
Abstract
Study Design:
Retrospective cohort study.
Objectives:
Anterior cervical discectomy and fusion (ACDF) demonstrates reliable improvement in neurologic symptoms associated with anterior compression of the cervical spine. There is a paucity of data on outcomes following 4-level ACDFs. The purpose of this study was to evaluate clinical outcomes for patients undergoing 4-level ACDF.
Methods:
All 4-level ACDFs with at least 1-year clinical follow-up were identified. Clinical outcomes, including fusion rates, neurologic outcomes, and reoperation rates were determined.
Results:
Retrospective review of our institutional database revealed 25 patients who underwent 4-level ACDF with at least 1-year clinical follow-up. Average age was 57.5 years (range 38.2-75.0 years); 14 (56%) were male, and average body mass index was 30.2 kg/m2 (range 19.9-43.4 kg/m2). Two (8%) required secondary cervical surgery at an average of 94.5 days postoperatively while the remaining 23 did not with an average follow-up of 19 months. Of 23 patients not requiring revision surgery, 16 (69%) patients fused by definition of less than 1 mm of spinous process motion per fused level in flexion and extension. Fifteen (65%) had at least one muscle group with one grade of weakness preoperatively. Nineteen of these patients (83%) had improved to full strength while no patients lost muscle strength.
Conclusions:
Review of our institution’s experience demonstrated a low rate of revision cervical surgery for any reason of 8% at mean 19 months follow-up, and neurological examinations consistently improved, despite a high rate of radiographic nonunion (31%).
Introduction
Anterior cervical discectomy and fusion (ACDF) is a commonly performed procedure for cervical radiculopathy or myelopathy arising from anterior compressive pathology at the level of the disc space in the cervical spine. 1 –6 In the appropriately selected patient, an ACDF has been associated with significant improvements in the symptoms of radiculopathy and myelopathy, as well as health-related quality of life (HRQOL) outcome measures. 7 –11 Patients with multilevel cervical spondylosis may require multilevel ACDF.
ACDF involving multiple levels has been associated with high rates of pseudarthrosis, which can be associated with neck pain and recurrent symptoms referable to the index surgical levels. 12 –14 Increased nonunion rates have been associated with increasing the number of cervical motion segments in the fusion construct. 12,15,16 The failure of fusion in longer segment anterior constructs has been attributed to greater surface area required for fusion, multiple mobile segments, and an increased moment arm across the fusion construct. 16 Pseudarthrosis rates after ACDF vary based on the number of segments fused; from 0% to 10% for single levels 15,17 –19 and up to 50% for 3-level constructs. 12 –14 Combined anterior-posterior circumferential fusion has been advocated for improved fusion rates and symptomatic relief in patients with multilevel cervical spondylotic disease. 16,20 –22 Though, the additional posterior cervical procedure is not the potential for increased morbidity. 23 –25
There is a dearth of outcomes data following 4-level ACDFs for multilevel cervical spondylotic disease. 26,27 Bolesta et al 13 demonstrated a radiographic nonunion rate of 47% among 15 patients who underwent noninstrumented 3- or 4-level ACDF with iliac crest autograft. 13 However, 2 more recent retrospective studies reported a radiographic fusion rate of 92% in 29 patients 26 and 86% in 26 patients 27 undergoing 4-level ACDF. No patients in either study required secondary cervical procedure for pseudarthrosis or recurrent symptoms. Given the dichotomy of reported radiographic outcomes and minimal data on clinical outcomes following 4-level ACDF, this study was designed to evaluate clinical outcomes following 4-level ACDF without a supplemental posterior fusion at our institution. Specifically, we evaluated the need for secondary cervical procedures, evidence of radiographic fusion, and improvement in preoperative motor examination.
Methods
Following approval from the institutional review board, a retrospective investigation of clinical and operative notes was performed to identify all patients undergoing a 4-level ACDF at a single academic institution between January 1, 2010 and December 31, 2014. All patients who underwent 4-level ACDF for treatment of cervical spondylosis with myelopathy and/or radiculopathy with at least 1 year of clinical follow-up were included. All patients presenting with clinical symptoms of radiculopathy and/or myelopathy were evaluated with flexion and extension radiographs, cervical magnetic resonance imaging, and electromyograms, when indicated, to confirm contributing cervical pathology. Patients were indicated for a 4-level ACDF if they demonstrated symptoms of radiculopathy and/or myelopathy consistent with multilevel anterior cervical spine compression on magnetic resonance imaging, loss of normal cervical lordosis, and absence of ossified posterior longitudinal ligament. Patients undergoing 4-level ACDF with a single corpectomy were also included; all 2- and 3-level corpectomy patients were excluded. All patients underwent instrumented ACDF using premachined cortical allograft. Patients undergoing surgery for a tumor, trauma, infection, revision surgery and patients who had a concomitant posterior surgery were not included.
Patient demographic information; age, sex, body mass index (BMI), smoking status, age-adjusted Charleson Comorbidity Index (CCI), 28,29 and preoperative motor strength measured by manual muscle testing (MMT) 30 were collected. Cervical segments fused for the each identified procedure was noted based on operative reports.
Primary outcomes measured included need for secondary cervical procedure, radiographic evidence of fusion, and change in preoperative motor examination. Patients requiring a secondary cervical procedure during the study period were identified along with associated diagnosis and secondary procedure. In accordance with the recommendations of the Cervical Spine Research Society (CSRS) Special Projects Committee, radiographic fusion was determined based on motion less than 1 mm between the spinous processes for each level of fusion as measured on most recent flexion and extension radiographs, or based on the presence of bridging bone in 2 planes on computed tomography scan, when available. 31 All patients demonstrating fusion by the above criteria had at least 4 mm of motion at an adjacent unfused segment to ensure appropriate effort consistent with CSRS criteria. 31 Radiographic evaluation of fusion was performed by 2 surgeons, one of whom was not involved in the patients care, in a blinded fashion.
Mann-Whitney and Fisher’s exact test were performed to assess for significant relationship between variables; age, BMI, CCI, and smoking status, between those who demonstrated radiographic fusion and those with pseudarthrosis. Significance was set at P = .05. Statistical analysis was performed by a single statistician, using R 3.2.3 software (R Foundation for Statistical Computing, Vienna, Austria).
Surgical Technique
Patients were placed supine with a bump placed transversely under the scapula providing appropriate neck extension. The shoulders were taped. Somatosensory-evoked potential monitoring was used in all cases. A left-sided transverse incision is used, and the anterior cervical spine exposed using a Smith-Robinson approach. 32 Caspar pins are placed in a slightly convergent manner in order to restore lordosis with distraction. Discectomies are performed under microscopic magnification. Precontoured lordotic machined allografts were used in the majority of cases. Tricortical iliac crest autograft was selected in patients who were current smokers or had poor bone quality. In patients undergoing corpectomy, premachined iliac crest strut allograft was used as necessary. A lordotic contoured 4-level anterior cervical plate was selected. The most cephalad and caudad screws were placed first, followed by intermediate screws allowing restoration of lordosis as the intermediate vertebral segments were reduced to the plate. A Jackson Pratt type drain was routinely used and patients were admitted for 1 to 2 nights in the hospital. Postoperatively, patients were maintained in a hard cervical collar for 4 weeks and then transitioned to a soft collar for an additional 2 weeks.
Figure 1 demonstrates pre- and postoperative imaging of a patient indicated for 4-level ACDF.
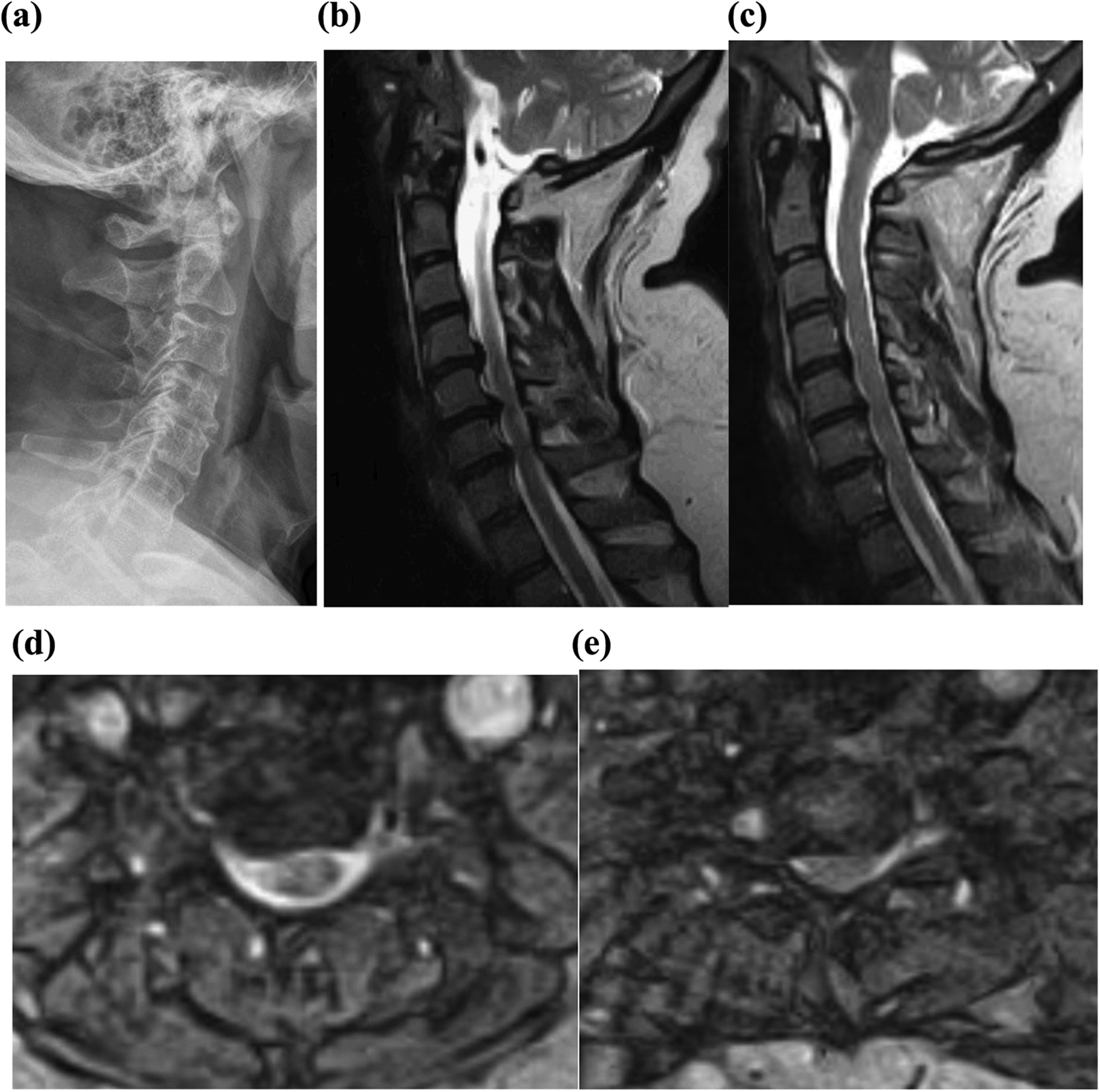
A 52-year-old woman presents with 9 months of worsening right-sided radicular symptoms in the distribution of the fifth and seventh cervical nerves, deltoid and triceps weakness. The patient also complains of gait imbalance and demonstrates hyperreflexia consistent with myelopathy. (a) Preoperative lateral radiograph demonstrating spondylosis most pronounced at C4/5, C5/6, and C6/7. (b) A T2-weighted midsagittal magnetic resonance imaging (MRI) scan demonstrating C4-C5, C5-6, C6-7 central disc herniation with moderate to severe stenosis with evidence of cord compression at C6-7. (c) A T2-weighted parasagittal MRI demonstrating paracentral disc herniation at C3-C4 with moderate central stenosis. (d) A T2-weighted axial image of the C5/6 disc space demonstrated moderate right-sided foraminal stenosis. (e) A T2-weighted axial image of the C6/7 disc space demonstrated severe right-sided foraminal stenosis.
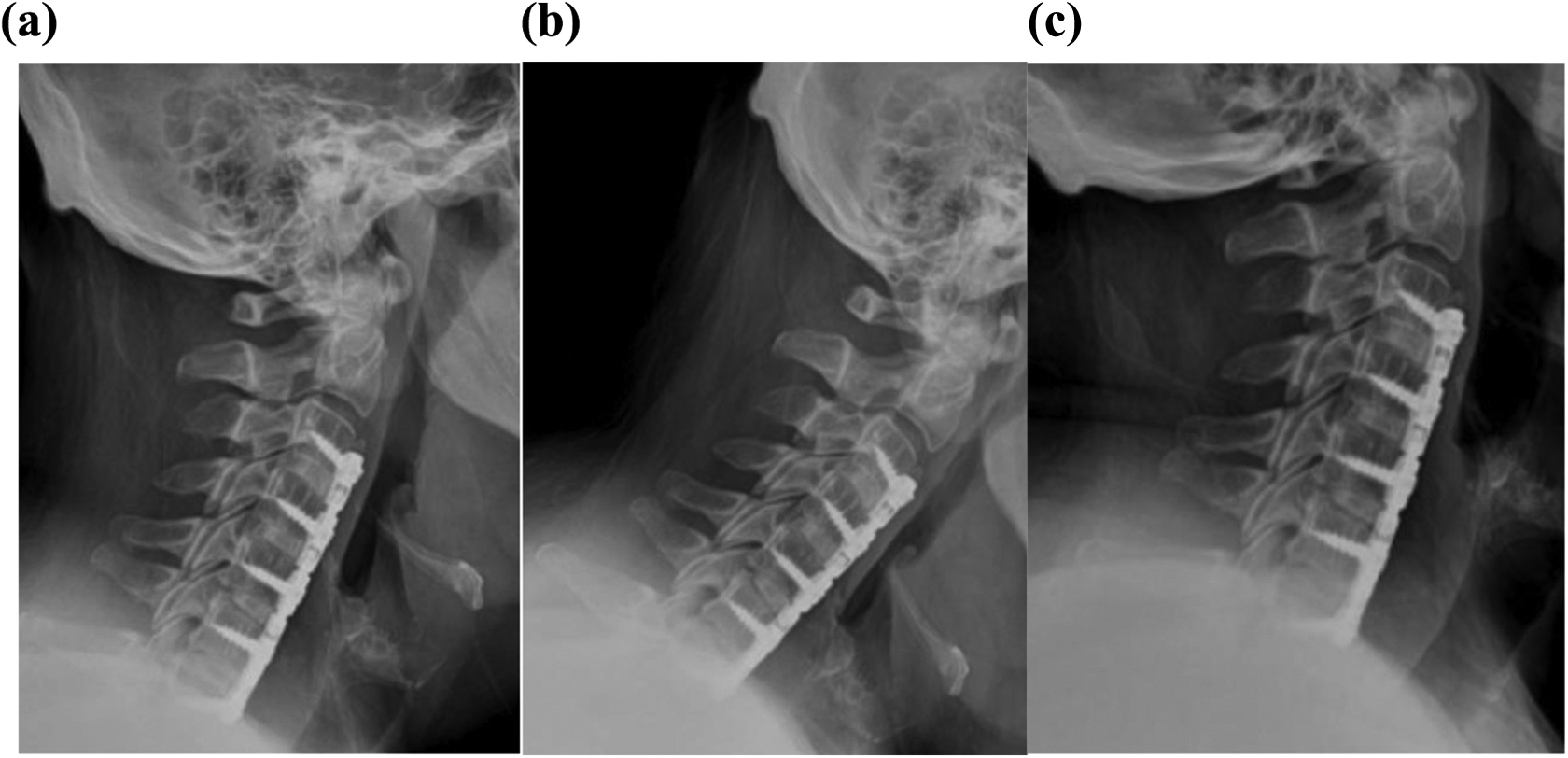
(a) A lateral radiograph taken 1-year postoperatively after anterior cervical discectomy and fusion between the C3/4, C4/5, C5/6, and C6/7 vertebrae. Interbody grafts demonstrate evidence of bridging bone, lack of periprosthetic lucency, or loosening consistent with fusion. (b) Lateral flexion and (c) lateral extension radiographs demonstrated motion less than 1 mm between spinous processes of fused levels consistent with fusion. 28
Results
Demographics
Retrospective review of our institutional database revealed 29 patients who underwent a standalone 4-level ACDF without a posterior fusion between 2010 and 2014, 25 of these patients had at least 1 year of clinical follow-up. There were 18 C3/7 fusions (72%), 2 C4/T1 fusions, 1 C2/6 fusion, 3 C3/7 fusions with C4 corpectomy, and 1 C3/7 fusion with C6 corpectomy. The average patient age was 57.5 years (range 38.2-75.0 years), average BMI was 30.2 kg/m2 (range 19.9-43.3 kg/m2) and age-adjusted CCI was 2.5 (range 0-7). Fourteen patients (56%) were male and 22 (88%) identified as Caucasian. A total of 3 patients were current smokers at the time of surgery and 8 had a smoking history (Table 1).
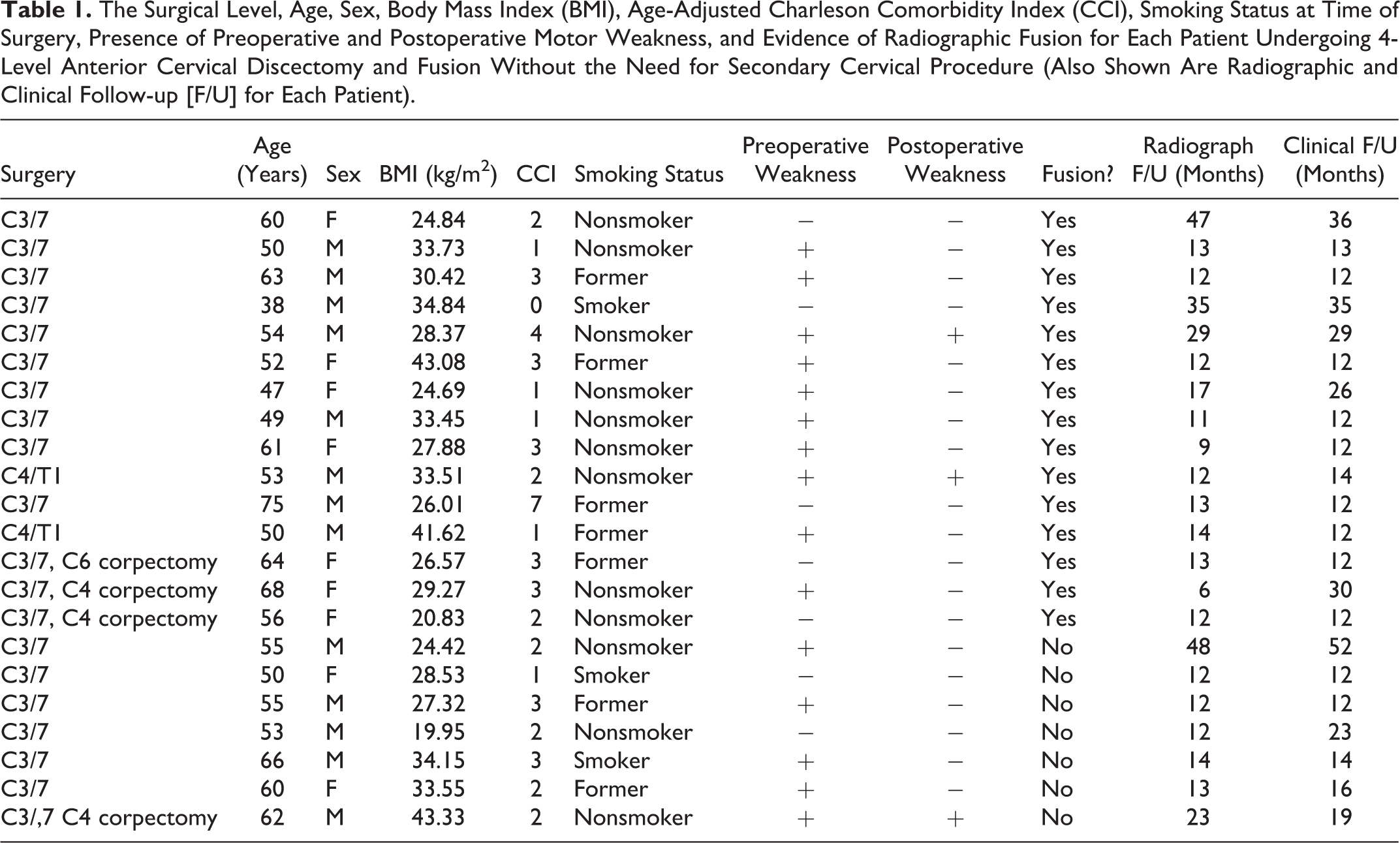
The Surgical Level, Age, Sex, Body Mass Index (BMI), Age-Adjusted Charleson Comorbidity Index (CCI), Smoking Status at Time of Surgery, Presence of Preoperative and Postoperative Motor Weakness, and Evidence of Radiographic Fusion for Each Patient Undergoing 4-Level Anterior Cervical Discectomy and Fusion Without the Need for Secondary Cervical Procedure (Also Shown Are Radiographic and Clinical Follow-up [F/U] for Each Patient).
Outcomes
Two of the 25 patients (8%) required secondary cervical procedure at an index level in the follow-up period. One patient required a posterior cervical decompression and fusion from C3-C7 on postoperative day 21 after initial ACDF from C3-C7, for persistent spinal cord compression and symptoms of myelopathy. The second patient required a posterior cervical fusion C2-C7 with bilateral foraminotomy at the C6-C7 level 5.5 months after the index ACDF from C3-C7, due to increasing neck pain and recurrence of radicular symptoms in the setting of a C6/7 pseudarthrosis. This secondary posterior cervical procedure was complicated by wound drainage requiring posterior cervical irrigation, debridement, and closure on postoperative day 19 (Table 2). Both patients requiring secondary procedure demonstrated at least one grade of motor weakness in major muscle group by MMT during initial examination. Both demonstrated full motor strength and improvement in myelopathy and neck pain symptoms respectively at most recent clinic visit. Twenty-three (92%) of patients had not required revision surgery at an average follow-up of 19 months.
The Index Procedure, Demographic Information, Diagnosis, Secondary Procedure, and Associated Postoperative Day for the 2 Patients Requiring Secondary Cervical Procedure.a
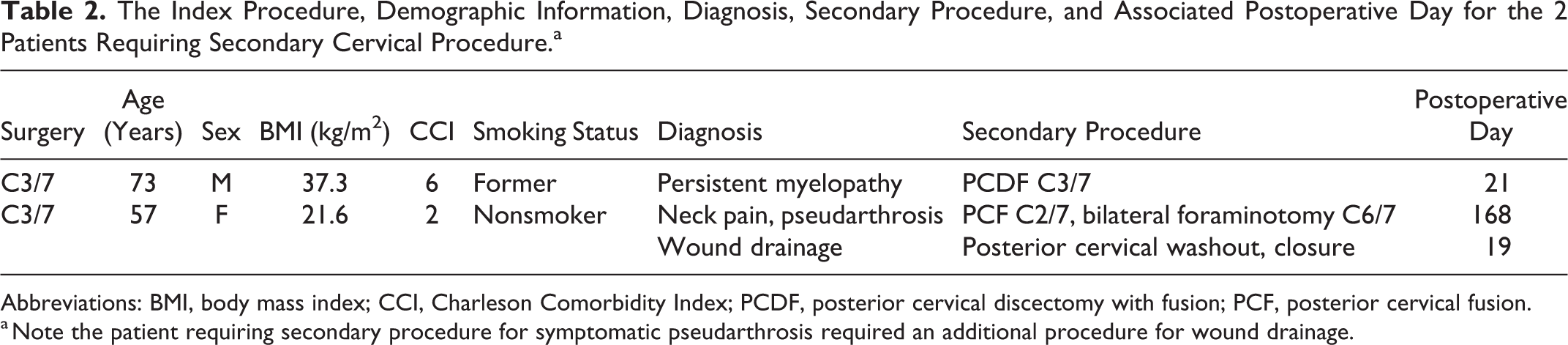
Abbreviations: BMI, body mass index; CCI, Charleson Comorbidity Index; PCDF, posterior cervical discectomy with fusion; PCF, posterior cervical fusion.
a Note the patient requiring secondary procedure for symptomatic pseudarthrosis required an additional procedure for wound drainage.
The 23 patients not requiring secondary cervical procedure had an average radiographic follow-up of 17.3 months (range 6-48 months). Sixteen of these patients (69%) patients demonstrated radiographic fusion by definition of less than 1 mm of spinous process motion per fused level in flexion and extension. Four of these 23 patients had clinical but not radiographic follow-up of at least 1 year. They demonstrated fusion on most recent radiographic evaluation and were therefore included in the analysis. One of the 4 patients who underwent concomitant corpectomy demonstrated radiographic nonunion (Table 1).
There was an insignificant association between smokers and radiographic fusion. Two of the 3 active smokers (66%) demonstrated nonunion on most recent radiographic follow-up (P = .89). There was no association between age (P = .671), BMI (P = .821), or age-adjusted CCI (P = .791) and radiographic fusion (Table 3).
The Number of Patients Who Underwent 4-Level Anterior Cervical Discectomy and Fusion Not Requiring Secondary Surgery, With Radiographic Evidence of Fusion and Those Demonstrating Pseudarthrosis With Associated Mean (±SD) Age, Body Mass Index (BMI), Smoking Status, and Distribution of Age-Adjusted Charleson Comorbidity Index (CCI).a
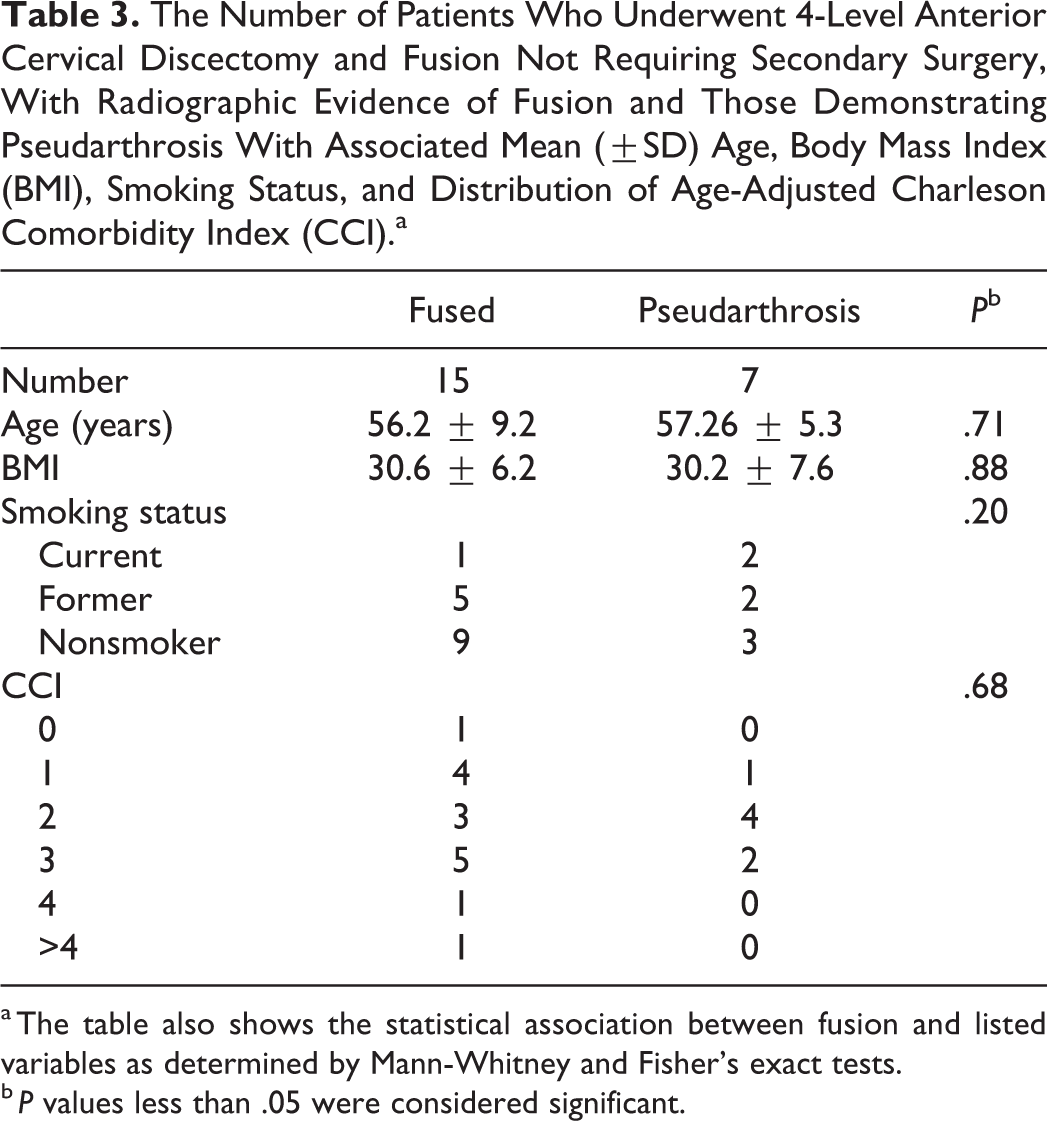
a The table also shows the statistical association between fusion and listed variables as determined by Mann-Whitney and Fisher’s exact tests.
b P values less than .05 were considered significant.
Of the 23 patients not requiring revision surgery, 15 (65%) had at least one muscle group with one grade of weakness on preoperative clinical exam. All patients who demonstrated preoperative motor weakness demonstrated improvement postoperatively. Nineteen of these patients (82.6%) demonstrated full strength. No patients demonstrated new or worsening muscle strength at an average of 19 months’ follow-up.
Discussion
ACDF demonstrates reliable improvement of radicular and myelopathic symptoms in the appropriately selected patients with cervical spondylosis. 7 –11 Those patients with multilevel disease may require multilevel ACDF. As the size of the anterior fusion construct increases, so does the rate of pseudarthrosis, increasing the risk of persistent symptoms and need for revision cervical procedure. 13,14,16 Some surgeons advocate a combined anterior and posterior procedure in patients with multilevel disease, though circumferential procedures may be associated with additional morbidity. 23 –25 The results of this study suggest that despite a high nonunion rate (31%), 4-level ACDF was associated with a low revision rate (8%) and excellent neurologic outcomes. Furthermore, only one of the revisions was due to symptomatic nonunion.
There are few studies reporting the clinical outcomes of patients undergoing standalone four level ACDF. 13,26,27,33 Chang et al 26 retrospectively reported on 29 patients indicated for a 4-level ACDF for radiculomyelopathy. They demonstrated a high fusion rate (92.6%) and improvement in neurologic symptoms in 88% of patients at mean radiographic follow-up of 20 months. All patients underwent instrumented ACDF using corticocancellous auto or allograft. Previous studies have demonstrated a wide range of fusion rates (47%-94%) 13,26,27,33 in patients undergoing 4-level ACDF. The postoperative fusion rate of our large retrospective study is on the lower end of the previously reported range (69%). The low fusion rate in this study may be attributed to the strict criteria for a solid fusion, defined as more than 1 mm of motion at each level fused on flexion/extension radiographs defined as a nonunion, consistent with CSRS fusion criteria. 31 Comparatively, Chang et al 26 reported much higher fusion rates using more liberal criteria for determining a solid fusion, including absence of motion, bridging trabeculae, or lack of lucency across the fusion site, and nondescript use of radiographs. 27 A retrospective evaluation of 32 patients undergoing 4-level ACDF by Wang et al 33 demonstrated a fusion rate of 94%. All patients underwent instrumented fusion using polyetheretherketone (PEEK) interbody cage and iliac crest autograft. Fusion criteria also involved absence of motion, bridging trabeculae, or lack of lucency across the fusion site. 33 Given that 1- and 2-level instrumented ACDF is associated with fusion rates between 90% and 97%, 14,15,18,19 it is unlikely that 4-level ACDF results in comparable fusion rates. Previous studies may be overestimating fusion rates due to more liberal fusion criteria.
Not surprisingly, we observed an association, although insignificant, between active smoking status and radiographic nonunion after 4-level ACDF. Several studies have demonstrated an association between smoking and decreased rates of union after anterior cervical spine fusion 21,34 –37 ; Hilibrand et al 21 demonstrated decreased fusion rates in active smokers who underwent multilevel noninstrumented ACDF compared with nonsmokers as measured by motion on lateral radiographs (P < .02). There was no difference in those patients who underwent multilevel ACDF with concomitant corpectomy; both smokers and nonsmokers demonstrated fusion rates of 93%. The authors suggested that reducing the number of healing surfaces with concomitant corpectomy can mitigate the detrimental effect of smoking on fusion. 21 Comparatively, Luszczyk et al 38 performed a large review of 573 patients who underwent single-level ACDF with allograft and plate fixation from the control groups of 5 separate prospective randomized Food and Drug Administration investigational device exemption studies; demonstrating no difference in fusion rates between smokers, 91%, and nonsmokers, 91.6%. Two of the 3 active smokers (66%) demonstrated evidence of pseudarthrosis at minimum 1-year follow-up; a larger patient cohort is necessary to demonstrate statistical significance.
Two patients in our study required secondary cervical surgery during the study period evaluated, one for persistent myelopathy and one for symptomatic pseudarthrosis. A large prospective randomized controlled trial by Murrey et al 18 evaluating outcomes of single-level ACDF and cervical disc arthroplasty for single level cervical spondylosis demonstrated a similar rate of both index and adjacent level secondary cervical procedure, 8.5%, for patients randomized to ACDF at 24 months postoperatively. Of the 106 patients randomized to single level ACDF, 6 (5.7%) patients required secondary procedure for symptoms associated with pseudarthrosis. However, these were single-level ACDF procedures, which should have a lower rate of nonunion that a 4-level ACDF. Similarly, a meta-analysis by Gao et al 39 evaluating outcomes of single-level ACDF versus cervical disc arthroplasty demonstrated a similar rate of secondary cervical procedure, between 2% and 11%, for all patients undergoing single level ACDF at 24 months postoperatively. In the retrospective review by Chang et al, 26 2 of 29 patients (6.9%), who underwent 4-level ACDF required reoperation for hematoma evacuation while another patient required revision surgery for hardware loosening at 6 years postoperatively. Additionally, 1 of the 32 patients reported by Wang et al 33 required reoperation for hematoma in the immediate postoperative period, while 3 required posterior cervical procedure for symptom recurrence at a mean 69 months’ follow-up. We demonstrate a comparable and acceptable rate of secondary cervical surgery for patients undergoing 4-level ACDF.
Although we demonstrated a high radiographic nonunion rate, patient clinical outcomes were reassuring. Of the patients not requiring revision surgery, 65% demonstrated preoperative motor function deficit, similar to the incidence reported by previous studies of patients undergoing 4-level ACDF. 26,27 All patients with preoperative motor deficit demonstrated improvement in strength postoperatively with 82.6%, demonstrated improvement to full strength at the final postoperative visit. Of the 2 patients requiring reoperation, both demonstrated improvement in strength after initial anterior procedure and neither demonstrated new weakness. Previous studies have demonstrated reliable improvement in preoperative motor deficit in patients undergoing ACDF for radiculopathy and myelopathy. 11,26 A retrospective review by Lehman et al 11 demonstrated improvement in preoperative motor deficit in 95% of patients undergoing single-level ACDF at 1-year follow-up. Both previous studies reporting exclusively on patients undergoing 4-level ACDF demonstrated a high rate of improvement in preoperative motor and sensory symptoms (88%). 26,33 We demonstrate a similar rate of motor deficit recovery. Patients who underwent 4-level ACDF demonstrated reliable improvement of preoperative motor deficit, similar to those with smaller fusion constructs.
This study is limited by its retrospective design, reliance on radiographic and physical examination findings, and availability of long-term follow-up data. Nonunion was determined based on motion across fused levels according to the CSRS Special Projects Committee criteria. 31 It is possible that reduced motion on postoperative flexion-extension radiographs due to neck pain may limit or underscore this radiographic determination. All patients demonstrated preserved motion at an adjacent level to limit this effect. Two patients demonstrating evidence of radiographic nonunion had 12-month radiographic follow-up available. This short-term follow-up may be overestimating the rate of nonunion and longer postoperative follow-up may demonstrate higher fusion rates. Future studies may evaluate postoperative fusion based on computed tomography scan findings, providing a more accurate assessment of fusion. Nevertheless, we demonstrate successful clinical outcomes following 4-level ACDF.
Conclusion
Review of our institution’s experience demonstrated successful clinical outcomes following 4-level ACDF. We found a low rate of revision cervical surgery for any reason of 8% at an average of 19 months follow-up, and neurological examinations consistently improved, despite a high rate of radiographic nonunion (31%). The low revision rates and successful clinical outcomes suggest that a 4-level ACDF without posterior fusion is a viable option for multilevel cervical spondylotic disease, and that the increased morbidity of a posterior stabilization procedure may not be necessary for most of these patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.