
Abstract
Study Design:
Retrospective cohort study.
Objective:
To evaluate inpatient outcomes in dialysis dependent patients undergoing elective cervical spine surgery.
Methods:
A total of 1605 dialysis dependent patients undergoing elective primary or revision cervical spine surgery for degenerative conditions were identified from the National Inpatient sample from 2002 to 2012 and compared to 1 450 642 nondialysis-dependent patients undergoing the same procedures. The National Inpatient Sample is a de-identified database; thus, no institutional review board approval was needed.
Results:
Dialysis dependence was associated with higher inpatient mortality rates (7.5% vs 1.9%; P < .001) as well as both major (17.3% vs 0.6%; P < .001) and minor (36.8% vs 10.5%; P < .001) complication rates as compared with nondialysis-dependent patients. Dialysis-dependent patients had substantially increased mean lengths of stay (9.8 days compared with 2.0 days; P < .001) and total hospital charges ($141 790 compared with $46 562; P < .001).
Conclusion:
Dialysis-dependence is associated with drastically increased complication rates, risk of mortality, and represent a significant financial and psychosocial burden to patients undergoing elective cervical spine surgery. Both surgeons and patients should be aware of these risks while planning elective surgeries.
Keywords
Introduction
Dialysis dependence is often a barrier to successful outcomes in orthopedic surgery. The associated poor health status, medical complexity, and dysfunctional bone metabolism provide a poor milieu for remodeling and fusion. Comorbidities such as diabetes mellitus, hypertension, cardiovascular disease, anemia, malnutrition, 1 and immune dysfunction are commonplace and further complicate the clinical management of this patient population. 2 End-stage renal disease (ESRD) is an unfortunately common condition. Statistics from 2013 cite a yearly prevalence of 117 162 and a growing incidence exceeding 660 000. Over 88% of new cases are initially treated with hemodialysis. 3 While the comorbidity profile clearly denotes an increased general risk for surgery, the effects of chronic hemodialysis on the postoperative outcomes of elective spine surgery have been only partially investigated. 4
Elective cervical spine surgery is performed to improve functional outcomes such as pain, sensory loss, and weakness. 5 In this regard, it has been shown that spinal surgery can be efficacious for patients on dialysis. However, complication rates are significantly higher. Spinal surgery in adult patients with renal failure is associated with higher rates of morbidity and mortality. 6 -12 Dialysis dependence is also independently predictive of longer hospital stays, complications, and reoperations. 13,14 Additionally, chronic renal failure and uremia have a disruptive effect on endocrine signaling and bone metabolism. 15 -18 As a result, successful fusion is less frequent in this population. 1,19 -23 Furthermore, revision spinal surgery is more commonly necessitated in dialysis-dependent patients, typically portending a poorer outcome than a successful index operation. 24,25 Specifically, adjacent segment destructive changes may necessitate extension of the cervical fusion at some point. 26 Long-term hemodialysis is associated with destructive spondyloarthropathy (DSA), a pattern of calcium and amyloid deposition that causes severe degenerative changes in the cervical spine. Despite these limitations, it has been shown that dialysis patients, with and without DSA, gain meaningful functional benefits from surgical treatment. 19,27
Previous studies have shown that dialysis dependence is associated with complications in elective cervical spinal surgery. 28 An accurate estimation of risk in this population is critical in individualizing patient management and shared decision making. In addition, initiatives to contain health care costs require adequate outcome data regarding elective surgeries in complex patients to forecast the utility of these procedures. 29 -33 The authors previously investigated inpatient outcomes between these two populations undergoing elective lumbar spine surgery. 4 The goal of the current study was to compare the outcomes of cervical spine surgery in dialysis-dependent patients to the normal population using the National Inpatient Sample (NIS). We hypothesized that postoperative complications and mortality rates would be higher in dialysis-dependent patients following elective cervical spinal surgery.
Materials and Methods
Population Selection
Data from the NIS was retrospectively queried for all patients who had undergone elective primary or revision cervical spine surgeries for degenerative conditions between 2002 and 2012. The NIS is a stratified survey of approximately 20% of all US hospitals that includes patient data and discharge information from over 7 000 000 hospital admissions each year. This sampling method represents an estimated 100% of all hospital discharges in the United States. All numbers presented in this study are national estimates, based on NIS provided sampling weights.
Inclusion and Exclusion Criteria
Patients were identified by recorded Clinical Procedural Terminology codes for anterior cervical discectomy and fusion (ACDF), as well as cervical posterior spinal fusion. Those diagnosed with cervical degenerative diseases were selected from this sample on the basis of International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes. 34 Patients with nonelective admissions were subsequently excluded, as well as ICD-9-CM diagnosis codes for vertebral fractures and spinal infections in an attempt to isolate an elective-only sample population. Last, the sample was divided into 2 cohorts based on the ICD-9-CM code for ESRD requiring chronic dialysis. All ICD-9 codes used to select our sample are presented in Table 1.
Inclusion and Exclusion Criteria.
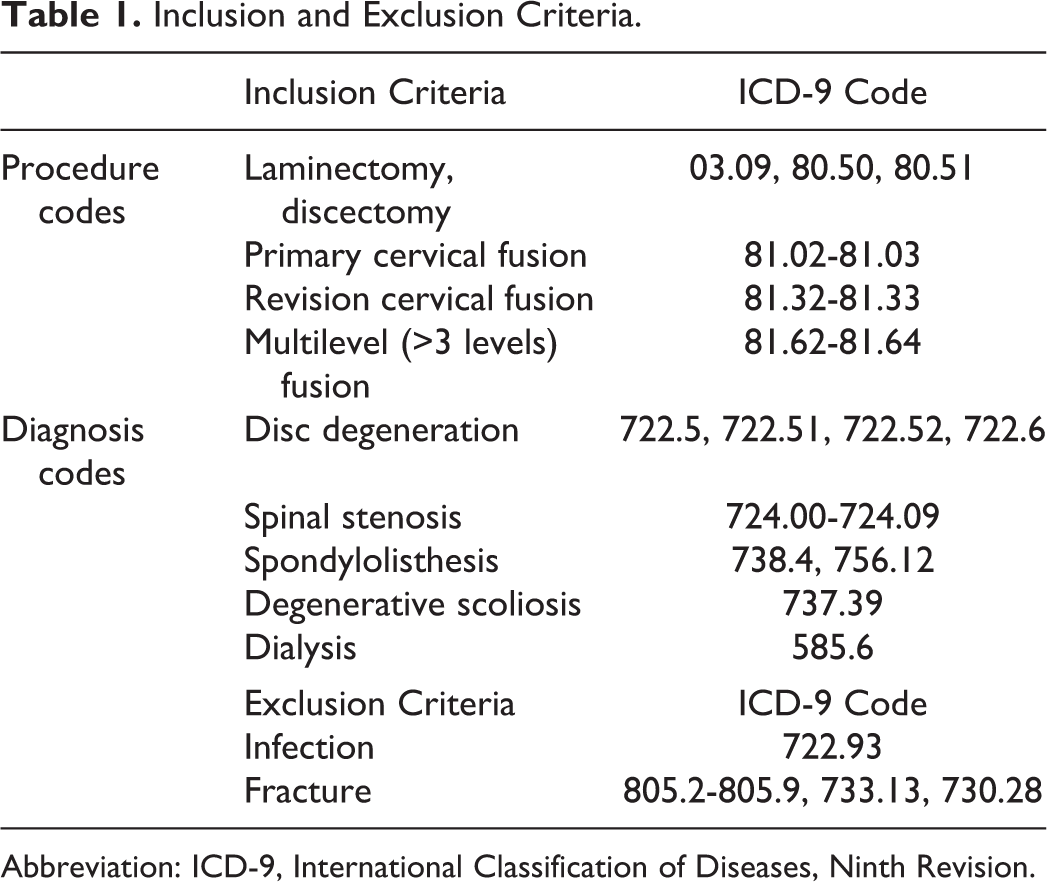
Abbreviation: ICD-9, International Classification of Diseases, Ninth Revision.
Patient Characteristics
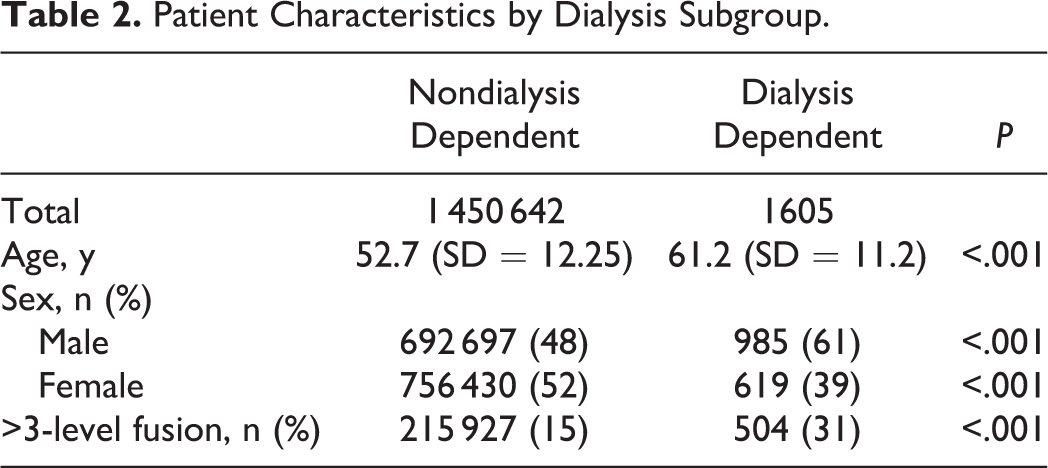
Patient characteristics were obtained from the NIS database. These included demographic information (age, sex), as well as need for multilevel fusion (>3 levels) and were included in our statistical analysis as covariates (Table 2). Preoperative comorbidities were identified utilizing ICD-9 and DRG (Diagnosis-Related Group) coding with the use of the Healthcare Cost and Utilization Project (HCUP) Comorbidity Software. 35 This software package identifies 29 patient comorbidities based off an Elixhauser Comorbidity Index. Only commonly occurring comorbidities (occurring in >1% of our sample population) were selected for use in our statistical analysis (Table 3). The Charlson Comorbidity Index was then calculated for each group to evaluate risk of perioperative complications and death from comorbid disease. 36
Patient Characteristics by Dialysis Subgroup.
Comorbidity and Postoperative Complication Codes.
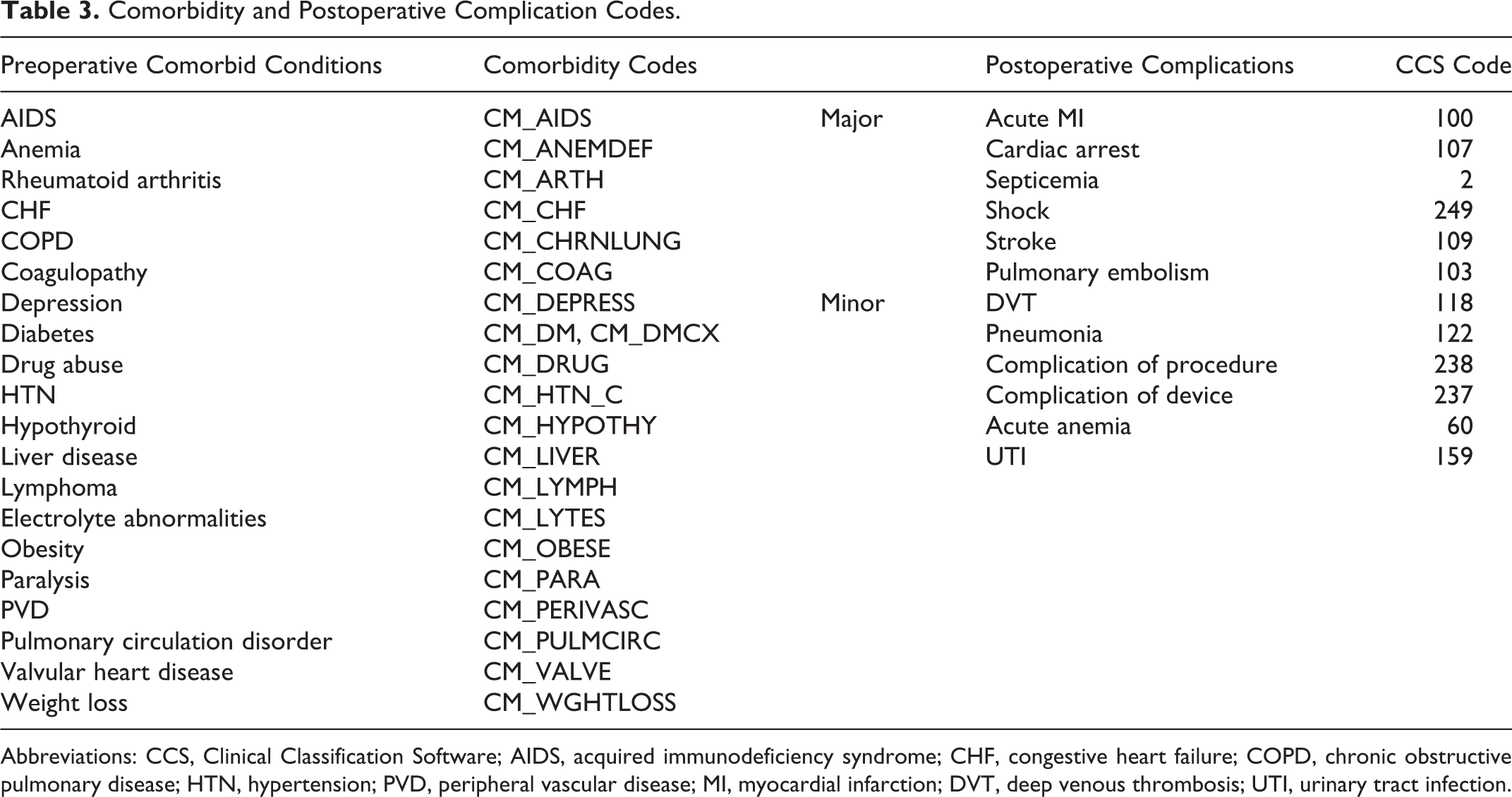
Abbreviations: CCS, Clinical Classification Software; AIDS, acquired immunodeficiency syndrome; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HTN, hypertension; PVD, peripheral vascular disease; MI, myocardial infarction; DVT, deep venous thrombosis; UTI, urinary tract infection.
Outcome Metrics
Postoperative complications were also identified using the HCUP clinical classifications software, which groups together related ICD-9 coded postoperative complications to facilitate statistical analysis 35 (Table 3). These complications were then subcategorized into major and minor categories. Major complications included acute myocardial infarction, cardiac arrest, septicemia, septic shock, stroke, and pulmonary embolism. Minor complications included deep vein thrombosis, pneumonia, complication of procedure, complication of device, postoperative anemia, and urinary tract infections. Last, inpatient mortality rate, hospital length of stay, and total hospital costs were also assessed.
Statistical Analysis
Patient characteristics and inpatient outcomes for both groups were analyzed with the use of chi-square and Student t tests. A chi-square test was used for categorical variables, and an independent Student t test was used to assess continuous variables. Multivariate logistic regression analysis was used for the analysis of associations between patient comorbidities, dialysis dependence, and consequent postoperative complications and inpatient mortality and to control for potential confounders including age, sex, race, hospital size, and hospital type. These calculated associations were reported as multivariate odds ratios with 95% confidence intervals. P < .05 was set as our measure of statistical significance.
Results
Patient Characteristics
In total, 1605 dialysis-dependent patients and 1 450 642 nondialysis-dependent patients were identified using our criteria as having undergone an elective primary or revision ACDF or posterior cervical spinal fusion for degenerative conditions between 2002 and 2012. While both patient populations had a male majority, dialysis-dependent patients were found to be older by approximately 8 years when compared with nondialysis-dependent patients (61.2, SD = 11.2 vs 52.7, SD = 12.25; P < .001). Full details are presented in Table 2.
Not surprisingly, dialysis dependence was associated with an increased Charlson Comorbidity Score (3.55, SD = 1.58 compared with 0.43, SD 0.84; P < .001). The most common preoperative comorbidities associated with dialysis dependence were: hypertension (84.7%), anemia (43.8%), electrolyte disorders (26.7%), diabetes (47.9%), congestive heart failure (18.4%), chronic pulmonary disease (16.8%), and peripheral vascular disease (11.5%). All associated diagnoses for both cohorts are presented in Table 4.
Comorbidities by Dialysis Subgroup.
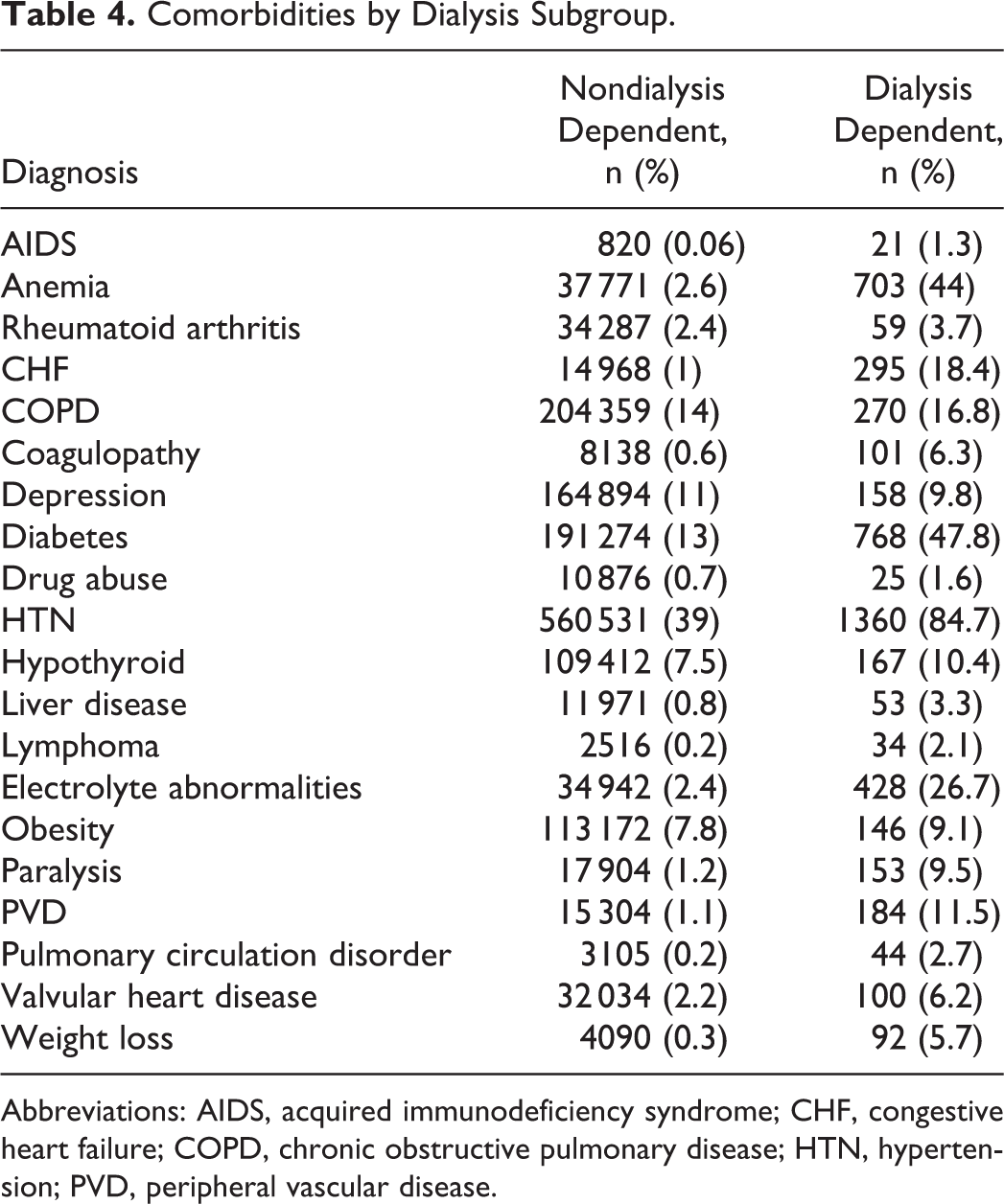
Abbreviations: AIDS, acquired immunodeficiency syndrome; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; HTN, hypertension; PVD, peripheral vascular disease.
Postoperative Complications
Dialysis dependence was associated with an approximate 28-fold increase in major postoperative complications (17.3% vs 0.6%; P < .001) when compared with nondialysis-dependent patients. The most common major complications in this cohort included: septicemia (9.4%), septic shock (4.7%), acute myocardial infarction (3.4%), and pulmonary embolism (3.1%); P < .001 (Table 5). Based on multivariate regression analysis, dialysis dependence was identified as an independent risk factor for major postoperative complications (odds ratio [OR] = 5.48; 95% CI, 4.65-6.47; P < .001). Congestive heart failure was also found to be an important independent risk factor for major postoperative complications (OR = 4.76; 95% CI, 4.42-5.116; P < .001). The results of this analysis are shown in Table 6.
Outcomes by Dialysis Subgroup.
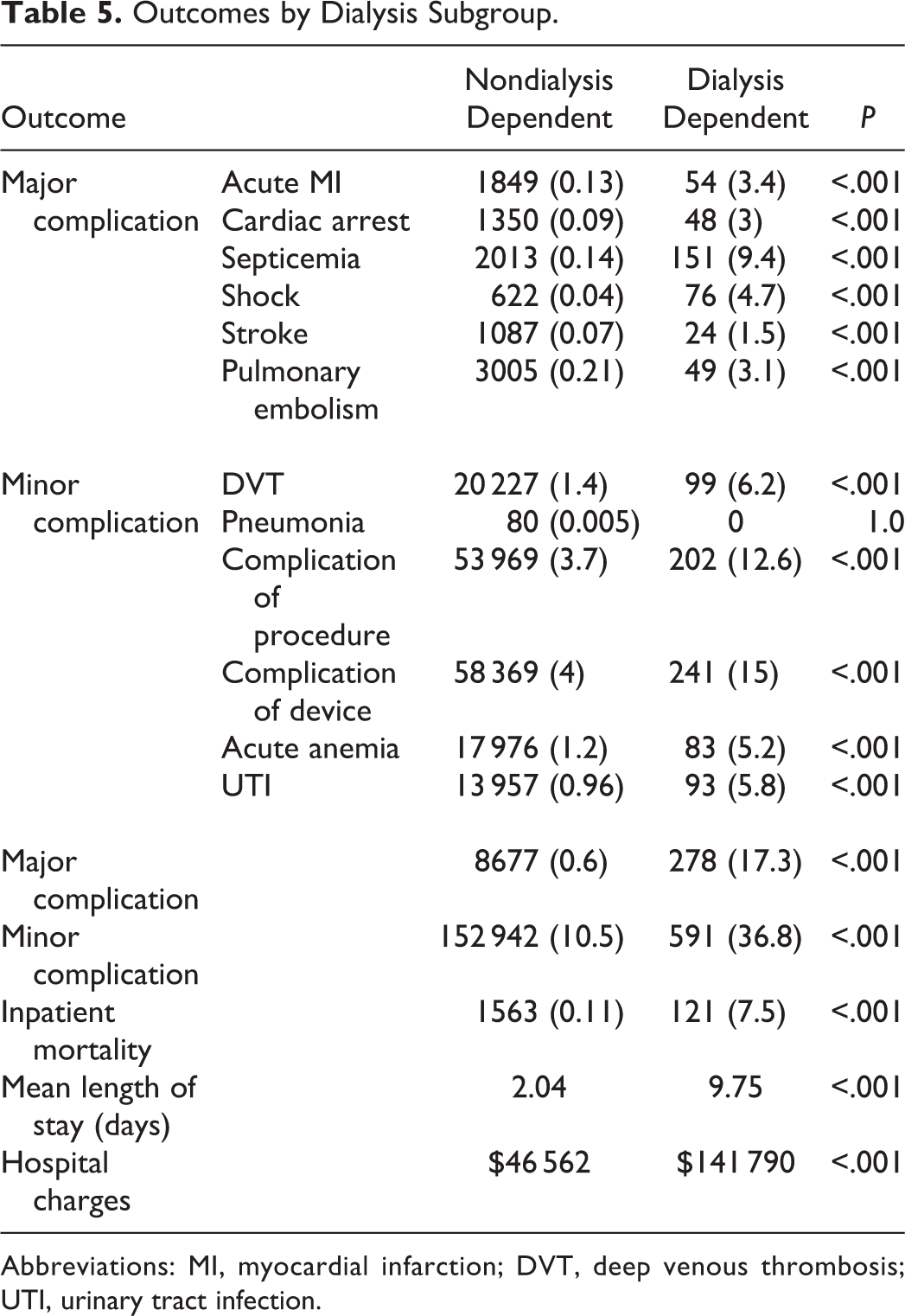
Abbreviations: MI, myocardial infarction; DVT, deep venous thrombosis; UTI, urinary tract infection.
Multivariate Analysis of Comorbidities and Outcomes.
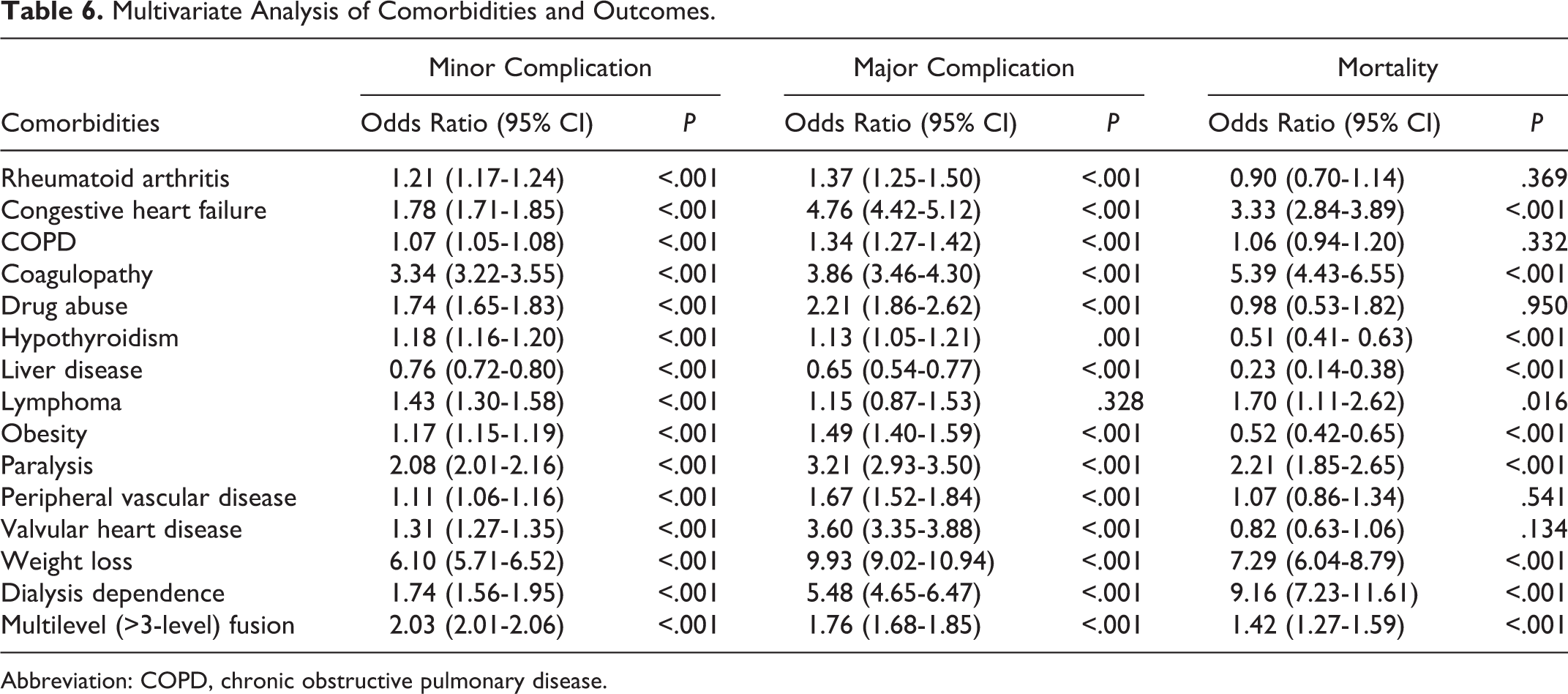
Abbreviation: COPD, chronic obstructive pulmonary disease.
Patients requiring chronic dialysis also had an increased likelihood of experiencing a minor postoperative complication (36.8% vs 10.5%; P < .001). The most common of these complications in the dialysis-dependent group included surgical device complications (15%), complications of surgical procedure (12.6%), and urinary tract infection (5.8%); P < .001.
In regard to effect of surgical procedure on outcomes, multilevel fusion of greater than 3 levels was found to be an independent risk factor for minor (OR = 2.03; 95% CI, 2.00-2.06; P < .001) and major postoperative complications (OR = 1.76; 95% CI, 1.68-1.85; P < .001), as well as mortality (OR = 1.42; 95% CI, 1.27-1.59; P < .001).
In-Hospital Mortality, Length of Stay, and Total Hospital Charges
Dialysis dependence was found not only to be associated with higher rates of inpatient mortality (7.5% vs 1.9%; P < .001), but it was identified as an independent risk factor with multivariate regression analysis for mortality as well (OR = 9.16; 95% CI, 7.23-11.6) when compared with nondialysis-dependent patients. Other important independent risk factors for mortality are shown in Table 6.
Patients receiving chronic dialysis had an increase in mean length of stay of 7.7 days, as well as significantly greater hospital costs ($141 790) when compared with patients who were not dependent on dialysis ($46 562$); P < .001.
Discussion
Within the past decade, the population of ESRD patients dependent on dialysis has grown by 24%. 37 Surgeons are therefore increasingly more likely to become involved with the surgical care of this fragile patient demographic. Elective spine surgery has repeatedly been shown to improve functional outcomes in the dialysis-dependent population. 1,19 -22,38 However, it is essential to understand the risks inherent to this delicate population and weigh them against the potential benefit to consider spine surgery as a treatment option. Though many studies have examined the risks of spine surgery of all types in dialysis-dependent patients, ours is the first large database study performed specifically examining the risks of elective cervical spine surgery in patients on chronic dialysis. Moreover, exclusion of patients with indications for surgery other than elective was unique as clinical decision making and postoperative outcomes in urgent or emergent cases often differ vastly from elective cases.
Diabetes mellitus and uncontrolled hypertension are the leading causes of ESRD in the United States, 39 and cardiac disease has been implicated in up to 50% of mortalities in this patient population. 40,41 Therefore, it is important to note that dialysis dependence is not a stand-alone diagnosis and associated multiple organ dysfunction is commonplace in this patient population. Using a large Japanese inpatient database, Chikuda et al 13 found that dialysis dependent patients had a 10-fold higher risk of death and an elevated risk of major postoperative complications after spinal surgery. Similar to the present study, De la Garza et al 28 compared patients without kidney disease, those with chronic kidney disease, and those with ESRD undergoing elective ACDF. They found that patients with chronic kidney disease did not have higher risk of postoperative mortality; however, ESRD patients had a 15 times higher risk of mortality compared to those without kidney disease. 28 In our sample population, dialysis-dependence was independently associated with a striking 28-fold increase in major postoperative complications and an almost 4-fold increase in mortality. Other smaller studies have suggested that dialysis-dependent patients undergoing 1- to 2-level posterior fusions have achieved equivalent postoperative functional outcomes to the normal population. However, larger, more complex multilevel fusions are associated with lower success and high mortality rates when compared with the same procedures in healthy patients. 22,38 Our results also showed multilevel fusion to be an independent risk factor for major and minor complications, as well as mortality in the immediate postoperative period among the dialysis-dependent population. Interestingly, the dialysis-dependent population in this study was found to be older by several years. The incidence of multilevel fusion in dialysis subgroup was double that in the nondialysis patients. Increased age and severity of disease on presentation could partially explain the need for larger operations and higher complication rates identified in this subgroup.
High complication rates among dialysis-dependent patients is becoming increasingly relevant as health care undergoes a shift from fee-for-service models to value-based reimbursement. In a similar large database study, Ottesen et al 42 found that the odds of readmission among dialysis-dependent patients within 30 days of elective spine surgery was almost 4 times greater than nondialysis patients. Furthermore, studies have shown that dialysis-dependent patients are more likely to undergo revision surgery and are subsequently more likely to suffer further complications or death. 24,25,42 In the present study, dialysis dependence was associated with lengthier hospital stays and, therefore, a significant increase in total hospital charges after elective cervical spine surgery. These medically challenging patients are among the most complex to undergo elective procedures. This highlights the necessity for careful surgical planning to accurately quantify risks and assess the cost-benefit ratio before performing elective cervical spine surgery on this vulnerable population. Overall, the ultimate goals of elective spine surgery are to improve functional capacity and relieve pain. 43 Additionally, as health care reimbursement trends change, and the metrics of cost-benefit analysis continue to progress, longer-term follow-up studies would be needed to clarify the precise cost-benefit of elective spine surgery in such a high-risk population.
The primary limitation to our study is that the data available in the NIS is limited to the duration of a single hospitalization and as such may underestimate the incidences of adverse events. 42 Additionally, long-term radiographic data and patient-reported outcomes that are crucial to the evaluation of successful cervical spine surgeries could not be assessed. The interpretation of results in NIS also requires the use of ICD-9 coding, which has been shown in some studies to have poor sensitivity and specificity 44,45 and additionally does not allow for assessment of intraoperative factors (blood loss, surgical time) or accurate evaluation of preoperative factors such as laboratory values. Finally, differing surgical procedures may be chosen for higher risk patients based on comorbidities and risk compared to relatively healthy patients; therefore, a confounder toward surgical decision making may exist with this study. These limitations, however, are accepted in exchange for the large sample size available in the NIS database, making it possible to examine outcomes in the relatively rare occurrence of elective surgery in dialysis-dependent patients.
In conclusion, dialysis dependence is associated with drastically increased perioperative complication rates and risk of mortality, as well as longer, more expensive hospital stays in dialysis-dependent patients undergoing elective cervical spine surgery. Thus, a thorough knowledge of risks inherent to this delicate population is essential to both surgeon and patient when considering elective cervical spine surgery as a treatment option.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.