
Abstract
Study Design
Case control study
Objective
Micro-lumbar discectomy or Interbody fusion procedure are work-horse surgical procedures in management of lumbar disc disease. Spine surgeon in their early years of practice gets confused in choosing ideal surgical plan when dealing with a complex scenario. A clinical score is needed to guide spine surgeons in choosing an optimal surgical plan.
Materials and methods
Study was done with research grant approval from AO Spine. A predictive score was formulated as per hypothesis following a pilot study. Two fellowship trained spine surgeons-one using the score (Group A) and other not using score (Group B-control) treated 40 patients included in their respective group. All patients were analysed preoperatively, post-surgery at 12 months follow-up with Visual analog scale score for back pain, leg pain, Oswestry disability index score, SF-36 score. Change in parameters at 12 months follow-up were analysed statistically. P ≤ .05 was considered statistically significant. Success rate of individual surgeon who managed respective group of patients and Difficulty index of surgeon who managed without using score was evaluated at 12 months follow-up.
Results
Success rate of Group A-surgeon was higher than Group B-surgeon .15% of Group B patients had poor surgical outcome at follow-up. Statistically significant improvement in Group A patients were seen in all 3 evaluated parameters when compared to Group B patients at 12 months of follow-up (P ≤ .05). Difficulty index of surgeon who didn’t use the score was 15%.
Conclusion
The proposed predictive score comprising all risk factors, can be used by spine surgeons when they are confronted with difficult scenario in decision-making. Accuracy, reliability and validity of the score needs to be evaluated in a larger scale.
Level of evidence
Ⅲ
Keywords
Introduction
The prevalence of lumbar disc degeneration progressively increases with age. It has been estimated to be 40 percent under 30 years of age and above 90 percent in people over 55 years of age in south Chinese population 1 . The cause of lumbar disc degeneration is multi-factorial. Genetic, occupational bio-mechanical factor and physical body habitus of an individual contribute to disc degeneration at an early age. Polymorphism in the coding region of human aggrecan gene, heavy physical work contributing to excessive stress at lumbar spine and tall stature of an individual 2,3 all have been attributed as risk factors of lumbar disc degeneration at a young age.
Surgical management of lumbar disc disease patients is challenging. The decision- making to choose exact surgical plan for the patient, either Micro-lumbar discectomy or an Interbody fusion procedure with Nerve root decompression remains decision dilemma for the Spine surgeon in dealing with problem. Though after properly analysing dynamic radiographs, magnetic resonance images (MRI) of lumbar spine the young spine surgeon (spine surgeon within 5 years of practice after graduation) gets confused in formulating a plan especially in complex scenarios. A survey, among spine surgeons of ‘Degenerative spine study group’ to evaluate the treatment option in degenerative condition of lumbar spine conducted in the last decade, highlighted those surgeons generally agreed on when to perform the surgery but differed on the type of surgical procedures to perform 4 .
Decision- making in formulating an ideal surgical plan is essential to provide successful outcome to the patient. Our hypothesis is that we can develop a decision-making predictive score for single level symptomatic lumbar disc disease patients based on the independent risk factors to formulate an ideal surgical plan taking into consideration all the relevant risk factors to provide optimal surgical outcome.
Materials and Methods
The study was done with research grant approval from AO Spine, reference project number: AOSIN[R]2019-08B. The study was carried after institutional ethical board approval no. 11234/BR.
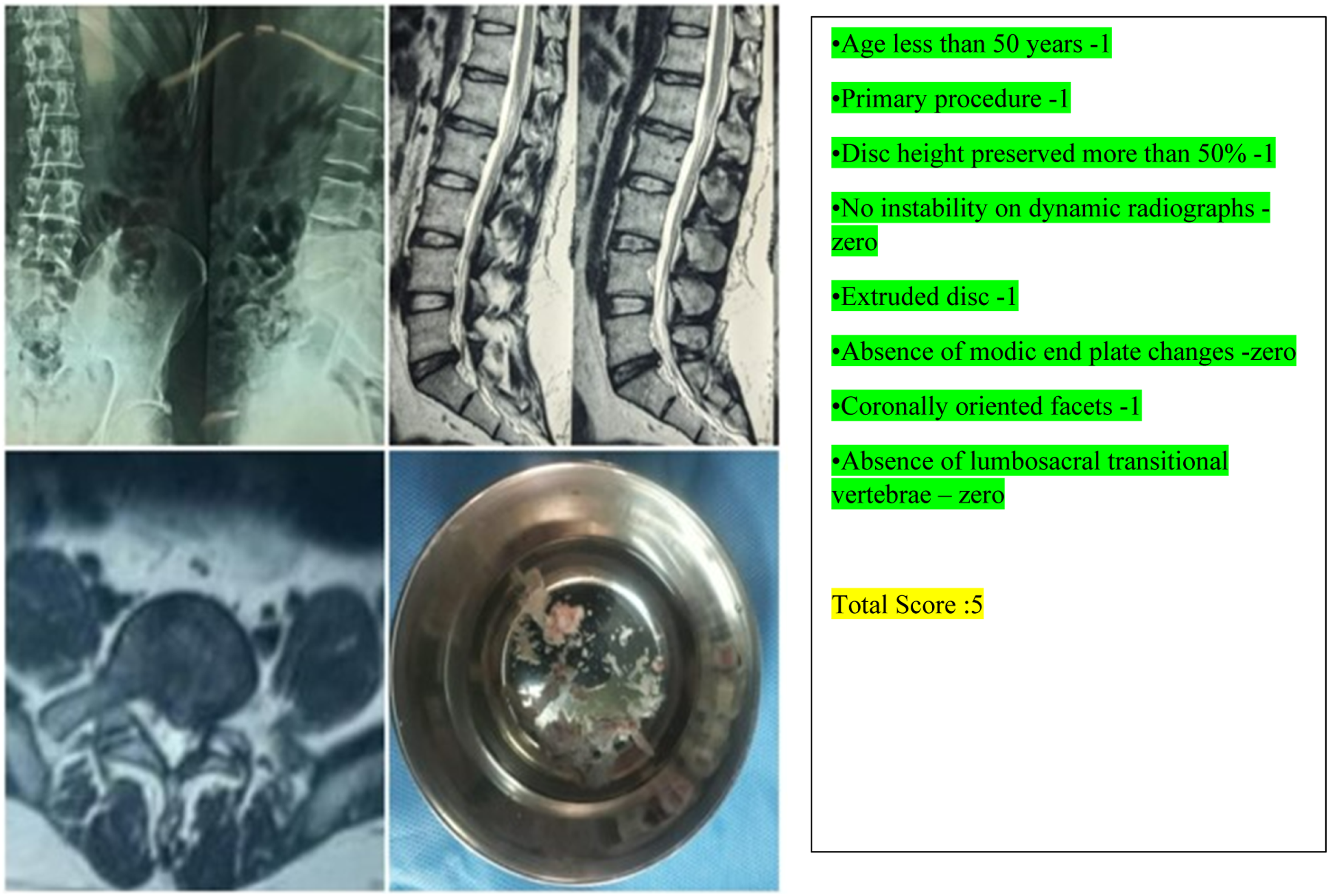
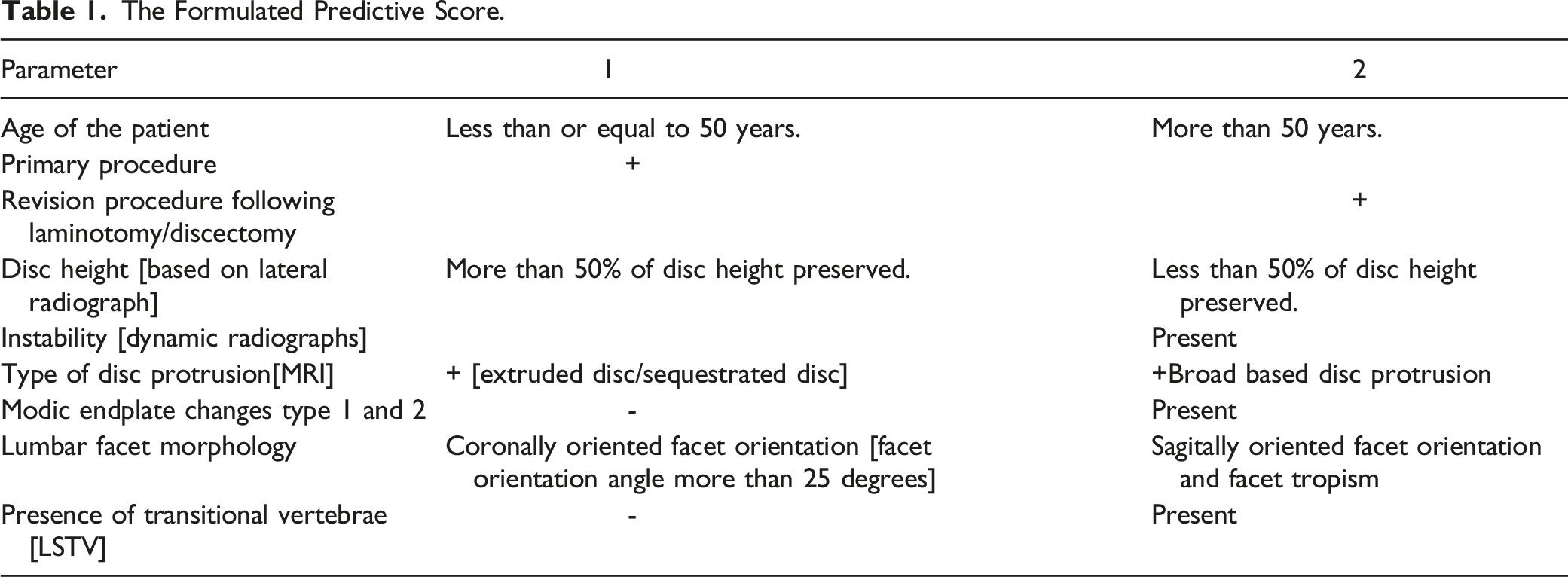
Before formulating the predictive score based on clinical and radiological parameters, the authors validated the score as pilot study. We had taken 8 parameters: Age, type of surgical procedure – primary or revision, disc height, instability in dynamic radiographs, morphology of disc protrusion, modic endplate changes in magnetic resonance imaging, lumbar facet morphology and presence of transitional vertebrae -all of which were found to be statistically significant parameters in predicting better outcome in lumbar disc disease patients if an appropriate surgical plan was followed. The pilot study helped us to choose the cut-off score of 5 as the discriminating point between the 2 choices while assessing the score. The patients scoring less than or equal to 5 to undergo Micro lumbar discectomy and patients who score equal or more than 6 to undergo Transforaminal lumbar Interbody Fusion.(Table 1)
The patients visiting the spine unit were randomly divided into 2 groups - group A and B during the study period from September 2019 to August 2020. Patients visiting the spine unit on first, third and fifth week of the month were included in group A and patients visiting the spine unit on second and fourth week of the month were included into group B. Patients with symptomatic single level lumbar disc disease were included into the study. All the patients included in the study had chronic low back pain with radicular leg pain and pain distribution corresponding to the dermatome correlating with their MRI images. Patients with disease more than one segment, patients not willing for follow-up, pregnant females, patients with age limit less than 18 and more than 70 years, patients with other known spinal disorders-spondylolisthesis, spinal tumours, metastases were excluded from the study. The study was conducted in an university affiliated hospital, south asia providing tertiary care to the patient population.
Under two- tailed distribution with level of significance at 5% and power of 80% the minimum sample size in each group was kept at 40 patients in each group. Group B patients were kept as control. As the patients were randomly divided into 2 groups, we followed the CONSORT [Consolidated standards of reporting trial] checklist while doing the study.
Patients undergoing surgery for the first time for lumbar disc disease were considered as primary procedure. Patients who did undergo surgical procedure again with previous history of surgery for lumbar disc disease once at the same spinal motion segment - to be considered as revision surgical candidates
5
. Translational displacement of more than 4.0 mm or 15% of the inferior vertebral body and sagittal angulation value of more than 15 degrees at L4/5 and L5/S1 spinal motion segments in flexion - extension view of lumbar spine is considered as the dynamic instability
6
. Pathologic changes at adjacent vertebral end plates with characteristic hypointense in T1w and hyperintense in T2w, hyperintense in T1w and intermediate in T2w sections of the MRI were considered as the Type 1 and Type 2 Modic end plate changes
7
. The Facet joint orientation or the facet angle was determined based on the method as described by Noren et al
8
. A line is drawn along the margins of superior articular facet at the level of intervertebral disc in the axial cut of MRI T2w image. Another line is drawn along the mid-sagittal line of the disc. Intersection angle formed between the mid-sagittal line and the line along the margins of superior articular facet is considered as the facet joint orientation angle (Figure 1A). A difference of 7 or more degrees between left and right side is considered as Facet tropism
9
. If the lines drawn on both sides along the margins of superior articular facet intersect beyond the junction of anterior one third - middle third of the intervertebral disc in the image, it is considered as Sagittal oriented lumbar facet
9
. (A) Participant flow diagram. (B) Facet joint orientation angle. (C) DHI measurement.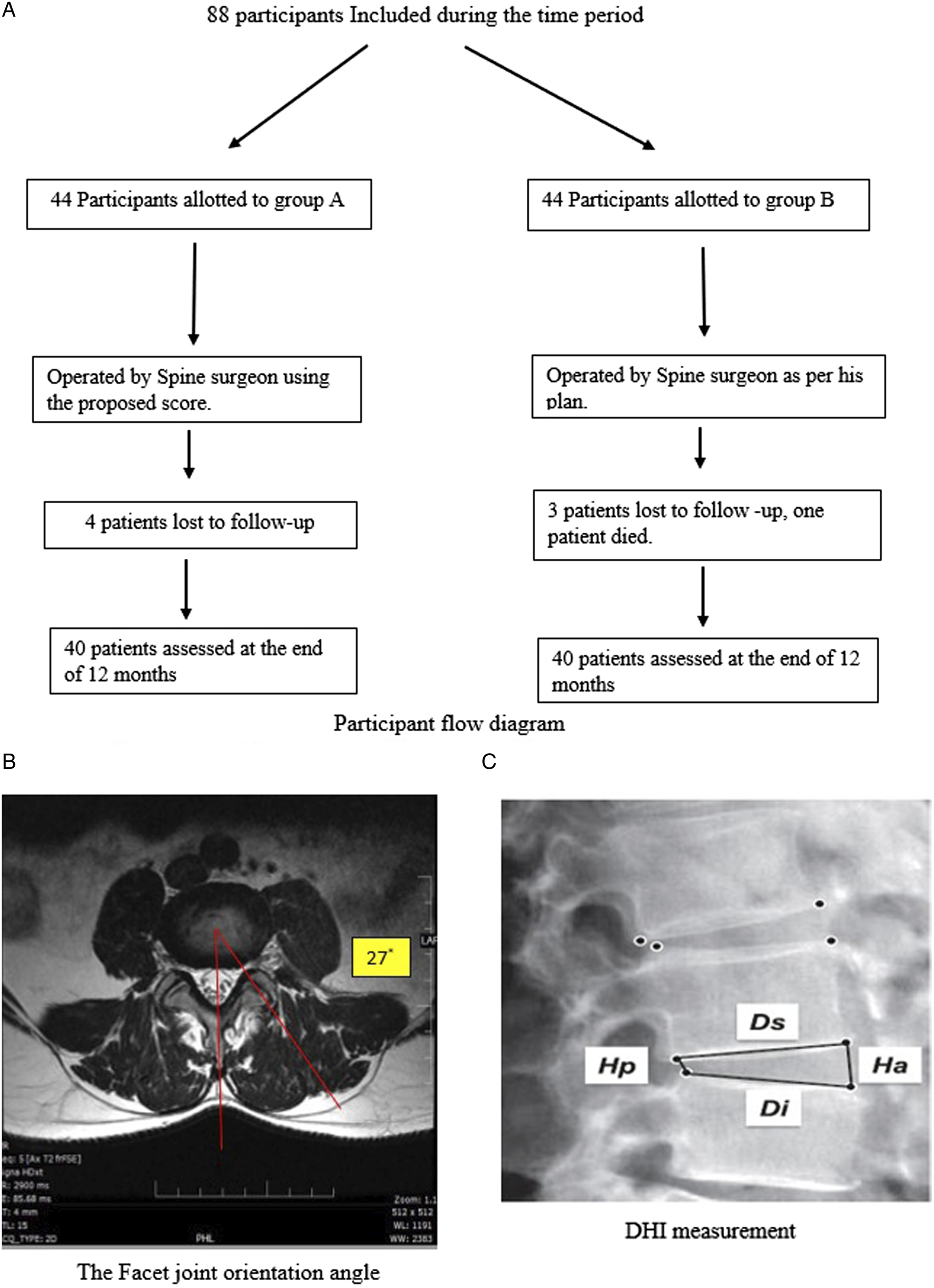
Lumbosacral transitional vertebrae 10 (LSTV) are congenital anomalies which occur due to complete or partial or unilateral fusion of transverse process of lumbar vertebrae to sacrum. It can be either lumbarised sacrum (S1) or sacralised lumbar segment (L5). Prevalence of LSTV has been documented to be between 4 and 36% in literature 11 . Disc height index (DHI) was measured using lateral radiograph of the patient with the involved intervertebral disc segment being compared to the normal superior adjacent motion segment. DHI was calculated by dividing the sum of anterior (Ha) and posterior disc height (Hp) and dividing it by the sum of superior (Ds) and inferior end plates (Di) using the method as described by Akeda et al (Figure 1B) 12 .
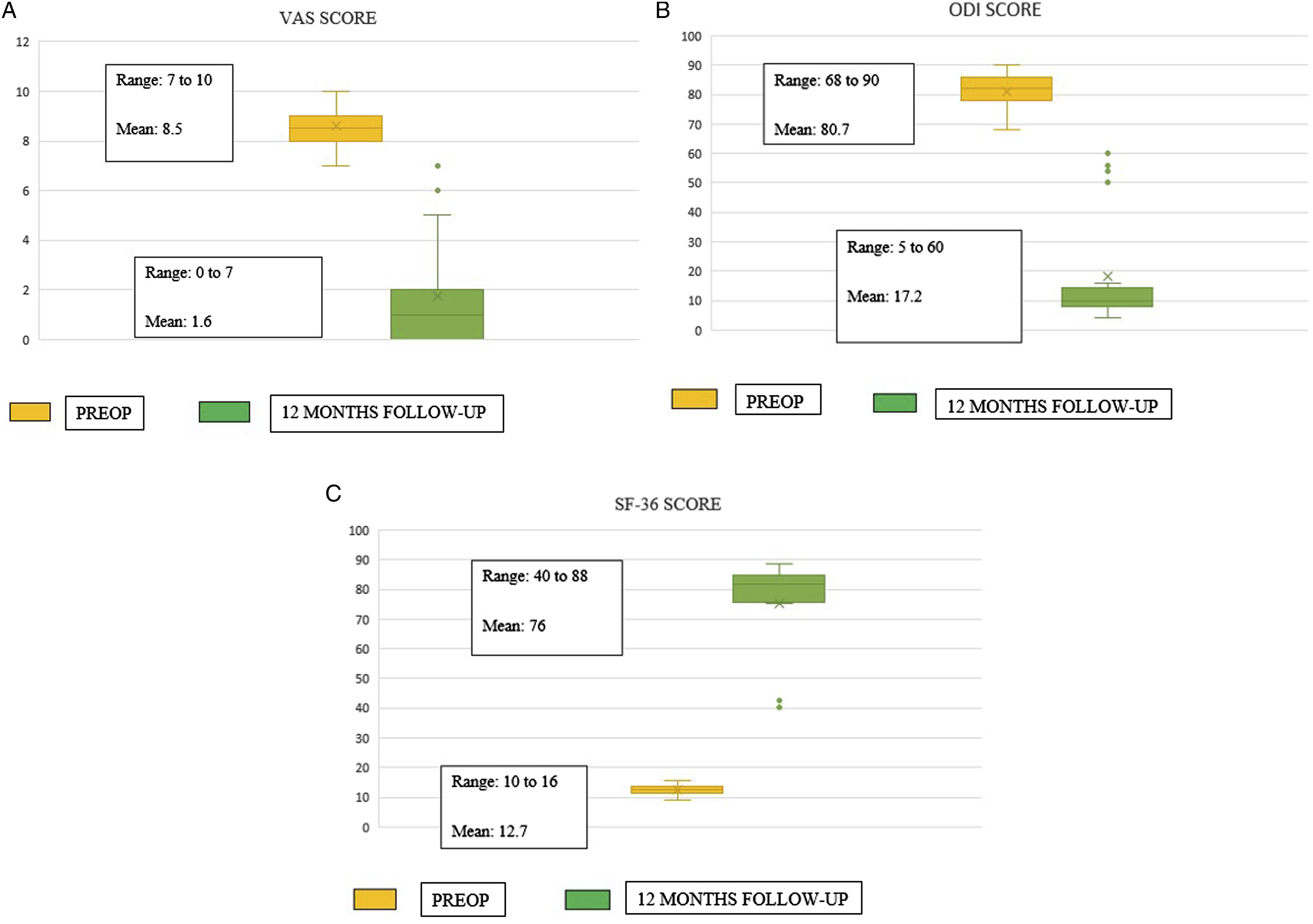
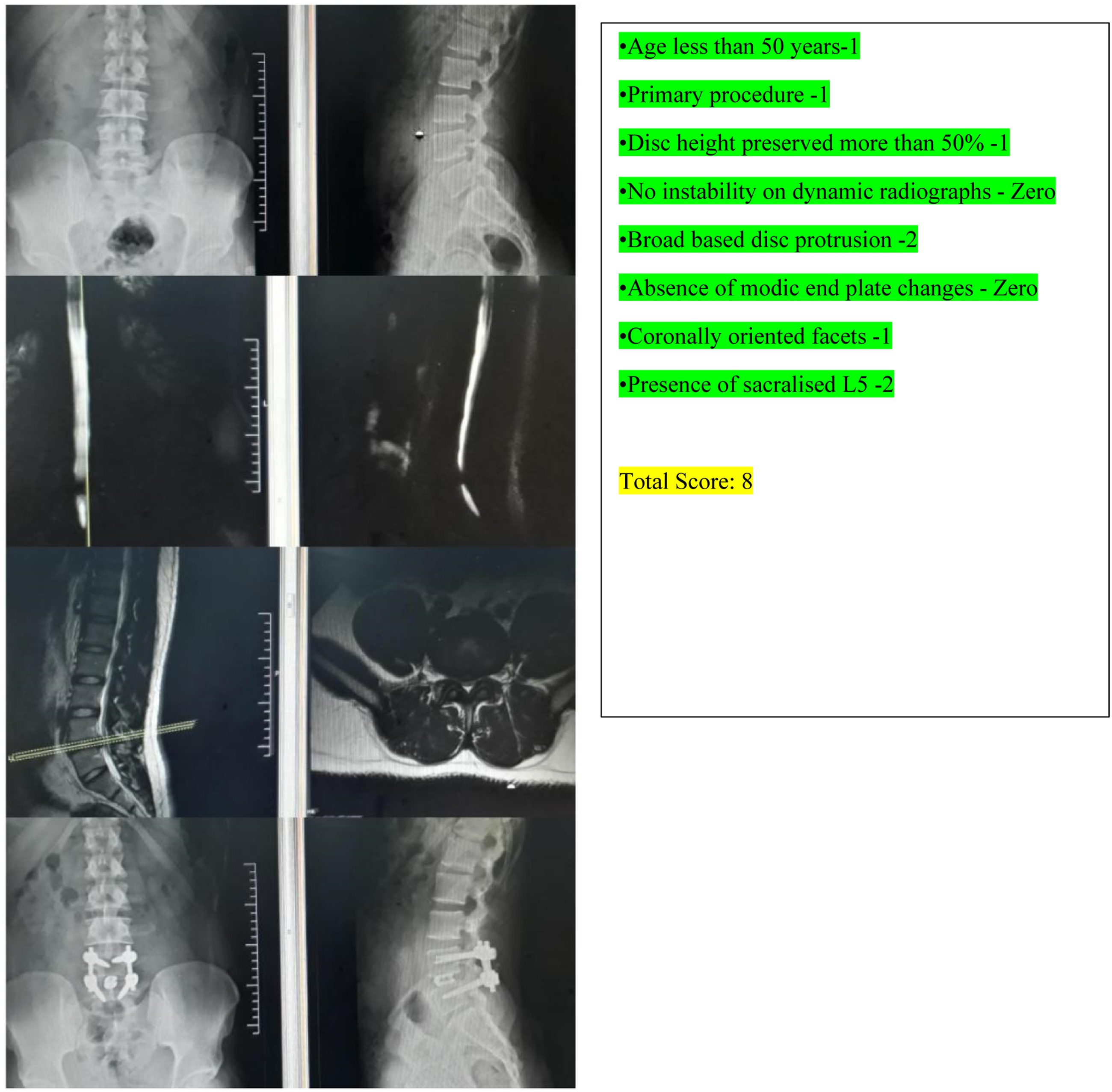
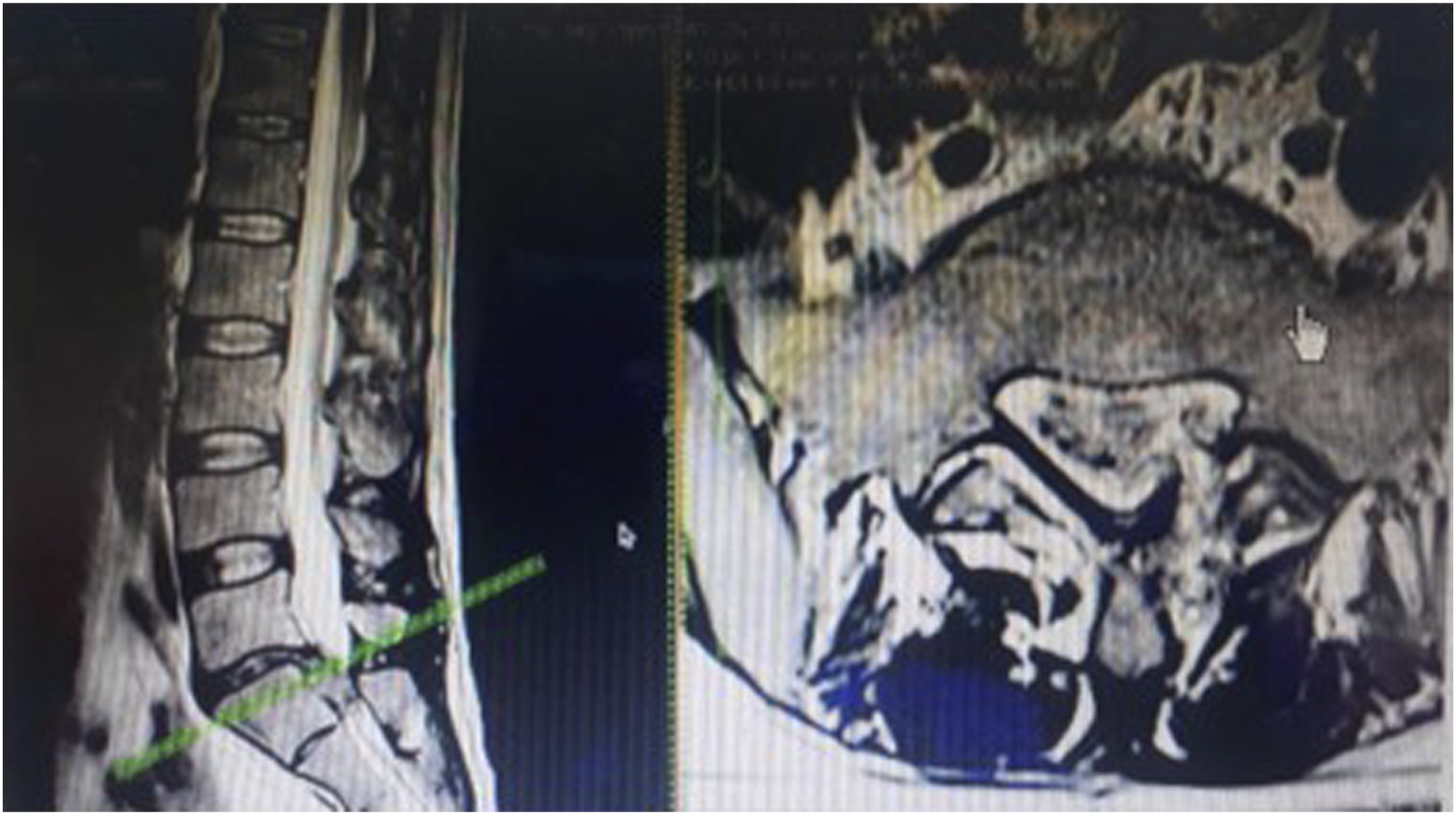
The Spine surgeons who were involved in the study in group A and B are fellowship trained spine surgeons with their independent spine surgery practice varying 3 to 5 years post fellowship. Patients in group A were evaluated by operating spine surgeon with the formulated score above and planned surgical procedure was determined based on the score obtained by each individual patient. Those who scored less or equal to 5 to undergo Micro lumbar decompression and patients who scored equal to or more than 6 will undergo Interbody fusion procedure with bilateral nerve root decompression. Group B patients were evaluated by another operating surgeon without using the score and to undergo either Micro-lumbar decompression or Interbody fusion procedure as per his plan. Enrolment of participants, allocation of participants to group A and B was done by first author (MHS). Participants were blinded about their allocation to 2 different groups. In both groups 44 patients were enrolled and 4 were excluded at the time of assessment of outcome. Outcome assessment was done by senior author (MV) who was blinded about the allocation of participants to the respective groups. (A) Group A: VAS score for back and leg pain. (B) Group A: ODI score. (C) Group A: SF-36 score. (A) Group B: VAS score for back and leg pain. (B) Group B: ODI score. (C) Group B: SF-36 score. Group A: Thirty-seven-year-old gentleman who had low back pain radiating to both lower limbs with right predominant over left. On evaluation with the proposed score, he scored 8 and underwent interbody fusion procedure. Group A: Thirty-five-year-old gentleman, who had left sided sciatica, with score of 5 underwent Micro-lumbar discectomy as per the score. Group B: Fifty-seven-year-old gentleman who underwent left sided Micro lumbar decompression [he should have undergone fusion procedure, if the score had been used] developed recurrence of contralateral leg pain [recurrent contralateral disc] by tenth month of post-surgery.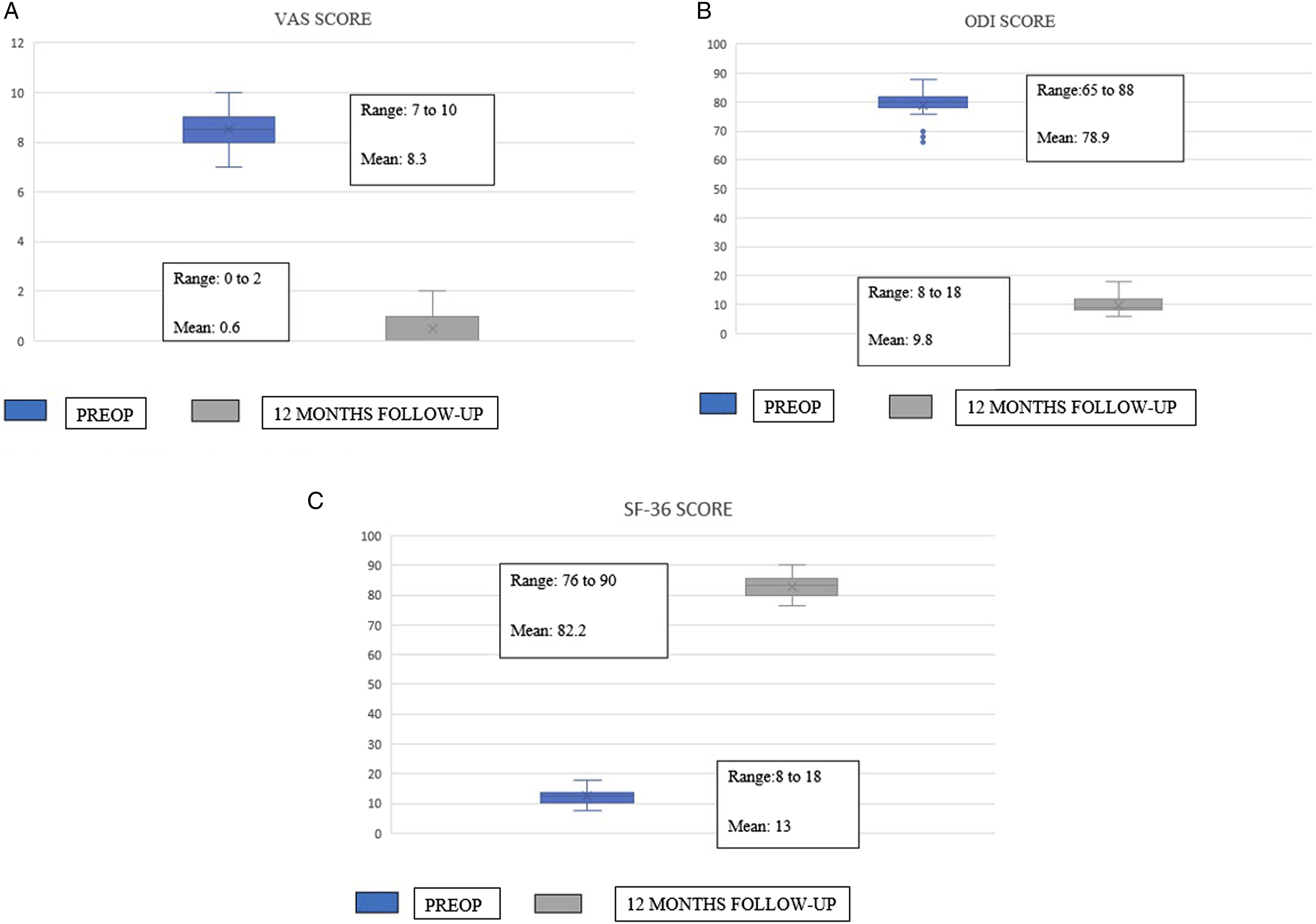
All the patients were analysed preoperatively and post-operatively at 12 months with Visual analog scale (VAS) score for back and leg pain, Oswestry disability index score (ODI score) for back pain, and SF-36 score for general, physical, emotional and social health. Data entry was done in Microsoft Excel 2007. Statistical analysis was carried out by IBM SPSS Statistics version 25.0 (IBM Corp, Armonk, NY, USA). Continuous variables were expressed as mean +/- standard deviation. Comparison of pre-op and post-surgery continuous variables in the respective groups was done by paired ‘t’ test. Comparison of continuous variables between the groups was done by independent sample ‘t’ test. Statistical significance was considered if p < 0.05.
The Formulated Predictive Score.
Patient Demographics of Group A and B.
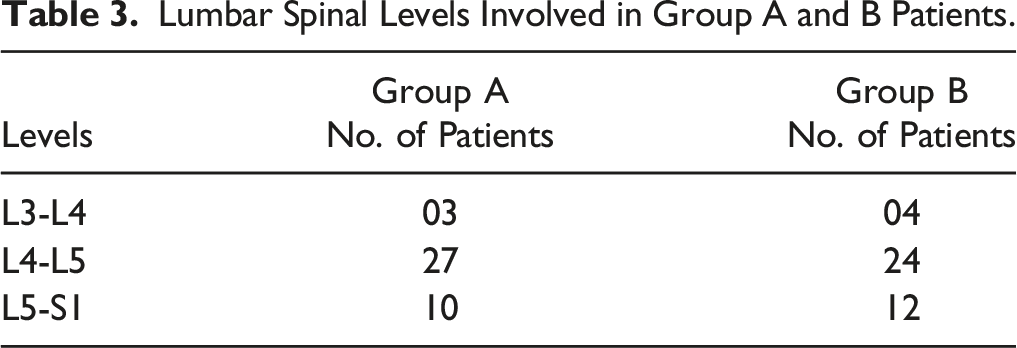
Lumbar Spinal Levels Involved in Group A and B Patients.
Group A Statistical Table.

Group B Statistical Table.

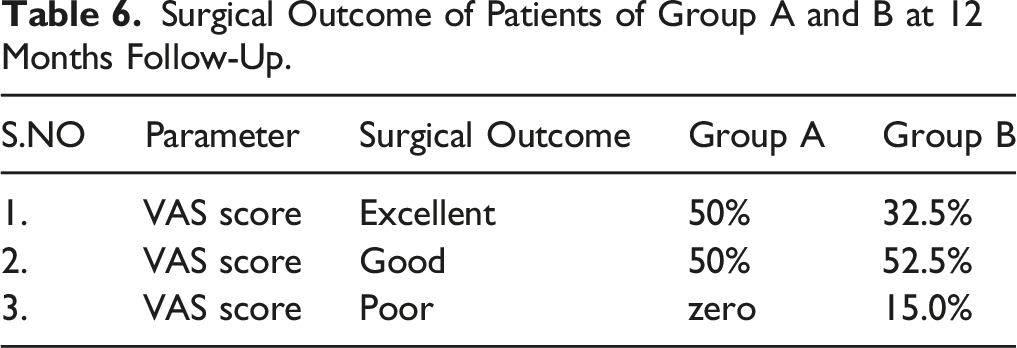
Surgical Outcome of Patients of Group A and B at 12 Months Follow-Up.
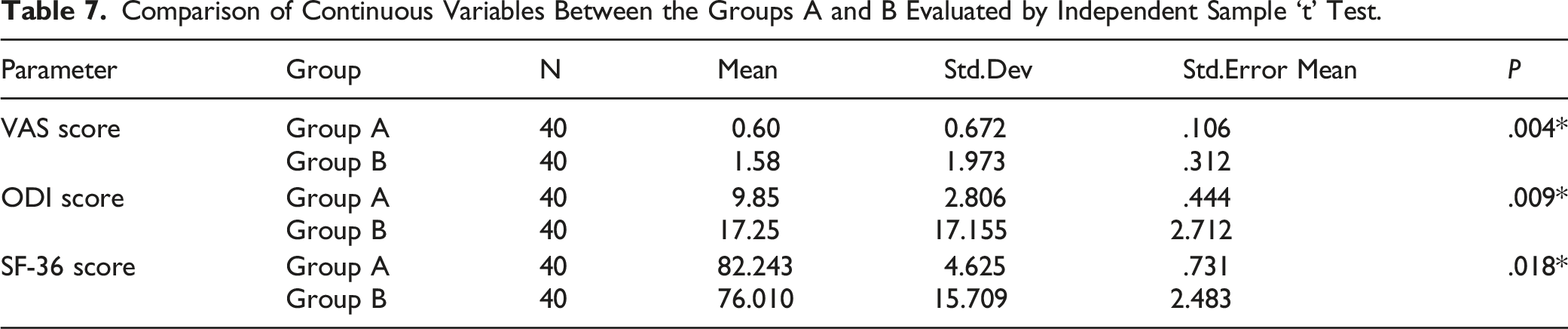
Comparison of Continuous Variables Between the Groups A and B Evaluated by Independent Sample ‘t’ Test.
Results
Patient Demographics
Mean age of the patients was 44.5 years in group A and 47.4 years in group B with males being predominant in both groups. 90% of patients in group A underwent surgery for primary lumbar disc disease and the remaining 10% underwent revision surgery with prior primary micro lumbar decompression surgery at an earlier mean period of 18.5 months. In group B, 92.5% of patients underwent surgery for primary lumbar disc disease with the remaining 7.5% underwent revision surgery with prior primary micro-lumbar decompression surgery at an earlier mean period of 20.2 months.
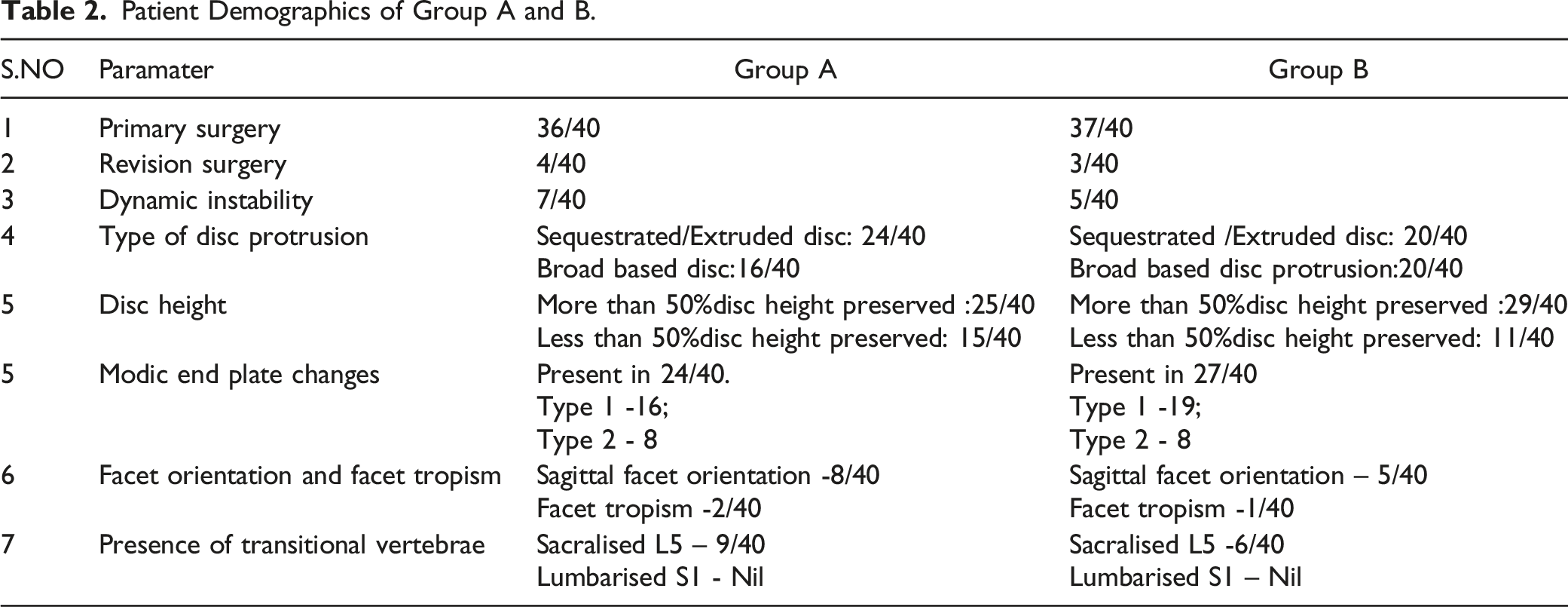
17.5% patients had dynamic instability in flexion-extension radiographs of lumbo-sacral spine in group A and 12.5% had dynamic instability in group B. 62.5% of patients in group A had more than 50% of the disc height preserved and in group B it was 72.5%. In group A, 60% had extruded/sequestrated disc and 40% had broad based disc protrusion in MRI images and it was equally of 50% in both segments among group B patients. 60% of patients in group A had modic endplate changes and in group B it was 67.5%. Majority of them had Type 1 modic end plate changes in both group cohorts.20% of patients showed sagittal facet orientation in group A with facet tropism seen in 5% of patients. 12.5% patients in group B showed sagittal facet orientation and facet tropism was seen in 2.5% of patients. 22.5% of patients in group A and 12.5% of patients in group B had LSTV. The groups were comparable in their demographic characteristics. (Table 2).
29 patients [72.5%] who had obtained score of more than 5 in preoperative planning, had undergone interbody fusion procedures in group A and the remaining had undergone micro-lumbar decompression [27.5%] procedure. In group B, 26 patients [65%] had undergone interbody fusion procedure and the remaining had undergone micro-lumbar decompression [35%] procedure. The predominant segmental level was L4/5 in both the groups followed by L5/S1 and L3/4 (Table 3).
In group A: VAS improved from mean 8.3 to .6, ODI improved from mean 78.9 to 9.8% and SF-36 score changed from mean 13.0 to 82.2 at 12 months follow-up. In group B: VAS improved from mean 8.5 to 1.6, ODI improved from mean 80.7 to 17.2% and SF-36 score changed from mean 12.7 to 76.0 at 12 months follow-up. (Figures 2, 3 and Tables 4, 5)
The Success rate of surgeon who used the score - Group A was 50% [20 patients become VAS-leg pain zero], and the surgeon [Group B] who didn’t use the score was 32.5% [13 patients become VAS-leg pain zero]. There was statistically significant improvement in VAS (P = .004), ODI(P = .009), SF-36 (P = .018) score in group A patients when compared to group B patients at 12 months follow-up. Patient’s outcome had been graded based on the VAS score at 12 months follow-up. None of the patients in group A had poor outcome, whereas 15% of the patients in group B had poor outcome. All those 15% of patients in group B who had poor outcome had significant mean ODI score of mean 57% and mean SF-36 score of 40.7% at 12 months of follow-up. (Table 6 and Table 7)
Difficulty Index of surgeon who didn’t use the score was 15% [needed help in 6 patients out of 40 in decision-making]. The surgeon of Group B patients had difficulty in decision- making in 2 of the revision surgery patients, 2 with sagittal oriented facet orientation and 2 with dynamic instability. This difficulty was more pronounced in the initial randomly allotted twenty patients and his difficulty become less conspicuous in the final randomly allotted twenty patients, probably able to identify the influential parameters in the decision-making.
Discussion
The rationale of proposing this score is to have clarity and uniformity in decision- making among spine surgeons to avoid revision procedure and to provide successful optimal outcome to the patient with single level symptomatic lumbar disc herniation. The cause for morbidity after primary discectomy procedure has been attributed to recurrence of lumbar disc herniation (rLDH) 16 . It is defined as recurrence of ipsilateral or contralateral disc herniation at the same level at least after a period of 6 months following micro lumbar decompression. It is reported to be between 5 and 15% and shows higher incidence with time 17 . The score has been proposed considering the various risk factors for recurrence of lumbar disc herniation following primary discectomy procedure.
A brief note about the parameters used in assessment of score mentioned in the literature are discussed below:
Age
Yao et al 18 in his paper has studied 111 patients with rLDH following discectomy procedure using Kaplan-Meier method and cox regression analysis to identify potential risk factors for the recurrence. He concluded- Age (more than 50 years) as the robust risk factor for rLDH. Zhonghai Li et al 19 attributes an odds’ ratio of 1.244 (P ≤ .0001) for the variable ‘Age more than 50 years’, in his study on rLDH.
Prior Surgical Procedure
Zhonghai Li et al 19 had evaluated patients who had undergone prior discectomy with laminotomy, discectomy with hemilaminectomy, discectomy with total laminectomy, discectomy-total laminectomy with non-instrumented fusion and reported patients who had undergone prior discectomy with total laminectomy had higher rLDH rates when compared to the remaining three. He documents an odds’ ratio of 2.828 (P = .003) in his series for patients who had undergone prior discectomy with total laminectomy. Bydon et al 20 in his paper on reoperations following total lumbar laminectomy has concluded laminectomy disrupts the equilibrium of disc-facet-posterior spinal ligamentous complex causing reoperation either due to rLDH or worsening spondylolisthesis at the index or at the distal segment level.
Disc Height
Kim et al 21 in his study of identifying the risk factors for rLDH in 156 patients found mean DHI of .37 +/− .09 in recurrent and mean DHI of .29+/−.09 in non-recurrent group. The DHI in recurrent group was statistically significant P = .028 and he suggests DHI as a significant risk factor for rLDH with an odds’ ratio of 1.16. He discusses the reason, why the patients with lesser DHI of .29 had avoided recurrence when compared to the patients with mean DHI of .37. The rationale being collapsed discs are sounder biomechanically when compared to those with height preserved with lesser incidence of rLDH as per Kirkaldy-Willis and Farhan hypothesis 22 .
Dynamic Instability
Zhonghai Li et al 19 documents spinal instability as the most important anatomical factor responsible for rLDH, and he attributes an odds’ ratio of 88.83 (P ≤ .0001) to the variable [discectomy at the instability level] in his paper on analysis of risk factors for rLDH. In his study, the patients had mean instability of 12.1 +/- 1.4 degrees. Kim et al 21 suggests a recurrence rate of 26.5% if the instability is more than 10 degrees and a recurrence rate of 4.1% if the instability is less than 10 degrees.
Morphology of Disc Herniation
Min seon kim et al 23 in his paper on rLDH after open discectomy in 241 patients has concluded a recurrence rate of 7.1% in his study. He has documented recurrence occurred in 15.9% of protruded discs and 3.7% of extruded discs and absolutely no recurrence in sequestrated discs based on the disc morphology. Morgan-Hough et al 24 in his study of 531 patients over a period of 16 years had reported a revision rate of 7.9% and added that contained disc protrusion had chance of 3 times of revision surgery when compared to extruded or sequestrated discs.
Modic Endplate Changes
Modic endplate changes (MC) has been attributed as independent risk factor for the development of segmental hypermobility and severe disabling chronic low back pain. The documented odds’ ratio for segmental hypermobility and chronic low back pain with presence of MC is 1.566; P = .03 25 . Tanaka et al 26 has reported patients who develop MC have strong cartilaginous vertebral end plate – annulus fibrosus junction and relatively weaker cartilaginous vertebral end plate and osteochondral bone junction. Hence, the disc herniation has rich cartilaginous tissue rather the more common nucleus rich herniation which is less likely to spontaneously resorb.
Facet Morphology and Facet Tropism
Miyasaki et al 27 had proposed in his study on lumbar spinal unit kinematics that sagittal oriented lumbar facet joints are prone to develop lumbar spinal canal stenosis. A biomechanical analysis by Kim et al 28 on the sagittal oriented lumbar facets and facet tropism has revealed the index lumbar motion segment is more prone for instability by anterior shear force. The same has been reiterated by Abbas et al 29 that sagittal facet orientation, facet tropism predisposes the lower lumbar spine up to 2.9 times to the development of spinal canal stenosis.
Lumbosacral Transitional Vertebrae
A biomechanical study by Luoma et al 30 has stated that hypermobility and abnormal torque movements occurring above LSTV alters the equilibrium of disc-facet- posterior spinal ligaments complex causing disc degeneration and progressive spinal canal stenosis. Abbas et al 31 had documented that LSTV predisposes to spinal stenosis at its superior adjacent lumbar segment with an odds’ ratio of 3.741 (P = .001).
Micro-Lumbar Discectomy and Transforminal Interbody Fusion
The commonly done surgical procedures for lumbar disc disease has their own advantages and disadvantages. Takahashi et al 32 in his in vivo study on 34 patients had measured the nerve root pressure using a transducer between the disc herniation and the corresponding nerve root. He found that a mean preop nerve root contact pressure of 53 mm hg had reduced to zero post discectomy in all his patients. The rationale behind the success of microsurgical decompression is that it reduces the nerve root pressure following discectomy. Lurie et al 33 in his eight-year follow-up of patients enrolled for spine patient outcome research trial [SPORT trial – 501 participants] documented that micro lumbar decompression improved all the primary outcome measures [SF -36, VAS score, ODI score] at the end of follow-up and pronounces rLDH rate of mean 7.8% as the main disadvantage with the procedure.
The main advantage of interbody fusion procedure is that it avoids recurrence of disc herniation and stabilises the motion segment however, it comes with the risk of dural tears, instrumentation related and fusion related complications. Ajiboye et al 34 emphasised in his paper [published by 2018] on ‘surgical treatment of recurrent lumbar disc herniation- A systematic review and metanalysis’ - the treating surgeon has to balance the risk profile of fusion surgery with micro-lumbar decompression and choose the option wisely during primary lumbar spine surgery as both the procedures can provide comparable functional outcome following the respective surgical procedures. A delicate balance is needed in preventing rLDH (with micro lumbar decompression) and mitigating instrumentation, fusion related complications (with interbody fusion). This justifies the need for a predictive score in preoperative decision- making in lumbar disc disease patients considering all the risk factors attributable to recurrence of disc herniation to provide optimal outcome following primary lumbar spine surgery.
To our knowledge this is the first attempted predictive score for lumbar disc disease patients considering all the relevant risk factors in the patient population. The obtained results depict the Surgeon who used the score [group A] had better success rate (50%) when compared to the surgeon who didn’t use the score (32.5%). Though group A and group B patients had statistical improvement in VAS score, ODI score, SF-36 score at 12 months follow-up, there was statistical comparative improvement in group A patients in all the 3 evaluated parameters when compared to group B patients at 12 months of follow-up (P ≤ .05). The Difficulty index of the surgeon who didn’t use the score was 15%, and it was nil with the surgeon who used the score. The Difficulty index could have been higher than 15%, if the influential parameters in decision making was not revealed to the operating surgeon in the initial randomly allotted twenty patients.15% of group B patients would have had different surgical plan, if the model would not have been followed and would have landed up in unnecessary revision surgeries. The above results depict the projected score to help the spine surgeon who are in their early years of practice in proper decision- making and to avoid erroneous surgical procedure in their endeavour to provide better quality of life to the patients. (Figures 4, 5 and 6)
Limitations
Though the score helps the clinician in appropriate decision- making, the accuracy, reliability and validity of the score needs to be assessed in a larger scale at multiple surgical centres. The other important parameters which could add value in decision making are body habitus of the patient [BMI > 40], history of smoking, operative room -technical setup, neurology of the patients have not been considered in formulating the score.
Conclusion
The proposed predictive score comprises all the risk factors in single segment symptomatic lumbar disc disease patients can be used by orthopaedic surgeons, neuro surgeons, spine surgeons who are in their early years of practice whenever they are confronted with a difficult scenario to provide better quality of life and optimal outcome to their patients.
Footnotes
Author’s Note
We the authors have named the proposed score as: Degenerative Lumbar spine Decision Making Score [DLDMS].
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the AO spine research grant Reference number: AOSIN[R]2019-08B
Availability of Data and Material [Data Transparency]
Not applicable
Code Availability [Software Application or Custom Mode]
Not applicable.