
Abstract
Study Design
Multicenter prospective study.
Objective
Patients with central sensitization (CS) are reported to be at high risk of poor outcomes after spinal surgery. However, the influence of CS on surgical outcomes for lumbar disc herniation (LDH) remains unknown. This study aimed to examine the association between preoperative CS and surgical outcomes in LDH patients.
Methods
A total of 100 consecutive patients with LDH (mean age 51.2) who underwent lumbar surgery were included in this study. The extent of CS was evaluated using the central sensitization inventory (CSI), a screening tool for CS-related symptoms. The patients completed the following CSI and clinical outcome assessments (COAs) preoperatively and 12 months postoperatively: the Japanese Orthopaedic Association (JOA) score for back pain, JOA back pain evaluation questionnaire (JOABPEQ), and Oswestry Disability Index (ODI). The association between preoperative CSI scores, and preoperative and postoperative COAs was analyzed, and the postoperative changes were statistically evaluated.
Results
The preoperative CSI score significantly decreased 12 months postoperatively. Preoperative CSI scores showed a significant correlation with most COAs; however, a significant correlation was only identified in the social function and mental health domains of JOABPEC postoperatively. Higher preoperative CSI showed worse preoperative COAs; however, all COAs significantly improved regardless of CSI severity. There were no significant differences in any COAs among the CSI severity groups 12 months postoperatively.
Conclusions
The results of this study showed that lumbar surgeries significantly improved the COAs regardless of preoperative severity of CS in patients with LDH.
Keywords
Introduction
Lumbar disc herniation (LDH) is one of the most common degenerative spinal diseases causing lower back pain and radiculopathy, affecting patients of working age.1-4 Acute lumbar radiculopathies due to a herniated disc are primarily managed with conservative treatments, and over 80% of patients experience symptom relief within 6 to 12 weeks. 1 Surgical interventions, such as discectomy, provide faster pain relief and perceived recovery in patients with severe or prolonged neurological symptoms. 1 Despite excellent short-term results after surgical treatment of symptomatic LDH, postsurgical degenerative disc disease, and recurrent back and leg pain have been reported in 3% to 43% of patients. 5 Several previous studies have reported prognostic factors for surgical outcomes, such as female sex, negative preoperative straight leg rising, 2 and duration of symptoms. 5 However, there are many unknown factors predictive of LDH surgical outcomes due to a variety of follow-up periods and surgical procedures. 6
Central sensitization (CS) is defined as the amplification of neural signaling within the central nervous system, affecting either normal or subthreshold afferent input, resulting in hypersensitivity, responsiveness to non-noxious stimuli, increased pain response evoked by stimuli outside the area of injury, and an expanded receptive field. 7 CS-related symptoms, characterized by complex physical and mental symptoms including disproportionate and diffuse pain due to hypersensitivity of the central neurons, are reported to negatively impact patient quality of life.8,9 The central sensitization inventory (CSI) is a self-report screening tool for CS-related symptoms.10,11 CS severity evaluated using CSI is significantly associated with preoperative neurological symptoms and health-related quality of life (QOL) in patients who undergo lumbar spine surgery. 12 Furthermore, higher CSI scores can predict worse surgical outcomes for decompression surgery for degenerative cervical myelopathy, 13 lumbar spinal stenosis (LSS)14,15 and thoracolumbar spinal fusion surgery. 16 However, the influence of CS on postoperative clinical outcomes following lumbar surgery in patients with LDH remains unknown.
The purpose of this multicenter prospective study was to investigate the influence of preoperative CS evaluated by CSI on the surgical outcomes of patients with LDH after discectomy surgery.
Methods
Study Design and Setting
This was a prospective multicenter cohort study.
Participants
In total, 569 consecutive patients underwent lumbar spine surgery at eight different institutions between May 2019 and May 2020. Among them, 149 patients with lumbar disc herniation who received surgical treatment were initially included; however, 49 patients (32.9%) dropped out of the study after 12 months of follow-up. Finally, data from 100 patients was analyzed (Figure 1). Study flow chart. LDH: lumbar disc herniation.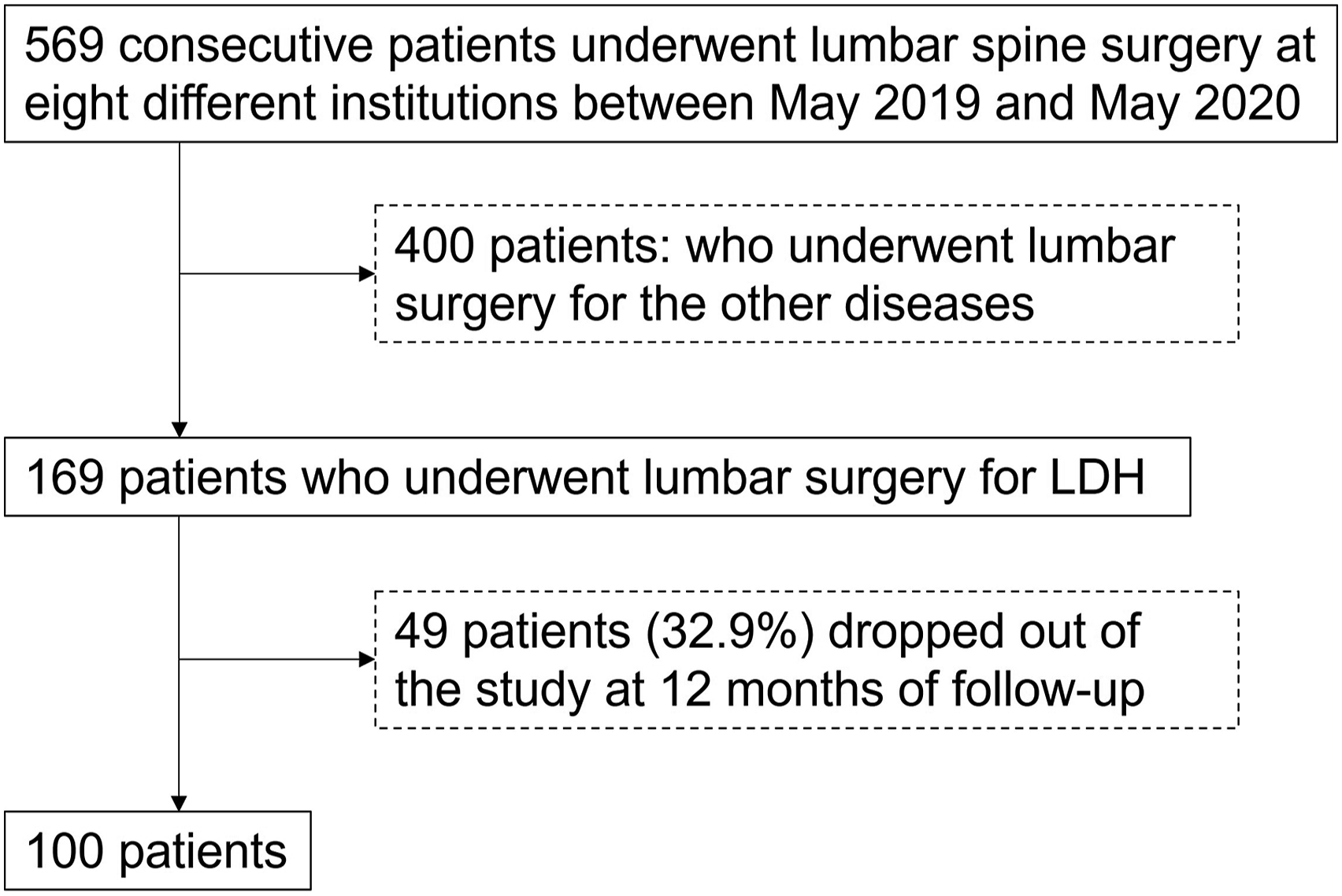
Measurement
Demographic information, including age and sex, was collected. CSI and COAs were evaluated preoperatively (pre) and 12 months postoperatively (post 12 M).
Central Sensitization Inventory
CSI is a self-report screening tool that helps quantify the extent of CS-related somatic and emotional symptoms. 11 For example, the following clinical symptoms were included in the questionnaire: non-refreshing sleep, sensitivity to bright light, headaches, skin problems, jaw pain, fatigue, concentration difficulties, and discomfort due to certain smells. 11 The Japanese version of the CSI, reported to have high reliability and validity, 10 was used in this study. The Japanese CSI is a 25‐ item questionnaire for assessing health-related symptoms common in CS conditions, 10 where each item is scored on a 5‐ point Likert scale ranging from 0 = “never” to 4 = “always.” The total score ranged from 0 to 100 points. CSI severity was classified into three groups: subclinical (0– 29 points), mild (30-39 points), and moderate-to-extreme (≥40 points), as previously reported, with modifications.
Japanese Orthopaedic Association Score for Back Pain
The JOA score is a clinician-reported outcome established and validated for evaluating lumbar back pain (LBP) and lumbar spinal diseases. 17 The JOA score consists of four domains, with a total of 29 points: subjective symptoms, clinical signs, activities of daily living, and bladder function. Higher scores indicate better conditions.
Japanese Orthopaedic Association Back Pain Evaluation Questionnaire
The JOABPEQ is composed of 25 items across five subscales (LBP, lumbar function, walking ability, social life function, and mental health) to measure multidimensional complications of low back disorders, including pain intensity, disability, and QOL.18,19 The score for each domain ranged from 0 to 100, with higher scores indicating better conditions. The intensity of LBP, pain in the buttocks and lower limb(s), and numbness in the buttocks and lower limb(s) were evaluated using a visual analog scale (VAS) of 0 to 100 mm, with higher values indicating worse pain.
Oswestry Disability Index
The ODI is the questionnaire mostly used to assess LBP-related QOL, with higher scores indicating a worse condition. 20 The ODI consists of 10 items that assess the level of pain and physical activity, including sleep, self-care, sexual life, social life, and travel. The Japanese version of the ODI, reported to have high reliability and validity, was used in this study. 21 The percentage of the total score, excluding information on sexual life, was analyzed in this study.
Statistical Analysis
Data are expressed as mean ± standard error. Differences in CSI, original JOA score, VAS (in mm), and the five domains of the JOABPEQ and ODI score differences between the pre and post 12 M periods were analyzed using a paired t test or Mann–Whitney U test. Correlations between CSI, age, and COAs were evaluated using Pearson’s correlation coefficient test or Spearman’s rank-order correlation test. Differences in VAS scores, the JOA score, each domain of the JOABPEQ and ODI for both pre and post 12 M, postoperative changes (post 12 - pre), and percentage changes ([post 12 M - pre]/pre × 100) among the CSI severity groups were analyzed using the Kruskal–Wallis test with Bonferroni correction post hoc tests. The percentage change in the JOA score was calculated using the following formula: (post 12 M – pre)/(29 – pre) × 100. Statistical significance was set at P < .05. All statistical analyses were performed using IBM SPSS Statistics version 28.0 (IBM Japan, Tokyo, Japan).
Results
Patient Characteristics
Preoperative (pre) and 12-month Postoperative (post 12 M) Clinical Outcome Assessments (COAs).
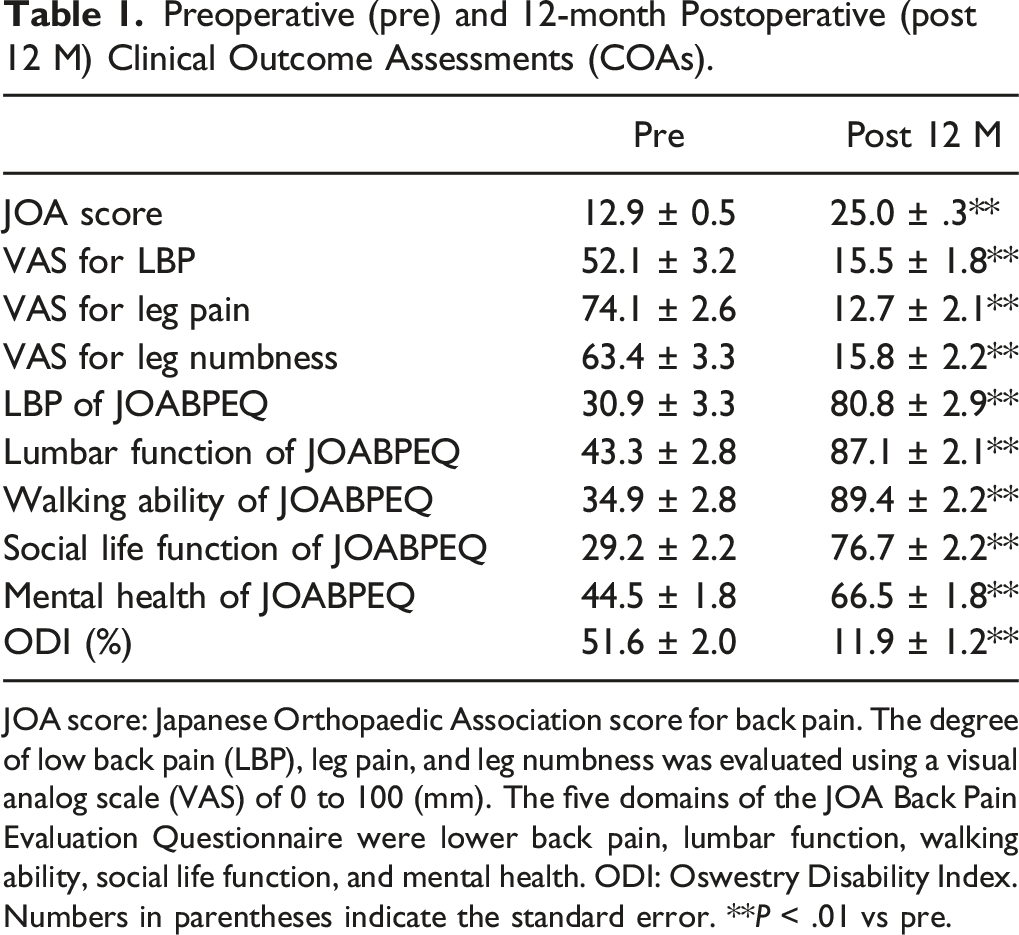
JOA score: Japanese Orthopaedic Association score for back pain. The degree of low back pain (LBP), leg pain, and leg numbness was evaluated using a visual analog scale (VAS) of 0 to 100 (mm). The five domains of the JOA Back Pain Evaluation Questionnaire were lower back pain, lumbar function, walking ability, social life function, and mental health. ODI: Oswestry Disability Index. Numbers in parentheses indicate the standard error. **P < .01 vs pre.
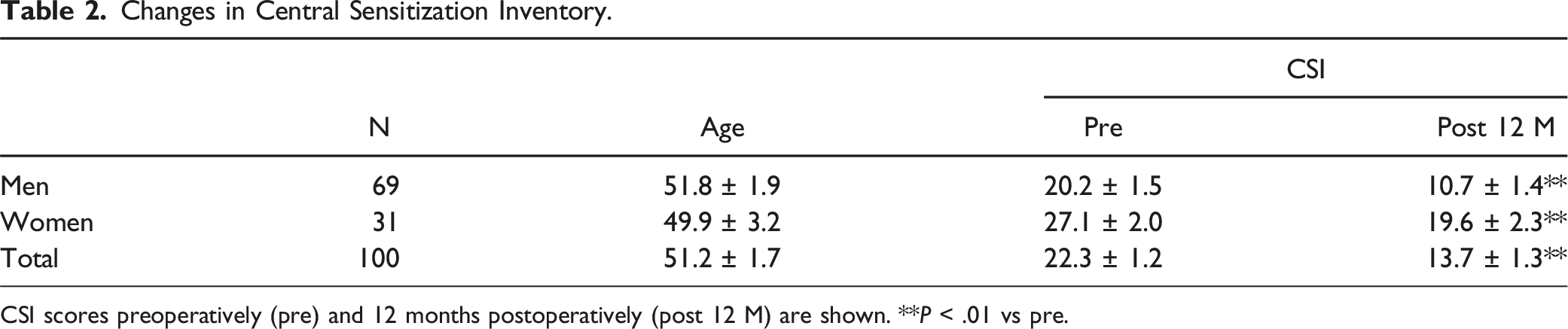
Changes in Central Sensitization Inventory
The average preoperative CSI score of the 100 subjects was 22.3 ± 1.2 (Figure 2A). According to the CSI severity group, the subjects were classified as subclinical (75.0%), mild (16.0%), or moderate to extreme (9.0%) (Figure 2B). The CSI score significantly decreased post 12 M (13.7 ± 1.3, P < .01) (Figure 2A), and the participants were classified as subclinical (88.7%), mild (9.7%), or moderate-to-extreme (1.4%) (Figure 2B). The preoperative CSI scores of both men and women significantly decreased post 12 M (P < .01). The average preoperative and postoperative CSI scores of women (pre:27.1 ± 2.0, post 12 M:19.6 ± 2.3) were significantly higher than those of men (pre:20.2 ± 1.5, post 12 M:10.7 ± 1.4, P < .01). There was no significant difference in age between the men and women (Table 2). No significant correlation was found between age and CSI scores before and after 12 M. Changes in the central sensitization inventory (CSI) score preoperatively and 12 months postoperatively. (A) Mean score preoperatively (Pre) and 12 months postoperatively (Post 12 M). (B) Change in percentage of CSI severity groups at pre and post 12 M. Subclinical (0-29 points), mild (30-39 points), and moderate-to-extreme (≥40 points). **P < .01. Changes in Central Sensitization Inventory. CSI scores preoperatively (pre) and 12 months postoperatively (post 12 M) are shown. **P < .01 vs pre.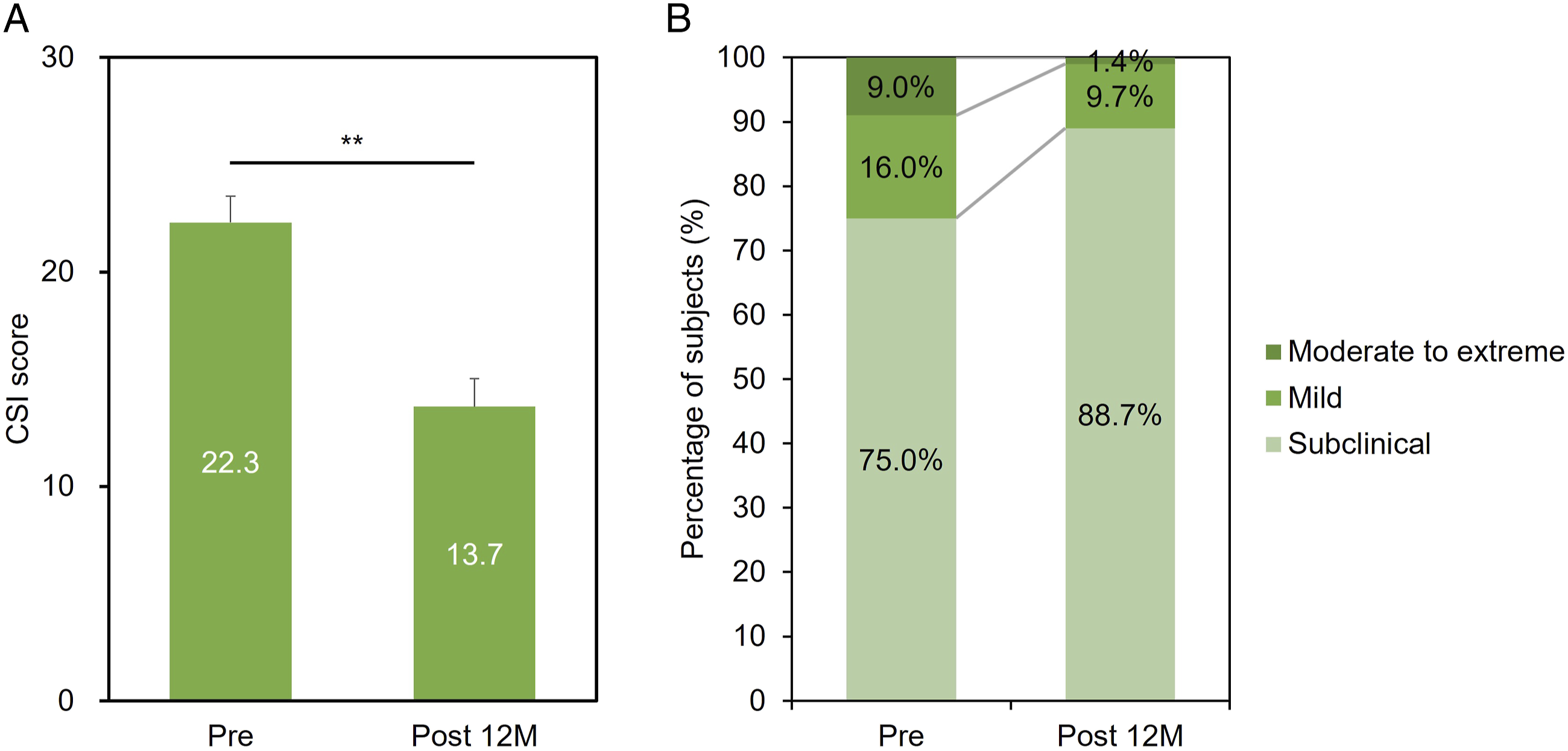
Correlation Between Preoperative CSI and COAs
Correlation Between the Preoperative Central Sensitization Inventory and Clinical Outcome Assessments.
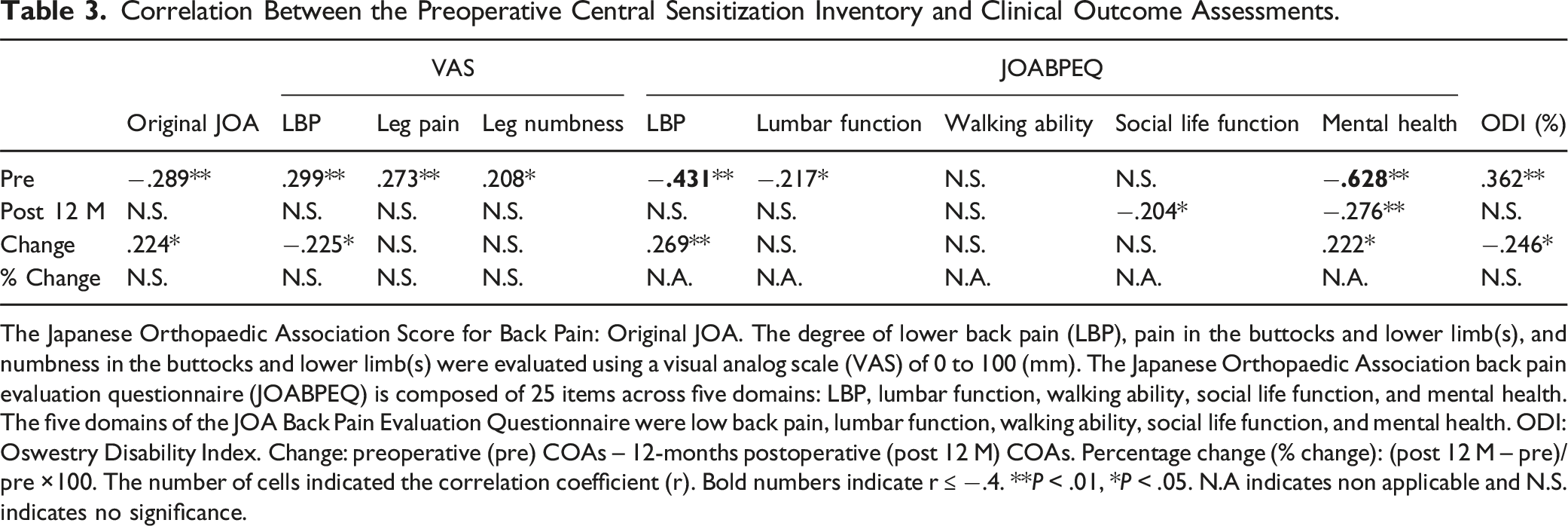
The Japanese Orthopaedic Association Score for Back Pain: Original JOA. The degree of lower back pain (LBP), pain in the buttocks and lower limb(s), and numbness in the buttocks and lower limb(s) were evaluated using a visual analog scale (VAS) of 0 to 100 (mm). The Japanese Orthopaedic Association back pain evaluation questionnaire (JOABPEQ) is composed of 25 items across five domains: LBP, lumbar function, walking ability, social life function, and mental health. The five domains of the JOA Back Pain Evaluation Questionnaire were low back pain, lumbar function, walking ability, social life function, and mental health. ODI: Oswestry Disability Index. Change: preoperative (pre) COAs – 12-months postoperative (post 12 M) COAs. Percentage change (% change): (post 12 M – pre)/pre ×100. The number of cells indicated the correlation coefficient (r). Bold numbers indicate r ≤ −.4. **P < .01, *P < .05. N.A indicates non applicable and N.S. indicates no significance.
Association Between Preoperative CSI Severity and COAs
Change in JOA Score
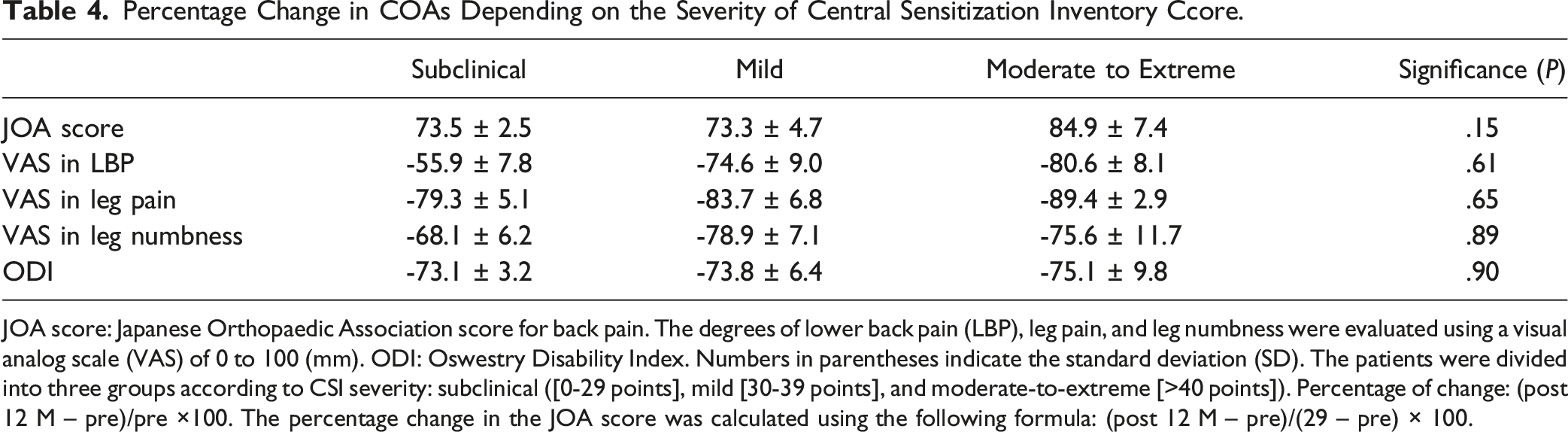
The preoperative JOA scores showed no significant differences among the groups (P = .72), and those of each of the three groups significantly increased post 12 M (P < .01; Figure 3). The changes in JOA scores did not differ significantly among the three groups (P = .052, Figure 3). There were also no significant differences in percentage change in JOA score among the three groups (Table 4). Japanese Orthopaedic Association (JOA) score for back pain according to the severity of the CSI. The patients are divided into three groups according to CSI severity: subclinical ([0-29 points], mild [30-39 points], and moderate-to-extreme [≥40 points]). The mean JOA score of each group at Pre and Post 12 M periods and the postoperative change (Post 12 – Pre) are presented. Percentage Change in COAs Depending on the Severity of Central Sensitization Inventory Ccore. JOA score: Japanese Orthopaedic Association score for back pain. The degrees of lower back pain (LBP), leg pain, and leg numbness were evaluated using a visual analog scale (VAS) of 0 to 100 (mm). ODI: Oswestry Disability Index. Numbers in parentheses indicate the standard deviation (SD). The patients were divided into three groups according to CSI severity: subclinical ([0-29 points], mild [30-39 points], and moderate-to-extreme [>40 points]). Percentage of change: (post 12 M – pre)/pre ×100. The percentage change in the JOA score was calculated using the following formula: (post 12 M – pre)/(29 – pre) × 100.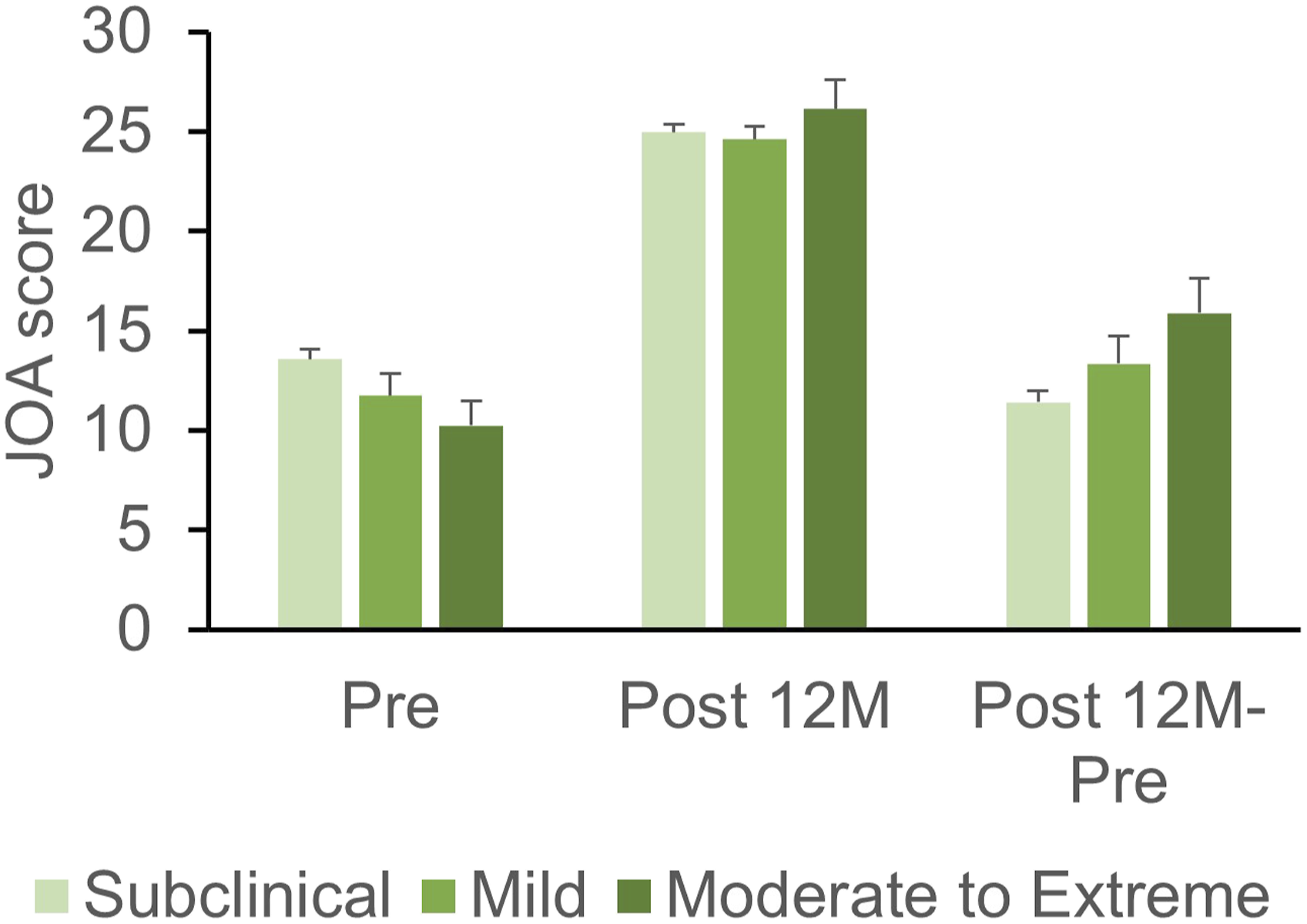
Change in VAS
Preoperative VAS scores for LBP significantly differed among the groups and were the highest in the moderate-to-extreme group followed by the mild and subclinical groups. VAS scores for LBP in each group significantly decreased post 12 M (P < .01) without significant differences among the groups (Figure 4A). There were no significant differences in the change (Figure 4A) and percent change (Table 4) of VAS among the groups. There were no significant differences in the preoperative VAS scores for leg pain and leg numbness among the groups (Figure 4B and C). The scores of each group significantly decreased post 12 M (P < .01); however, no significant differences were found among the groups (Figure 4B and C). No significant differences in the changes (Figure 4B and C) and the percentage of change (Table 4) among the three groups were observed in the VAS for leg pain and leg numbness. Visual analog scale (VAS) by severity of the central sensitization inventory (CSI). The patients are divided into three groups according to CSI severity: subclinical ([0-29 points], mild [30-39 points], and moderate-to-extreme [≥40 points]). The degree of (A) low back pain (LBP), (B) pain in the buttocks and lower limbs (leg pain), and (C) numbness in the buttocks and lower limbs (leg numbness) is evaluated using a visual analog scale (VAS) of 0-100 mm. The mean VAS score of each group at the Pre and Post 12 M periods and change (Post 12 – Pre) are presented. The italics above square brackets indicate P-values against group comparisons.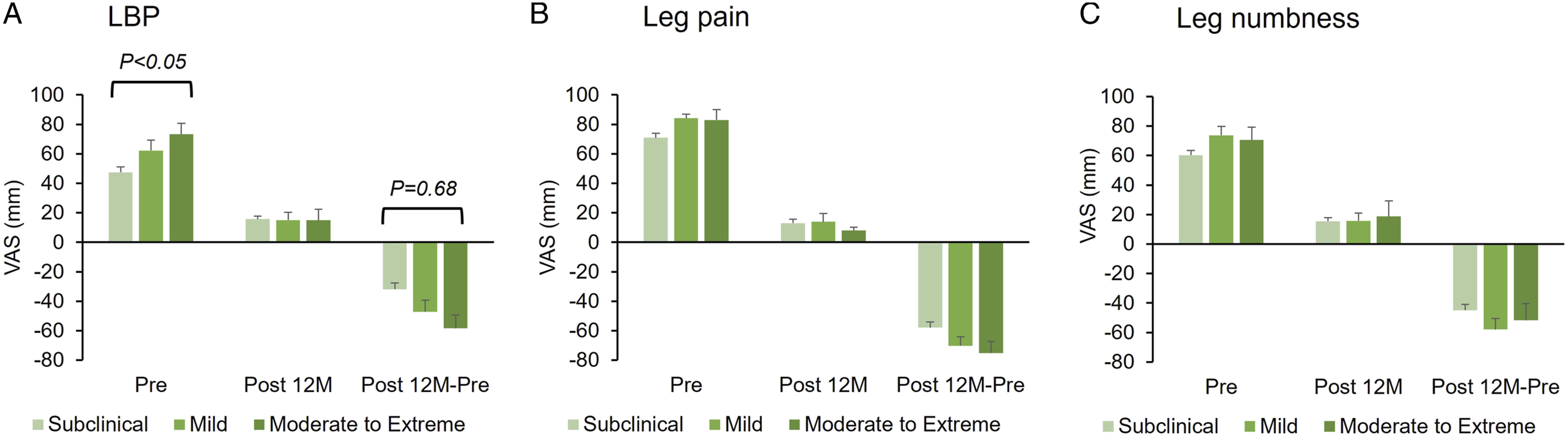
Change in JOABPEQ
Preoperatively, the LBP, lumbar function, and mental health domains of the JOABPEQ differed significantly among the three CSI severity groups, with the highest scores in the subclinical group, followed by the mild and moderate-to-extreme groups (Figure 5A, B, and E). However, no significant differences were found in the preoperative scores of walking ability and social life function (Figure 5C, and D). Scores in each of the three groups in all five domains of JOABPEC increased significantly post 12 M (P < .01). Consequently, no significant differences were found in the changes in JOABPEC domains (Figure 5B-E), except for the change in the LBP domain (Figure 5A). Changes in the LBP domain were significantly higher in the mild group than in the subclinical group (P < .05, Figure 5A). The Japanese Orthopaedic Association back pain evaluation questionnaire (JOABPEQ) according to the severity of the CSI score. The patients are divided into three groups according to CSI severity: subclinical ([0-29 points], mild [30-39 points], and moderate-to-extreme [≥40 points]). The JOABPEQ is composed of 25 items across five subscales: (A) LBP, (B) lumbar function, (C) walking ability, (D) social life function, and (E) mental health. The mean score of each group at the Pre and Post 12 M periods and change (Post 12 – Pre) are presented. The italics above square brackets indicate P-values against group comparisons.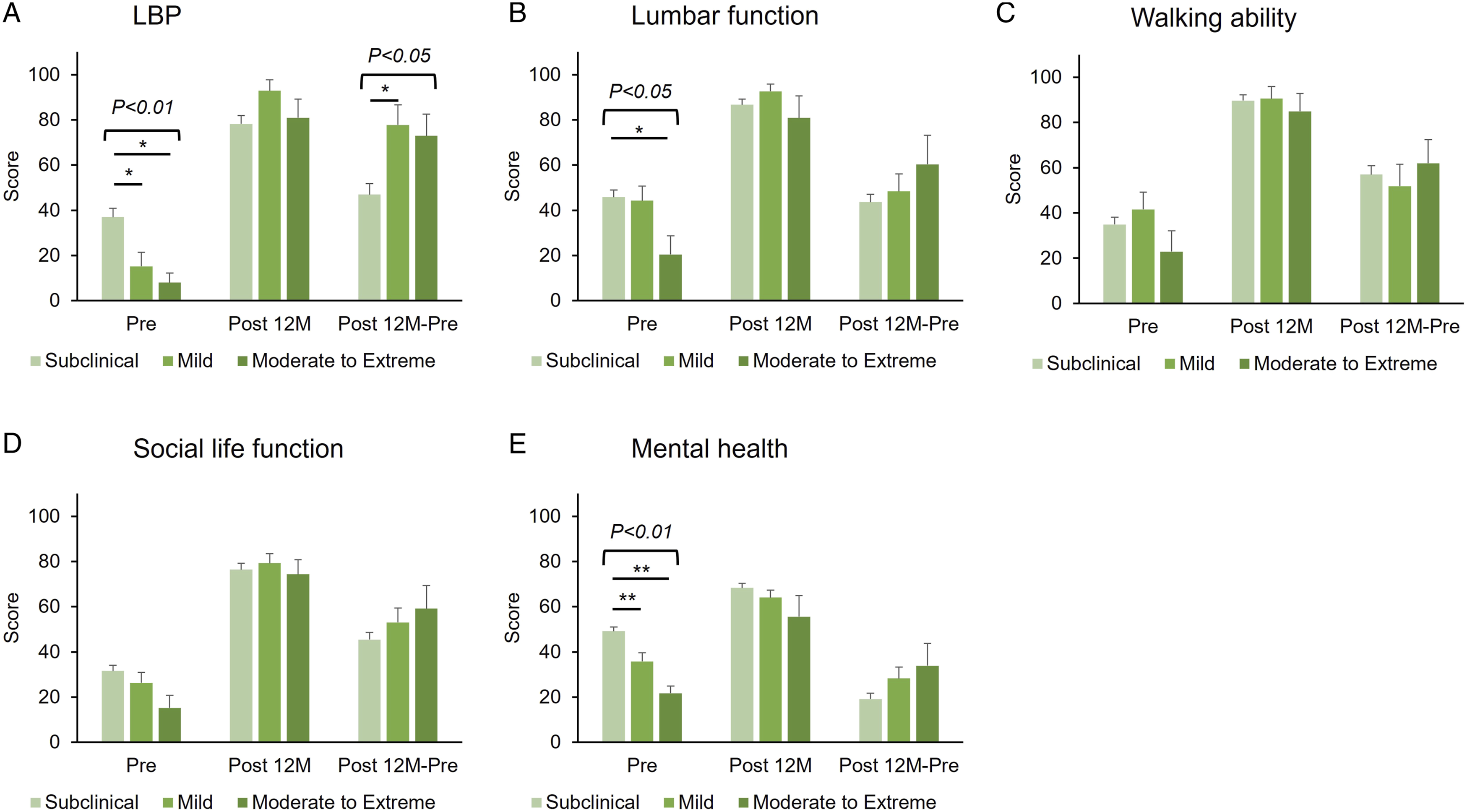
Change in ODI
The preoperative ODI scores were highest in the moderate-to-extreme group, followed by the mild and subclinical groups; the scores in the moderate-to-extreme group were significantly higher than those in the subclinical groups (P < .05, Figure 6). The preoperative ODI score of each of the three groups significantly decreased post 12 M (P < .01, Figure 6). The changes in the ODI scores did not differ significantly among the three groups. The percentage change in ODI score also showed no significant differences among the groups (Table 4). Oswestry Disability Index (ODI) according to the severity of the central sensitization inventory (CSI) score. The patients are divided into three groups according to CSI severity: subclinical ([0-29 points], mild [30-39 points], and moderate-to-extreme [≥40 points]). The mean score of each group at the Pre and Post 12 M periods and change (Post 12 – Pre) are presented. The italics above square brackets indicate P-values against group comparisons.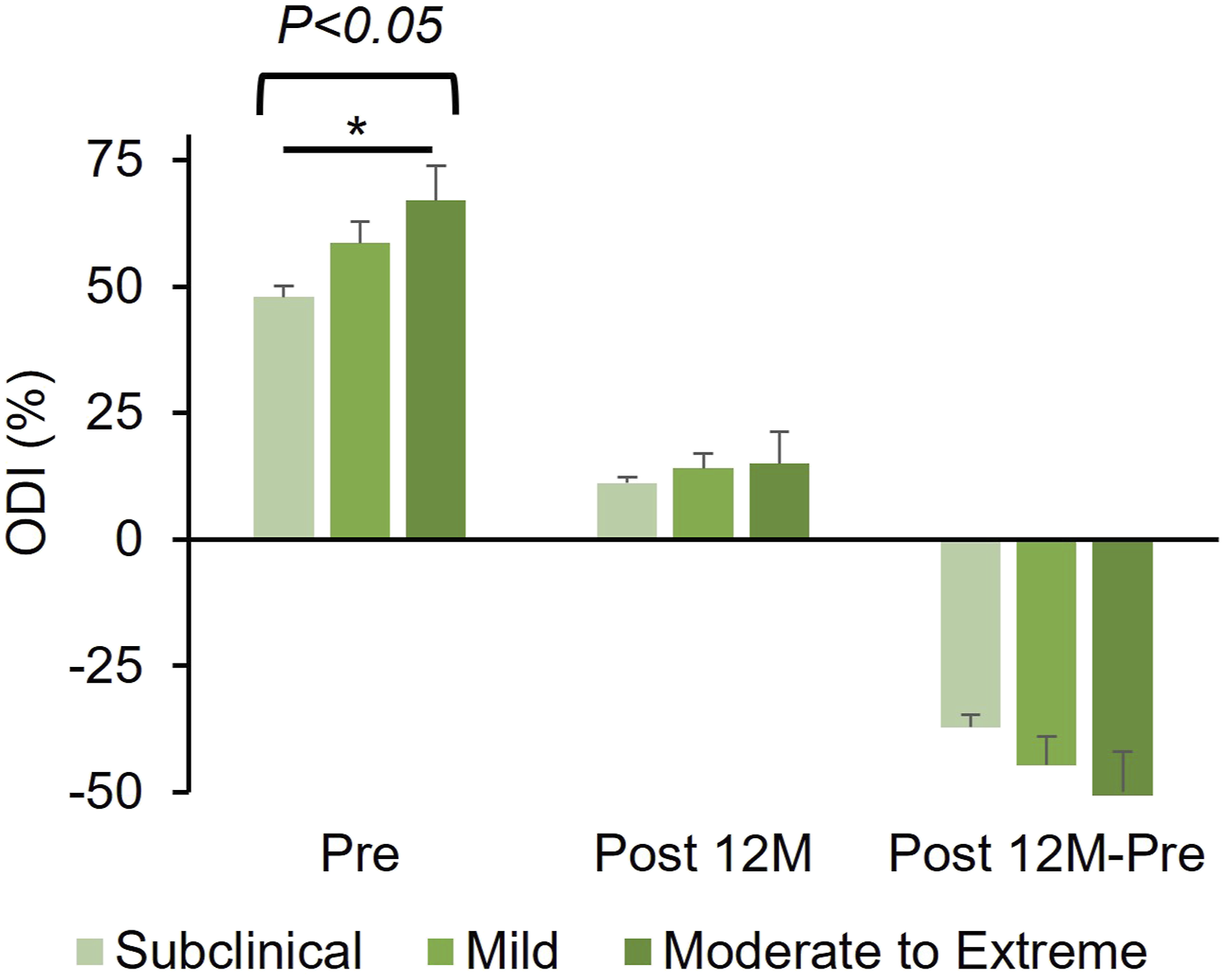
Discussion
This multicenter prospective study demonstrated for the first time that surgical outcomes for LDH were not influenced by preoperative CS evaluated using CSI. In this study, we noted a significant decrease in preoperative CSI 12 months after lumbar surgery. This suggests that decompression of the nerve roots and/or improvement of the inflammatory environment around the nerve roots by discectomy significantly improved the extent of CS in patients with LDH.
We demonstrated significant correlations between preoperative CSI and preoperative COAs; this suggests that CS as evaluated by CSI is significantly associated with neurological symptoms, disability, QOL, and mental health in patients with LDH. A trend was also noted between preoperative COAs and CSI severity, with COAs worst in the moderate-to-extreme group, followed by the mild and subclinical groups, as previously reported in post-lumbar surgery patients. 12 However, there were no significant differences among the CSI severity groups in postoperative COAs, suggesting that surgical intervention was effective in improving neurological symptoms, disability, QOL, and mental health in patients, regardless of the severity of preoperative CS.
In contrast, previous studies reported that CS contributes to postoperative pain in patients undergoing spinal surgery.13-16 Akeda et al reported that in 77 patients who underwent posterior decompression surgery for degenerative cervical myelopathy, preoperative CSI score severity was significantly associated with worse preoperative and postoperative JOA scores for cervical myelopathy, and JOA cervical myelopathy evaluation questionnaire (JOACMEQ) score. 13 Preoperative CSI scores were noted to be associated with worse quality of life outcomes and an increased length of stay in 664 patients who underwent thoracic and/or lumbar fusion. 16 Preoperative CSI affects the 3 months postoperative lumbar function, social life, and mental health domains of the JOABPEQ, as observed in a retrospective study of 114 patients who underwent lumbar surgery for LSS. 14
A previous study evaluated 197 patients who underwent lumbar surgery for LSS and reported that the preoperative CSI score significantly decreased at 12 months postoperatively and was significantly correlated with all COAs both preoperatively and 12 months postoperatively. 15 Higher preoperative CSI scores were associated with worse postoperative COAs and inferior postoperative improvement rates in several COAs. 15 In this multicenter study, we observed that the preoperative mean CSI scores of patients with LDH (22.3 ± 1.2) and patients with LSS (21.8 ± .8) were similar; however, the mean postoperative CSI scores of those with LDH (13.7 ± 1.3) were significantly lower than those of patients with LSS (17.9 ± 1.0). The postoperative change in CSI score was higher in patients with LDH compared to that in patients with LSS, suggesting that surgical interventions for patients with LDH improved the extent of CS more effectively than in patients with LSS, along with improvements in neurological symptoms. Younger age and short disease duration until surgical interventions in patients with LDH patients may contribute to higher postoperative improvement in CSI score than patients with LSS. However, further investigation is required to identify the factors associated with CSI improvement.
In the current study, the CSI score was used to for evaluation of CS-related symptoms but not sensory disturbance itself. The assessment of sensory disturbance by quantitative sensory testing (QST) 22 might improve the accuracy of evaluating CS for the patients with LDH.
This study had several limitations. First, the duration of neurological symptoms from symptom onset to lumbar surgery was not investigated in this study. This has been reported to contribute to surgical outcomes.5,23 Second, the extent or size of LDH, type of herniation (central or lateral), or symptoms (cauda equina syndrome or radiculopathy) may have a significant impact on the degree of CS and surgical outcomes; however, imaging analyses using computed tomography and/or magnetic resonance imaging were not conducted in this study.
Conclusions
This multicenter prospective study showed that preoperative CS evaluated using CSI was remarkably improved after surgical intervention in LDH patients. Preoperative CSI scores had a significant influence on preoperative COAs, but less on COAs postoperatively. We revealed that surgical interventions significantly improved the neurological symptoms, disability, and QOL of LDH patients, regardless of the severity of CS preoperatively. Therefore, the authors concluded that LDH patients with CS-related symptoms (CSI score >40) are also candidates for surgical treatment.
Footnotes
Authors’ Note
Ethics were approved by the institutional review boards of Mie University Hospital (IRB reference number: H2020-027). Informed consent was obtained in the form of opt-out on the website.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.