
Abstract
Study Design
Observational study.
Objective
To analyze the cervical sagittal parameters for standing Digital radiography (DR) and supine Magnetic resonance imaging (MRI), and to further clarify the relationship between odontoid incidence (OI) and cervical spondylotic myelopathy (CSM).
Methods
52 CSM patients aged 54.46 ± 2.89 years underwent both standing DR and supine MRI scans of cervical spine between November 2021 and November 2022. OI, odontoid tilt (OT), C2 slope (C2S), T1 slope (T1S), C0-2 angle, C2-7 angle (cervical lordosis [CL]), and T1S-CL were measured in both DR and MRI images using Surgimap (Version 2.3.2.1). Pearson correlation and linear regression were used to compare these parameters between the two modalities.
Results
Cervical sagittal parameters, including OI, OT, C2S, C0-2 angle, T1S, C2-7 angle (CL) and T1S-CL, showed no significant differences in the measurements between the two modalities. Based on the DR images, OI was related to OT (r = .386, P < .01), C2S (r = .505, P < .01), CL (r = -.412, P < .01), and T1S-CL (r = .320, P < .05), and OI was matched with CL (r2 = .170) and T1S-CL (r2 = .102). Based on MRI images, OI was related to OT (r = .433, P < .01), C2S (r = .516, P < .01), CL (r = -.355, P < .01), and T1S-CL (r = .271, P < .05), and OI matched with C2-7 (r2 = .126) and T1S-CL (r2 = .073).
Conclusion
OI is an independent parameter related to cervical anatomy and its measurement is unaffected by external factors. In patients with CSM, odontoid parameters may effectively describe the sagittal alignment of the cervical spine on DR and MRI images.
Introduction
Cervical spine parameters are essential tools for investigating the sagittal alignment of the cervical spine. Reliable, simple, and repeatable cervical spine parameters are helpful for surgeons to evaluate the clinical manifestations of cervical spondylosis, formulate a surgical plan, and predict the postoperative healing effect. 1 Over the past decade, various new cervical parameters have been investigated. T1 slope (T1S), 2 C2-7 angle (cervical lordosis, CL), 3 C2 slope (C2S), 4 C0-C2 angle, 5 and C2-C7 cervical sagittal vertical axis (cSVA) are key parameters for evaluating the sagittal balance of the cervical spine.6,7 This is of great importance for selecting surgical methods in patients with cervical spondylotic myelopathy (CSM) and evaluating sagittal balance of the cervical spine after surgery. 8 However, these parameters are flawed because they are not constant anatomical parameters, and the measured values may have significant errors. Therefore, discovering new independent and constant anatomical parameters in the cervical spine is crucial for the in-depth evaluation of cervical spine alignment.
Lee et al. proposed a new cervical parameter, odontoid incidence (OI). 9 This is an independent anatomical parameter obtained by measuring the internal angle of the odontoid process, which is not influenced by external factors. 9 Simultaneously, it can be displayed completely and clearly on digital radiography (DR) images. More importantly, OI is significantly correlated with health-related quality of life (HRQoL), 10 a parameter of great clinical importance.
Currently, research on odontoid process parameters is limited to normal controls and DR images and has not been applied to CSM patients and magnetic resonance imaging (MRI) images. This study aimed to evaluate whether OI can be applied to MRI images and the significance of OI in patients with CSM by reviewing standing DR and supine MRI images. Furthermore, we analyzed the relationship between odontoid process parameters and other cervical spine parameters.
Materials and Methods
Patient Exclusion Criteria
This study was approved by the Ethics Committee of the First Affiliated Hospital of Guangxi Medical University (2023-E008-01). The imaging data of patients with CSM treated at our hospital between November 2021 and November 2022 were retrospectively analyzed. The inclusion criteria include: (1) the patient with the symptoms, signs, and underwent imaging examination of cervical spondylotic myelopathy. (2) complete and clear standing DR and supine MRI images of the cervical spine. Exclusion criteria include: (1) patients with DR and MRI imaging intervals greater than 2 months were excluded to avoid bias caused by disease progression; (2) patients with a history of cervical surgery and trauma were excluded; and (3) patients with systemic diseases, including a history of infection, history of tuberculosis, combined tumor, and ankylosing spondylitis were excluded to avoid interference with objective measurement. According to these criteria, 52 eligible patients were selected with a male-to-female ratio of 1:1.
Radiographs of the cervical spine were taken in a standing position, with the upper limb suspended in a neutral position, naturally at the side of the trunk, and eyes looking straight ahead. The center of the projection is at the C4-C5 level, and the projection area includes the upper orbit to the thoracic vertebra. Cervical MRI was performed with the patient in a neutral supine position, and the neck was scanned using 1.5 T magnetic resonance tomography. Cervical spine parameters were measured using T2-weighted imaging.
Parameter Measurement
OI is defined as the mid vertical angle line of the endplate below C2 and the line from the midpoint of the endplate below C2 to the center of the odontoid (the center of the odontoid is the center of a circle tangential to the anterior and posterior boundaries and the vertex of the odontoid).
9
Odontoid tilt (OT) is defined as the angle generated from the line and vertical axis from the midpoint of the endplate below C2 to the center of the odontoid (Figure 1).
9
Measurement of odontoid process parameters. A: Schematic diagram of the parameters of the odontoid process parameters; B: Measurement of OI and OT on DR images of a 56-year-old female patient; C: Measurement of OI and OT on MRI images of a 56-year-old female patient. The red and green corners are OI and OT, respectively.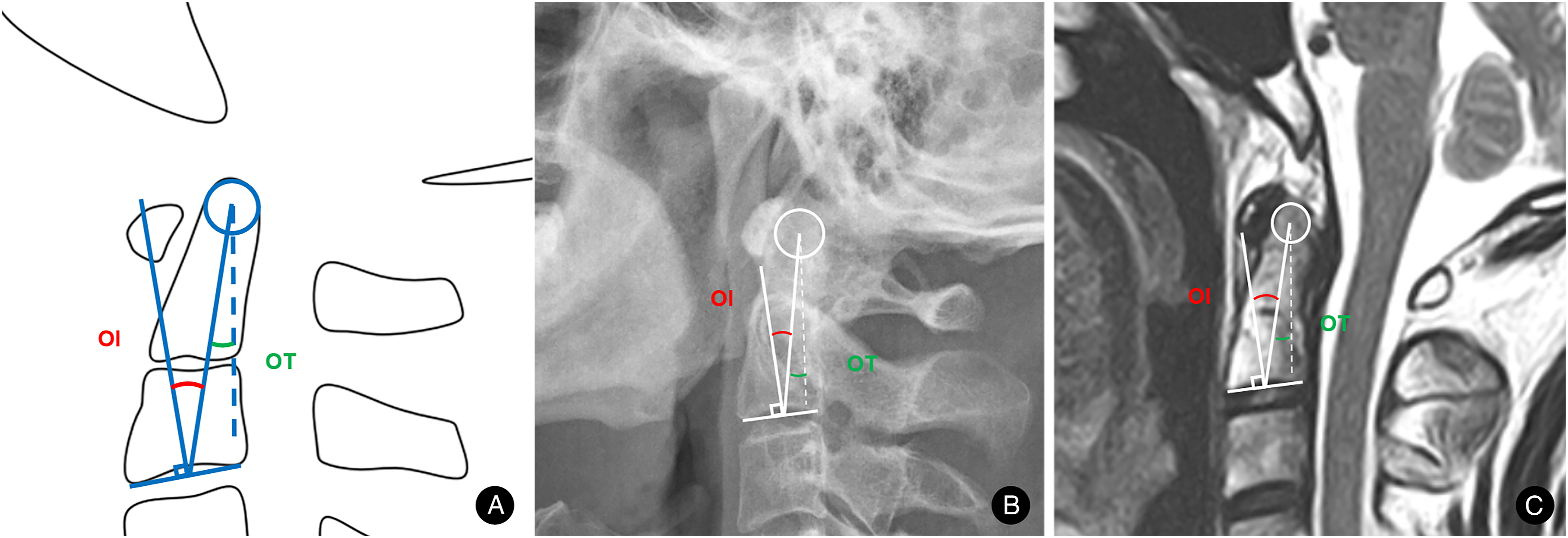
C2S was defined as the angle between the C2 endplate and the horizontal line. C0-2 angle is the angle between the lower endplate C2 and McRae line. C2-3 angle is the angle between the lower endplate C2 and the lower endplate line C3. Similarly, C2-4 angle, C2-5 angle, C2-6 angle, and C2-7 angle are the included angles between the C2 lower endplate and the corresponding vertebral endplate line. The C2-7 angle is also called CL. T1S is the angle between the upper endplate of T1 and the horizontal plane line (Figure 2). Measurement of cervical spine parameters. A: Schematic diagram of the cervical spine parameters; B: Measurement of cervical spine parameters on DR images of a 56-year-old female patient. C: Measurement of cervical spine parameters on MRI images of a 56-year-old patient.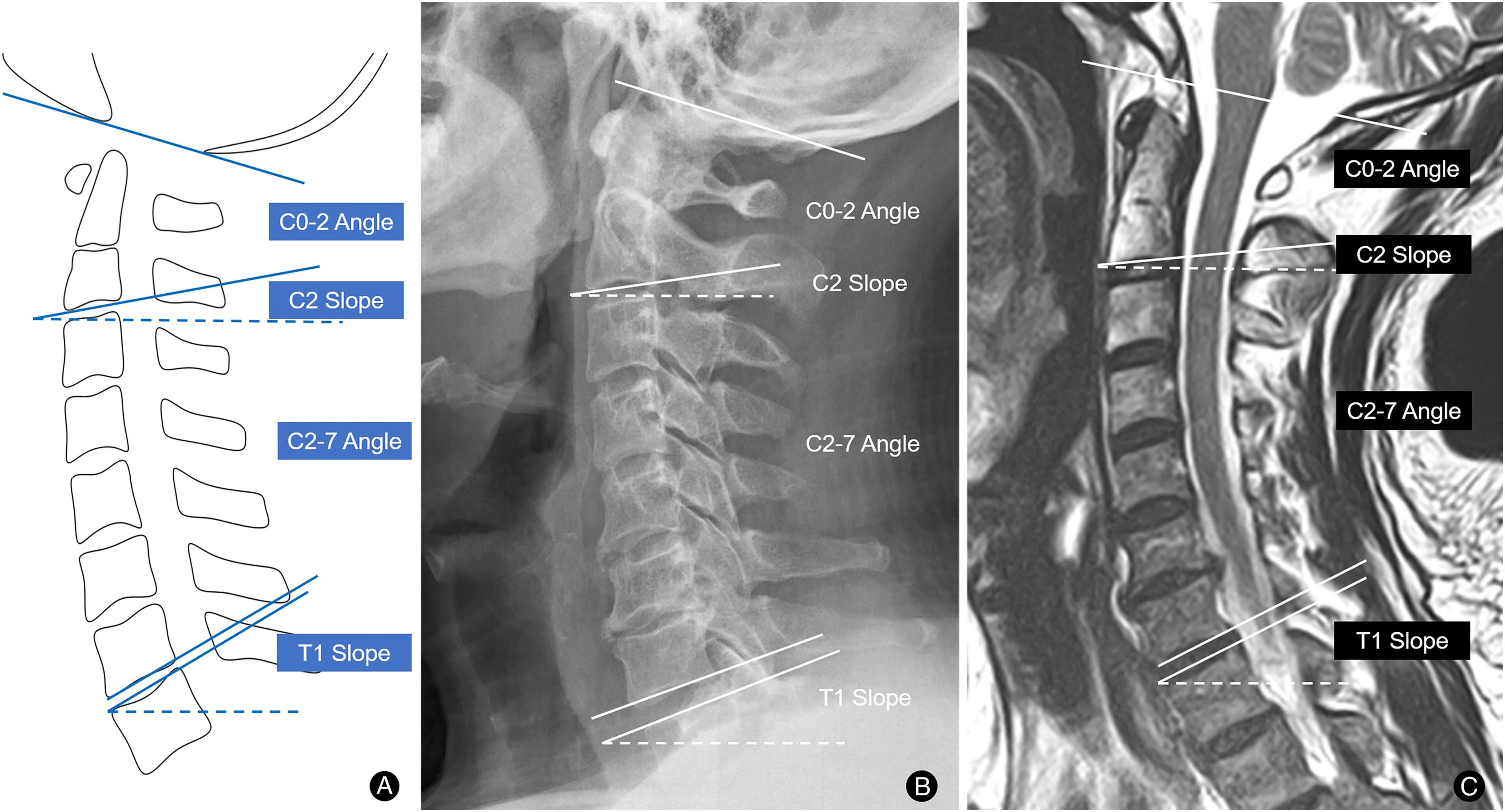
Statistical Analysis
The professional spine measurement software Surgimap (version 2.3.2.1; Nemaris, Inc.) was used to measure the spinal parameters of the CSM patients. SPSS (version 26.0; SPSS, Inc.) was used for the statistical analysis. The paired sample T test was used to analyze the statistical differences between the DR and MRI measurement data. Pearson’s correlation and linear regression were used to analyze correlations among the parameters. Statistical significance was set at P < .05.
Result
Mean cervical parameters of CSM patients.
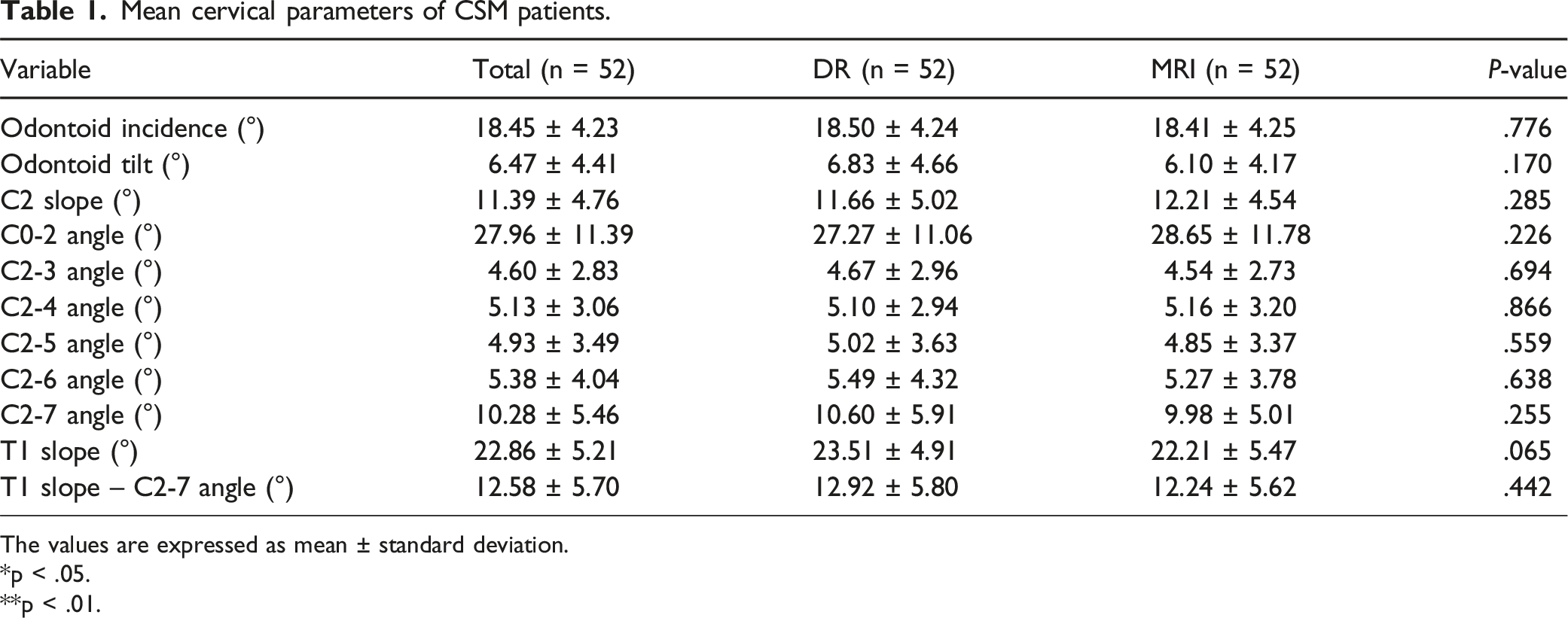
The values are expressed as mean ± standard deviation.
*p < .05.
**p < .01.
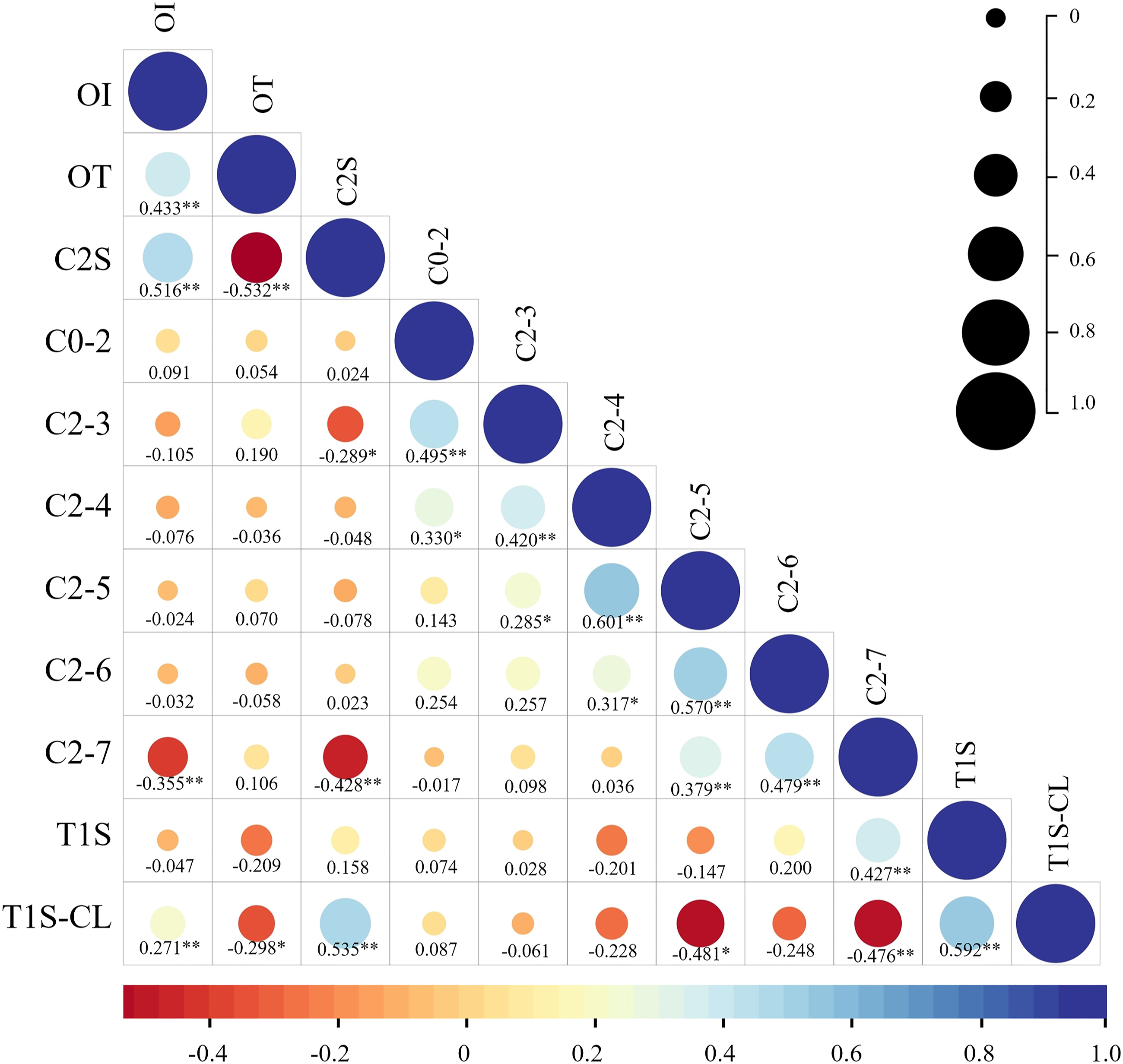
Based on the DR images, OI was significantly correlated with OT (r = .386, P < .01), C2S (r = .505, P < .01), CL (r = −.412, P < .01), and T1S-CL (r = .320, P < .05). OT was significantly correlated with C2S (r = −.616, P < .01) (Figure 3). Based on MRI images, OI was significantly correlated with OT (r = .433, P < .01), C2S (r = .516, P < .01), CL (r = −.355, P < .01), and T1S-CL (r = .271, P < .05). OT was significantly correlated with C2S (r = −.532, P < .01) and T1S-CL (r = −.298, P < .05) (Figure 4). Pearson correlation analysis between OI, OT and cervical parameters on cervical DR images. Pearson correlation analysis between OI, OT and cervical parameters on cervical MRI images.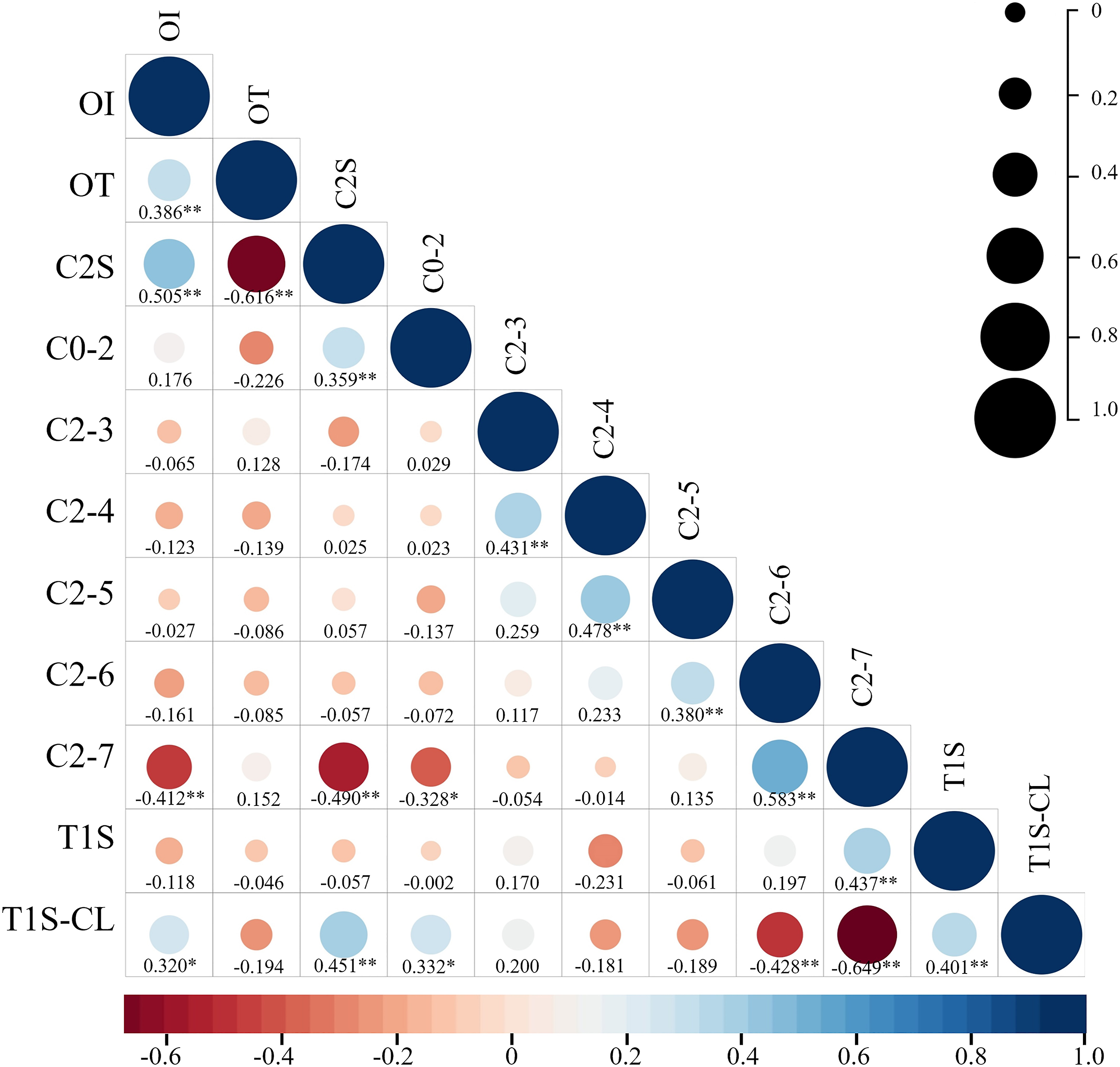
Linear regression analysis between OI, OT, C2S, T1S, and cervical parameters on cervical DR images.
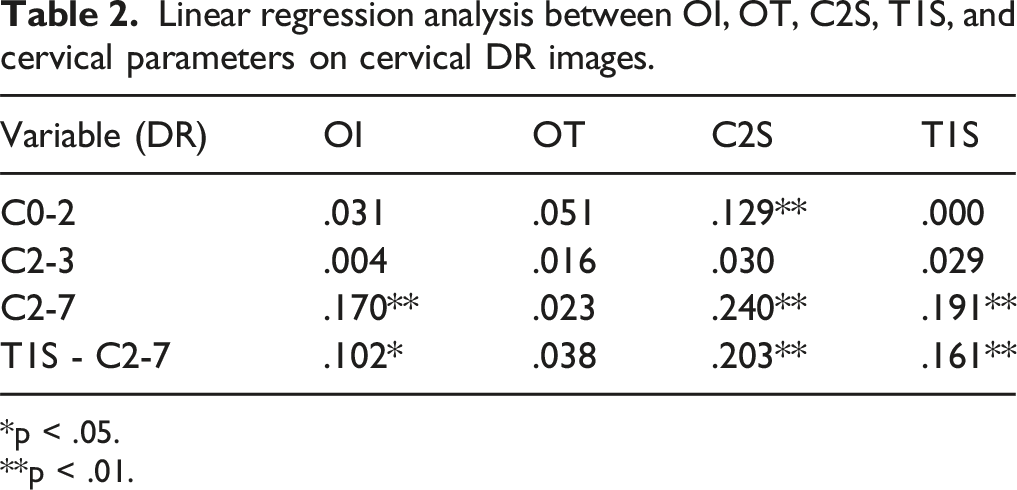
*p < .05.
**p < .01.
Linear regression analysis between OI, OT, C2S, T1S, and cervical parameters on cervical MRI images.
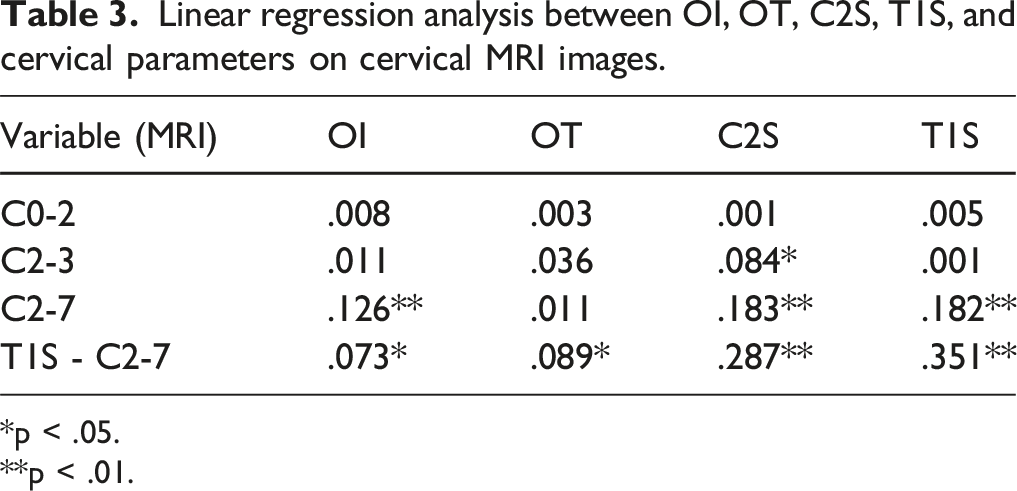
*p < .05.
**p < .01.
Discussion
Cervical parameters, including T1S, 2 CL, 3 C2S, 4 and C0-C2 angle have been reported. 5 These parameters are of great importance in selecting surgical methods for patients and evaluating sagittal balance of the cervical spine after surgery. 11 However, these parameters exhibit several limitations. For starters, there were no constant anatomical cervical alignment parameters. Moreover, when measuring the sagittal parameters of the cervical spine on conventional radiographs, there is often double shoulder joint occlusion, resulting in an unclear representation of the cervicothoracic junction, inability to identify the T1 vertebral body. Sometimes the inferior endplate of the C7 vertebral body cannot be determined, which makes it difficult to measure the parameters of the cervicothoracic spine. 12 Furthermore, the measurement of T1S and C2S is based only on the horizontal axis, which leads to measurement errors. 13 Additionally, although there are many cervical spine parameters and there is a statistical correlation between these parameters, except for C2S, T1S, and T1S-CL, other parameters were not correlated with clinical outcomes. 12 Therefore, discovering new independent and constant anatomical parameters in the cervical spine is crucial for the in-depth evaluation of cervical alignment.
Lee et al reviewed the spinal X-rays of 42 asymptomatic subjects and proposed a new cervical parameter, OI, 9 by measuring the internal angle of the odontoid process. OI is a constant parameter related to the anatomical structure of the cervical spine and is not affected by external factors. In addition, OI adds the measurement of the vertical axis based on the horizontal axis to analyze the alignment of the cervical spine in two directions. Different from C7 and T1, which are not visible on some patients, OI is clearly displayed on plain radiographs. This improves the practicability and reliability of the analysis. 14 Notably, the data in the study mentioned above were based solely on asymptomatic adults without cervical disease, which limited the clinical relevance of the study for diagnosis and prognosis in patients with CSM. Moreover, the measurement of odontoid process parameters has not been applied in MRI studies.
In our study, OI measured was 18.50 ± 4.24° on DR images and 18.41 ± 4.25° on MRI images, showing no statistical difference in the measurements between the two modalities (P = .776). Based on the DR and MRI images, OI were highly correlated with CL. This result is consistent with those reported by Lee et al. 9 The results confirmed that OI is a constant anatomical parameter that does not change with body position. The measurements of CL and T1S on the DR images were larger than those on the MRI images, which is consistent with Oshina’s research. 15 This may be because the older adult patients with CSM have a forward tilt posture when standing, and when MRI is performed in the supine position, the neck tilts backward, correcting the forward tilt of the cervical spine. This reduces the final T1 vertebral rotation. 16 In addition, when T1S is small, CL must be reduced to maintain the physiological balance of the cervical spine; 13 thus, CL and T1S in MRI images are smaller than those in DR.
In the lumbar spine and pelvis, a constant anatomical parameter, the pelvic incidence (PI), has been reported. 13 PI is crucial role in assessing the sagittal alignment of the lumbar spine and pelvis.17,18 The matching degree of PI and lumbar lordosis (LL) is an index to predict the success rate of short-segment spinal fusion after surgery. 19 In contrast, the more mismatched the PI-LL after surgery, the higher the risk of adjacent segment lesions and the lower the HRQoL score. 20 Consistent with PI, OI is a constant anatomical parameter of the cervical spine. Our results shows that OI is significantly correlated with CL in both DR and MRI images. Therefore, by evaluating the degree of agreement between OI and CL, surgeons can effectively analyze the sagittal alignment of the cervical spine and accurately plan cervical surgery.
The results of Lee’s study found that the OT value is related to the C0-2 angle, C2-7 angle, 9 T1S, and T1S-CL on the lateral X-ray film of the normal cervical spine. Based on the DR and MRI images of CSM patients, our study showed that OT was related to C2S or/and T1S-CL and was not associated with the C0-2 angle and C2-7 angle. This may reflect the fact that anatomical change of cervical sagittal alignment between patients with and without CSM.
In our study, C2S was significantly positively correlated with T1S-CL in DR and MRI and significantly negatively correlated with CL. This finding is consistent with that of a previous report. 21 This is because C2S is the approximate value for T1S-CL. 11 T1S-CL is a parameter describing the alignment between the cervical and thoracolumbar spine.4,22 Responding to the greater T1S, the larger CL required to maintain the head balance. If the patient’s CL is insufficient to match the T1S, C2 will tilt forward to increase C2S. 9 Therefore, in patients with difficulty in measuring T1S or C7S, odontoid parameters can be used instead of T1S-CL to describe the alignment of the cervical and thoracic vertebrae.
There are several limitations in this study. Some parameters of global sagittal balance could not be analyzed in the current study. In addition, stratification by age or gender subgroups could not be conducted owing to relatively small sample size. We would like to enlarge the group of cases in the future, to confirm our results in a larger cohort of subjects.
Conclusion
This study showed that OI was an independent parameter related to cervical anatomy, and its measurement was not influenced by external factors such as body position and examination instruments. For patients with CSM, odontoid parameters may accurately and reliably describe the sagittal alignment of the cervical spine in both the DR and MRI images.
Footnotes
Authors’ Contribution
QHY and JH designed the study and collected the data. CWY, XX, YQH and HLA did the data analysis. QHY wrote the manuscript. JH revised the manuscript and decided to submit the manuscript for publication. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of China (81860406), Guangxi Natural Science Foundation (2018GXNSFAA281127) and Youth Science Foundation of Guangxi Medical University (GXMUYSF201329). No benefit in any form has seen or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Ethical Approval
The study has been approved by the Medical Ethics Committee of the First Affiliated Hospital of Guangxi Medical University (2023-E008-01).
Consent
Written patient consent was obtained for publication of all aspects of the case including personal and clinical details and images, which may compromise anonymity.
Data Availability Statement
All supporting data can be provided upon request to the authors.