
Abstract
Study Design
Retrospective cohort study.
Objectives
To compare the clinical and radiographic outcomes of Anterior Cervical Discectomy and fusion (ACDF) and cervical disc arthroplasty (CDA) in patients with preoperative segmental kyphosis.
Methods
Patients with segmental cervical kyphosis at the operative levels undergoing 1- or 2-level ACDF or CDA from 2017 to 2020 with 2 years of follow were identified. Patient demographics, perioperative data, complication rates, radiographic findings and reported outcomes were analyzed.
Results
A total of 48 patients met inclusion criteria and were included in our study (ACDF: n = 24, CDA: n = 24). Patient demographic data between the 2 cohorts was similar expect for proportion of males (ACDF: 62.5% vs CDA: 33.3%, P = .043). There was no statistical significance in the change of segmental lordosis (ACDF: +8.09° vs CDA: +5.88°, P = .075) between the preoperative and final postoperative period. Additionally, the change in cervical lordosis was similar between groups (ACDF:+ 9.86° vs CDA: +7.60°, P = .226). VAS scores were similar between the 2 groups at every follow-up interval. NDI scores were significantly different at the 6-month, 12 month and the final follow-up. Mean improvements between preoperative and final postoperative periods were statistically superior in the CDA cohort compared to the ACDF cohort (ACDF: 22.8 vs CDA: 24.1, P = .0375).
Conclusion
CDA was superior to ACDF in regards to NDI scores following index procedure in patients with preoperative segmental cervical kyphosis. Those in the CDA cohort had similar complication rates, revision rates and radiographic outcomes as those who underwent ACDF.
Introduction
Anterior cervical discectomy and fusion (ACDF) has historically been the gold standard treatment for patients with cervical degenerative disc disease (DDD) who have failed conservative measures.1,2 However, complications associated with cervical fusion, especially those related to loss of motion segments, can lead to an increased risk of postoperative morbidity. Cervical disc arthroplasty (CDA) is an increasingly popular, motion-preserving alternative to ACDF aimed at reducing some of these complications. Recent literature has demonstrated equivocal or superior patient-reported and radiographic outcomes in appropriately indicated patients receiving CDA compared to ACDF.3,4 Strict inclusion and exclusion criteria for CDA has been established by the United States Food and Drug Administration (FDA). 5 Marked cervical instability, advanced facet degeneration and severe osteoporosis are recognized absolute contraindications. However, deliberations exist regarding relative contraindications including prior cervical surgery, modest disc height loss and the presence of segmental kyphosis. 6
Segmental cervical kyphosis has been of particular debate due to important clinical implications. Several studies have demonstrated that adequate correction of sagittal misalignment improves patient satisfaction and long-term outcomes in the management of cervical DDD.7-9 Some authors have demonstrated that CDA can worsen segmental kyphosis due to asymmetric endplate milling, arbitrary placement of the prosthesis and use of an unconstrained construct.10-12 However, in a study conducted by Rong et al, 13 the investigators were able to restore cervical lordosis with CDA. Additionally, the degree of segmental lordosis was correlated with greater improvements in arm pain following surgical intervention.
There is a paucity of literature assessing clinical and radiographic outcomes in patients with segmental cervical kyphosis who have undergone ACDF or CDA, especially in the United States. However, several studies have emerged highlighting the potential efficacy of CDA in patients with preoperative kyphosis. CDA may provide these patients with potential for motion-preservation and the avoidance of postoperative complications associated with fusion. Therefore, the purpose of this study was to compare radiographic and clinical outcomes of ACDF and CDA in patients with preoperative cervical kyphosis.
Methods
Study Design
Institutional review board (IRB) approval was obtained for this study (PR# 22-006) from the St. Joseph’s University Medical Center IRB review. Informed consent was not required for this study and exemption was granted in the IRB given the retrospective nature of the study. A retrospective review at a single institution was performed of all patients who underwent either 1- or 2-level ACDF or CDA from 2017 to 2020 with a minimum follow-up of 2 years. Patients were grouped based on procedure performed. Inclusion criteria consisted of adult patients (>18 years of age), operative indication of cervical DDD causing unilateral cervical radiculopathy, either 1 or 2 cervical operative levels between C3-C7, presence of segmental kyphotic deformity (5 – 10°) and availability of complete medical records. Patients with previous cervical spine surgery, or those undergoing surgery related to trauma, malignancy, and infection were excluded. Complete medical records were reviewed including history and physical examinations, imaging studies, progress notes, operative reports, discharge summaries, office visit notes and functional outcome score questionnaires. Demographic data including age, sex, body mass index (BMI), medical history including diabetes, and tobacco use. Number of operative levels were recorded and perioperative data including estimated blood loss (EBL), operative time and length of stay (LOS) were also documented. Complications including dysphagia, dysphonia, infection, hardware failure, heterotopic ossification (HO), spontaneous fusion and ASD were noted. ASD was defined by the development of clinical radiculopathy or myelopathy correlating to a motion segment adjacent to the CDA construct with radiographic evidence of degeneration at the corresponding level. ASD was determined based on disc height at the adjacent level and anterior osteophyte formation visualized on X-ray imaging according to the classification system defined by Goffin et al. 14
Operative Procedure
All procedures were performed by 2 of 4 fellowship trained orthopedic spine surgeons, always utilizing the same technique. A standard anterior approach to the cervical spine was employed. During ACDF procedures, Caspar pin distraction, radical discectomy and decortication was employed prior to placement of plates and locking, self-tapping, self-drilling screws. During CDA procedures, Caspar pins were placed in contiguous vertebral bodies and a distractor was applied. Mobi-C (ZimVie, Westminster, Colorado, USA) or ProDisc-C (Centinel Spine, West Chester, Pennsylvania, USA) total disc replacement device was assembled on the back table and impacted within the disc space. During both procedures, the wound was thoroughly irrigated and a deep drain was placed. The fascia and skin were properly approximated with sutures. No steroids or non-steroidal anti-inflammatory drugs (NSAIDs) were routinely given to the patients following either procedure during the perioperative or postoperative periods.
Clinical Evaluation
Postoperatively, patients were followed at 2 weeks, 6 weeks, 3 months, 6 months, 1 year and annually thereafter as per standard protocol. Patient reported outcome scores including visual analog scale for neck and arm pain (VAS-neck and VAS-arm, respectively), and neck disability index (NDI) were collected at the preoperative and each postoperative office visits.
Radiographic Evaluation
AP and lateral radiographs of the cervical spine were analyzed. Segmental cervical lordosis was measured during the preoperative period, 2 weeks following surgery and at the final postoperative period. Segmental lordosis was assessed using the superior endplates of consecutive vertebrae on neutrally positioned lateral radiographs at the levels that were indicated for operative intervention. Cervical lordosis was assessed using the C7 and C2 inferior endplates on neutrally positioned lateral radiographs.
Statistical Analysis
All data was de-identified and tabulated into an Excel spreadsheet (Microsoft Corporation, Redmond, WA) for analysis. Univariate analysis was conducted to compare demographics, functional outcome scores, revision rates, complication rates, radiographic outcomes, and perioperative data between the 2 cohorts. Categorical or dichotomous variables were compared using chi-squared tests or Fisher exact tests. Continuous variables were assessed using an independent samples t test or analysis of covariance (ANCOVA). All statistical analyses were performed using SPSS version 24.0 (IBM Corp., Amonk, NY, USA). P-values less than .05 were considered statistically significant.
Results
Patient Sample
Patient Demographics and Number of Operative Levels.
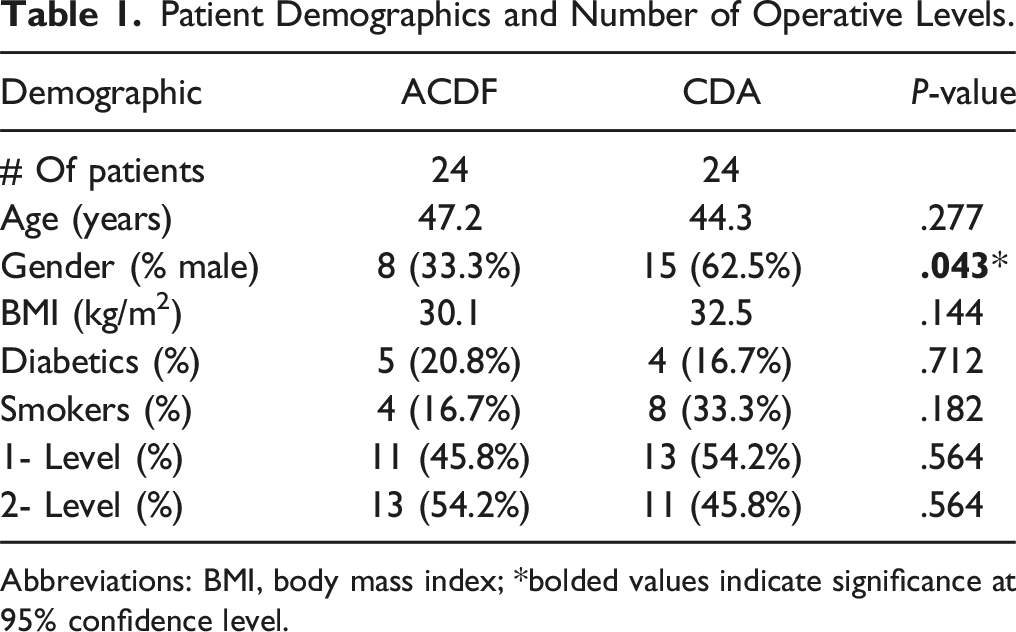
Abbreviations: BMI, body mass index; *bolded values indicate significance at 95% confidence level.
Perioperative Outcomes
Perioperative Data.
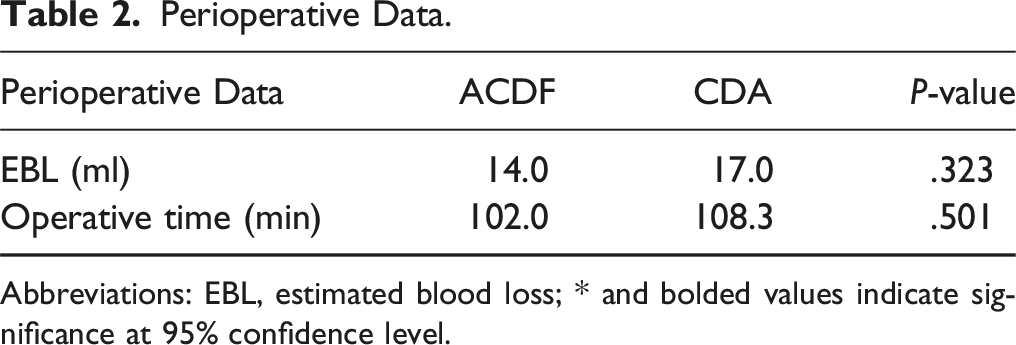
Abbreviations: EBL, estimated blood loss; * and bolded values indicate significance at 95% confidence level.
Revision Rates and Postoperative Complications
Postoperative Complications.
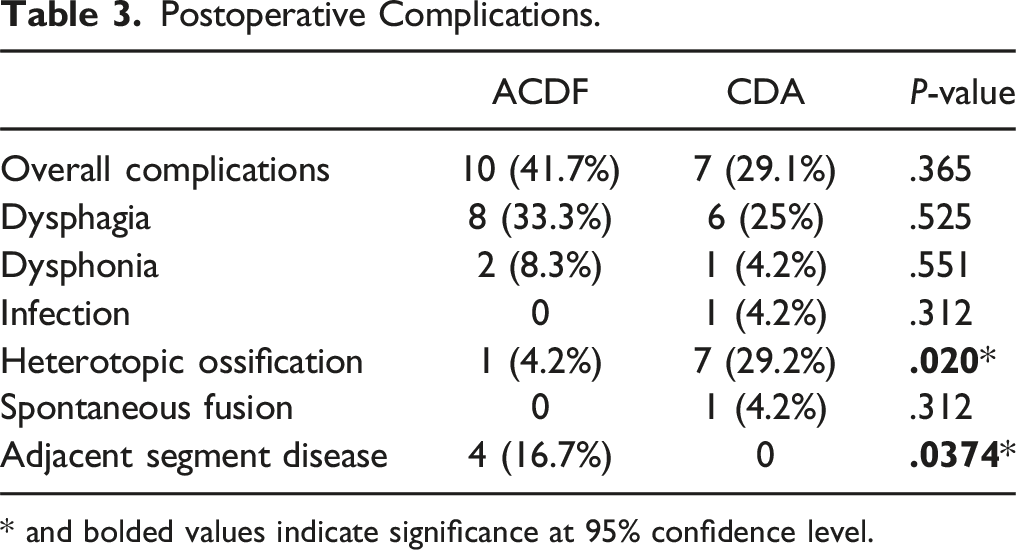
* and bolded values indicate significance at 95% confidence level.
Radiographic Outcomes
Radiographic Outcomes.
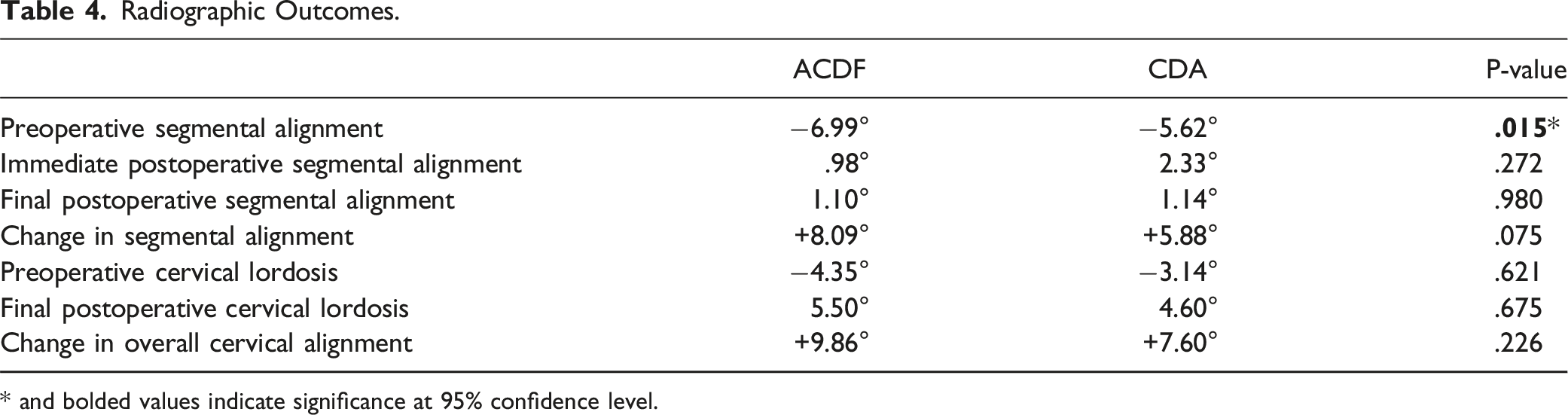
* and bolded values indicate significance at 95% confidence level.
Patient Reported Outcome Measures
Patient Reported Outcomes Measures.
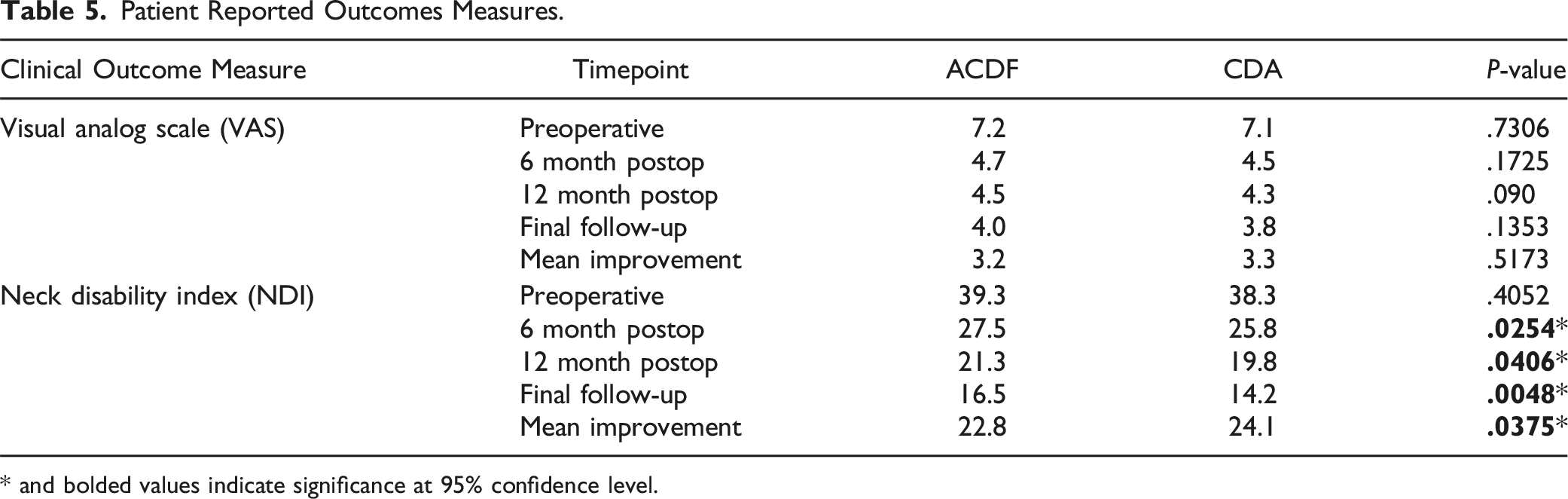
* and bolded values indicate significance at 95% confidence level.
Discussion
The use of CDA in appropriately indicated patients has continued to gain popularity as an alternative to ACDF in the United States. 15 CDA has shown to have an advantageous biomechanical profile compared to ACDF as the patients have improved range of motion and decreased stress on the implant interfaces and facet joints. 16 Fears of worsening segmental kyphosis following CDA has sparked controversy among spinal surgeons.11,12,17 Conversely, studies by Guérin et al and Wang et al showed improvements in segmental and cervical lordosis following CDA.18,19 There is a paucity of literature that directly compares clinical and radiographic findings following either ACDF or CDA in patients with preoperative segmental cervical kyphosis. In the present study, we found that patients had analogous perioperative results, complication rates and improvements in radiographic outcomes. Additionally, patients in the CDA cohort experienced greater improvements in NDI scores compared to the ACDF cohort.
There were comparable rates of complications that included dysphonia, dysphagia, infection, spontaneous fusion and hardware failure between the ACDF and CDA groups. Similarly, in a 10 year study conducted by Loidolt et al, 20 there were no significant differences in the cumulative complication rates of dysphonia, dysphagia, infections, respiratory complications, implant displacement or loosening between CDA and ACDF. In the present study, rates of HO differed significantly between the 2 cohorts. 29.2% of patients who received CDA had an occurrence of HO, which was similar to other published rates.21-23 Interestingly, Xu et al 24 found a higher incidence of HO in patients who had preoperative kyphosis compared to those with lordosis. The authors concluded that the rates of HO were higher in those with cervical kyphosis because of increased compressive stress and abnormal intervertebral motions at the kyphotic segments. Although the rates of HO following CDA are high, published reports suggest that it does not impact clinical outcomes or patient satisfaction.25,26
The presence of cervical kyphosis has several important clinical consequences. Published studies have shown cervical kyphosis can contribute to accelerated degenerative changes. Consequently, restoration of the cervical spine to a more physiological sagittal alignment is a predictor of more favorable clinical outcomes.27,28 Cervical kyphosis can contribute to the development of debilitating cervical myelopathy. Intuitively, correction of the kyphotic deformity can improve patient reported outcomes and spinal cord recovery and function. 29 Furthermore, in patients who have undergone ACDF, multiple studies have shown that uncorrected cervical kyphosis is associated with poor functional recovery, axial neck pain, narrowing of the fused neuroforamina and the propagation of symptomatic ASD.29-32
In our study, the ACDF cohort had more severe segmental cervical misalignment compared to the CDA cohort during the preoperative period. However, the change in both segmental and cervical lordosis was similar between the 2 groups at the final follow-up. Similarly, Katsuura et al conducted a systematic review comparing sagittal reconstruction of patients who underwent ACDF with plate and cage, stand-alone ACDF or CDA and found no significant differences in the change from pre-op to post-op lordosis between the 3 implant types. One of the key conclusions of this study was that CDA produced a similar sagittal profile as other cervical fusion procedures and had comparable lordosis producing properties. 31 Biomechanical studies can help explain why CDA and ACDF provide similar sagittal restoration. CDA can provide adequate intervertebral distraction mimicking the space afforded by ACDF with a cage or a native disc in a healthy control. 33 Additionally, surrounding soft tissue recruitment, C7 and T1 tilt are all major contributors to maintaining cervical sagittal vertical alignment.34,35 Changes to these parameters are generally equivocal following either ACDF or CDA.
Additionally, our results demonstrated significant differences in NDI scores between the 2 cohorts. Those who underwent CDA experienced lower disability scores and greater improvements postoperatively. These results demonstrate a divergence from a randomized control trial conducted by Chen et al. 36 In their study of 32 patients with reversible preoperative kyphosis, individuals who underwent CDA had similar clinical NDI scores as those who had an ACDF procedure. In a study conducted by Xu et al 24 that examined CDA in patients who had either reversible cervical kyphosis or lordosis, patients experienced similar benefits in NDI and VAS scores. These results suggest that the presence of preoperative segmental kyphosis does not substantially affect postoperative patient satisfaction or disability. In a randomized, prospective, multicenter clinical trial conducted by Radcliff et al, 95% of patients in the CDA cohort reported that they were “very satisfied” with their results after 7 years compared to 88% of patients in the ACDF cohort. These results become more striking in patients who were treated for 2 level disease rather than a single level. CDA demonstrated clinical superiority over ACDF that was driven by differences in disability scores, a lower incidence of subsequent surgery and neurological failures. 37
There are several limitations present in this study. This study utilized a small sample size which limited the statistical power of our results. Confounding variables were limited as there were no statistically significant differences in age, number of operative levels, BMI, smoking and diabetic status between the 2 cohorts. Furthermore, our study had a minimum follow-up period of 2 years. This time period may be inadequate to observe cumulative incidences of ASD, HO, pseudoarthrosis and hardware failure as they may present several years following the index procedure.38-42 Additionally, this may hamper our ability to establish definitive safety and efficacy comparisons between these 2 surgical interventions. Despite these limitations, this present study serves as an excellent demonstration of advancements in cervical spine surgery, particularly CDA.
Conclusion
Our study found that CDA was superior to ACDF in regards to NDI scores following index procedure in patients with preoperative segmental cervical kyphosis. Additionally, those in the CDA cohort had similar complication and revision rates as those who underwent ACDF. In comparison of radiographic evaluations, patients who underwent CDA experienced comparable improvements in segmental sagittal alignment compared to those who underwent ACDF. These findings indicate that in properly selected patients who suffer from cervical degenerative disease with segmental cervical kyphosis, CDA is may offer some clinical benefits. However, future prospective studies with longer periods of follow-up are necessary to corroborate our results.
Footnotes
Author Note
Previous Presentations: Society for Minimally Invasive Spine Surgery Annual Forum 2023.
Author Contributions
Dr Arash Emami receives grants/research support from NuVasive. Dr Ki Hwang is a consultant for Stryker Spine. None of these are applicable to the current study. For the remaining authors, none was declared.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.