
Abstract
Study Design
Systematic Literature Review
Objective
Perform a systematic review evaluating postoperative fusion rates for anterior cervical discectomy and fusion (ACDF) using structural allograft vs various interbody devices augmented with different osteobiologic materials.
Methods
Comprehensive literature search using PubMed, Embase, The Cochrane Library, and Web of Science was performed. Included studies were those that reported results of 1–4 levels ACDF using pure structural allograft compared with a mechanical interbody device augmented with an osteobiologic. Excluded studies were those that reported on ACDF with cervical corpectomy; anterior and posterior cervical fusions; circumferential (360° or 540°) fusion or revision ACDF for nonunion or other conditions. Risk of bias was determined using the Cochrane review guidelines.
Results
8 articles reporting fusion rates of structural allograft and an interbody device/osteobiologic pair were included. All included studies compared fusion rates following ACDF among structural allograft vs non-allograft interbody device/osteobiologic pairs. Fusion rates were reported between 84% and 100% for structural allograft, while fusion rates for various interbody device/osteobiologic combinations ranged from 26% to 100%. Among non-allograft cage groups fusion rates varied from 73-100%. One study found PEEK cages filled with combinations of autograft, allograft, and demineralized bone matrix (DBM) to have an overall fusion rate of 26%. In one study comparing plate and zero-profile constructs, there was no difference in fusion rates for two-level fusions.
Conclusion
There was limited data comparing fusion outcomes of patients undergoing ACDF using structural allograft vs interbody devices augmented with osteobiologic materials to support superiority of one method.
Introduction
When anterior cervical discectomy and fusion (ACDF) was initially described by Smith and Robinson in 1958, the authors utilized iliac crest autogenous graft (ICAG) as the interbody material. Although outcomes following ACDF using ICAG are favorable with fusion rates of 95–100%, advances over the past few decades have sought to develop methods that aim to eliminate the donor site morbidity of autograft harvesting and seek to minimize subsidence while maximizing fusion rates. 1 Currently, the available options for ACDF interbody devices include allograft variants (cortical, cancellous, composite), and synthetic cages or interbody fusion devices (most commonly titanium, carbon fiber reinforced polymers, and polyetheretherketone (PEEK). There is global variation in use of these products. In a 2017 survey of 5334 spine surgeons, PEEK cages were most commonly used outside North America, while structural allograft remained the most commonly utilized interbody devices for ACDF in North America. 2
In order to augment the fusion, there has been widespread development of osteobiologic materials and bone graft substitutes to be used in conjunction with interbody devices in ACDF. 3 Although autograft still remains the gold standard, demineralized bone matrix (DBM), bone marrow aspirate (BMA), bone morphogenic protein (BMP), and various bioceramics have been studied for this purpose, and have demonstrated clinically favorable results when used as bone graft substitutes. 4
The evolving landscape of mechanical interbody devices and osteobiologic materials for use in ACDF warrants critical review. Each combination of interbody and osteobiologic material has the potential to modulate radiographic outcomes such as subsidence 5 and fusion. While over 91% of spine surgeons deem fusion as the necessary goal, 6 there are a limited number of studies that critically evaluate fusion outcomes following ACDF with various combinations of interbody devices and osteobiologic materials.
The primary objective of this systematic review was to identify studies examining fusion rates using synthetic interbody devices with the addition of osteobiologic material vs structural allograft in patients undergoing ACDF. Our hypothesis was that both allograft and alternative interbody device/osteobiologic combinations would achieve high fusion rates.
Methods
This study used publicly available information and was not subject to review by the institutional review board.
Search Strategy
The literature search was designed in accordance with the Preferred Reporting Items of Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 7 With the help of a clinical informationist, a comprehensive literature search using PubMed, Embase, The Cochrane Library, and Web of Science was performed in September 2020.
Inclusion and Exclusion Criteria
Included studies reported results of 1–4 levels ACDF using pure structural allograft compared with a mechanical interbody device (PEEK, carbon fiber reinforced polymer (CFRP), or metal cages) augmented with an osteobiologic. Osteobiologic classes were defined as autologous bone graft, allogenic bone graft, bone marrow aspirate (BMA), demineralized bone matrix (DBM), hydroxyapatite (HA), bone morphogenetic protein (BMP), platelet-rich plasma (PRP), ceramic-based bone graft, mesenchymal stem cells (MSC), or other synthetic materials such as β-TCP or bioactive glass ceramic (BGC). In addition, we included studies that analyzed participants between 18 and 80 years old with herniated or degenerative cervical neck discs; were randomized control trials, cohort studies, or prospective or retrospective studies with ≥10 patients per group; were written in English; were published in 2000 or later; and reported radiographic fusion rates with at least 6 months of follow up.
Excluded studies reported on ACDF with cervical corpectomy; anterior and posterior cervical fusions; circumferential (360° or 540°) fusion; ACDF for adjacent-segment disease; ACDF for non-degenerative conditions; or revision ACDF for nonunion or other conditions. We also excluded studies with patients with a history of tumor, infection, spinal cord injury, trauma/fracture, scoliosis or cervical deformity, or skeletally immature patients. Finally, we excluded in vitro studies, animal studies, or case reports; studies with <10 patients per treatment group; abstracts, editorials, and letters; white papers; narrative and systematic reviews; preliminary reports; single reports from multicenter trials; and duplicate publications of the same study.
Definition of Fusion
The following criteria outlined by Rhee et al was used as the gold standard for assessment of fusion: <1-mm of interspinous motion on flexion-extension radiographs, with computed tomography (CT) follow-up if fusion status was indeterminate. 8 The fusion definitions of the studies included in this review were compared against Rhee et al.
Study Selection
Two independent reviewers screened the studies for eligibility, with a third reviewer resolving disagreements between the two primary reviewers. Each article’s title and abstract were reviewed. Articles that could not be excluded at this stage were transferred to full text review (n = 21). Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, Victoria, Australia) was used for the screening and selection process.
Data Extraction and Analysis
The following information was extracted by multiple reviewers: authors, study years, study designs, sample sizes, patient ages, duration of follow-up, types of interbody device and osteobiologic used, indication for surgery, number of levels fused, fusion rates, and definitions of fusion. Descriptive statistics were calculated and reported as appropriate. There was insufficient data to perform a meta-analysis.
Classification of Level of Evidence and Risk of Bias Assessment
Rating and classification of level of evidence and risk of bias assessment for the included studies were carried out using the Oxford Centre for Evidence-Based Medicine (OCEBM)and Methodological Index for Non-Randomized studies (MINORS), respectively. 9
Results
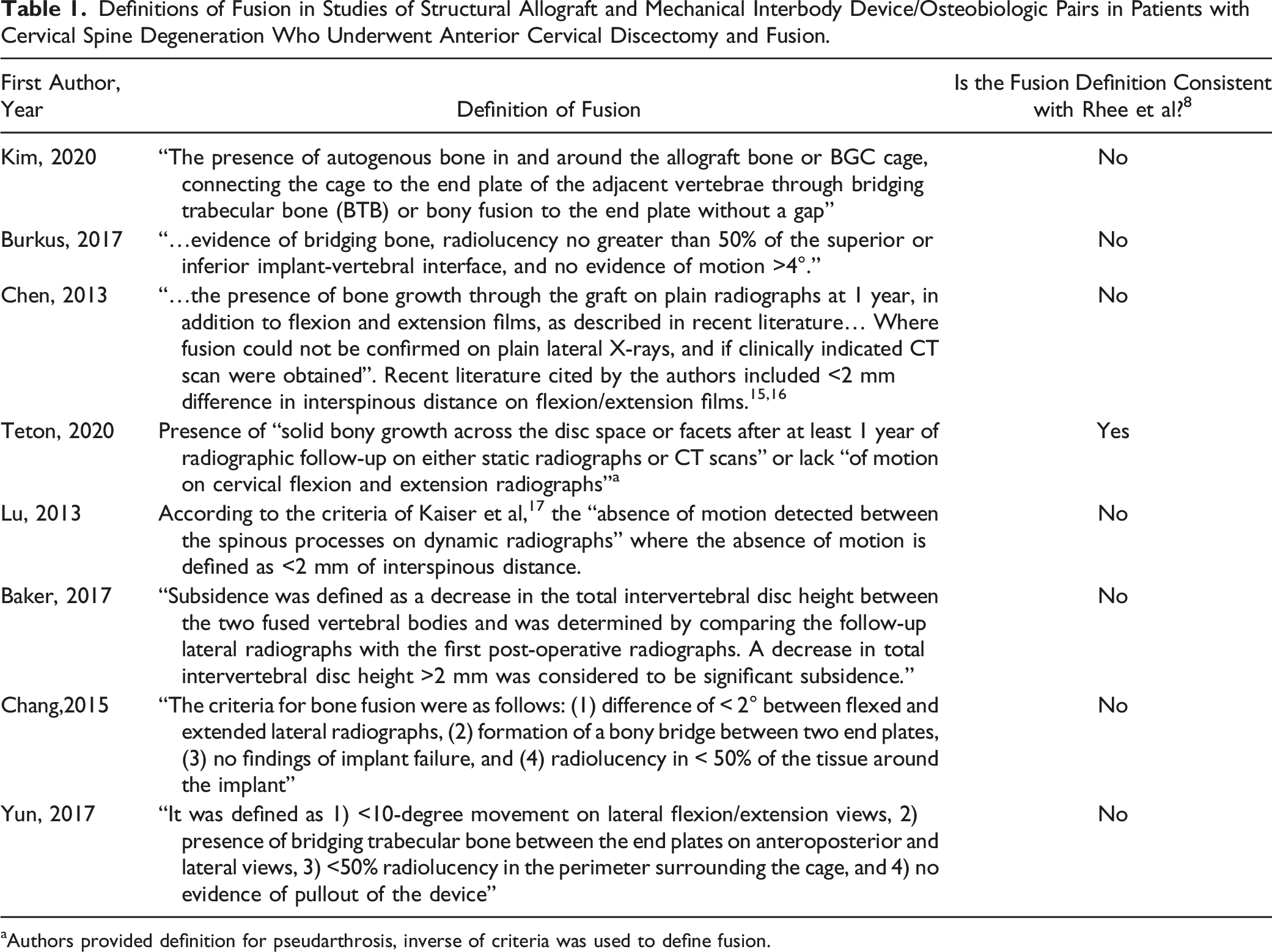
A total of 1306 articles were identified (Figure 1). Eight articles (7 retrospective reviews and 1 prospective historically controlled study) identified that compared fusion rates between structural allograft and a mechanical interbody device/osteobiologic pair met the eligibility criteria and were included.10–14 Criteria for fusion rates differed among the studies, although evidence of bone growth and lack of motion at the level of the procedure were commonly used to determine fusion (Table 1). Only one study used the definition of fusion developed by Rhee et al.
8
Flowchart demonstrating the literature search and article screening process. The purpose was to compare fusion rates of structural allograft vs mechanical interbody devices augmented with an osteobiologic in patients who underwent anterior cervical discectomy and fusion for cervical spine degeneration. Definitions of Fusion in Studies of Structural Allograft and Mechanical Interbody Device/Osteobiologic Pairs in Patients with Cervical Spine Degeneration Who Underwent Anterior Cervical Discectomy and Fusion. aAuthors provided definition for pseudarthrosis, inverse of criteria was used to define fusion.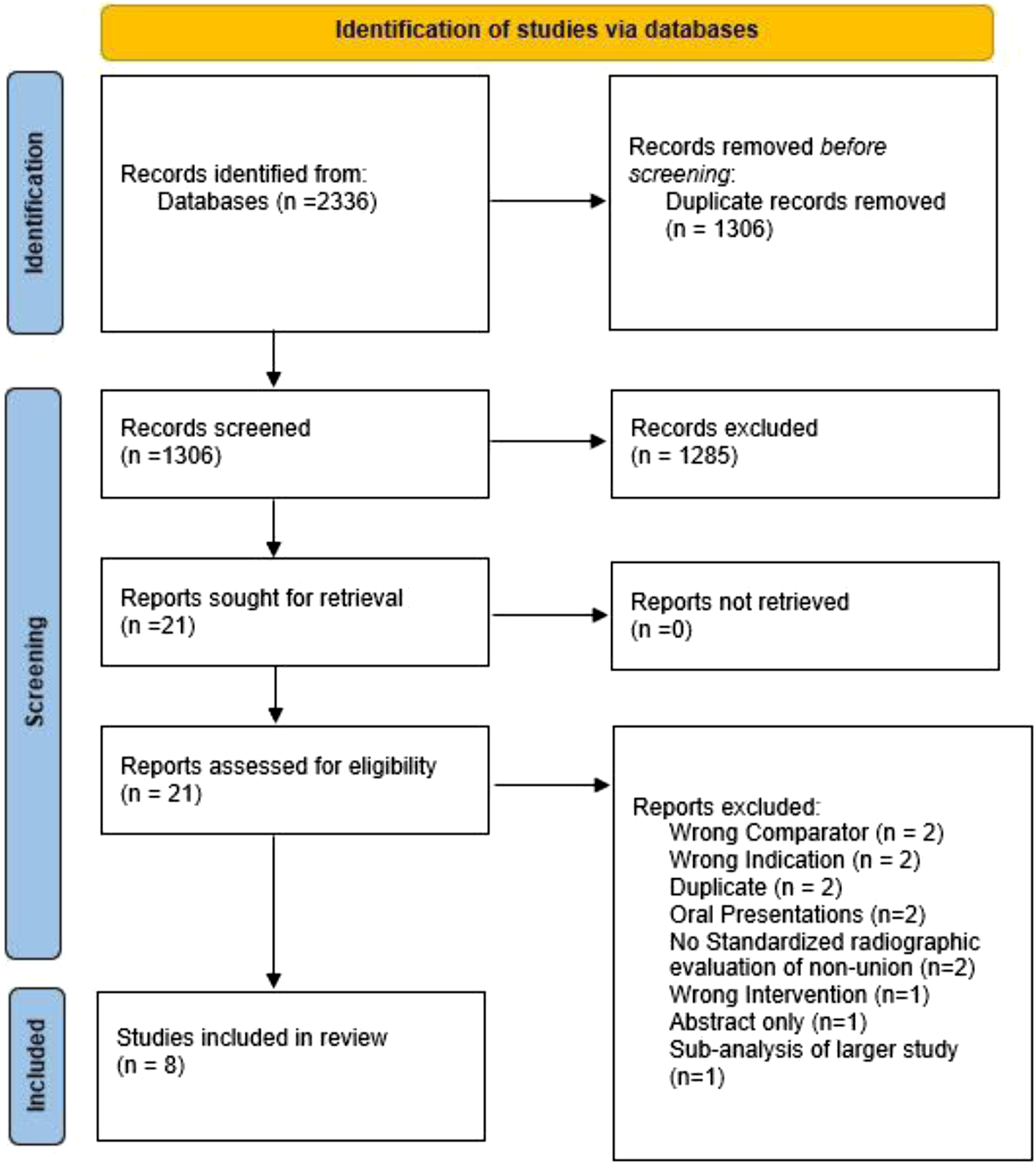
Structural Allograft
Studies of Fusion Rates in Patients Who Underwent Anterior Cervical Discectomy and Fusion for Cervical Spine Degeneration.
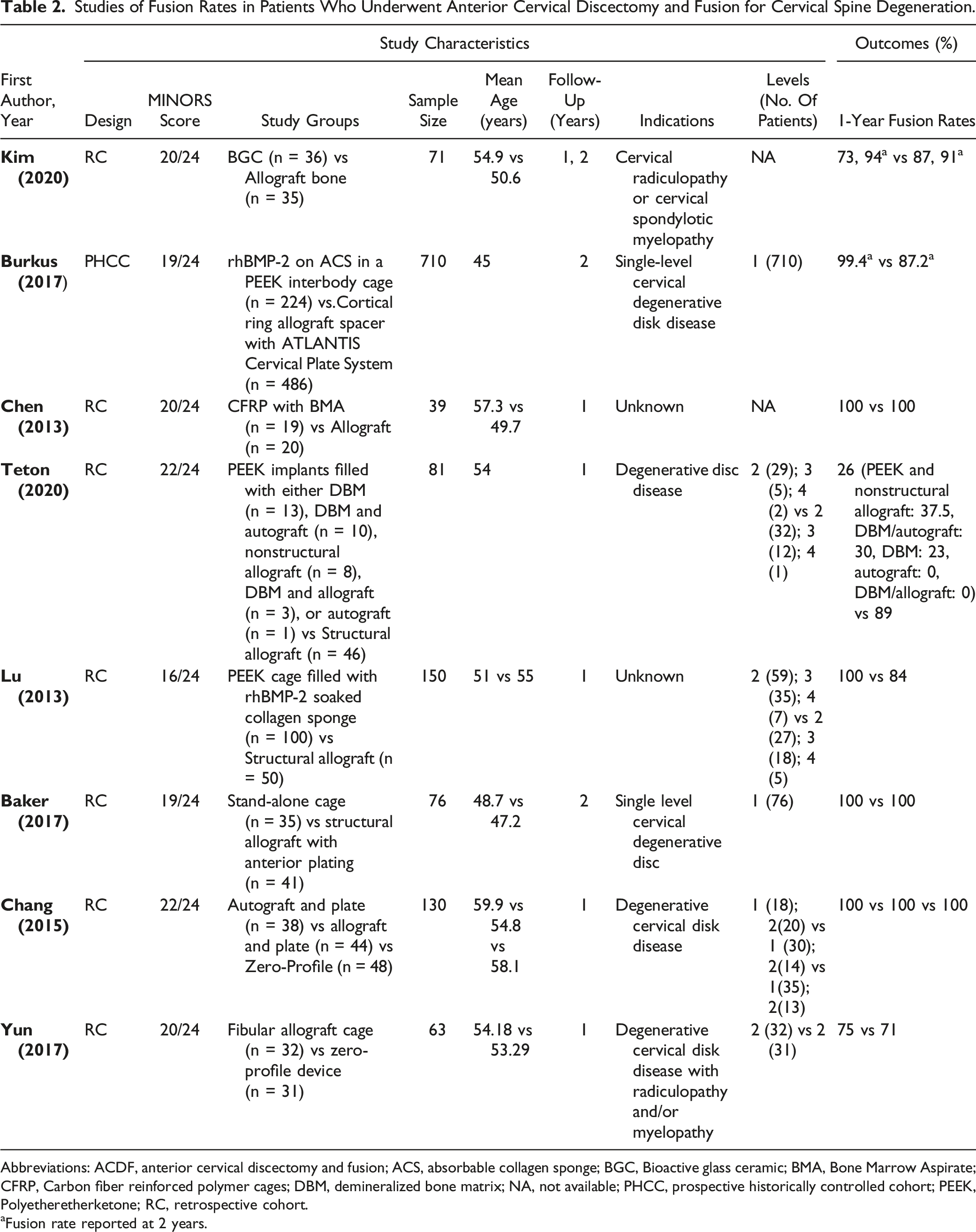
Abbreviations: ACDF, anterior cervical discectomy and fusion; ACS, absorbable collagen sponge; BGC, Bioactive glass ceramic; BMA, Bone Marrow Aspirate; CFRP, Carbon fiber reinforced polymer cages; DBM, demineralized bone matrix; NA, not available; PHCC, prospective historically controlled cohort; PEEK, Polyetheretherketone; RC, retrospective cohort.
aFusion rate reported at 2 years.
A prospective, historically controlled study by Burkus et al using cortical ring allograft spacers for multilevel ACDF reported fusion rates of 87.2% at 2 years. 14 Another retrospective chart review using unspecified allograft bone found a 91% fusion rate at 2 years. 13
PEEK Cages With rhBMP-2 or DBM and Autogenous Bone Graft
Three studies using PEEK interbody devices augmented with osteobiologics met the aforementioned inclusion criteria, including 1 prospective, historically controlled trial 14 and 2 retrospective reviews.10,12 Two studies (n = 324) with patients undergoing multilevel ACDF examined PEEK cages filled with rhBMP-2 on a collagen sponge and reported 1- and 2-year fusion rates of 100% and 99.4%, respectively (Table 2).12,14
In a study by Teton et al, the authors reported 1-year fusion rates for patients undergoing multilevel ACDF using PEEK implants filled with various osteobiologic materials. The treatment groups were defined as PEEK + nonstructural allograft (n = 8), PEEK + DBM and local autograft (n = 10), PEEK + DBM (n = 13), PEEK + autograft (n = 1), and PEEK + DBM and allograft (n = 3). 10 In this study, overall fusion rate was 26% at 1 year. Of the cages that displayed fusion, PEEK + DBM had the lowest fusion rate (23%), while PEEK + nonstructural allograft had the highest (37.5%). PEEK + DBM/allograft and PEEK + autograft cages did not result in fusion (0% fusion rate at 1 year) (Table 2).
Stand-Alone and Zero-Profile Devices
A single retrospective review analyzed the radiographic outcome of patients undergoing ACDF with either a stand-alone (SA) device (n = 35) or traditional cage and plate construct (n = 41) with purpose of measuring implant subsidence. No statistically significant difference between the 2 groups with a mean subsidence, after 2 years, in the SA and traditional cage and plate construct groups of 1.41 and 1.92 mm, respectively. 18
Two retrospective studies looking to evaluate the efficacy of anterior fusion using Zero-Profile devices met the aforementioned inclusion criteria. In a study by Han Chang et al, treatment groups were defined as autograft and plate (n = 38, group A), allograft and plate (n = 44, group B), and Zero-P (n = 48, group C). This study showed that maintenance of entire and segmental lordosis after surgery was better in those groups that did not use the Zero-profile devices. 19 Additionally, they found no significant differences regarding the extent of loss of lordosis from the surgery to the final follow-up. 19 Dong-Ju et al compared zero-profile (n = 31) and cage with plate construct devices (n = 32) for the treatment of contiguous 2-level ACDF. Fusion at 1 year was observed in 75% of the cage with plate construct group and 71% of the Zero Profile group; these results were deemed not significantly different. 18
CFRP With BMA
One retrospective review for patients undergoing ACDF using CFRP filled with BMA (n = 19) was included in our analysis. 11 At 1-year follow-up, the fusion rate was 100% (Table 2).
BGC Cages
One retrospective review using BGC composed of CaO-SiO2-P2O5-B2O3 (n = 36) met our inclusion criteria. 1- and 2-year fusion rates were 73% and 94%, respectively (Table 2). 13
Classification of Level of Evidence
Power Calculation, Sample Size, and Reporting of Patients Lost to Follow-Up.
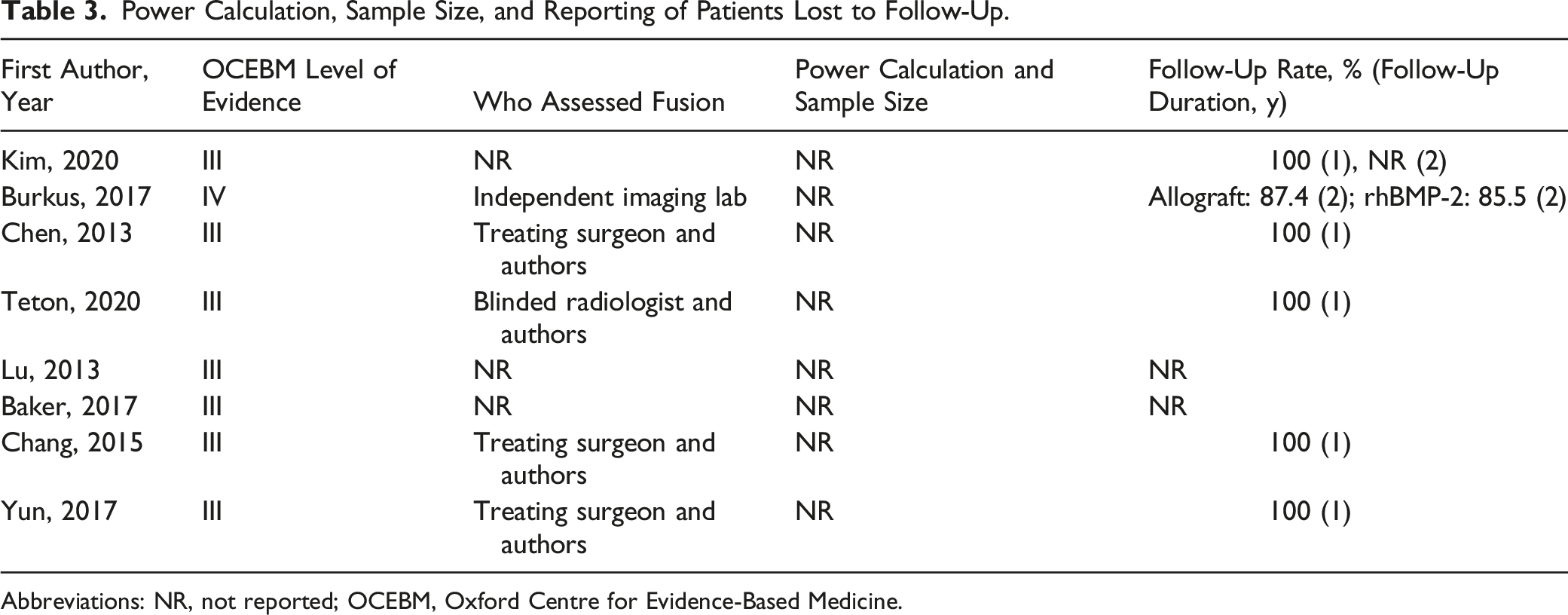
Abbreviations: NR, not reported; OCEBM, Oxford Centre for Evidence-Based Medicine.
Risk of Bias Assessment
Using the Cochrane review guidelines, the 8 included studies were analyzed to check if they have selection, performance, detection, attrition and reporting biases. The 7 retrospective studies included were categorized as having a high risk for selection bias. The prospective, historically controlled study by Burkus et al was deemed to have a low risk for selection bias. There was low risk for performance bias in the 7 retrospective studies because blinding of personnel and participants did not influence the outcome. The prospective, historically controlled study by Burkus et al used the propensity score statistical technique to adjust for potential biases. Yet, this study has higher risk for performance bias due to nonrandomization. Moreover, detection bias was determined to be low risk for the 8 studies. All studies included used data from medical records and databases that have the potential of having high risk for reporting bias.
Discussion
With the expansive use of novel interbody materials and osteobiologics in ACDF, it becomes increasingly important to critically evaluate the association between the use of these materials and subsequent fusion rates. This systematic review of the literature identified studies which examined structural allograft vs alternative interbody material + osteobiologic. A total of 8 studies were included that met our inclusion criteria, with fusion rates in these various studies ranging from 26% 10 to 100%.11,12 Seven out of eight of these studies were retrospective cohort studies,10-13 while one was a prospective, historically controlled cohort study. 14 According to the Centre for Evidence-Based Medicine levels of evidence, these studies were of Level III and IV evidence. The quality of evidence in existing studies demonstrates the clear need for randomized controlled trials on this topic in the future. It was not possible to perform a quantitative meta-analysis due to the heterogeneity of data reporting and the lack of randomized controlled trials.
Most of the studies included in this systematic review reported high 1-year fusion rates for structural allograft (84%–100%), CFRP (100%), BGC (73%), and PEEK cages filled with rhBMP-2 (100%) (Table 2). However, Teton et al reported a 26% fusion rate for PEEK cages augmented with various combinations of DBM, allograft, and autograft, which is different from traditionally reported 1-year fusion rates of 73% for single level ACDF using empty PEEK cages.10,20 The lower fusion rates could possibly be attributed to the fact that the study’s patient population consisted of only multilevel ACDF procedures, which has previously been found to result in lower fusion rates. 21 Despite this, other trials have historically found a fusion rate of 91% for multilevel ACDF using PEEK filled with DBM or bone grafts.21,22 This highlights the need for more studies directly comparing pure structural allograft and PEEK/bone graft combinations in ACDF. Encouragingly, the overall trend of fusion rates in the studies identified in this review is in agreement with the broader literature demonstrating fusion rates ranging from 69% to 100% for mechanical interbody devices such as carbon, ceramic, and PEEK cages augmented with various osteobiologics.23-27
When comparing the studies identified in this systematic review, it is important to mention heterogeneity in the criteria used to define fusion (Table 1). While many criteria have been described for evaluating fusion following ACDF using dynamic radiography,28-30 computed tomography,31-33 and magnetic resonance imaging, 31 the systematic review by Rhee et al in 2015 recommended the following strict definition when using plain radiographs to evaluate fusion following ACDF: “flexion-extension radiographs using the interspinous process method (<1-mm motion difference) regardless of graft or instrumentation type.” 8 While all 8 of the studies discussed in this manuscript used an accepted definition of fusion which was clearly defined in the methodology, only 1/8 studies used the definition recommended by Rhee et al, and only 3/8 studies clearly defined which study member was responsible for determination of fusion (and if they were blinded).
Given the small number of studies on this topic, we mandated that studies included 1-year radiographic follow-up at a minimum rather than the current preferred standard of 2-year follow-up. 34 The study by Burkus et al examined patients up to 2 years, however, <90% of patients achieved follow-up at 2 years or greater. Given that 70% of patients who do not achieve radiographic fusion at 1 year following ACDF will eventually fuse by 2 years, 35 this may have resulted in underreporting fusion rates in some of the studies identified by this systematic review. In future studies, authors should aim to obtain 2-year follow-up although we recognize the logistic challenges of obtaining this goal in a prospectively designed study.
Despite the paucity of high-quality evidence comparing fusion rates of structural allograft and various interbody device/osteobiologic pairs, there are several interesting studies that aim to identify trends in the use of different cage materials for ACDF. In the previously mentioned AOSpine survey of spine surgeons worldwide assessing preferred graft selection in ACDF, 64% of surgeons used cages, of which 84% utilized PEEK and 4.1% used synthetic or other cages. North American surgeons, however, mostly utilized allograft. In addition, 74% of surgeons added a nonstructural osteobiologic material to the graft. Furthermore, this study found that most surgeons are not satisfied with available literature comparing effectiveness of grafts but believed that there was sufficient evidence to support the use of their chosen graft. 2 While changes in standard of care do not always align with the advent of level I evidence, it is our hope that this review highlights the current landscape of evidence that supports the use of PEEK, CFRP, and BGC in addition to osteobiologics as being capable of achieving high rates of fusion following ACDF. 36
Study Limitations
Several limitations of this study should be acknowledged and considered by readers. A meta-analysis was not performed due to heterogeneity in the reviewed studies, especially in the definition of fusion. While this systematic review was comprehensive and performed in alignment with PRISMA guidelines, the lack of any level I randomized studies on this topic limits quantitative conclusions from being drawn when comparing fusion rates among allograft vs the various comparison groups. We also recognize that there are many important clinical outcomes aside from fusion rate and chose not to examine these as part of this systematic review given that clinical outcomes reporting is likely to be even more varied than fusion rate which can be more objectively and reproducibly assessed.
Conclusion
Through a systematic review of the literature, 8 studies were identified comparing structural allograft and mechanical interbody cages in single and multilevel ACDF patients meeting inclusion criteria and reporting a standard definition of fusion. Fusion rates for groups identified in these studies ranged from 84 to 100% for structural allograft, while most interbody device/osteobiologic pairs had fusion rates between 26 and 100%. Prospective, randomized studies are necessary to study this topic further as none were identified in the literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Each author certifies that he or she has no commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements) that might pose a conflict of interest in connection with the submitted article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine experts.