
Abstract
Study Design:
Retrospective cohort study.
Objective:
We evaluated the effectiveness of minimally invasive (MIS) tubular discectomy in comparison to conventional open surgery among patients enrolled in the Canadian Spine Outcomes and Research Network (CSORN).
Methods:
We performed an observational analysis of data that was prospectively collected. We implemented Minimum Clinically Important Differences (MCIDs), and we adjusted for potential confounders with multiple logistic regression. Adverse events were collected according to the Spinal Adverse Events Severity (SAVES) protocol.
Results:
Three hundred thirty-nine (62%) patients underwent MIS tubular discectomy and 211 (38%) underwent conventional open discectomy. There were no significant differences between groups for improvement of leg pain and disability, but the MIS technique was associated with reduced odds of achieving the MCID for back pain (OR 0.66, 95% CI 0.44 to 0.99, P < 0.05). We identified statistically significant differences in favor of MIS for each of operating time (MIS mean (SD) 72.2 minutes (30.0) vs open 93.5 (40.9)), estimated blood loss (MIS 37.9 mL (36.7) vs open 76.8 (71.4)), length of stay in hospital (MIS 73% same-day discharge vs open 40%), rates of incidental durotomy (MIS 4% vs open 8%), and wound-related complications (MIS 3% vs open 9%); but not for overall rates of reoperation.
Conclusions:
Open and MIS techniques yielded similar improvements of leg pain and disability at up to 12 months of follow-up, but MIS patients were less likely to experience improvement of associated back pain. Small differences favored MIS for operating time, blood loss, and adverse events but may have limited clinical importance.
Keywords
Introduction
Lumbar disc herniations that cause symptomatic radiculopathy are a leading cause of disability, and lumbar discectomy is one of the most commonly performed spine operations worldwide.1-3 Among appropriately selected patients, lumbar discectomy often yields excellent clinical results with satisfactory cost-effectiveness,4,5 but there is ongoing debate about whether specific surgical techniques might be preferable.1,6-9
One of the earliest descriptions of lumbar discectomy was that reported by Mixter and Barr in 1932, in which an L2 to S1 exploratory laminectomy led to removal of a “mass one centimeter in diameter” that was “pressing on the left fifth nerve root and displacing the cauda equina to the right”. 10 Since that time, one of the most important trends in lumbar discectomy surgery has been minimization of soft tissue dissection to achieve less invasiveness. 11 Conventional open microdiscectomy as summarized by McCullough in 1992 is the most widely adopted technique, 12 but minimally invasive surgery (MIS) via table-mounted tubular retractor systems as described by Foley et al is also popular. 13 In an MIS tubular discectomy, sequential dilators and fluoroscopic guidance are used to create a surgical pathway through the lumbar paraspinous muscles rather that detaching their insertions and retracting them from the midline.
To date, studies of MIS tubular discectomy have failed to identify consistent advantages, and some have suggested increased rates of adverse events such as nerve injury and incidental durotomy. 1 The current best available evidence comes from a 2009 randomized controlled trial in which 328 patients underwent either tubular discectomy or conventional open microdiscectomy. 8 This trial did not identify any statistically significant differences for function or rates of complications at one year of follow-up, and reported greater residual back and leg pain among patients treated with the tubular technique. More recently, Li et al pooled data from 8 randomized controlled trials and 2 observational studies and found no significant differences for operative time, blood loss, length of stay, complications, short or long term back and leg pain, and Oswestry Disability Index scores. 9
Further high-quality evidence could help resolve uncertainty and inform clinical decision-making. Although large randomized controlled trials provide the most reliable evidence, well-designed observational studies can favorably balance data quality with feasibility, practicality, and generalizability.14-16 The Canadian Spine Outcomes and Research Network (CSORN) is an ongoing prospective multicenter observational study, and data from CSORN are optimally suited to answer questions about the effectiveness of surgical interventions in routine clinical practice.
In this study, we aimed to determine the effectiveness of MIS tubular discectomy in comparison to conventional open surgery for symptomatic lumbar disc herniations among patients enrolled in CSORN. Our primary objective was to evaluate potential differences in patient-reported leg pain, back pain, disability, function, and satisfaction at 3 and 12-months after surgery, and our secondary objective was to evaluate potential differences in reoperations, adverse events, operating room time, blood loss, and length of stay. Our null hypothesis was that there would be no significant differences between groups.
Methods
We performed a retrospective controlled observational study using data that was prospectively collected from consecutive patients enrolled in CSORN. As described elsewhere,17-21 CSORN is a group of over 50 neurosurgical and orthopedic spine surgeons from 18 tertiary care academic and non-academic hospitals across Canada. Teams of surgeons and local research coordinators collected patient data at each site, which were then tracked and audited by a national coordinator. We obtained Clinical Research Ethics Board approval at each participating site prior to enrolling patients, collecting data, and performing this study. All patients provided written informed consent to participate.
Patient Sample
We included all patients who presented to surgeons participating in CSORN at 12 Canadian sites with lower extremity radiculopathy secondary to a lumbar disc herniation and underwent primary discectomy surgery via either a minimally invasive tubular retractor approach (“MIS”) or via a conventional open (“Open”) approach. We excluded patients with recurrent disc herniations, patients undergoing revision procedures, patients treated for concurrent disc herniations at multiple levels, patient undergoing urgent or emergent procedures such as for Cauda Equina Syndrome and patients who underwent fusion or arthroplasty rather than discectomy.
Surgical Techniques
Patients underwent discectomy surgery via either MIS or open techniques according to the recommendations and preferences of the local participating surgeons at each site (Figure 1). There was no standardization of any aspects of care, including patient selection, surgical decision-making, and peri-operative management. All surgeons were fellowship-trained and were experienced with their procedure(s) of choice.
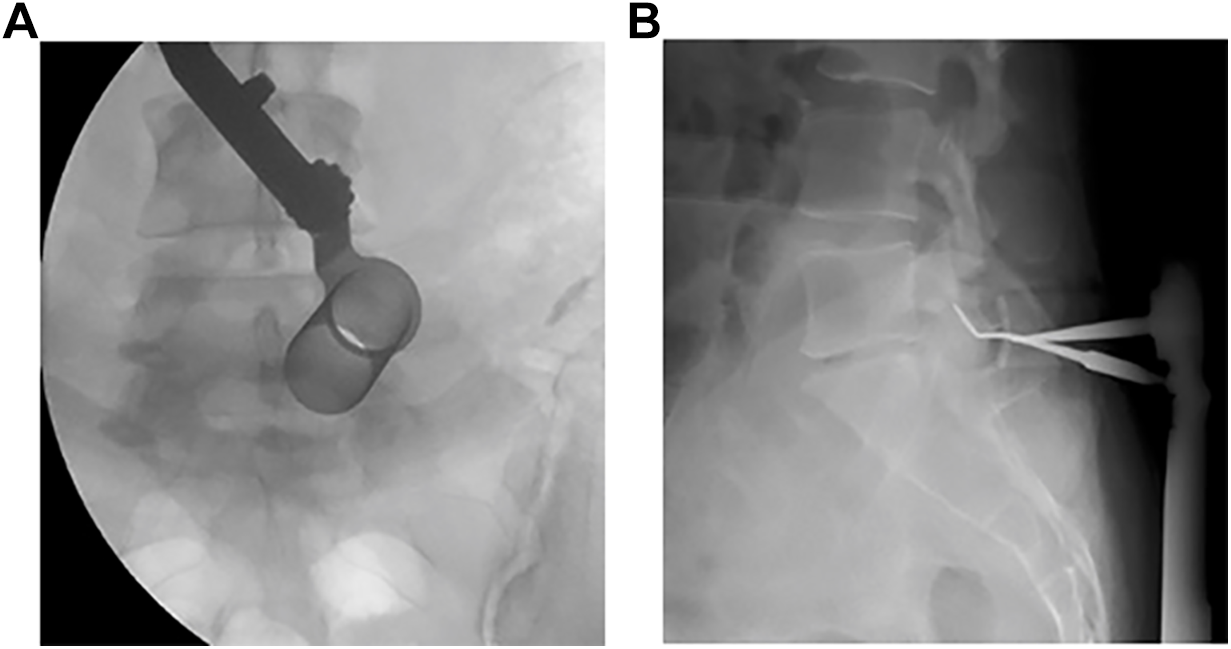
Illustrative cases: (a) intra-operative fluoroscopic image of a minimally invasive tubular lumbar discectomy performed at L5-S1 in a 34-year old female, and (b) intra-operative cross-table radiograph of a conventional open lumbar discectomy performed at L5-S1 in a 38-year old male.
MIS discectomies were performed with use of a table mounted tubular retractor system, whereby fluoroscopic guidance was used to place sequential dilators via a small incision through the paraspinal muscles to the level of interest until final access was established. Discectomies were then performed with aid of an operating microscope by performing a unilateral laminotomy, removing overlying ligamentum flavum, mobilizing the affected nerve root, and removing herniated disc material.
Open procedures were performed via unilateral midline subperiosteal exposures, whereby the paraspinal muscles were detached from the spinous processes and laminae at the level of interest until final access was established with use of a McCulloch or similar hook and blade retractor system. Discectomies were then performed in similar fashion as described for the tubular retractor system with aid of an operating microscope or loupe magnification at the surgeons’ discretion.
Data Sources
We used standardized case report forms to collect the following pre-operative baseline characteristics: age, sex, body mass index (BMI), living alone (versus not alone), education (post-secondary or greater), smoking status, presence of disability or insurance claims, number of comorbidities, daily opioid use, and duration of symptoms.
We collected baseline and follow-up measures of patient-reported leg and back pain with an 11-item numeric pain rating scale (NPRS), where 0 represents no pain and 10 represents worst imaginable pain. Patient reported disability and function were collected using the Oswestry Disability Index (ODI) and the Short Form 12 (SF-12) Physical and Mental Component Summary scores (PCS and MCS).
Adverse events were collected prospectively using the Spinal Adverse Events Severity (SAVES) protocol, from intra-operatively up to 12 months after surgery.22-24 Blood loss and total procedural operating room time were recorded prospectively by surgeons at the end of each case, and length of stay was recorded prospectively by research personnel at the time of discharge.
Statistical Analysis
We report discrete variables as counts or proportions, normally distributed continuous variables as means with standard deviations (SDs), and skewed continuous variables as medians with interquartile ranges (IQRs). We used parametric tests (independent samples t-test, chi-square test) for data with normal distributions and nonparametric tests (Mann-Whitney U test) for data without normal distributions.
We tested for changes in mean patient-reported leg pain, back pain, disability, and function, and we interpreted these changes using Minimal Clinically Important Differences (MCIDs), which are the smallest magnitude treatment effects that informed patients are likely to perceive as beneficial enough to justify changes in their management.25,26 We implemented the following MCIDs, which have been established elsewhere:21,27,28 NPRS leg pain – 1.6 points, NPRS back pain – 1.2 points, ODI – 12.8 points, SF12 PCS – 3.3 points, SF12 MCS – 3.8 points.
We tested for unadjusted and adjusted associations between surgical technique and patient-reported outcomes using univariate and multiple binomial logistic regression. Candidate variables were initially selected based on potential clinical importance, and variables with univariate P-values <0.2 were included in final adjusted models, from which we report Odds Ratios (OR) with 95% Confidence Intervals (CIs). We performed sensitivity analyses in which categorical and continuous versions of variables were exchanged, study site was controlled for, and alternative model building strategies were tested (full model, backward elimination, and forward selection). We evaluated model fit using the coefficient of determination (adjusted R2). We also performed a subgroup analysis in which only patients with BMI greater than 30 were included.
All analyses were complete case analyses in which patients with missing data were excluded and imputations were not performed. All tests of significance were 2-tailed and P-values <0.05 were considered statistically significant. We used IBM SPSS (version 26.0.0.1, IBM Corp.) and Microsoft Excel (version 16.43, Microsoft Corp.).
Results
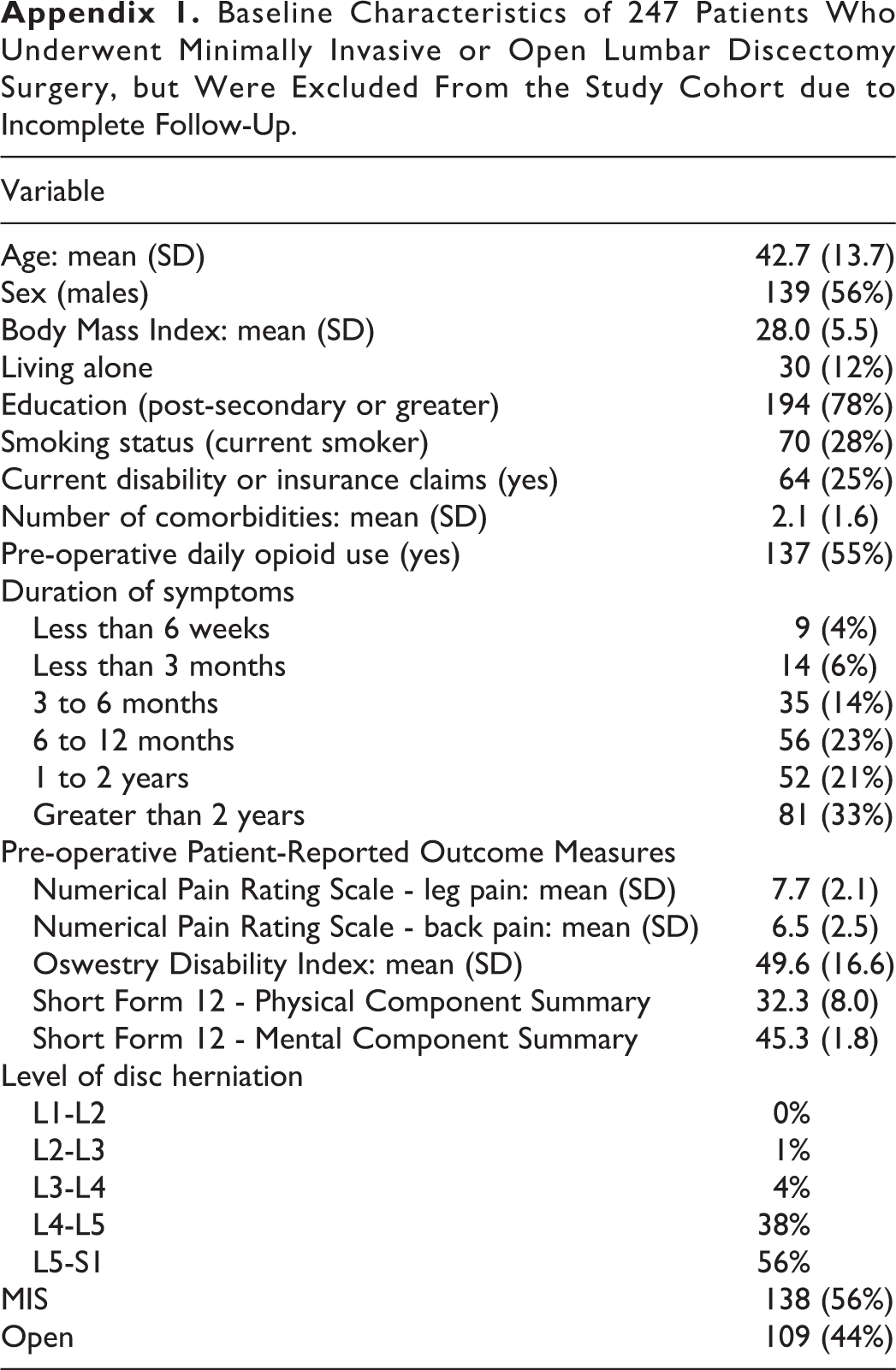
We identified 797 patients in the CSORN registry database who presented with lumbar radiculopathy, met the inclusion criteria, completed their baseline data collection, and underwent discectomy surgery (Figure 2). Of these, we excluded 247 (31%) because of missing data for patient reported outcome measures at 12 months of follow-up. Of note, the baseline demographics of these patients excluded for missing data did not differ substantially from our final study sample (Appendix 1). This yielded a final study sample of 550 patients that had been enrolled across 12 centers between 2015 and 2019. There were 339 (62%) patients who underwent MIS tubular discectomy and 211 (38%) who underwent conventional open discectomy.
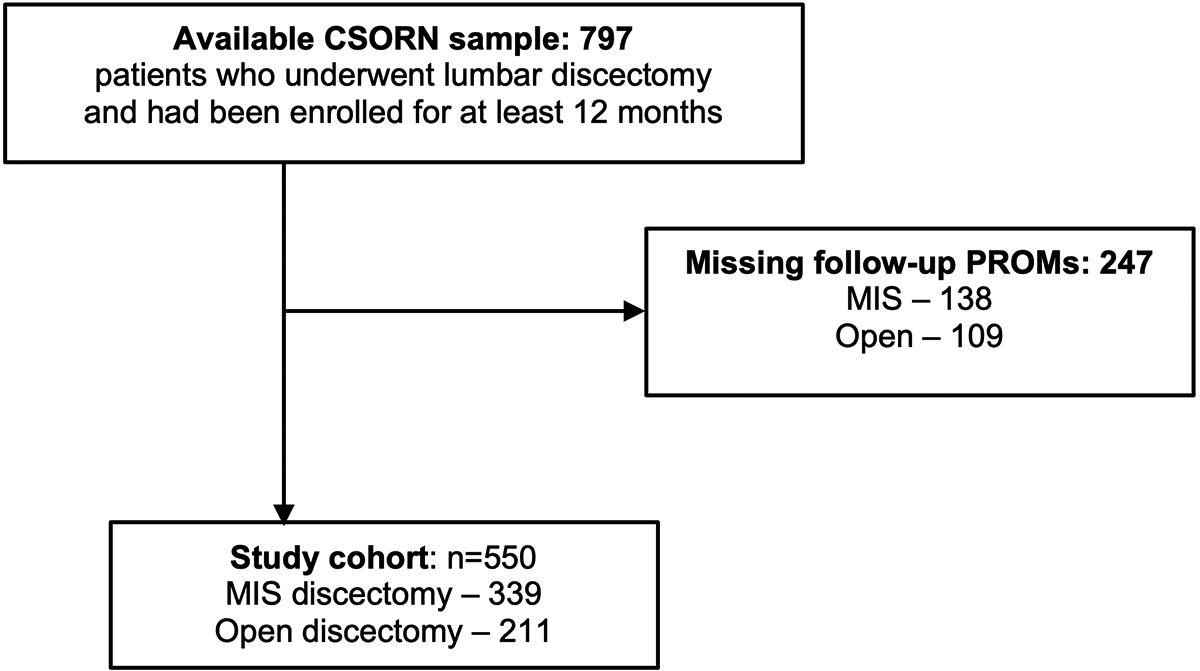
Identification of the study cohort: 550 patients who underwent minimally invasive (MIS, n = 339) or open (n = 211) lumbar discectomy surgery. CSORN = Canadian Spine Outcomes and Research Network; PROMs = Patient-Reported Outcome Measures.
We report the baseline characteristics of our study sample in Table 1. Mean age was 45.6 (SD 13.1), and 52% were male. There were no significant differences between MIS and Open groups for baseline demographics or baseline measures of pain, disability, and function. Across the combined cohort, mean pre-operative leg pain was 7.4 (SD 2.0) and back pain was 6.3 (SD 2.5). The most commonly involved spinal levels were L4-L5 (39%) and L5-S1 (53%). Mean operating time was 80 minutes (SD 36), mean blood loss was 53 mL (SD 56), and median length of stay was 0 days (IQR 0 - 1).
Baseline Characteristics of 550 Patients who Underwent Minimally Invasive (MIS) or Open Discectomy Surgery.

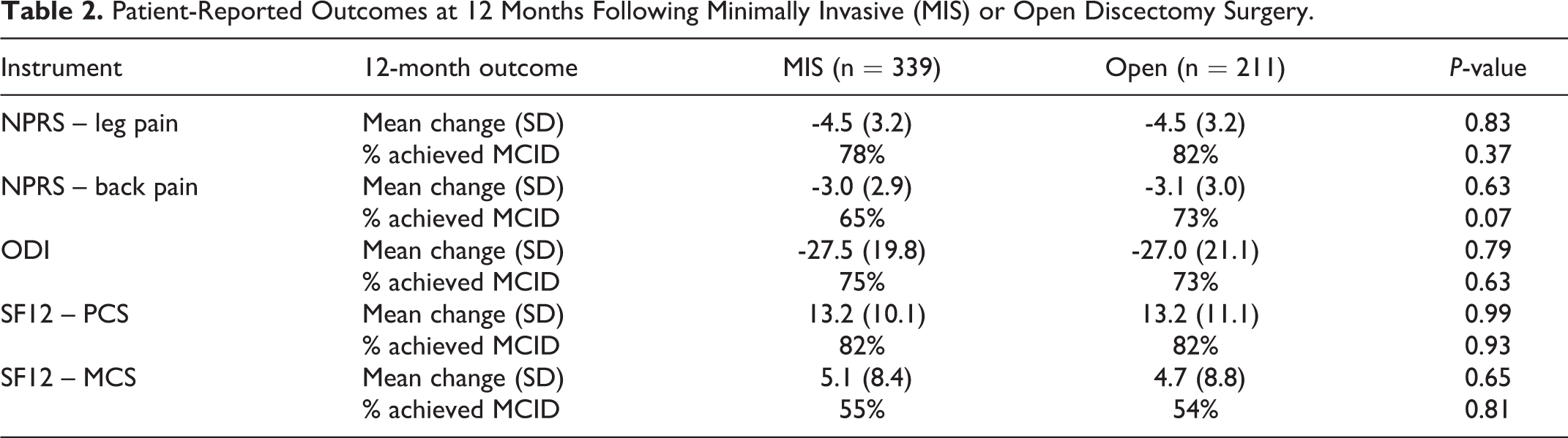
In unadjusted analyses at 3- and 12-months of follow-up after surgery, there were no significant differences between MIS and Open for mean NPRS leg pain, NPRS back pain, ODI, SF-12 PCS, or SF-12 MCS. We show the 12-month data in Table 2 and Figure 3. Mean change in leg pain across the combined cohort was -4.5 points (SD 3.2) and 80% of patients achieved the MCID for leg pain, while mean change in back pain across the cohort was -3.0 points (SD 2.9) and 68% of patients achieved the MCID for back pain. Mean change in disability according to ODI was -27.3 (SD 20.4) and 74% of patients achieved the MCID for ODI.
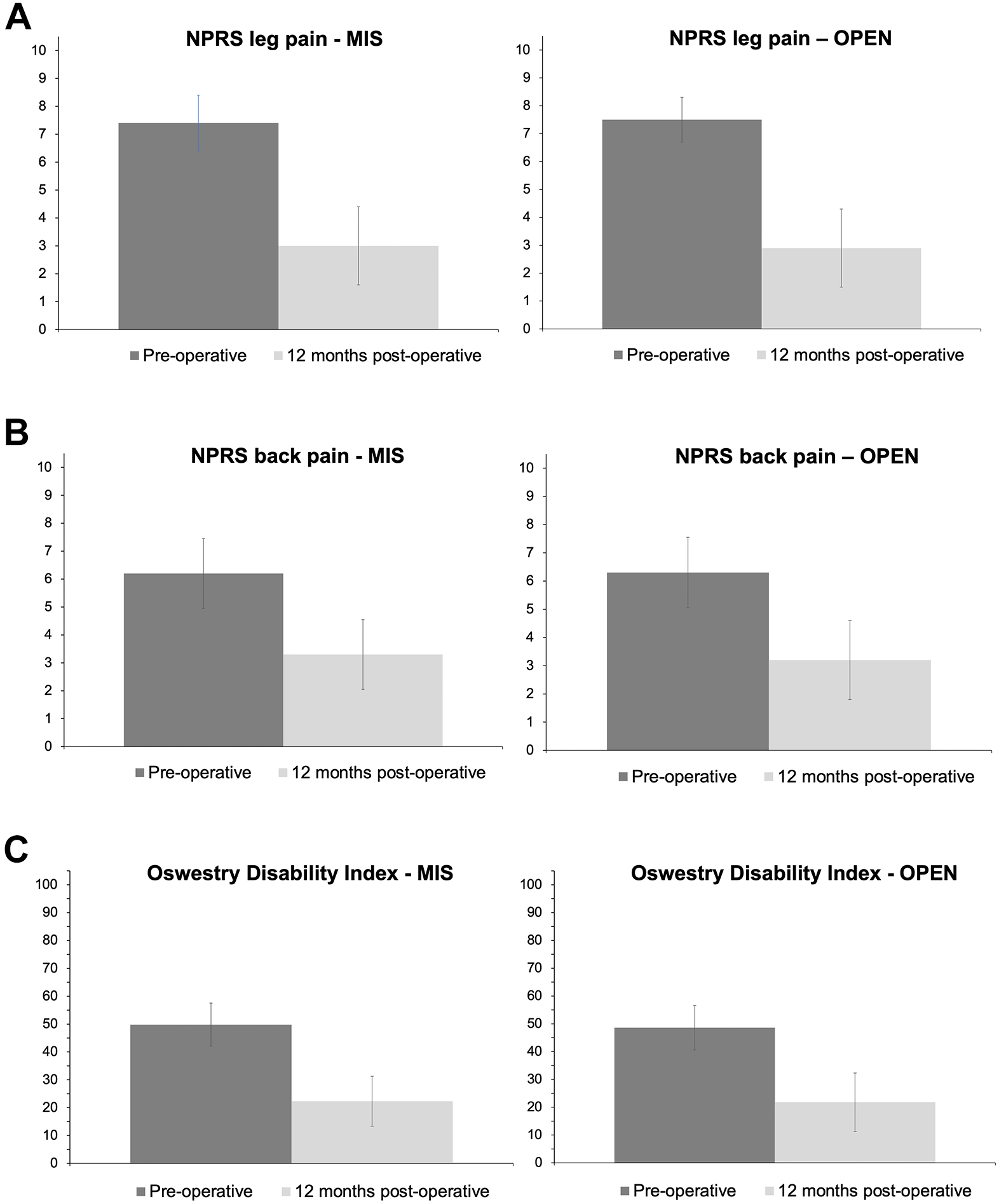
Pre-operative and 12-month post-operative Numerical Pain Rating Scale (NPRS) for (a) leg pain and (b) back pain, and (c) Oswestry Disability Index (ODI) scores patients who underwent minimally invasive (MIS) tubular lumbar discectomy (n = 339) or conventional open (OPEN) lumbar discectomy (n = 211). (a) NPRS leg pain (b) NPRS back pain (c) ODI.
Patient-Reported Outcomes at 12 Months Following Minimally Invasive (MIS) or Open Discectomy Surgery.
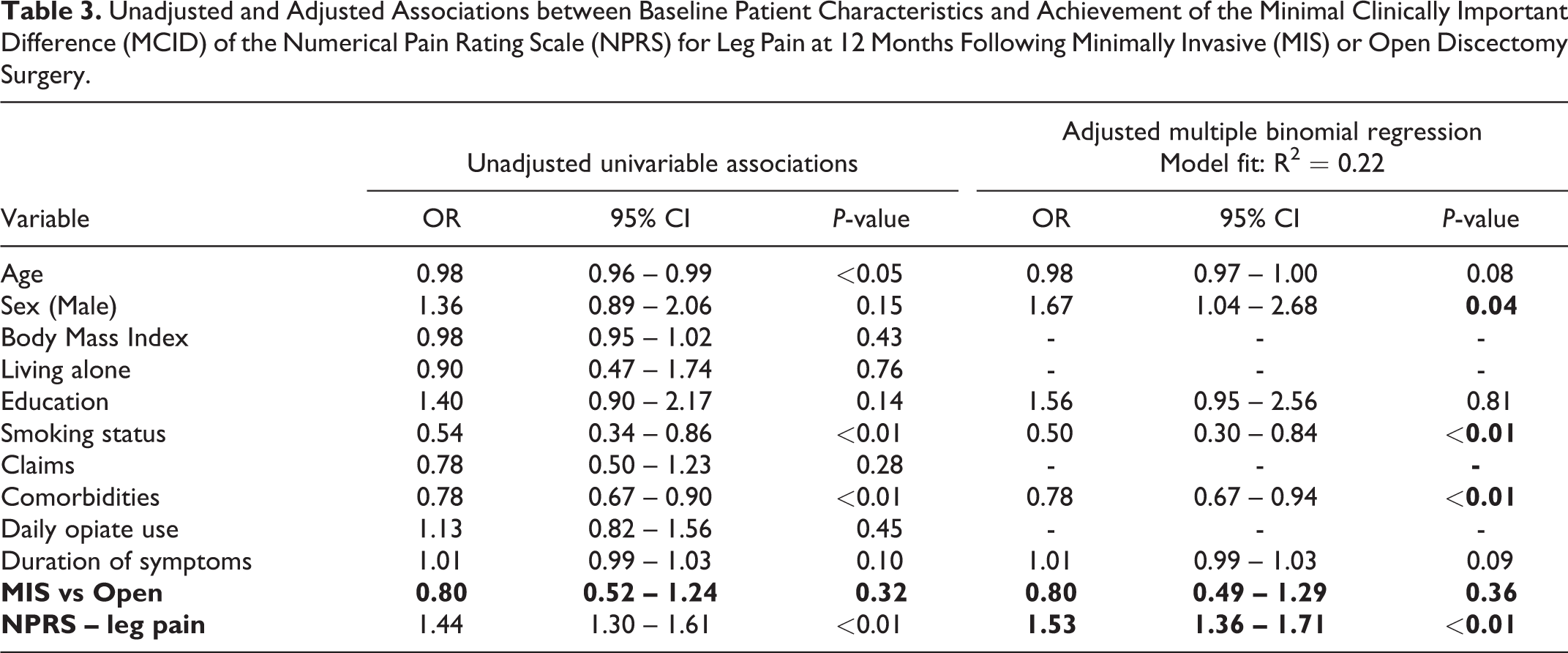
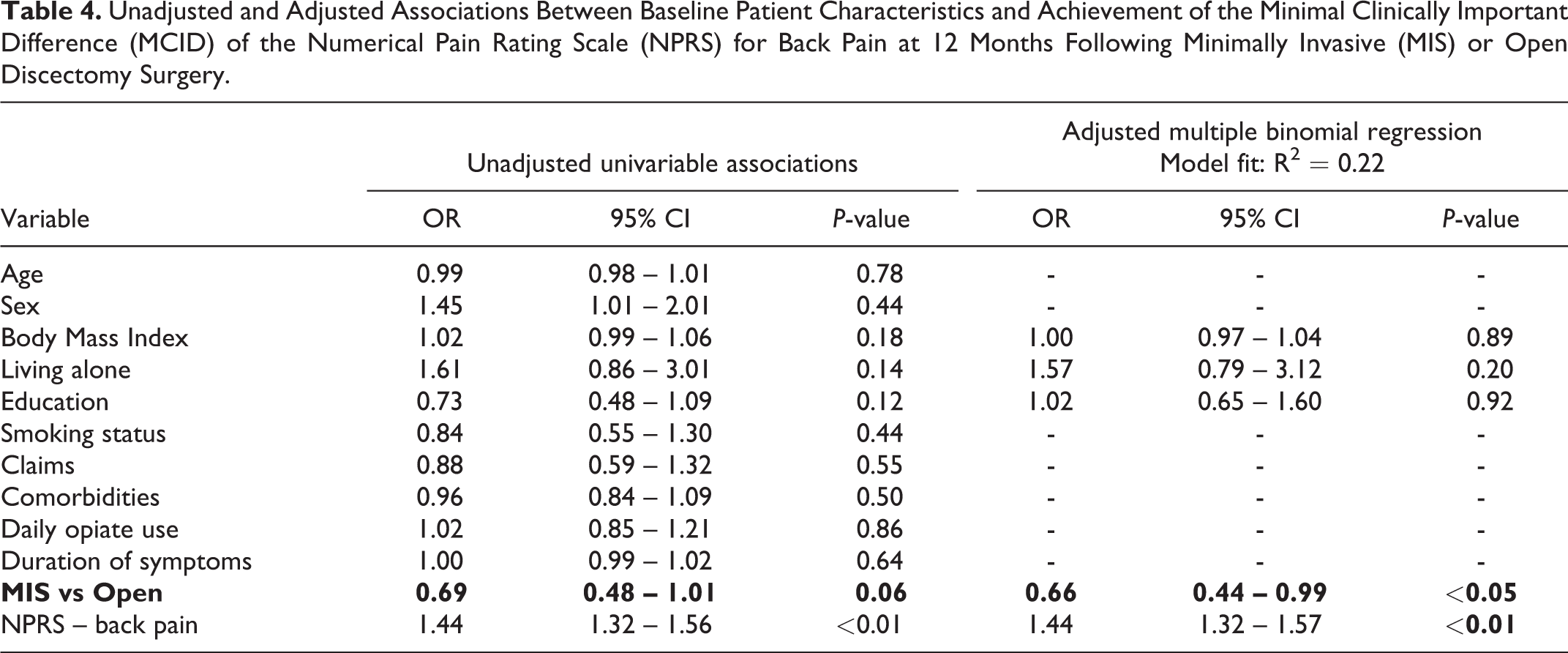
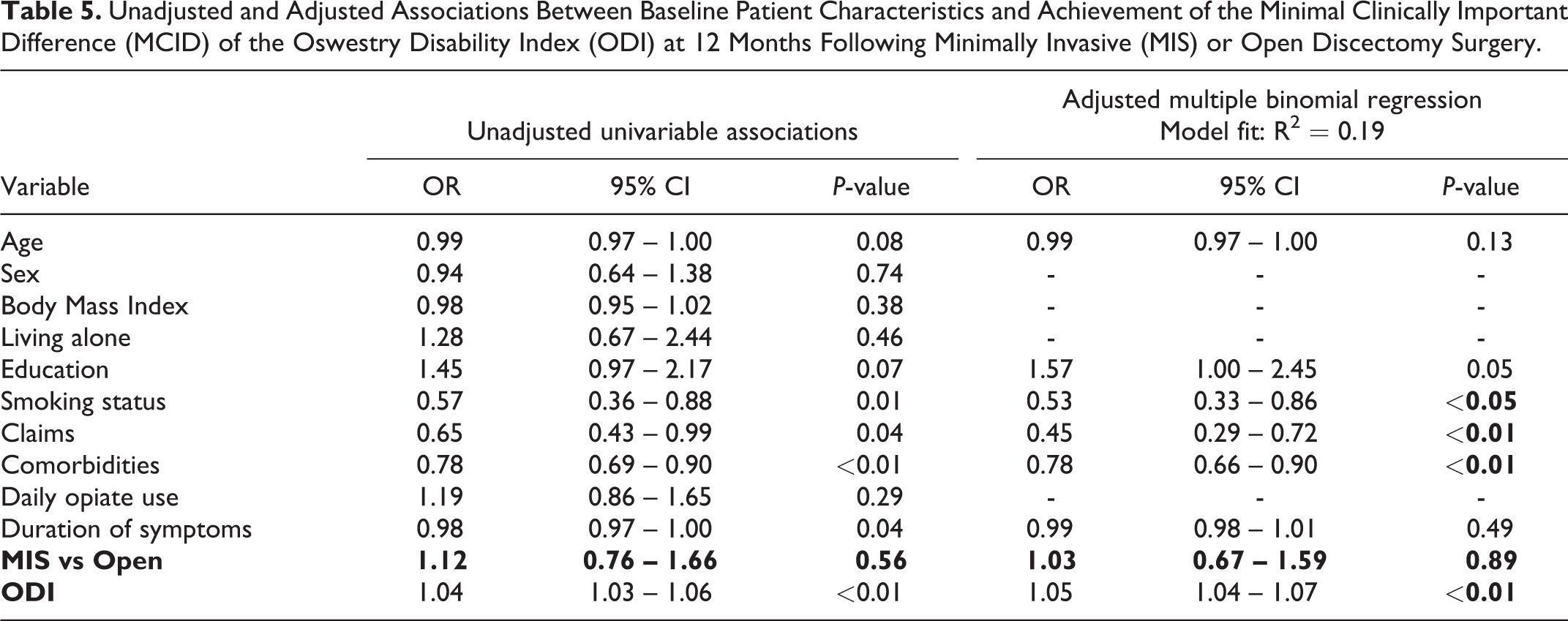
In regression analyses that adjusted for potential confounders by baseline characteristics (Tables 3-5), MIS technique was associated with a significantly reduced odds of achieving the MCID for back pain in comparison to open technique (OR 0.66, 95% CI 0.44 to 0.99, P < 0.05, Table 4), but there were no differences for leg pain or ODI at 12 months. Worse baseline disability (higher ODI score; OR 1.05, 95% CI 1.04 – 1.07, P < 0.01), current smoking (OR 0.53, 95% CI 0.33 – 0.86, P < 0.05), presence of disability or insurance claims (OR 0.45, 95% CI 0.29 – 0.72, P < 0.01), and number of comorbidities (OR 0.78, 95% CI 0.66 – 0.90, P < 0.01) were each inversely associated with achieving the MCID for ODI.
Unadjusted and Adjusted Associations between Baseline Patient Characteristics and Achievement of the Minimal Clinically Important Difference (MCID) of the Numerical Pain Rating Scale (NPRS) for Leg Pain at 12 Months Following Minimally Invasive (MIS) or Open Discectomy Surgery.
Unadjusted and Adjusted Associations Between Baseline Patient Characteristics and Achievement of the Minimal Clinically Important Difference (MCID) of the Numerical Pain Rating Scale (NPRS) for Back Pain at 12 Months Following Minimally Invasive (MIS) or Open Discectomy Surgery.
Unadjusted and Adjusted Associations Between Baseline Patient Characteristics and Achievement of the Minimal Clinically Important Difference (MCID) of the Oswestry Disability Index (ODI) at 12 Months Following Minimally Invasive (MIS) or Open Discectomy Surgery.
There were no significant differences between techniques for leg pain, back pain, or ODI in subgroup analyses that included only patients with BMI greater than 30.
There were also no significant differences between groups for patient-reported satisfaction, with 87% of MIS patients reporting being either “extremely” or “somewhat” satisfied at 12 months compared to 84% of Open patients (P = 0.38), and 87% of MIS patients reporting feeling “much better” or “better” compared to 84% of Open patients (P = 0.44). When asked if they would choose to have surgery again, 87% of MIS patients reported “definitely yes” or “probably yes” compared to 89% of Open patients (P = 0.64).
We observed statistically significant differences that favored the MIS technique for each of operating time (72 min (SD 30) versus 94 min (SD 41), P < 0.01), estimated blood loss (38 mL (SD 37) versus 77 mL (SD 71), P < 0.01), and length of stay in hospital (median 0 days (IQR 0 to 0) versus 1 day (IQR 0 to 1), P < 0.01) (Table 6). Seventy-three percent of patients who underwent MIS surgery had their operation performed as day surgery in comparison to 40% of patients who underwent open surgery (Figure 4).
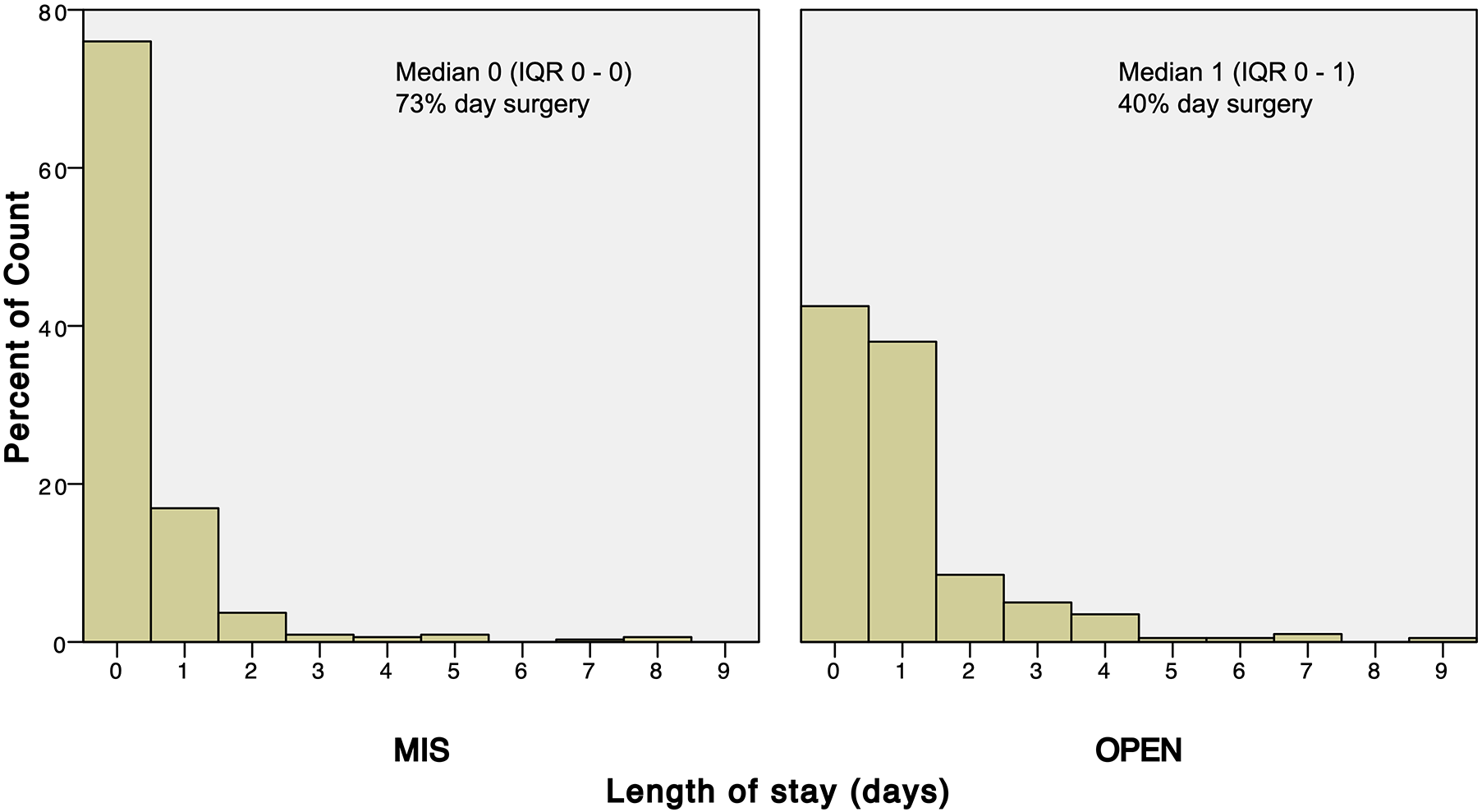
Length of stay among patients who underwent minimally invasive (MIS) tubular lumbar discectomy (n = 339) or conventional open (OPEN) lumbar discectomy (n = 211). Zero days denotes day surgery
Peri-Operative Outcomes and Adverse Events At Up to 12 Months Following Minimally Invasive (MIS) or Open Discectomy Surgery.
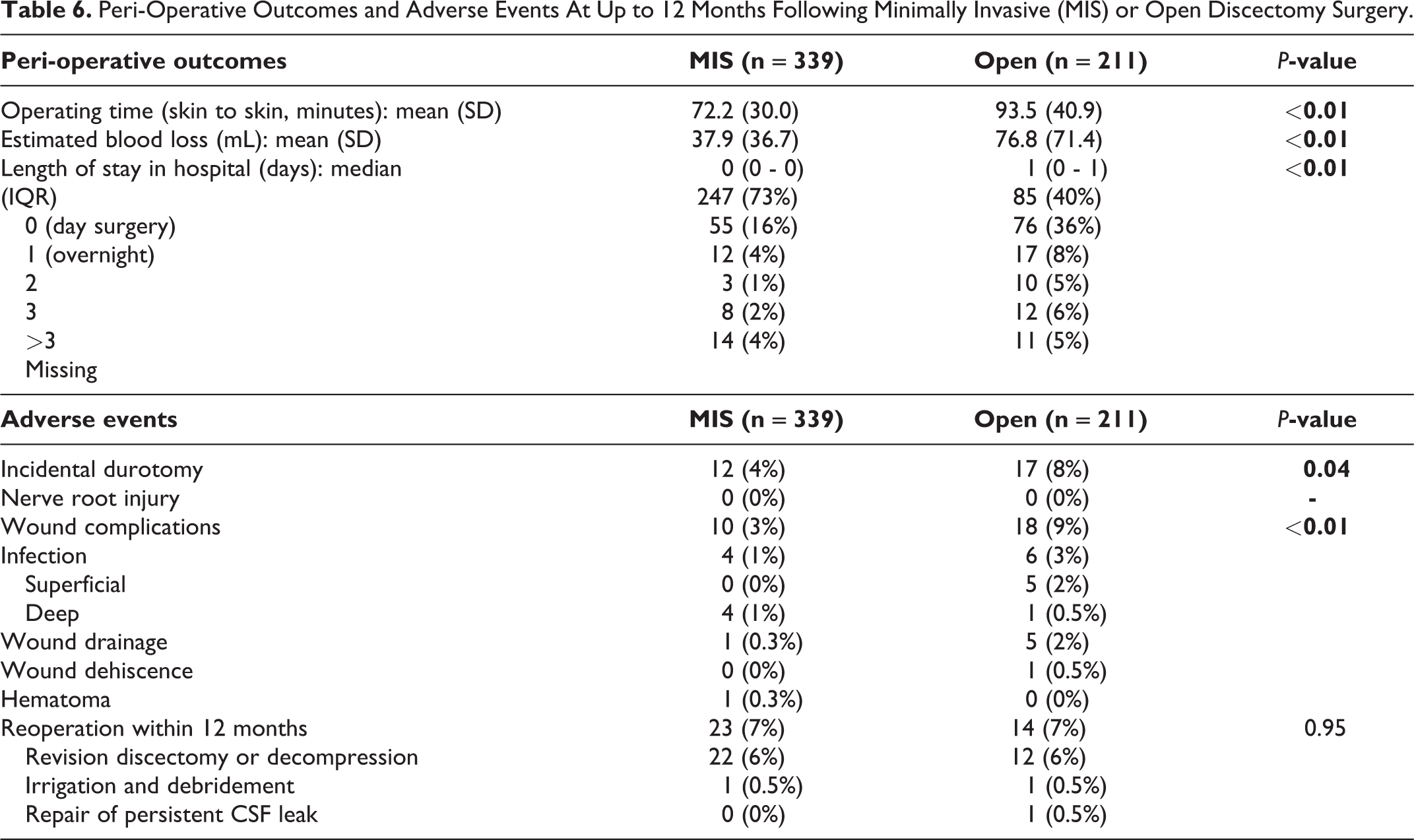
We also observed statistically significant differences that favored MIS for rates of incidental durotomy (4% vs 8%, P = 0.04) and the composite outcome of all wound complications (3% vs 9%, P < 0.01; Table 6). There were 4 patients with post-operative infections in the MIS group (1%) in comparison to 6 (3%) in the Open group, and there were 2 patients (1%) with excessive wound drainage, dehiscence or hematoma in the MIS group in comparison to 6 (3%) in the Open group. However, we did not observe a significant difference between groups for total rates of reoperation for all reasons at up to 12 months of follow-up. Across the entire cohort, there were 37 reoperations (7%; Table 6): 34 for revision discectomy or decompression (6%), 2 for irrigation and debridement (<1%), and 1 for repair of a persistent CSF leak (<1%).
Discussion
We performed an observational study to determine the effectiveness of MIS tubular techniques in comparison to conventional open surgery for lumbar discectomy in routine Canadian clinical practice. We did not identify significant differences between groups for patient-reported leg pain, back pain, disability, function, and satisfaction at up to 12-months after surgery, except that MIS technique was associated with a significantly reduced odds of achieving the MCID for back pain in comparison to open technique after adjusting for potential confounders. We observed statistically significant differences which were of relatively small magnitude favoring the MIS technique for each of operating time, estimated blood loss, length of stay in hospital, rates of incidental durotomy, and wound-related complications; but not for overall rates of reoperation. We also found that smoking, the presence of disability and insurance claims, and number of comorbidities were independently associated with greater post-operative disability independent of technique.
Strengths and Limitations
We have previously discussed many strengths and limitations of the CSORN research platform and dataset.17,18,20,21 Important strengths include prospective collection of patient-reported outcomes, “real world” generalizability to multiple centers and practice settings, implementation of MCIDs to aid in interpretation of treatment effects, and prospective reporting of adverse event data to fully inform the balance of both desirable and undesirable treatment effects. Important limitations include that detailed technical data were not available (such as use of microscope versus loupes, size of incisions, size or specific details of tubular and open retractors, and administration of surgical and peri-operative co-interventions), and that almost one third of potentially eligible patients had to be excluded because of missing follow-up data. Although missing data clearly threaten the validity of any analyses, we have previously shown that excluded CSORN patients do not have identifiable differences in baseline characteristics, disease severity, or interim follow-up when available.17,20,21 Similarly, there was no difference in baseline characteristics between patients with missing data and those with complete data in this study.
Our sample size was determined by convenience rather than an a priori power analysis, but conventional estimations applied post hoc confirm that a study of this size is more than adequately powered to detect differences in the patient-reported outcomes by at least the MCIDs (i.e. mean difference 1.6 for leg pain, SD 3.2, alpha 0.05, beta 0.2 yields n = 63 in each group). 29 However, our study was underpowered to reliably detect important differences in rates of adverse events. Our findings of greater improvements among patients with worse baseline leg pain, back pain, and disability may suggest ceiling effects inherent to the patient-reported outcome measures or could represent a regression toward the mean phenomenon.
This study may be at risk of selection bias due to its observational design, but we suggest the potential effect of this bias was probably minimal. While it is plausible that surgeons could preferentially treat cases with greater apparent technical complexity or supervise learners via open techniques, which would lead to worse outcomes and greater adverse events such as dural tears in the open group, we excluded patients undergoing revision and multi-level procedures and we observed that distributions of baseline characteristics (including BMI) did not differ between groups. Further, we did not identify any apparent effect in favor of the MIS group for patient-reported outcomes and the differences in rates of adverse events were small.
This study may also be at risk for a unique type of bias known as differential expertise bias, but we suggest that our observational design protected against this. Differential expertise bias is unique to studies of technical procedures, and it occurs when the expertise with which interventions are delivered is systematically greater in one group or the other.30,31 It most commonly occurs when surgeons have variable experience with a novel procedure, and differences in their expertise - rather than the procedure itself – influence patient outcomes. Variable expertise can also limit generalizability if the expertise within a study is substantially greater or less that that in one’s own practice setting. 32 It seems most likely that surgeons in an observational study who were more familiar, experienced, and confident with tubular retractors would have been more likely to offer MIS surgery to their patients (and vice versa), but we did not collect data about surgeon expertise to evaluate this possibility.
Relation to Prior Literature
Our study adds to a relatively focused body of literature, which has been summarized in several recent systematic reviews.1,6,9,33,34 The single largest randomized controlled trial was reported by Arts et al in 2009, and it involved 328 patients who were allocated to tubular discectomy or conventional microdiscectomy.7,8 There were no clinically important differences between groups for leg pain or disability at up to 5 years follow-up, and there were also no significant differences in rates of intra-operative or post-operative complications or long-term reoperations. The average length of stay was 3.3 days in both groups, which presumably represents a different era of peri-operative care or a different practice environment. A recent survey of Canadian neurosurgeons found that the tubular retractors were the preferred choice of 33% of respondents. 35 Others have demonstrated variable implementation of MIS techniques globally. 36 We interpret the best available evidence to date has as having not yielded a distinct advantage for MIS with regard to infections or deep infections. The Arts et al randomized controlled trial and a prior systematic review of all data from randomized controlled trials both failed to identify a statistically significant advantage in favor of MIS with regard to infection.1,8
We believe that our observed rates of non-same day discharges reflect actual practice patterns across the Canadian hospital setting of this study. First, these results are unlikely to be a spurious or misleading finding because length of stay data was recorded prospectively by research coordinators. Second, a recent survey of Canadian surgeons who perform lumbar discectomy asked “If there are no complications, when do you discharge from hospital?” and found that only 59% routinely discharged same day, while 39% routinely discharged next day. 35 We acknowledge that these rates may differ from those published from some other settings, but we also note considerable variability in the literature. For example, a recent retrospective review of prospectively collected registry data from a large academic hospital in the United States reported 90% outpatient procedures, 37 but an analysis of administrative data from over 50 000 patients in the United States reported a mean length of stay of 1.83 days after open microdiscectomy. 38 A pilot study of 58 patients in a developing country reported a 100% success rate of same day discharge. 39
Our finding of greater residual back pain among the MIS group in our adjusted analysis may seem counter-intuitive, but it was previously reported by Arts et al in a secondary paper from their trial, in which serum creatine phosphokinase (CPK) and the cross-sectional area (CSA) of the multifidus muscle on magnetic resonance imaging were compared as measures of muscle injury. 40 They found no significant differences for CPK, but a significantly greater loss of relative CSA and significantly greater 1-year back pain among MIS patients. These results could relate to trauma caused by traversing the paraspinal muscles rather than detaching their insertions, or to denervation of the muscle, facet joint, and other local structures in the open approach.
Most prior studies have failed to identify a consistent advantage for MIS discectomy with respect to back pain. There were no significant differences between groups for back pain in systematic reviews and meta-analyses reported by each of Alvi et al, 33 Li et al, Kamper et al, 41 and Evaniew et al 1 , and a Cochrane review reported by Rasouli et al actually found low-quality evidence that various minimally invasive techniques including tubular discectomy were associated with worse back pain in comparison to open surgery at 6-months (mean difference 0.35, 95% CI 0.19 to 0.51) and 2 years (mean difference 0.54, 95% CI 0.29 to 0.79) of follow-up. 34
A more recent study by Takahashi et al showed point estimates suggesting slightly greater back pain among tubular discectomy patients both while sitting and while in motion, but these differences were not statistically significant. 42 This study also found that back pain after discectomy was significantly greater among patients who experienced changes in Pfirrmann grade or Modic type on MRI at one year of follow-up. We did not measure these variables or routinely obtain post-operative MRIs in our study. Increased back pain after lumbar discectomy has also been reported in association with aggressive disc removal versus limited sequestrectomy, with a trade-off of higher recurrent disc herniations after limited sequestrectomy.43,44 We did not collect data to evaluate for differences in extent of discectomy between techniques in this study.
Implications
From a clinical point of view, our results suggest that surgeons and their patients can expect similar improvements in leg pain and disability after MIS and open techniques for lumbar discectomy at up to 12 months, and that strong recommendations in favor of one technique over the other are probably not warranted. Although we observed more incidental durotomies and wound complications in the open group, the overall rate of reoperations was not increased and there were no differences in patient-reported leg pain, disability, or satisfaction. Further, the differences in adverse event rates were small and confidence in them is limited by few outcome events and statistical fragility.45,46 We interpret the difference in blood loss (39 mL) as unlikely to be clinically important, but the differences in operating time (21 minutes) and in rates of same-day discharge (MIS 73% versus open 40%) may be important to some stakeholders. 47 Given that many centers routinely perform MIS and open discectomy as day surgery, this latter finding suggests an opportunity to develop or improve peri-operative day surgery care pathways regardless of surgical technique. 48 Differences in rates of same-day discharge could result from differences in surgeon preferences, whereby those inclined to perform MIS discectomy also favor day surgery.
From a research point of view, our data suggest that tubular and conventional discectomy can be considered equivalent comparators in clinical trials and meta-analyses for other interventions, such as spinal endoscopy. 49 Further research is warranted to clarify rates of uncommon adverse events and their risk factors, and larger observational studies from administrative datasets may have some merit for this purpose. 50 Our study does not inform about the potential advantages or disadvantage of using tubular retractors for cases with greater technical complexity and patient morbidity, such as multi-level degenerative, deformity, trauma, and/or oncology procedures.51-53
Conclusions
In comparison to those treated with conventional open techniques, patients who underwent MIS tubular lumbar discectomy experienced similar improvements of leg pain and disability at up to 12 months with no difference in rates of reoperation, but were less likely to experience improvement of associated back pain. Small differences favored MIS for operating time, blood loss, and adverse events but may have limited clinical importance. Variable lengths of stay suggest an opportunity to improve peri-operative care pathways regardless of technique.
Footnotes
Baseline Characteristics of 247 Patients Who Underwent Minimally Invasive or Open Lumbar Discectomy Surgery, but Were Excluded From the Study Cohort due to Incomplete Follow-Up.
| Variable | |
|---|---|
| Age: mean (SD) | 42.7 (13.7) |
| Sex (males) | 139 (56%) |
| Body Mass Index: mean (SD) | 28.0 (5.5) |
| Living alone | 30 (12%) |
| Education (post-secondary or greater) | 194 (78%) |
| Smoking status (current smoker) | 70 (28%) |
| Current disability or insurance claims (yes) | 64 (25%) |
| Number of comorbidities: mean (SD) | 2.1 (1.6) |
| Pre-operative daily opioid use (yes) | 137 (55%) |
| Duration of symptoms | |
| Less than 6 weeks | 9 (4%) |
| Less than 3 months | 14 (6%) |
| 3 to 6 months | 35 (14%) |
| 6 to 12 months | 56 (23%) |
| 1 to 2 years | 52 (21%) |
| Greater than 2 years | 81 (33%) |
| Pre-operative Patient-Reported Outcome Measures | |
| Numerical Pain Rating Scale - leg pain: mean (SD) | 7.7 (2.1) |
| Numerical Pain Rating Scale - back pain: mean (SD) | 6.5 (2.5) |
| Oswestry Disability Index: mean (SD) | 49.6 (16.6) |
| Short Form 12 - Physical Component Summary | 32.3 (8.0) |
| Short Form 12 - Mental Component Summary | 45.3 (1.8) |
| Level of disc herniation | |
| L1-L2 | 0% |
| L2-L3 | 1% |
| L3-L4 | 4% |
| L4-L5 | 38% |
| L5-S1 | 56% |
| MIS | 138 (56%) |
| Open | 109 (44%) |
Acknowledgement
The authors thank all of the subjects who participated in the study and the support and research coordinator staff and investigators from the Canadian Spine Outcomes and Research Network (CSORN) contributing sites.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No funds were received in direct support of this work. The Canadian Spine Outcomes and Research Network (CSORN) is funded by the Canadian Spine Research & Education Foundation (CSREF) fund grant. CSREF had no involvement in the development of this study, analysis or interpretation of data, writing of the manuscript, or decision to submit for publication.
Research Ethics Board Approval
This study was approved by the Research Ethics Boards at each participating institution (approval numbers not applicable): University of Calgary, Canada East Spine Centre, University of Toronto, Universite Laval, Western University, University of Ottawa, Northern Ontario School of Medicine, McGill University, University of Manitoba, and University of British Columbia.