
Abstract
Study Design
Retrospective Upright MRI Study.
Objectives
Determine the relationship between lumbar disc herniation and presence of the nerve root sedimentation sign on upright kinematic MRI patients.
Methods
T2-weighted axial upright kMRI images of 100 patients with the presence of disc herniation in at least 1 lumbar disc between L1/L2 and L5/S1 were obtained. Sedimentation sign, spinal canal anterior-posterior (AP) diameter, disc height, disc herniation size, type of herniation, and zone of herniation were evaluated. A positive sedimentation sign was defined as having either the majority of nerve roots running ventrally or centrally in the canal or conglomeration of the nerve roots at the mid-disc level. Herniation types were defined as either no herniation, disc bulge, protrusion, extrusion, or sequestration. Zones of herniation were categorized as either central, lateral, or far lateral.
Results
The kappa value of intra-observer reliability was .915. The kappa value of disc levels with a negative sedimentation sign were seen more frequently (n = 326, 65.2%) than those with a positive sedimentation sign (n = 174, 34.8%). The spinal canal AP diameter was significantly decreased at the L3/L4 and L4/L5 level in patients with a positive sedimentation sign. Discs with a positive sedimentation sign had a larger average size of disc herniation compared to those with a negative sign at all levels. A relationship between positivity of the sedimentation sign and disc herniation type was significant at L2/L3, L3/L4, and L4/L5.
Conclusions
Patients with a positive sedimentation sign were seen to have larger disc herniations and more severely degenerated discs.
Introduction
Lumbar spinal stenosis (LSS) is defined as a degenerative condition leading to narrowing of the spaces surrounding neurovascular structures of the spinal canal and is the most common reason for spine surgery in those over 65 years. 1 LSS cannot be diagnosed on clinical symptoms alone; however, imaging studies, such as magnetic resonance imaging (MRI), can confirm the diagnosis by demonstrating narrowing of the spinal canal diameter. 2 The sedimentation sign, first described by Barz et al, has also been shown to be a radiological marker to rule in patients with clinically symptomatic LSS. In those patients needing operative treatment for LSS, a positive sedimentation sign was found to be a better predictor for operative success compared with those with a negative sedimentation sign. 3
A negative sedimentation sign is seen when the nerve roots sediment dorsally in the spinal canal. A positive sedimentation sign is seen when the nerve roots are displaced centrally or ventrally in the spinal canal. In a supine MRI, gravity plays a major role in the dorsal sedimentation.4,5 The sedimentation sign was initially noted only in supine MRI studies, but recent studies have shown that the sedimentation sign may be valid in predicting symptomatic lumbar spinal stenosis in the upright position as well. 6 It is suggested that a positive sedimentation sign may occur due to increased epidural pressure leading to the tethering of nerve roots. 7
Lumbar disc herniation is the most common degenerative diagnosis of the lumbar spine and is the most common overall cause for lumbar spinal surgery. 8 Herniated discs can cause compression of the spinal canal leading to impingement of the nerve roots. Supine MRI studies have shown that the incidence of a positive sedimentation sign is most seen in patients with central or combined disc lumbar stenosis but may also be seen in patients with posterolateral disc herniations. 9
Upright MRIs allow the spine to be visualized under weight-bearing conditions similar to what one may experience when sitting or standing. Due to alterations in the position of loading on the spine between the standing and supine positions, there may be differences in spinal canal dimensions, such as anterior-posterior (AP) diameter and cross-sectional area (CSA). Prior studies have found that in patients with paracentral disc herniations, there was an increase in nerve root compression seen during the standing MRI evaluation compared with the supine MRI evaluation. 10 This may be attributed to a decrease in spinal canal (CSA) in the standing position.11,12
Both LSS and lumbar disc herniations can lead to dural sac compression and nerve root impingement. However, few studies have examined the relationship between lumbar disc herniation and sedimentation sign. The goal of this study was to further determine if there exists a relationship between lumbar disc herniation and the presence of a sedimentation sign on multi-positional MRI studies in the upright position.
Materials and Methods
This study was a retrospective imaging study approved by the Institutional Review Board (HS-14-00 397). Patients with nonspecific back pain were imaged with a multi-positional MRI from periods 11/1/2018 to 1/1/2019 and 3/1/2022 to 5/1/2022. Only patients with disc lesions between segments L1/L2 and L5/S1 were included. Patients with a prior history of spine surgery, infection, trauma, tumor, spinal inflammatory disease, and congenital anomaly were excluded from the study. 100 consecutive patients (62 male, 38 female) with a mean age of 50.5 ± 14.8 were included in the study.
A .6-T MRI machine (Upright Multi-Position, Fonar Corporation, New York, NY, USA) was used to obtain T1-weighted (repetition time 671 milliseconds, echo time 17 milliseconds, thickness 4.0 mm, field of view 30 cm, matrix 256_224, NEX 2) and T-2 weighted spin echo (repetition time 3000 milliseconds, echo time 140 milliseconds, thickness 4.0 mm, field of view 30 cm, matrix 256_224, NEX 2) multi-positional images of the lumbar spine. Only T2-weighted upright images of patients in the neutral position were used in this study. Images of the sagittal and axial plane were used for measurements. All images were obtained and measured by using the Lifetrack medical system (version 2, Lifetrack Medical Systems Pte. Ltd, Singapore, Singapore).
Measurements of the sedimentation sign were taken at the mid-slice image of each patient on a T2-weighted axial image from the L1/L2 to L5/S1 disc level. The sedimentation sign was assessed at the disc level rather than at the pedicle level as in Barz’s initial report of the sedimentation sign, because all patients in the study had the maximal level of stenosis at the disc level. This also corresponds with the measurements of the AP diameter at the disc level.
A negative sedimentation sign was defined as having greater than 50% of the visible nerve roots located either dorsally (Figure 1A) or dorso-laterally (Figure 1B) in the spinal canal at the mid-disc level. A positive sedimentation sign was defined as having the majority of nerve roots running either ventrally (Figure 1C) in the canal at the mid-disc level. If the nerve roots were conglomerated, it was also considered a positive sedimentation sign (Figure 1D).13,14 Left to right: (A) Dorsal pattern, (B) dorso-lateral pattern, (C) ventral pattern, (D) conglomeration pattern.
The spinal canal anterior-posterior (AP) diameter was measured at the mid-disc slice on axial images. While there is no standardized radiological criteria for measurement of LSS, measurement of the spinal canal AP diameter is often used.1,15 A Delphi Survey noted AP Diameter as the highest rated quantitative criteria used for measurement of LSS, and thus has been the method used to measure stenosis in this study.
16
The spinal canal AP diameter was measured using the method described by Linkoaho et al
17
(Figure 2). Spinal canal AP diameter measurement.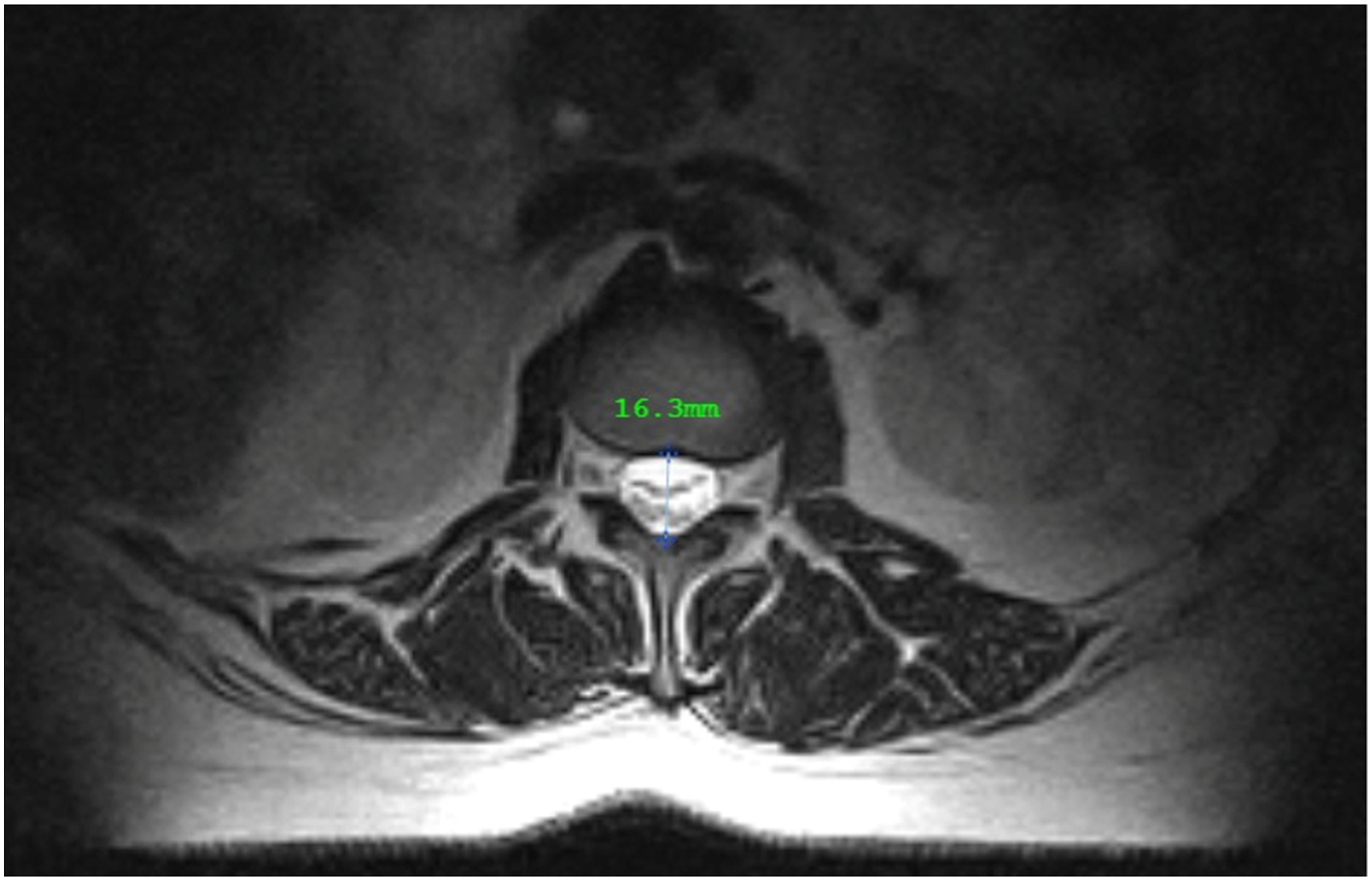
Disc herniation measurements were made on the axial image at the level of maximal compression of the spinal canal. The anterior-posterior measurements represented the maximum length that the disc lesion impinged onto the spinal canal as outlined in Carragee and Kim’s method of disc lesion measurements. 18 The location of disc lesions was described as an adaptation of the Michigan State University (MSU) classification of disc herniations. Three zones were created, with zone A representing the region between a perpendicular line lying on the spinous process to halfway between the spinous process and the facet joint. Zone B represents the lateral region from zone A to the facet joint. Zone C represents any lesion that lies lateral to the facet joint. 19 Disc lesion types were categorized into 4 categories per North American Spine Society (NASS) criteria: bulge, protrusion, extrusion, sequestration. 20 A disc bulge was defined as having greater than 25% of the disc circumference extending less than 3 mm from the apophyses edge. A protrusion was defined as having less than 25% of the disc circumference herniated, with the base of the herniation wider than the herniation. An extrusion was defined as having less than 25% of the disc circumference herniated with the base of the herniation narrower than the herniation. Lastly, a sequestration was defined as having herniated disc material that has been separated and is no longer attached to the disc. Discs with a simultaneous herniation and disc bulge not seen in the study.
Disc lesion measurements including size, location, and type were measured by an orthopedic spine surgeon. All other measurements were made by a second observer made independently of measurements by the first observer. To determine the intra-observer reliability of measurements, 10 patients with a total of 50 T2-weighted axial images were randomly collected from 100 patients and re-assessed by the same researchers who made the initial measurements.
Independent student t-test was used to evaluate the difference in spinal canal AP diameter and amount of disc herniation between positive and negative sedimentation signs. The chi-square test was used to evaluate whether a potential relationship exists between the sedimentation sign and (1) Pfirrmann grade, (2) herniation type, and (3) herniation zone. Cohen’s kappa values were calculated to assess the intra-observer reliabilities. All analyses were performed using SPSS 21.0 (IBM Corp, Chicago, IL, USA). A P-value <.05 was considered as statistically significant.
Results
Based on the randomly selected 10 patients with a total of 50 T2-weighted axial images, the intra-observer reliability was .915.
Distribution of Sedimentation Signs at Disc Levels From L1/2 to L5/S1.

Distribution of Pfirrmann Grades at Disc Levels From L1/2 to L5/S1.
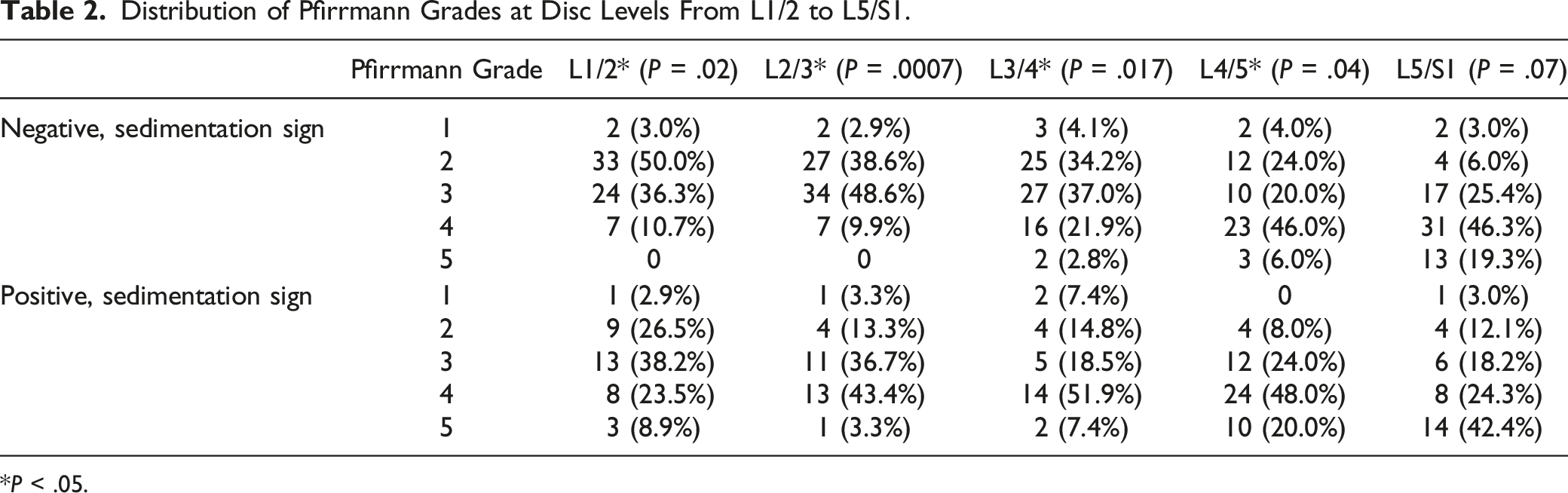
*P < .05.
Compared to discs with negative sedimentation signs, positive sedimentation signs were found to have significantly decreased spinal canal AP diameter at L3/4 (18.68 ± 3.06 mm to 16.47 ± 3.53 mm, P < .01) and L4/5 (16.94 ± 3.39 mm to 15.46 ± 3.14 mm, P < .05, Figure 3). Spinal canal antero-posterior Diameters (mm) between positive and negative sedimentation sign.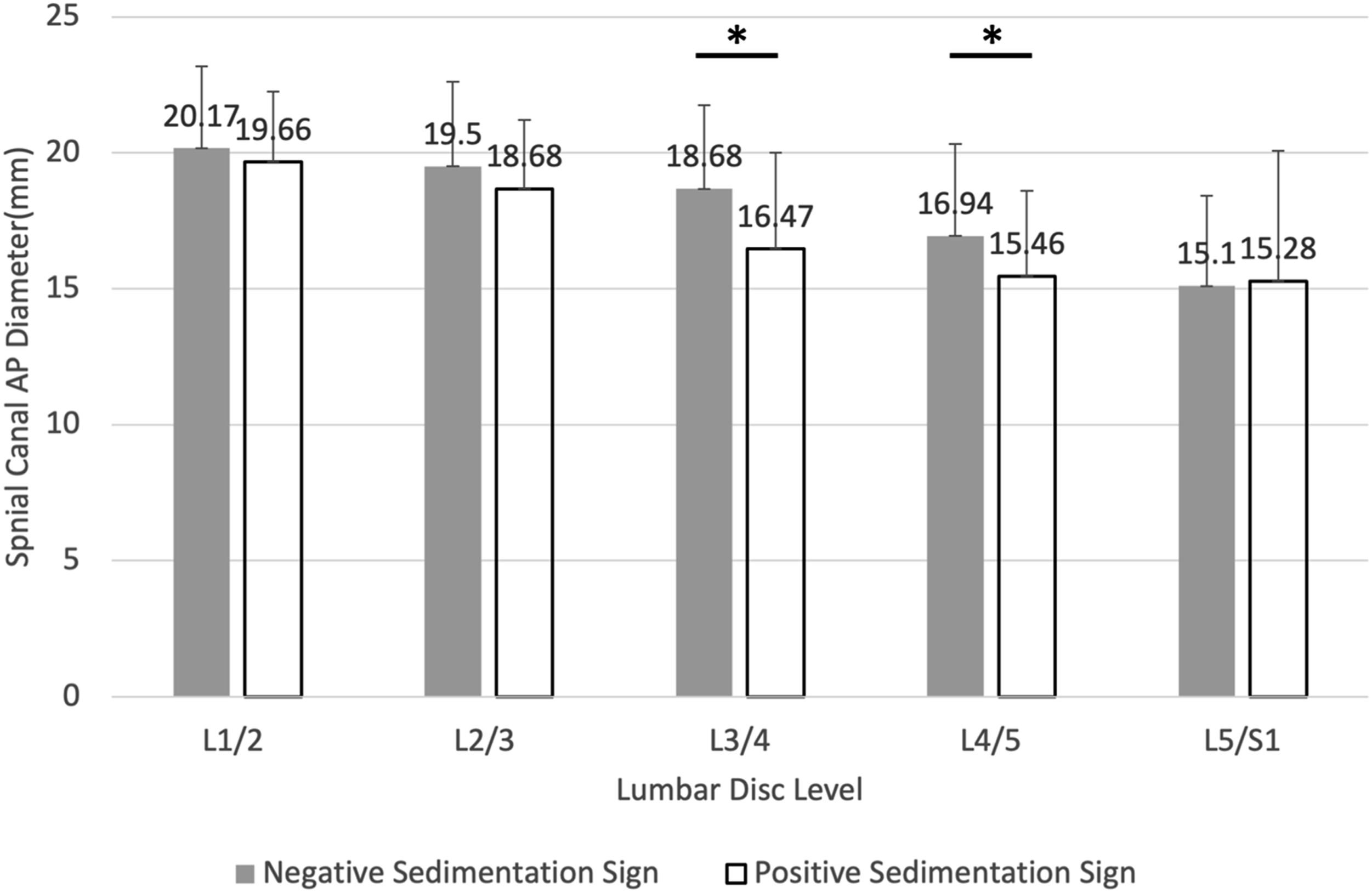
Amount of Disc Herniation (mm) Between Positive and Negative Sedimentation Sign.

*P < .05.
Distribution of Herniation Types Between Positive and Negative Sedimentation Sign.
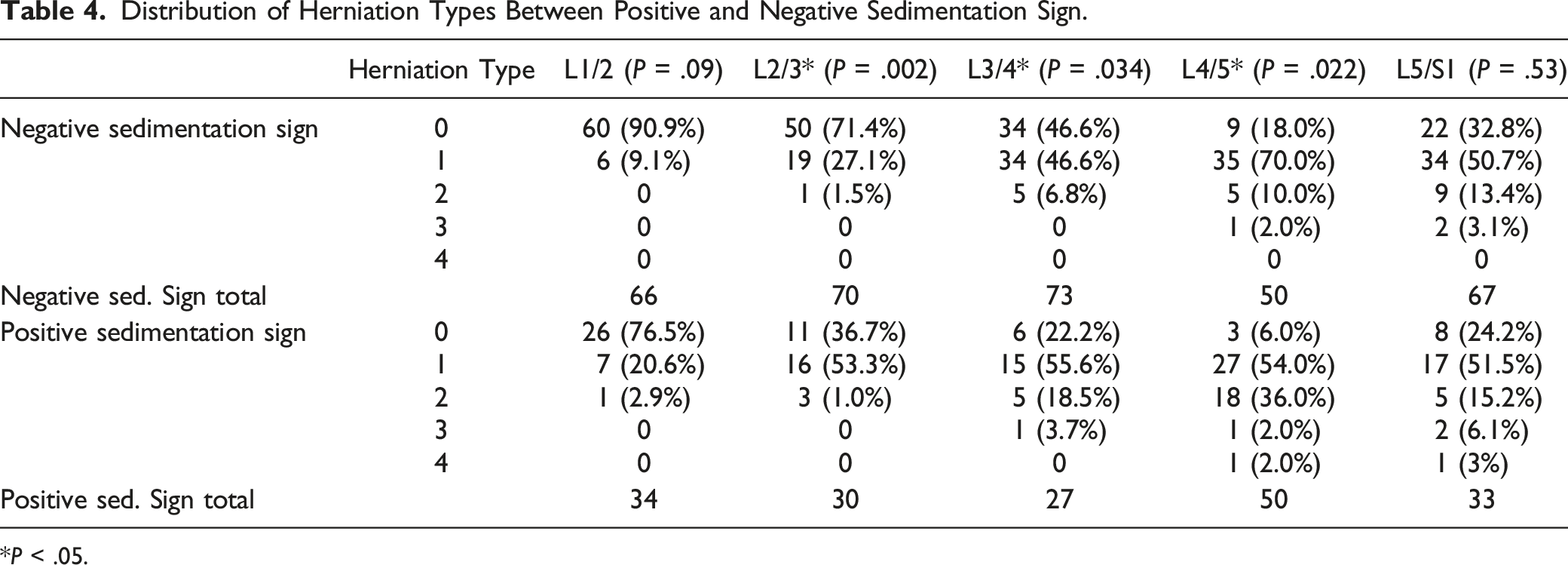
*P < .05.
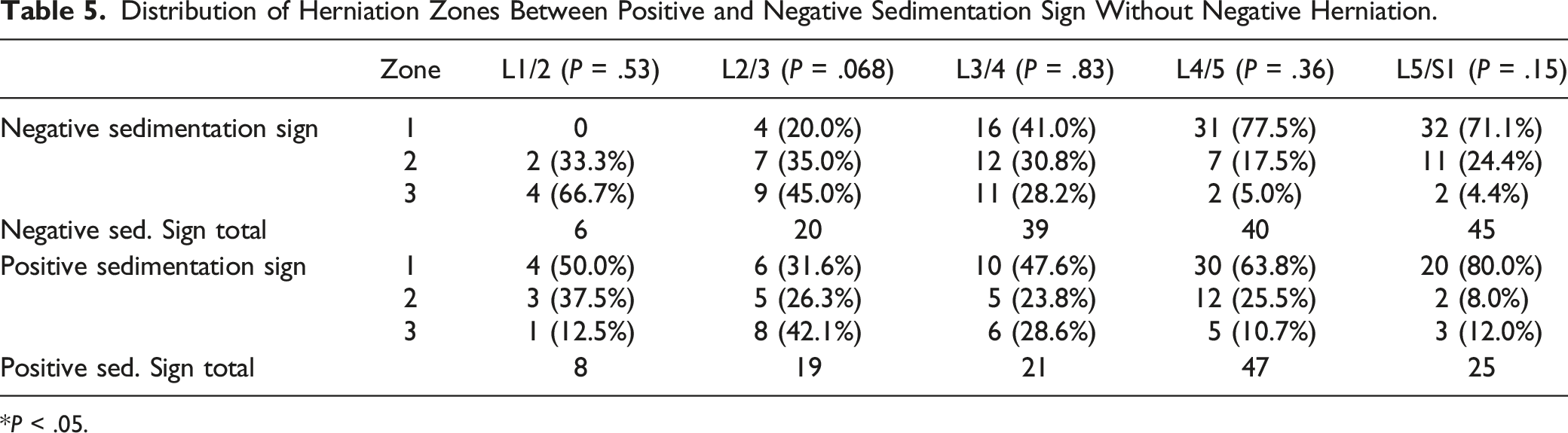
Distribution of Herniation Zones Between Positive and Negative Sedimentation Sign Without Negative Herniation.
*P < .05.
Discussion
Barz et al introduced the nerve root sedimentation sign in 2010 as an imaging marker to help diagnose lumbar spinal stenosis. Since then, the sedimentation sign has been widely used to diagnose and evaluate the outcome of surgical treatment in patients with clinically symptomatic LSS.4,7,13,21 Several studies have since reported that the sedimentation sign exhibits high specificity and sensitivity for the diagnosis of severe LSS and can be recommended as an auxiliary index for the diagnosis and screening of LSS.22,23
Disc herniations are a common cause of lower back pain due to external pressure on the dural sac from a herniated nucleus pulposus, leading to compression of the nerve roots. 21 The mechanism of the formation of a positive sedimentation sign in LSS is debated but is believed to be due to compression of the dural sac leading to nerve root displacement to the ventral side of the sac. 7 Both disc herniations and LSS have similar effects of compression on the spinal canal; however, the sedimentation sign has historically only been utilized as a diagnostic tool in LSS.
While there are few studies noting that LSS may occur secondary to lumbar disc herniation, there are no studies correlating the correlation between the 2.24,25 Additionally, this is the first examining the relationship between lumbar disc herniation and the sedimentation sign. As the sedimentation sign has been used to diagnose LSS, the presence of the sedimentation sign in patients with lumbar disc herniation may also indicate the presence of LSS. Patients in this study underwent upright MRI imaging, minimizing the effects gravity may have on dorsal positioning of the nerve roots.
At all measured levels, a higher Pfirrmann score was associated with an increased presence of a positive sedimentation sign (Table 2). The Pfirrmann grade is an imaging marker used to grade disc degeneration. 23 Intervertebral disc degeneration can lead to degenerative disc disease and lumbar disc herniation. 21 Results of this study agree with prior studies that degenerated discs are at higher risk for herniation.26,27
In this study, positive and negative sedimentation signs were seen at every disc level (Table 1). Furthermore, a positive sedimentation sign was correlated with a decreased spinal canal diameter at the L3/L4 and L4/L5 levels (Figure 3). At all disc levels except L5/S1, a positive sedimentation sign was associated with a larger average disc herniation compared to disc levels with a negative sedimentation sign (Table 3).
The association at L3/L4 and L4/L5 between a positive sedimentation sign and spinal canal AP diameter may be related to the similar effects of spinal canal compression in disc herniation and LSS. Furthermore, the relationship indicating larger disc herniations are more likely seen with a positive sedimentation sign is consistent with the suggested mechanism of increased external pressure causing a positive sedimentation sign. In this setting, a larger herniation of the nucleus pulposus leads to increased compression of the spinal canal and thus greater impingement of the nerve roots. This is the first study demonstrating a relationship between size of a disc herniation and spinal canal AP diameter in upright patients. However, prior studies have shown that in supine MRIs, patients with disc herniations leading to greatly decreased spinal canal AP diameters are more likely to present with cauda equina syndrome compared to those with less severe AP diameter narrowing. 22
A significant relationship between a positive sedimentation sign and spinal canal AP diameter was not seen at the L1/L2, L2/L3, and L5/S1 levels. Disc herniations at the L1/L2 and L2/L3 level are infrequent compared with herniations in the lower lumbar spine. Approximately 1-2% of lumbar disc herniations occur at the L1/L2 and L2/L3 level. 28 Furthermore, these herniations are more likely to lead to polyradiculopathies due to the narrower spinal canal at these levels and closer proximity to the conus medullaris. 28 These patients would have been unlikely to have undergone imaging in the outpatient setting, resulting in an increased number of patients without radicular symptoms being measured and potential explanation for a lack of association at these levels. At the L5/S1 level, nerve roots leave in a ventral pattern as opposed to dorsal in the levels above and the sedimentation sign may not be evaluated correctly leading to inability to note an association at this level. 14
This study showed no significant relationship between zones of herniation and presence of a positive or negative sedimentation root sign. This finding may be explained by relative herniation sizes. While herniations within zone A and B are in an anatomic position to cause direct spinal cord compression, larger herniations in zone C may also lead to dural sac compression. The sizes of zone C herniations were not measured in relation to foraminal diameter, and further studies may elucidate if larger lateral herniations have a similar effect on the presence of the sedimentation sign as central herniations do.
In this study, discs with a negative sedimentation sign were more likely to have no herniation compared with discs with a positive sedimentation sign at the L2/L3, L3/L4, and L4/L5 levels (Table 4). This finding agrees with the proposed mechanism of disc herniation causing spinal canal compression resulting in formation of a positive sedimentation sign. Furthermore, disc bulge and disc protrusion were the most common herniation types seen at levels with a positive sedimentation sign. While extruding and sequestering discs are known to cause radicular symptoms of nerve compression more often than bulging and protruding, this is not seen in this study and may be due to the small sample size and prevalence of extruding and sequestering discs in this population. 29
There are several limitations in this study. First, as this is a retrospective study for the patients with nonspecific back pain, multi-positional MRI protocols were not standardized, and MRI data was not available for all patients. Second, there is a limitation in that the association between the sedimentation sign and clinical symptom cannot be determined because there is no clinical assessment of patient symptoms or treatment course. Additionally, spinal canal diameters prior to disc herniation were unknown, thus it was not possible to determine percent change in patient AP diameter. Furthermore, measurement of spinal canal horizontal diameter, and therefore, cross-sectional area (CSA) was not performed. While AP diameter is sufficient for determination of LSS, CSA would be a useful additional measurement. Despite these limitations, this study is meaningful as the first study to investigate the relationship between lumbar herniated disc and sedimentation sign using upright MRI.
Conclusion
A positive sedimentation sign was more often seen in upright patients with increased severity of intervertebral disc degeneration, increased size of the herniated disc, decreased spinal canal AP diameters. No association was found between the location of the herniation and presence of the sedimentation sign. These findings are in agreement with the proposed mechanism of external compression of the dural sac leading to a positive sedimentation sign and validate the presence of the sedimentation sign in upright patients with lumbar disc herniations. A follow-up study relating the presence of disc herniation and a positive sedimentation sign to clinical symptoms such as pain level or radiculopathy and treatment course may elucidate further the clinical use and significance of the sedimentation sign in LDH.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.