
Abstract
Study Design
Retrospective Cohort.
Objectives
Most data regarding cervical disc arthroplasty (CDA) outcomes are from highly controlled clinical trials with strict inclusion/exclusion criteria. This study aimed to identify risk factors for CDA reoperation, in “real world” clinical practice using a national insurance claims database.
Methods
The PearlDiver database was queried for patients (2010-2020) who underwent a subsequent cervical procedure following a single-level CDA. Patients with less than 2 years follow-up were excluded. Primary outcome was to evaluate risk factors for reoperation. Secondary outcome was to evaluate the types of reoperations. Risk factors were compared using descriptive statistics. Multivariate regression analyses were used to ascertain the association among risk factors and reoperation.
Results
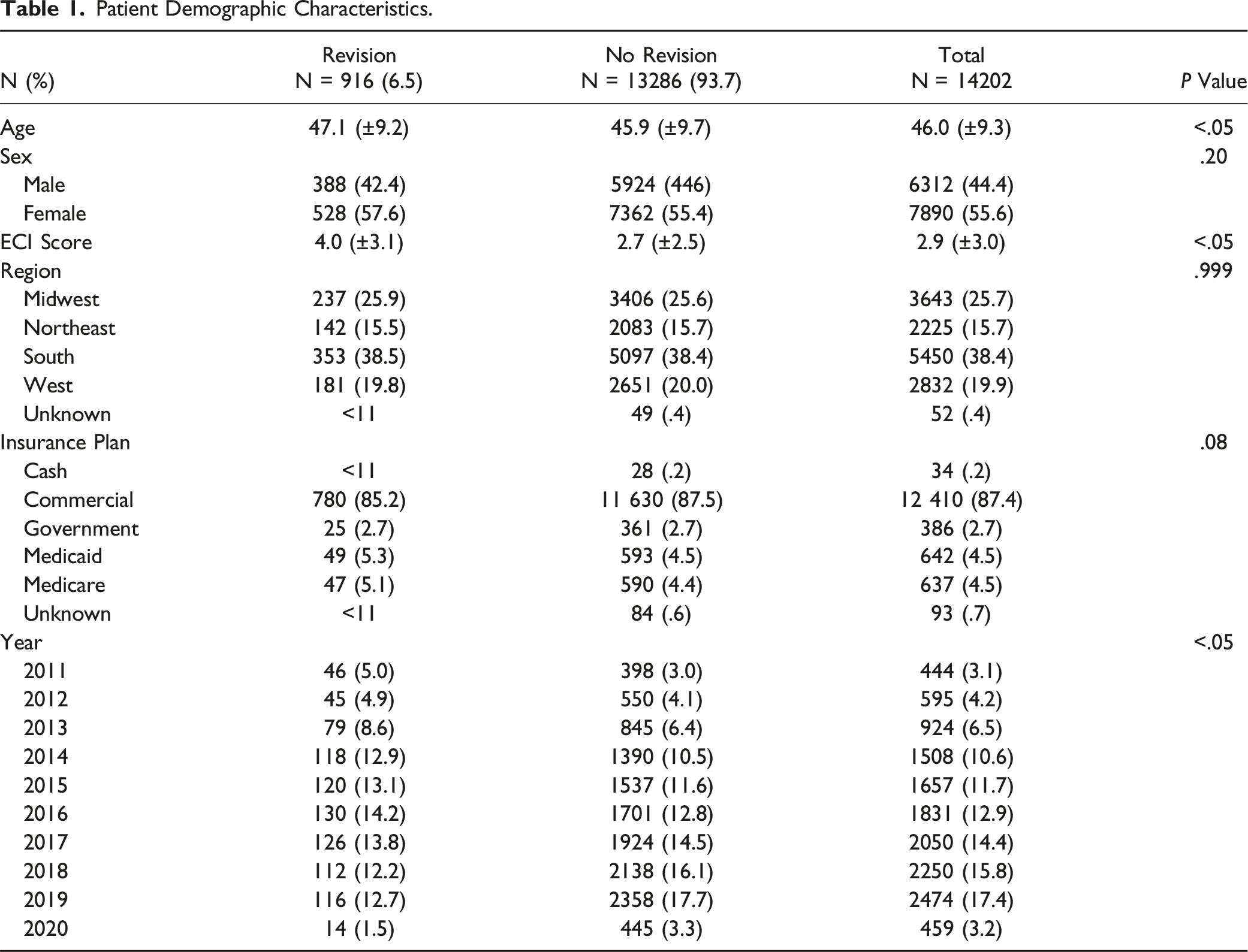
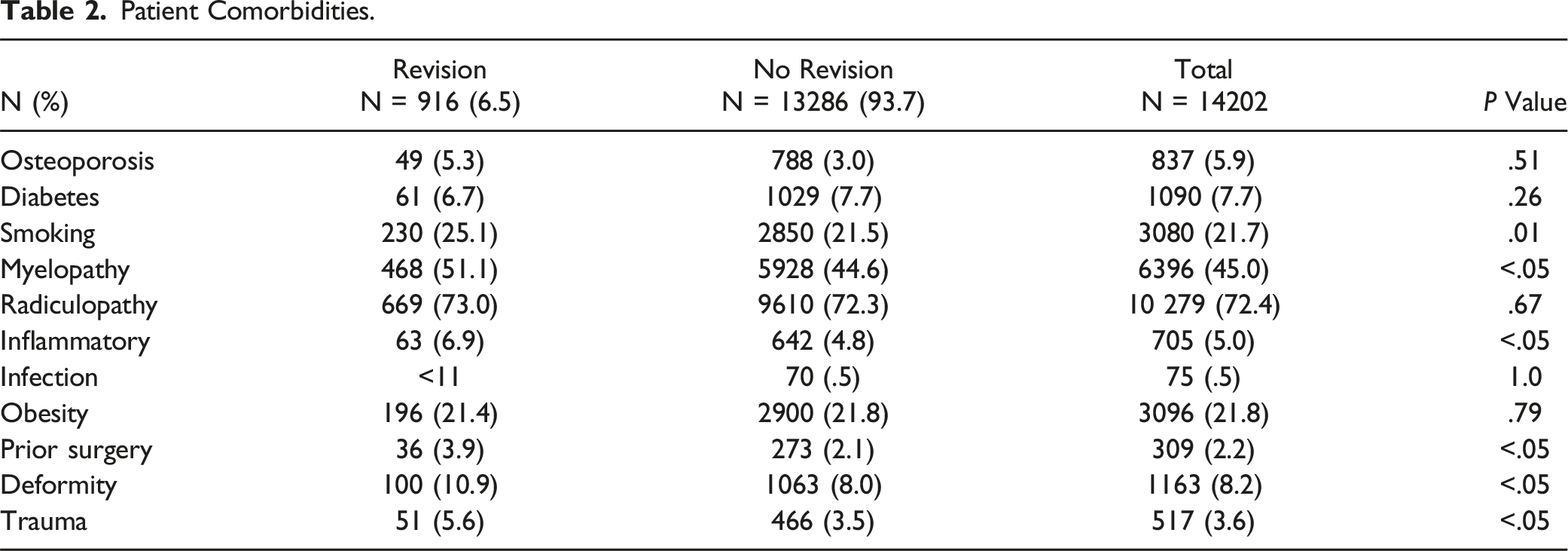
Of 14,202 patients who met inclusion criteria, 916 (6.5%) underwent reoperation. Patients undergoing reoperation were slightly older with higher Elixhauser Comorbidity Index (ECI) scores, however both were not risk factors for reoperation. Patients with diagnoses such as smoking, myelopathy, inflammatory disorders, spinal deformity, trauma, or a history of prior cervical surgery were at greater risk for reoperation. No association was found between the year of index surgery and reoperation risk. The most common reoperation procedure was cervical fusion.
Conclusions
As billed for in the United States since 2010, CDA was associated with a 6.5% reoperation rate over a mean follow-up time of 5.3 years. Smoking, myelopathy, inflammatory disorders, spinal deformity, and a history of prior cervical surgery or trauma are risk factors for reoperation following CDA. Though patients who underwent a reoperation were older, age was not found to be an independent risk factor for a subsequent procedure.
Introduction
Cervical disc arthroplasty (CDA) is a well-established surgical intervention for degenerative cervical myelopathy and radiculopathy.1,2 In contrast to anterior cervical discectomy and fusion (ACDF), which relies on the formation of a solid fusion, CDA was developed as a motion preserving procedure to mitigate the major risks associated with fusion: pseudoarthrosis, adjacent segment disease (ASD), and reduced range of motion.3–5 By mitigating these factors, CDA is thought to lower the need for subsequent procedures. 5
Currently, the literature supports equivalent or superior clinical outcomes with CDA compared to ACDF.6–11 A recent 2021 systematic review by Shin et al. reported that with a minimum 5-year follow-up, CDA reoperation rates range from 1.8% to 5.4%. 5 They further concluded that as the number of CDA procedures increases, the number needed to be revised will also likely increase. 5 With only a recent emergence of long-term data from prospective clinical trials, there still lacks a large-scale analysis of the most influential risk factors for subsequent cervical spine procedures. 12
The present study aims to fill this gap by utilizing a national database to longitudinally follow patients undergoing an index CDA and evaluate the incidence of reoperation and its associated risk factors. The scarcity of available literature and absence of treatment protocols for addressing unsuccessful CDA procedures highlight the significance of this study.
Methods
Study Design
This study utilized the PearlDiver Patient Records Database (PearlDiver Technologies Inc, Colorado Springs, CO). PearlDiver is a comprehensive medical claims database that aggregates medical data for 161 million patients across all payer types in the United States (U.S.). All providers supplying claims are required to have annual, independent, third-party audits to ensure the validity and reliability of their data. All data are deidentified and U.S. Health Insurance Portability and Accountability Act compliant. Therefore, this study was deemed exempt from review by the Cedars-Sinai Institutional Review Board.
Selection Criteria
Current Procedural Terminology (CPT) codes were used to identify the cohort for this study. All patients who underwent a single-level CDA between January 2010 and April 2022 were identified with CPT-22856. To identify an isolated single-level CDA, patients were excluded if the index surgery included an additional level code (CPT-22858), or any other posterior or anterior spine procedures performed on the same day as the index surgery (Supplemental Table 1). Patients were also excluded if they did not have continuous enrollment for two years after their index surgery.
Outcome Measures
Demographic characteristics of the study cohort were extracted from the database. Factors analyzed included: age, sex, payment method (Medicaid, Medicare, commercial, cash, unknown), U.S. region as defined by the U.S. Census Bureau (Midwest, Northeast, South, and West), and Elixhauser Comorbidity Index (ECI). The primary outcome was to assess risk factors associated with CDA reoperation. Reoperation was defined by the occurrence of any sub-axial cervical spine procedure after the index surgery. Secondary outcome was to evaluate the types of billing codes associated with reoperations that were performed following single-level CDA. Secondary surgeries were categorized as at least single-level and multi-level anterior cervical fusion, posterior decompression, removal of CDA, revision of CDA, subsequent CDA, and at least single-level posterior spinal fusion (Supplemental Table 1). Due to corpectomy procedures preceding fusions, corpectomies were grouped in the multi-level anterior cervical fusion cohort. The overall cervical spinal fusion cohort was defined as patients undergoing an ADCF, multi-level anterior cervical fusion, or single-level posterior spinal fusion.
Statistical Analysis
Statistical analyses were performed using R statistical software (The R Project for Statistical Computing) integrated within PearlDiver Bellwether software. Statistical significance was determined at a P value of <.05. Patient demographic data and clinical characteristics were compared using descriptive statistics, such as chi-squared analysis for categorical variables and student t-tests for continuous variables. A univariant analysis was used to evaluate the association of risk factors with reoperation. Variables such as female sex, ECI score, U.S. region, morbid obesity, tobacco use, osteoporosis, diabetes, myelopathy, radiculopathy, prior cervical surgery, deformity, inflammatory disorder, and trauma (Supplemental Table 1) were included in our models. A multivariable logistic regression including these variables was used to determine relative importance of each covariate. To protect patient privacy, frequencies of 10 or fewer patients in any given group are represented by “<11” in PearlDiver and in our data.
Results
Patient Demographics
Patient Demographic Characteristics.
Patient Comorbidities.
Risk Factors for Subsequent Procedure
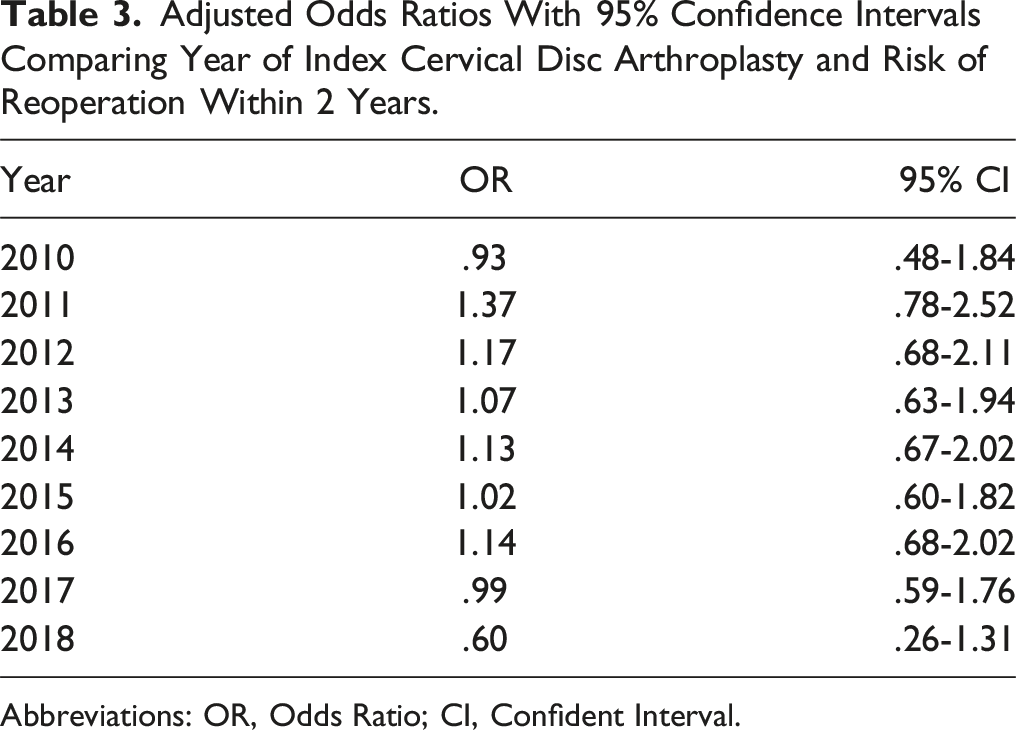
A multivariate logistic regression analysis revealed patients with a history of smoking (OR 1.20, 95% CI 1.02-1.40), myelopathy (OR 1.31, 95% CI 1.14-1.50), inflammatory disorders (OR 1.50, 95% CI: 1.13-1.96), spinal deformity (OR 1.33, 95% CI 1.06-1.65), trauma (OR 1.54, 95% CI 1.12-2.06), or prior cervical surgery (OR 1.68, 95% CI 1.15-2.38) were at greater risk for subsequent surgery (Figure 1). A preoperative diagnosis of osteoporosis, diabetes, radiculopathy, infection, or obesity was not associated with subsequent surgery (Figure 1). Similarly, patient age and ECI were not associated with additional procedures. [Insert Figure 1] Lastly, the year of index CDA surgery and risk for reoperation within 2 years was investigated via a multivariable logistic regression. Of the 547 patients identified to have a reoperation within 2 years from their index surgery, no association was found between the year the index surgery and risk of subsequent procedures (Table 3). Forest plot of odds ratios with corresponding 95% confidence intervals comparing variables and the risk for reoperation in patients undergoing single-level cervical disc arthroplasty Adjusted Odds Ratios With 95% Confidence Intervals Comparing Year of Index Cervical Disc Arthroplasty and Risk of Reoperation Within 2 Years. Abbreviations: OR, Odds Ratio; CI, Confident Interval.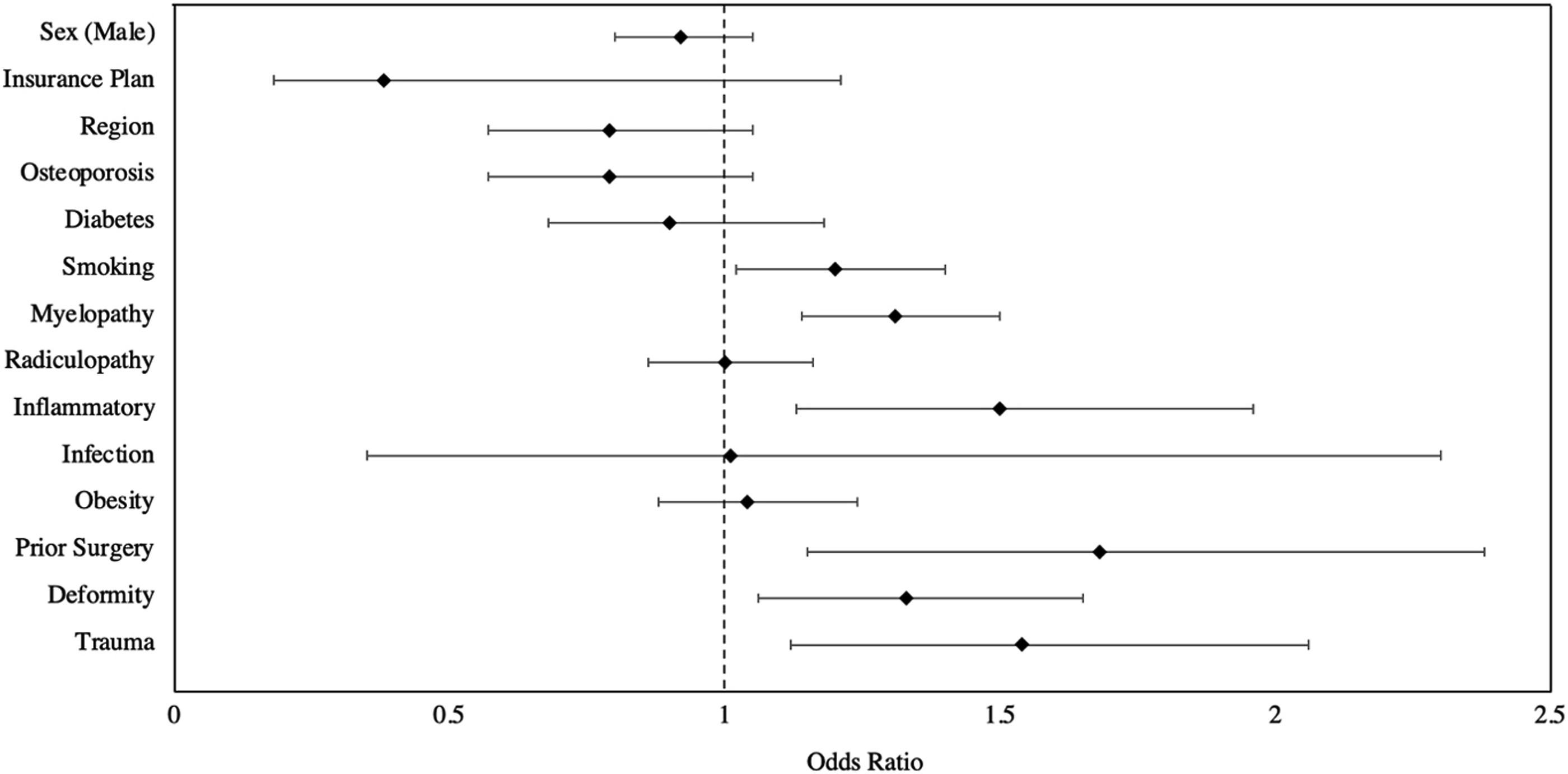
Type of Secondary Surgery Performed
Billing Code Classifications Associated With the Reoperation Procedure Following an Index Cervical Disc Arthroplasty.
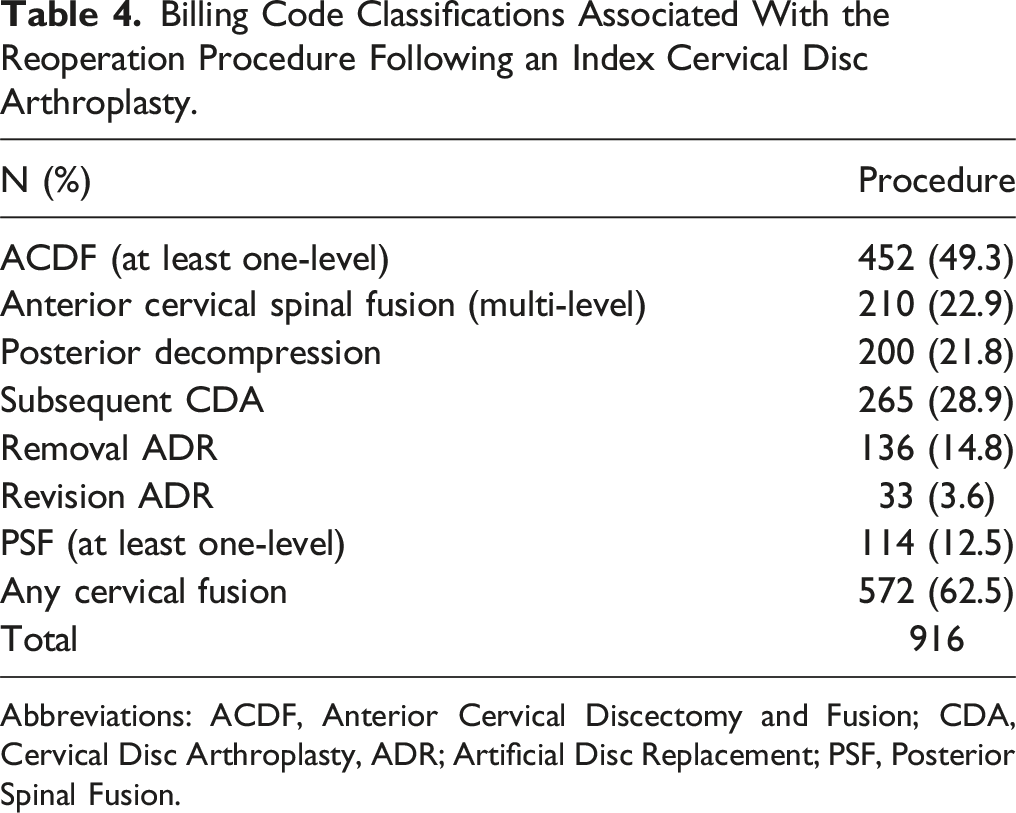
Abbreviations: ACDF, Anterior Cervical Discectomy and Fusion; CDA, Cervical Disc Arthroplasty, ADR; Artificial Disc Replacement; PSF, Posterior Spinal Fusion.
Discussion
As billed for in the United States since 2010, CDA was associated with a 6.5% reoperation rate over a mean follow-up time of 5.3 years. Smoking, myelopathy, inflammatory disorders, spinal deformity, trauma, and a history of prior cervical surgery were risk factors for another operation following index CDA. While patients who underwent subsequent procedures were older, age itself was not found to be an independent risk factor. To our knowledge, this study is the first to evaluate risk factors for reoperation in patients undergoing CDA using a national cohort with long-term follow-up.
When CDA was introduced to the market, the Food and Drug Administration (FDA) used strict inclusion and exclusion criteria derived from the Investigational Device Exemption (IDE) studies. 13 While most patients selected for CDA in the U.S. are based on the FDA criteria, there are patients who receive CDAs where the criteria are not strictly adhered to. For example, of the patients who received a CDA in our study, 5.9% contained a diagnosis code associated with osteopenia/osteoporosis, 5.0% had an inflammatory arthropathy, 2.2% had previous cervical surgery, and 4.1% were over 65 years old, all of whom may have been excluded from the original IDE trials. Likewise, Auerbach et al investigated the prevalence of indications and contraindications to CDA and found that out of 167 patients identified as requiring cervical surgery, 72 qualified. 14 With less than 50% of patients qualifying for a CDA using the current selection criteria, the question arises as to whether the strict patient selection is helping or harming patients, and if it is time to expand the indications for CDA. In our study we found that 25.4% of patients who underwent CDA carried a diagnosis code or other factor that may have excluded them from the IDE trials. This percentage is likely underrepresented given the known inaccuracies of ICD9/10 diagnostic documentation in real world practice and the lack of radiographic measures in this study.
In this study, we investigated some of the selection criteria utilized in the original IDE trials performed by the FDA and their association with reoperation. We found that patients with a preoperative diagnosis of smoking, myelopathy, inflammatory disorder, trauma, spinal deformity, or a history of prior cervical surgery were at an increased risk of needing a subsequent cervical spine procedure. Interestingly, age was not identified as an independent risk factor, suggesting that older patients may benefit from CDA as long as comorbidities are appropriately taken into consideration. It is important to note that this is a retrospective observational analysis. Patient selection bias related to which older patients a surgeon is willing to offer CDA may factor in to this result. Other studies have eluded poor outcomes to be linked to poor patient selection but have not investigated them in depth.15-17 To our knowledge, this is the first study investigating the likelihood of preoperative factors and the risk of reoperation using a large cohort.
This study’s 6.5% reoperation rate is similar to previous reports from other database studies: 5.9% in the National Inpatient Sample, 18 7.8% in the National Swedish Spine Register, 19 and 8.06% in the MarketScan database. 15 It is notable that nearly all real world observational studies find higher reoperation rates than the available data from the original IDE studies (1.8% to 5.4%).6-11,17 Since the IDE studies had extremely narrow inclusion and exclusion criteria, some have questioned how representative they are of today’s usage in a more liberally defined real-world patient sample. 20 While there is a difference in reoperation rates between IDE studies and real world observational studies, the difference is a relatively modest one. This indicates that in select clinical scenarios performing CDA outside the strict inclusion and exclusion criteria may be a reasonable option. Notably though, it is clear some of these factors effect long-term outcomes following CDA. Therefore, as more long-term data for CDA becomes available, the rate of subsequent procedures is important to consider as it carries considerable clinical and financial burden for patients.21,22
Options for secondary procedures following a failed CDA depend on the nature of the complication, the clinical picture, and radiographic imaging. 16 Due to the limited number of studies reporting long-term follow-up and overall low complication rates, there lacks data to identify and classify failures. In 2022, Zavras et al sought to create a novel system for classifying failure of CDA and identified six primary mechanisms: recurrent or persistent stenosis at operative segment (Type I), migration (Type II), instability (Type III), device motion loss (Type IV), implantation error (Type V), or prosthesis wear (Type VI). In most mechanisms described by the authors, treatment with spinal fusion was recommended with a consideration for revision CDA. 23 Similarly, Skovrlj et al proposed in cases of infection, extrusion, malposition, subsidence, or retropulsion, the best option is to remove the implant and perform a spinal fusion. 16 In this study, we found that the most common secondary procedure was spinal fusion. In the literature, spinal fusion is the most common salvage procedure, but the reported range is large.12,23 For instance, a recent systematic review by Joaquim et al in 2021 investigated 90 patients undergoing reoperation and found that 76 (84.4%) had subsequent spinal fusion. 12 On the other hand, a different systematic review by Zavras et al in 2022 found a lower rate of 44.2% (73/165), noting that 13.3% of the secondary procedures had not been specified. 23 Our finding of 62.5% falls in the middle of this range. Notably, our data, drawn from a national cohort of patients, adds a valuable perspective to the literature.
Lastly, it is important to assess whether there has been any improvement in the rate of CDA reoperation in the past decade. In this study, we compared how reoperation rates changed in patients undergoing index CDA from the years 2010-2018 with a minimum 2-year follow-up. By each year, there were no significant differences in overall reoperation rate. Our results suggest that reoperation outcomes have remained stagnant despite continued evolution of device technology and surgical technique. Therefore, it is possible that our algorithm for selecting eligible patients has not improved at the same rate. For instance, Skovrlj et al reported that the majority of complications following CDA were related to poor patient selection and surgical techniques with only a small percentage attributed to device failure. 16 Future investigations are needed to understand this at a more granular level.
This study is not without limitations. First, database research is made up of billing data, which may have some degree of misclassification of symptomatology and misrepresentations of reoperations. Second, they are limited by the amount of detail and type of information provided. For instance, there was an inability to evaluate radiographic data, operative reports, pain scores, surgeon experience, technical expertise, and indications for operation. All of which is valuable to inform the decision-making process for treatment, the indication for surgery, and reason for reoperation in individual patients. Using insurance data makes it difficult to identify causality or make direct associations. Additionally, the billing codes used in this study do not provide information on the spinal level where the surgery was performed. This limits the ability to investigate index vs adjacent segment pathology. Lastly, although the PearlDiver database includes large data with all payer types, it is not inclusive of all major insurance companies in the U.S., which each have their own beneficiary from different socioeconomic levels and regions. For example, our cohort geographically overrepresented the South with over 38% of the cases studied. Nonetheless, our research offers valuable prognostic and treatment-related insights applicable to the real-world patient population in the U.S. Most importantly, our results serve as a starting point for hypotheses generation and enables researchers to design prospective, multi-center studies to generate more definitive answers.
Conclusions
As used in United States clinical practice, with a mean follow up of 5.28 years, CDA was associated with a 6.5% reoperation rate. Smoking, myelopathy, inflammatory disorders, spinal deformity, trauma, and a history of prior cervical surgery were risk factors for reoperation following index CDA. While patients who underwent a reoperation were older, age was not found to be an independent risk factor for subsequent surgery. To our knowledge, our study is the first to evaluate risk factors for reoperation in patients undergoing CDA using a large national cohort with long-term follow-up. The lack of literature investigating risk factors for subsequent surgery makes this an important topic for consideration.
Supplemental Material
Supplemental material - Risk Factors for Reoperation Following Single-Level Cervical Disc Arthroplasty as Utilized in a Representative Sample of United States Clinical Practice: A Retrospective PearlDiver Study
Supplemental material for Risk Factors for Reoperation Following Single-Level Cervical Disc Arthroplasty as Utilized in a Representative Sample of United States Clinical Practice: A Retrospective PearlDiver Study by Paal K. Nilssen, Nakul Narendran, Ida Chen, Linda E Kanim, Corey T Walker, Hyun W Bae, David L. Skagg, and Alexander Tuchman in Global Spine Journal.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.