28 Furthermore, in a cadaveric experimental model with CDA prostheses, Zhang et al reported a linear correlation between BMD values and endplate compressive strength, as well as endplate-related complications, including subsidence and endplate fractures. 29 Lee et al analyzed and compared the required bone-prosthesis contact area to tolerate normal physiologic load in patients with different BMD values. From their results, the inclusion of patients with a BMD T value of −2.0 to −1.5 for CDA was supported. 30 Our study obtained approximate outcomes by observing aspects of in vivo segmental height variation. Specifically, osteopenia does not affect the sustained height-maintenance functioning of the prostheses in this series, as evidenced by equivalent disc height and FSU height between patients with or without osteopenia. However, there was still an alarming rise in the incidence of subsidence in the osteopenia group. Aside from the less strength of the endplate mentioned above, another possible explanation could be differences in the occurrence of ABL. This study included it as an observation indicator owing to its correlation with the bone remodeling period within 6 months after surgery. It has been suggested that severe ABL could compromise endplate stability and consequent implant subsidence. Kieser et al reported a subsidence incidence of 66.7% in the severe ABL group, classifying the former as the most critical form of ABL. 20 Moreover, osteopenia was identified as a potential risk factor for ABL in this study. This finding was consistent with previous cadaver studies, which found bone loss always present in the anterior endplate with relatively lower bone density and strength.29,31
To date, ASD and HO are the 2 most commonly reported complications in patients treated with CDA. Although controversial, high-quality studies provided evidence that the development of ASD could be prevented by preserving segmental mobility.6-8,22,24 We found no significant relationship between ASD and osteopenia. This contrasts with the findings of Nunley et al, who showed in a prospective clinical study that osteopenia significantly increased the risk of adjacent level disease regardless of ACDF or CDA. 24 This could be attributed to the different evaluation methods of complication and the impact of fusion.5-9 On the other hand, HO was mostly found located in the posterior and lateral intervertebral disc space, right adjacent to the area of highest-level bone density. 31 A recent study also implied postoperative HO is related to individual osteogenic capacity. 32 However, HO was recorded in 42.1% of osteopenia patients and had no identified correlation with it in our study.
There are several limitations to this study that should be considered. First, in matched cohort studies, cases are matched to controls based on known confounders. 33 However, only gender, segment, and follow-up time were matched, but not the age, to provide a sufficient sample size in our study. This current limitation will guide a future multicenter study. The duration of follow-up in this study may not comprehensively capture the variation in complications, including ASD and HO. Another shortcoming that we identified is the confounding factor of postoperative osteopenia treatment. Concerning that the related drug treatment received by patients varies, it was not included and analyzed in this study. Nonetheless, numerous drugs effectively reduce mechanical complications after spine surgery, and osteoporotic patients have improved in bone microarchitecture. 34 On the contrary, while this study shows that osteopenia is not an absolute contraindication to CDA, patient selection should be done cautiously and cannot be generalized.
Conclusions
The most obvious finding to emerge from this study is that single-level CDA for patients with osteopenia achieved similar improvements in clinical parameters compared with the normal BMD group. Meanwhile, the osteopenia group maintained satisfactory sagittal balance and segmental height. However, the occurrence of postoperative ABL and implant subsidence remains a source of concern. Overall, these principal findings are reassuring. Based upon the results of this study, CDA may be feasible for selected patients with osteopenia.
Footnotes
Author Contributions
Conception and design: Junbo He, Hua Chen, and Hao Liu. Acquisition of data: Junbo He, Tingkui Wu, and Chen Ding. Analysis and interpretation of data: Hua Chen, Xin Rong, and Beiyu Wang. Drafting the article: Junbo He and Hao Liu. All authors have read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the research grants from the National Key Research and Development Program of China (2017YFA0105402), the National Natural Science Foundation of China (81902190), Department of Science and Technology of Sichuan Province (2019YFS0135), This needs to be updated to the Functionary Health Care Project of Sichuan Province (ZH2023-105), and the Science and Technology Project of The Health Planning Committee of Sichuan (21PJ039).
Ethical approval
This study was approved by our facility’s institutional review board.