
Abstract
Study Design:
Retrospective analysis of prospectively collected data.
Objective:
To identify modifiable factors associated with successful return to work 12 weeks following discectomy. Lumbar disc herniation is a common cause of sciatica and sick leave. This presents an economic burden to the individual and the society.
Methods:
Data from DaneSpine on a consecutive cohort of patients operated due to lumbar disc herniation during a 3-year period was identified and merged with data from the Ministry of Employment’s register on public welfare payments. Data on welfare payments 2 years prior to the date of operation and 1 year postoperative was included. Patients were considered to be on sick leave if they received welfare payments for the week. Patients are considered to have returned to work if they did not receive public welfare payments for a 4-week period.
Results:
Of 1134 patients meeting inclusion criteria, 98.5% had complete preoperative surgical data available. Postoperatively, 79.1% of the patients returned to the work within 12 weeks. Physically demanding jobs, low preoperative EQ5D score, and long duration of sick leave prior to surgery were associated negatively with return to work at 12 weeks.
Conclusion:
The results of this study indicate that patients who have a longer duration of sick leave have a physically demanding job and are in a poor health are more likely not to return to work by 12 weeks after surgery for lumbar disc herniation. Future studies are needed to determine if earlier referral to a surgeon leads to an earlier return to work.
Keywords
Introduction
Lumbar disc herniation (LDH) is a common low back disorder and the most frequent cause of sciatica.1,2 The natural history of sciatica is favorable, with spontaneous resolution of leg pain within 8 weeks in the majority of patients.
3
The treatment options for patients with prolonged symptoms are controversial, as the evidence comparing the effectiveness of surgical to nonsurgical treatment of symptomatic LDH are inconclusive. Focusing on clinical or radiographic outcomes in the Clinical Guidelines for Diagnosis and Treatment of Lumbar Disc Herniation with Radiculopathy published in 2012 by the North American Spine Society: Discectomy is suggested to provide more effective symptom relief than medical/interventional care for patients with lumbar disc herniation with radiculopathy whose symptoms warrant surgical intervention. In patients with less severe symptoms, surgery or medical/interventional care appear to be effective for both short- and long-term relief.
4
In Denmark, opportunities for registry-based research are unique, as data on public welfare payments, like sickness benefits, are registered on a weekly basis with the Ministry of Employment’s register, Danish Register for Evaluation of Marginalisation, called DREAM. 7 In addition, data on surgical treatment of LDH patients is registered on a daily basis in the Danish national spine surgical register, DaneSpine. 8 At our center, almost all patients (99%) scheduled for surgery for degenerative conditions of the lumbar spine are enrolled in DaneSpine. 9
The primary purpose of this study is to identify modifiable factors that are associated with successful return to work 12 weeks following discectomy using combined data from the DREAM database and DaneSpine.
Materials and Methods
This is a retrospective study of prospectively collected data from DaneSpine 8 and the DREAM database. Relevant approvals for the use of DaneSpine and DREAM data were obtained from the Danish Data Protection Agency (File Nr. 14/26 345 with Extension Nr. 18/22 270). The study was approved by the departments review board.
The study population comprised a consecutive cohort of patients aged between 17 and 62 years at the time of surgery undergoing discectomy at Danish Spine Center due to LDH during the period from June 1, 2010, to May 31, 2013. Patients who had previous low back surgery were excluded from the study. All patients had magnetic resonance imaging findings consistent with LDH at the level and side concordant with the patient’s symptoms, leg pain, or impaired neurologic function with or without pain. The surgical techniques varied between open discectomy with or without the use of microscope or magnifying surgical loupes depending on the surgeon’s preference.
Data from the DREAM database included weekly public welfare payments to the patients 2 years prior to the date of operation and 1 year postoperative. Patients are considered to have returned to work if they did not receive public sickness benefits for a 4-week period postoperative. Unemployed patients were included in the study, as the DREAM database differentiates between unemployment benefits and sickness benefits. To be eligible to receive unemployment benefits, citizens must be available for the job market by Danish law. During periods were they are unavailable due to illness patients receive sickness benefits.
Data collected from DaneSpine included preoperative patient reported data on age, gender, smoking, work load, pain medication, Oswestry Disability Index (ODI),10,11 EuroQol (EQ-5D),12,13 Short Form-36 Version 1, 14 Visual Analogue Scale (VAS) score (0 to 100) 15 for Back Pain and Leg Pain, and surgical data on level and type of surgery.
Statistical Analyses
All statistical analyses were performed using IBM SPSS version 25. For multivariate analyses, logistic regression was used and all factors that showed a potential influence (P < .05) in the bivariate analyses were included. The logistic regression models were also analyzed with a stepwise selection procedure, aiming at finding the most influential predictor.
Results
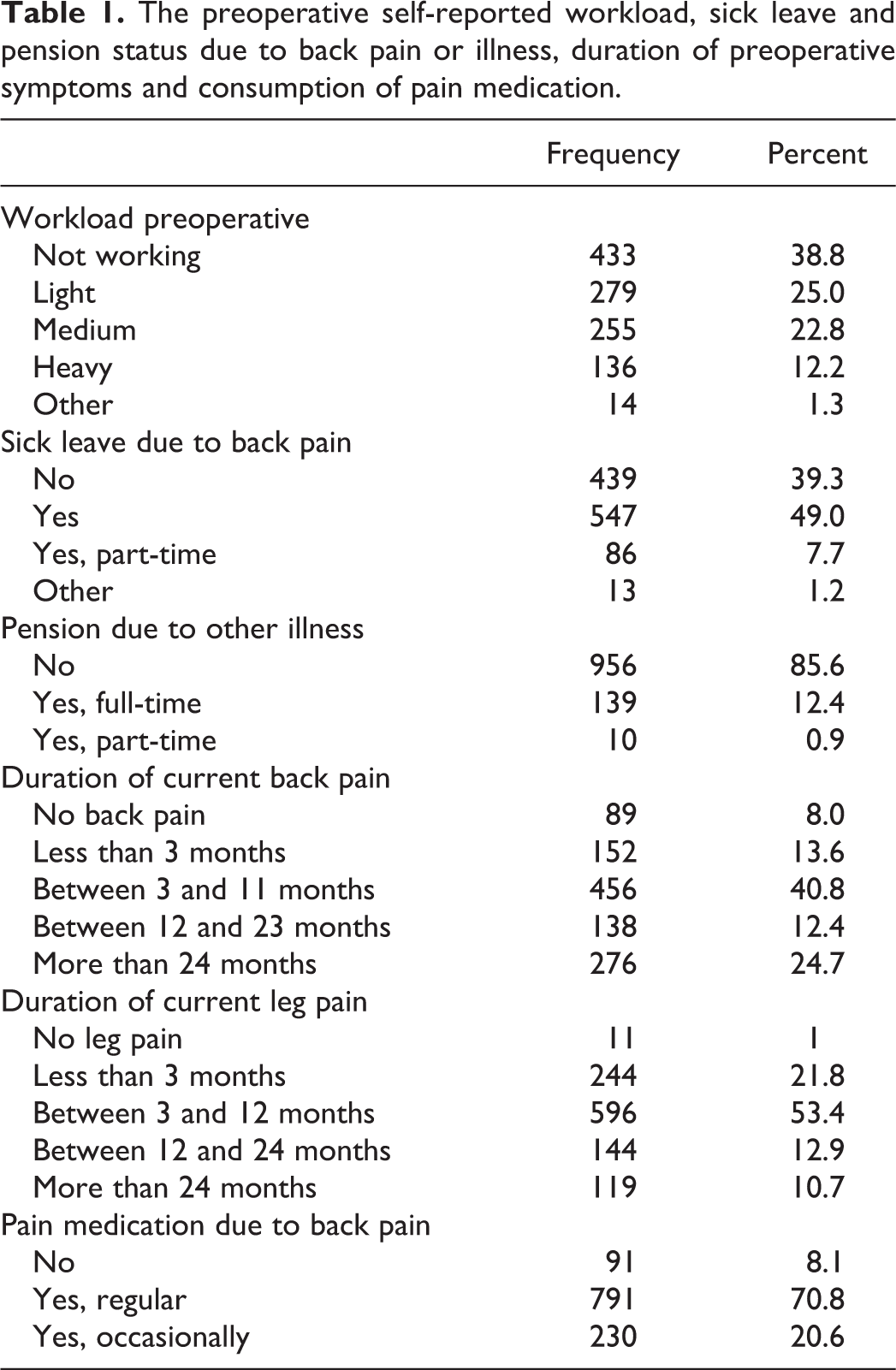
Of 1134 consecutive patients operated due to LDH eligible to be in the study, 1117 (98.5%) completed the preoperative surgical DaneSpine questionnaire and were included in the analysis. The mean age of the cohort was 48.2 (SD 14.8) years, 587 (52.6%) were males and 348 (31.2%) of the cohort were smokers at the time of operation. Prior to the surgery, 200 patients (17.8%) reported that they were unemployed. The preoperative self-reported workload, sick leave, and pension status due to back pain or illness, duration of preoperative symptoms, and consumption of pain medication are presented in Table 1. Preoperative self-reported measures of quality of life, work load, disability, well-being, pain, and duration of sick leave are presented in Table 2. The mean number of weeks not working prior to the operation was 52.1 (SD 43.2), Table 2.
The preoperative self-reported workload, sick leave and pension status due to back pain or illness, duration of preoperative symptoms and consumption of pain medication.
Preoperative self-reported measures of quality of life, disability, well being, pain, and duration of sick leave.
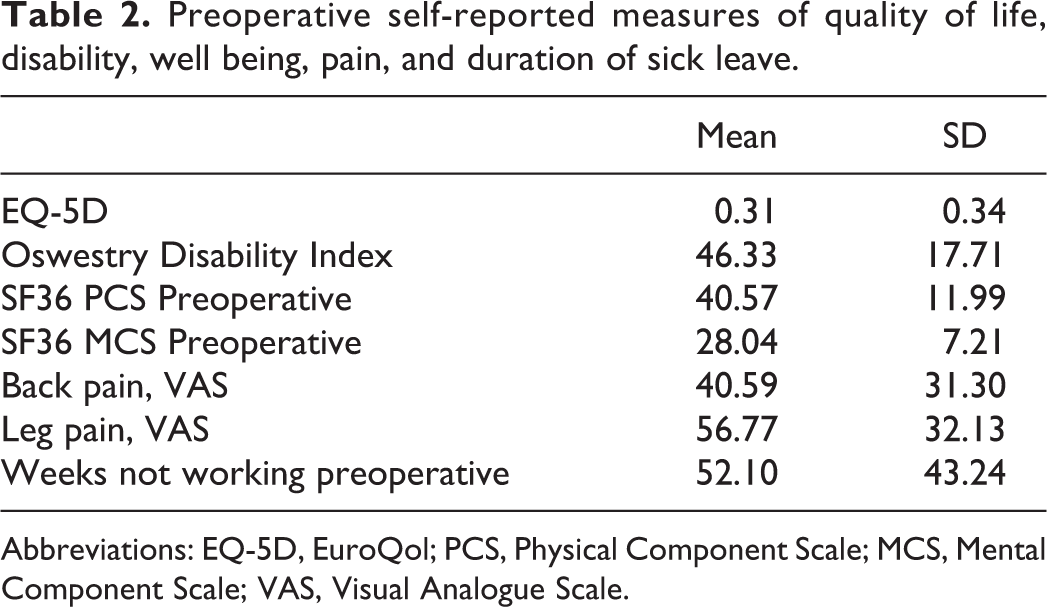
Abbreviations: EQ-5D, EuroQol; PCS, Physical Component Scale; MCS, Mental Component Scale; VAS, Visual Analogue Scale.
Postoperatively, 883 patients (79.1%) returned to the workforce within 12 weeks after the surgery. Factors not influencing return to work in the bivariate analysis included age, gender, smoking, medication, SF-36 physical function score, SF-36 mental function score, and VAS score for Back Pain and Leg Pain. In the stepwise logistic regression model only preoperative workload, preoperative EQ-5D, and the number of weeks not working prior to the surgery affected the return to work rate at 12 weeks (Table 3).
Stepwise logistic regression: Pre-operative work-load, pre-operative EQ5D and the number of weeks not working prior to the surgery.
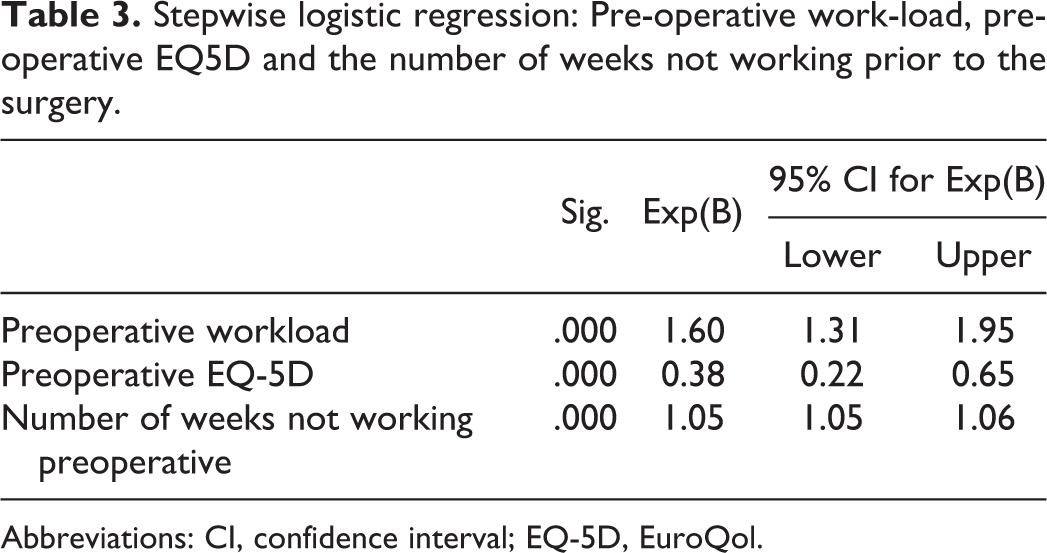
Abbreviations: CI, confidence interval; EQ-5D, EuroQol.
Discussion
Return to work as an outcome is readily understood and can be regarded as an important, practical, and reliable parameter for patients’ recovery and rehabilitation. However, the definition of return to work as reported in the literature is not standardized. Some studies report the point prevalence at 6 or 12 months after the operation or time to first occurrence of 4 consecutive weeks of working. 16 In the current study, return to work was defined as not receiving any public sickness benefits for 4 weeks. As the data comes directly from the Ministry of Employment, the authors believe that the current study provides a reliable metric of return to work.
In the present study, of the factors found to be significantly associated with return to work, duration of sick leave can potentially be modified in a systematic manner. This finding correlates well with the findings of Silverplats et al 17 that 60% of the patients report full working capacity if the duration of preoperative sick leave was less than 3 months, compared with 23% for patients with longer sick leave. In a Norwegian paper from 2000 the authors report that patients who took sick leave of more than 28 weeks before surgery were at higher risk of not returning to work. 18 In a Danish paper 6 of a mixed cohort of surgically and nonsurgically treated patients, one of the strongest predictors for unfavorable vocational prognosis was less than 40 weeks of employment within 2 years prior to presentation in the clinic. Interestingly, the same study showed that simple discectomy did not negatively affect the vocational prognosis. The results of the current study raises the need to revisit several of the Danish Regional Guidelines19,20 requiring 8 to 12 weeks of nonsurgical treatment prior to referral to a surgeon for patients with LDH without neurologic deficits. Future studies are needed to determine if earlier referral to a surgeon, within the setting of shared decision making with the patient, leads to an earlier return to work.
That the preoperative workload was also associated with return to work has been previously reported. 6 Unlike duration of sick leave, preoperative workload may be more difficult to modify, as this requires vocational retraining at the individual level. However, this finding can help surgeons and physical therapists counsel their patients regarding their prospects for returning to work. Health care providers can better prepare their patients mentally and physically as to what to expect, and possibly offer vocational options after a discectomy.
The last factor found in the current study that is associated with return to work is the patient’s preoperative EQ-5D. As EQ-5D is a generic health state utility measure, 11 EQ-5D may be reflective of the patient’s general health. Patients with lower EQ-5D scores are probably less healthy and may have more comorbidities than patients with higher scores. A low EQ-5D prior to surgery should prompt the surgeon to identify and treat medical conditions and optimize the patient’s health prior to surgery.
The strength of this study is that we used prospectively collected data from a consecutive series of patients enrolled in DaneSpine and the Dream database. Almost all cases (99%) seen in the Center for Spine Surgery and Research are enrolled in DaneSpine 9 with an 88% follow-up rate at 1 year. 9 The DREAM database has been validated by comparing the data to self-reported information on sources of income using a population survey with about 5000 participants. 21 By combining DaneSpine and DREAM the current study accessed reliable and accurate data in terms of outcomes and public welfare payments. As medical care is publicly funded and available to everyone in Denmark, the patients in this study are representative of LDH patients irrespective of income, education, or social class. That is, there is no barrier for patients to seek medical or surgical care if they need it. One weakness of this study is that information on duration of sick leave symptoms are based on the DREAM database and self-employed patients might not receive public welfare payments. Furthermore, the relevance of the study could be questioned as the DREAM data analyzed is covering the period between 2010 and 2013. As there have not been any fundamental changes in care, socioeconomic support for patients, or workers’ rights changes in Denmark we believe the presented results are valid. Another limitation is the lack of granularity in terms of the type of job the patient returned to, for example, if the patient returned to the same job or a different, less physically demanding job.
The result of this study indicate patients who have a longer duration of sick leave, have a physically demanding job, and are in poor health are more likely not to return to work by 12 weeks after surgery for LDH. Patients in physically demanding jobs should be counseled appropriately regarding their ability to return to work after surgery. Patients should be medically optimized prior to surgery to improve their overall health. Lastly, future studies are needed to determine if earlier referral to a surgeon leads to an earlier return to work.
Footnotes
Authors’ Note
This study was reviewed and approved by the research board of the sector of spine surgery and research, Middelfart Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.