
Abstract
Study Design
Systematic Review and Meta-Analysis.
Objectives
To compare complication incidence in patients with or without the use of recombinant human Bone Morphogenic Protein-2 (BMP2) undergoing anterior cervical discectomy and fusion (ACDF) for degenerative conditions.
Methods
A systematic search of eight online databases was conducted using PRISMA guidelines. Inclusion criteria included English language studies with a minimum of 10 adult patients undergoing instrumented ACDF surgery for a degenerative spinal condition in which BMP2 was used in all patients or one of the treatment arms. Studies with patients undergoing circumferential fusions, with non-degenerative indications, or which did not report post-operative complication data were excluded. Patients with and without BMP2 were compared in terms of the incidence of dysphagia/dysphonia, anterior soft tissue complications (hematoma, seroma, infection, dysphagia/dysphonia), nonunion, medical complications, and new neurologic deficits.
Results
Of 1832 preliminary search results, 27 manuscripts were included. Meta-analysis revealed the relative risk of dysphagia or dysphonia (RR = 1.39, CI 95% 1.18 – 1.64, P = <.001), anterior soft tissue complications (RR = 1.43, CI 95% 1.25-1.64, P = <.001), and medical complications (RR = 1.32, CI 95% 1.06-1.66, P = .013) were statistically significant in the BMP2 group while the relative risk of non-union (RR = .5, CI 95% .23 - 1.13, P = .09) trended lower in the BMP2 group. Neurological deficit (RR = 1.06, CI 95% .82-1.37, P = .66), and additional medical complications (RR = 1.53, CI 95% .98-2.38, P = .06) were not found to be statistically different between the groups.
Conclusions
This meta-analysis identified a high rate of arthrodesis when BMP2 was used in ACDF, but confirmed increased rates of dysphagia and anterior soft tissue complications. Surgeons may consider reserving BMP2 implementation for cases with a high risk of non-union, and should be aware of the risk of airway compromise.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) is amongst the most commonly performed surgical interventions in spine surgery with generally reported excellent outcomes. 1 In one and two level procedures, high fusion rates have been reported with a variety of graft materials.2,3 However, concerns over nonunion persist in certain patient populations, such as those with nicotine use, diabetes, osteoporosis or vitamin D deficiency, immunosuppressive conditions, and particularly in those undergoing fusions of three or more levels where nonunion rates approach 40% in some series.4–9
Some authors have investigated recombinant human bone morphogenic protein-2 (BMP2) as a strategy to combat nonunion, particularly in these higher risk patient groups. Initially approved by the Food and Drug Administration (FDA) for use in anterior lumbar interbody fusions in 2002, 10 off-label use of BMP in other spinal indications increased substantially in the subsequent decade. 11 Initial reports in the anterior cervical spine were favorable, with low rates of nonunion. 12 However, in 2006, Smucker et al reported a significantly increased incidence of anterior swelling and dysphagia with use of BMP2. 13 Additional complication concerns, such as increased incidence of seroma and post-operative radiculitis, were also reported. 10 In response to this, as well as other reports,12,14 in 2008 the FDA issued a warning recommending against BMP2 use in anterior cervical applications. 9
Nonetheless, in spite of this warning, BMP2 continues to be used off label in the anterior cervical spine using strategies such as dose containment, 15 select delivery routes, 15 and immediate post-operative tapered steroid use,16,17 which are reported to successfully reduce morbidity risk. However, the overall morbidity profile of BMP2 use in anterior cervical surgery remains unclear. The purpose of this study was to compare complication incidence in patients with or without the use of recombinant human Bone Morphogenic Protein-2 (BMP2) undergoing anterior cervical discectomy and fusion (ACDF) for degenerative conditions.
Methods
Search Strategy
The search strategy used a combination of natural language searching and controlled vocabulary reflecting the concepts of ACDF and BMP. The search was executed across eight databases: Medline via PubMed and Ovid, Embase via Ovid, SPORTDiscus via EBSCO, Web of Science Core Collection, Cochrane Library via Wiley, Scopus, ClinicalTrials.gov, and Global Index Medicus. The search was most recently conducted on August 14, 2020.
Selection Criteria
The eligibility of the 887 articles identified in the systematic search was assessed by 3 independent reviewers using the inclusion and exclusion criteria described in the following paragraphs. Initially, the titles and abstracts were screened to determine eligibility. If eligibility could not be determined discrepancies were then resolved by the third independent reviewer. We included studies that directly compared rates of post-surgical complications and fusion status in patients undergoing treatment for degenerative spinal conditions with instrumented ACDF between C2-7 who were administered BMP2 pre-surgery vs those that did not, studies that were published in English, and full-text articles published in a peer-reviewed journal. Exclusion criteria included nonhuman studies, studies that focused on procedures other than ACDF, studies that focused on non-degenerative pathologies, studies that did not report post-operative complication data, studies that did not use BMP2 to address non-unions and evidence level 2-5 studies. After this process, 47 articles were then selected for full text review. After full text review, an additional 20 articles were excluded, leaving 27 articles for inclusion and data abstraction (Figure 1). PRISMA 2020 methodology flow diagram.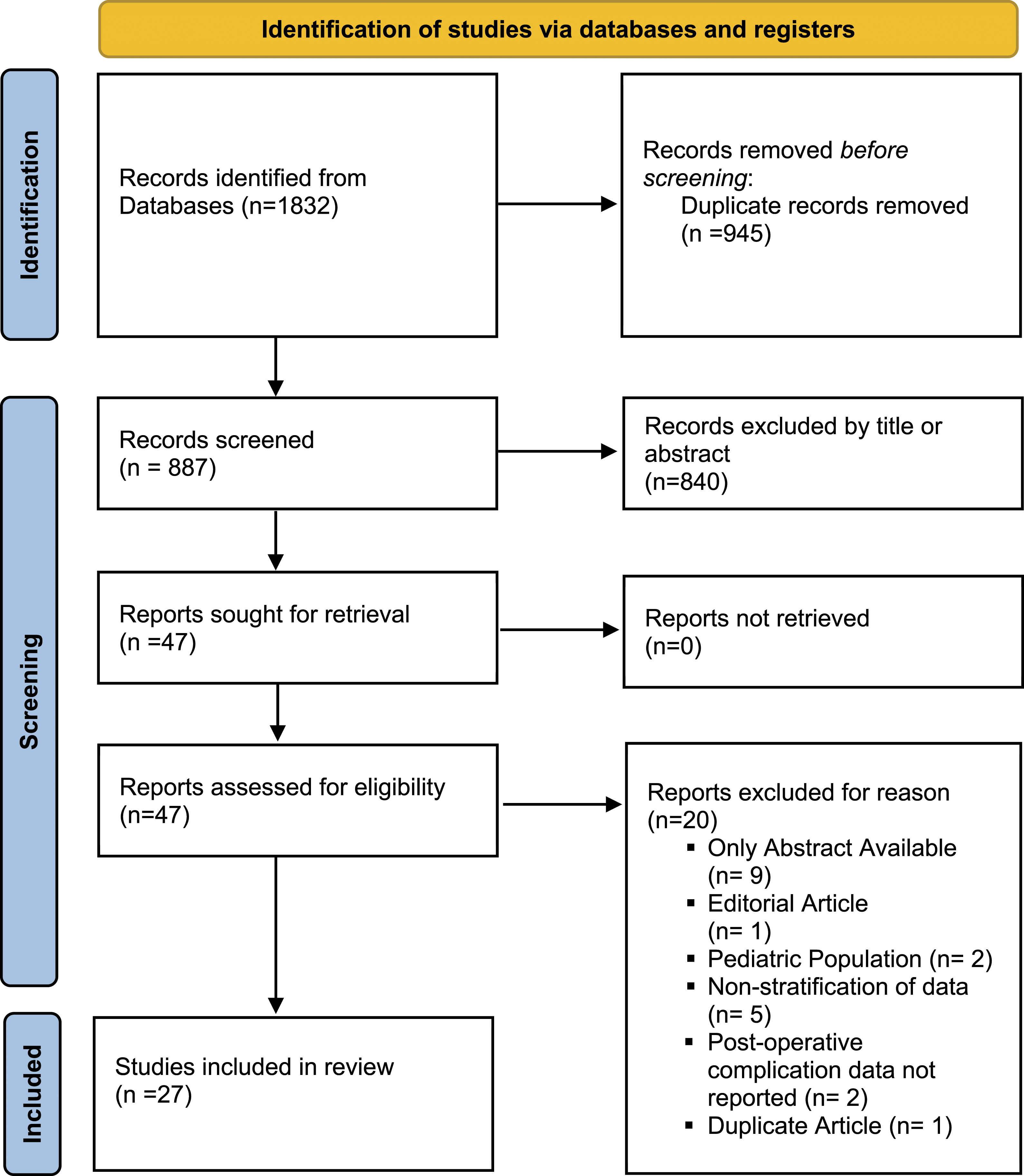
Data Collection
From each study, we collected general demographic information (age, gender, body mass index, smoking status), information on graft choice (BMP2 including dosing, allograft, autograft, or other), and recorded the incidence of complications in each treatment cohort. For the assessment of fusion status we required a minimum of 6 months follow-up and a report based on either computed tomography (CT) or flexion-extension radiographs. For the other complications a minimum of 3 months follow-up was required.
Assessment of Bias
Individual studies were assessed for risk of bias using validated tools including Cochrane Risk of Bias (RoB) 18 for randomized studies and the MINORS score for non-randomized studies. The MINORS criteria has a 24 point scoring system, with the risk of bias considered moderate for scores 17-24, serious for scores 9-16, and critical for scores 8 or less. Risk of bias was completed by two independent reviewers for each study and discrepancies were resolved by a third reviewer. The overall quality of evidence was then assessed according to the GRADE guidelines. 19
Statistical Analysis
Patients were stratified into cohorts of those who received BMP2 at the time of surgery, and those who did not. We compared the incidence of complications between the two cohorts, deriving DerSimonian-Laird 20 weighted means of the incidences. 21 The reporting of complication categories varied across the manuscripts. Thus, we chose to combine certain types of complications into larger groups for analysis. These included a grouped analysis of the incidence of either dysphagia or dysphonia, the incidence of any anterior soft tissue complications (which included any incidence of seroma, hematoma, dysphagia, or dysphonia), the incidence of any medically related complication (such as cardiac, pulmonary, gastrointestinal, or renal), the incidence of any new neurologic deficit of any kind, and the incidence of other complications not captured in the categories above. As a secondary analysis we then attempted to analyze complication incidence in sub-categories based on the dosage of BMP received. The meta-analysis was completed using a random effects (due to anticipated heterogeneity) model from the included studies using the bias-corrected DerSimonian-Laird method to calculate relative risk (RR) with 95% CI, and these data were presented in forest plots. Additionally, the I2 statistic was calculated to quantify the degree of heterogeneity and was presented in corresponding forest plots. Meta-analysis and generation of forest plots were performed using Stata 17 (StataCorp LLC, College Station TX).
Results
Methodological Quality Assessment
MINORS Score by Article for Non-Randomized Studies.
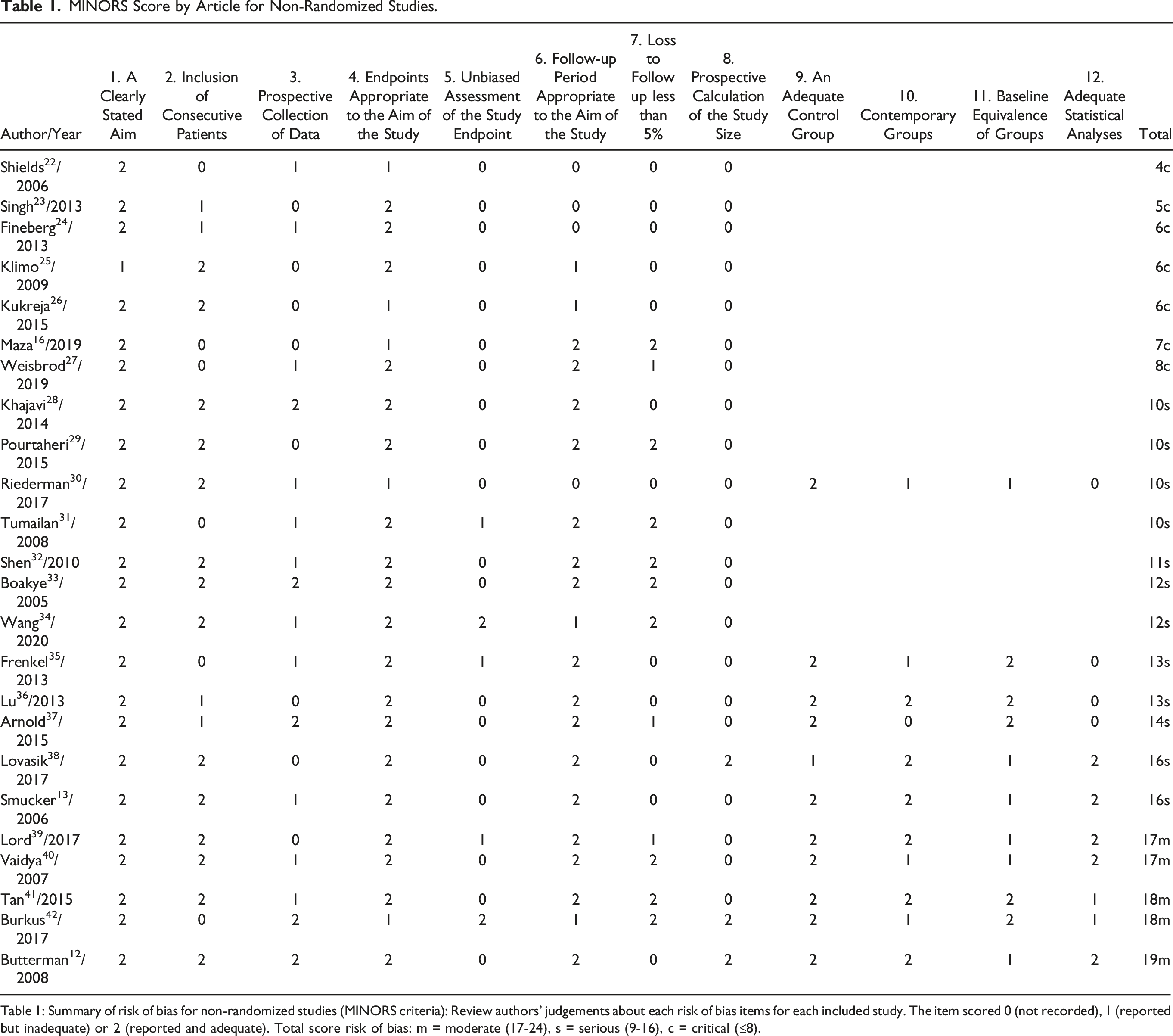
Table 1: Summary of risk of bias for non-randomized studies (MINORS criteria): Review authors' judgements about each risk of bias items for each included study. The item scored 0 (not recorded), 1 (reported but inadequate) or 2 (reported and adequate). Total score risk of bias: m = moderate (17-24), s = serious (9-16), c = critical (≤8).
Risk of Bias (RoB) Scores for Randomized Studies.
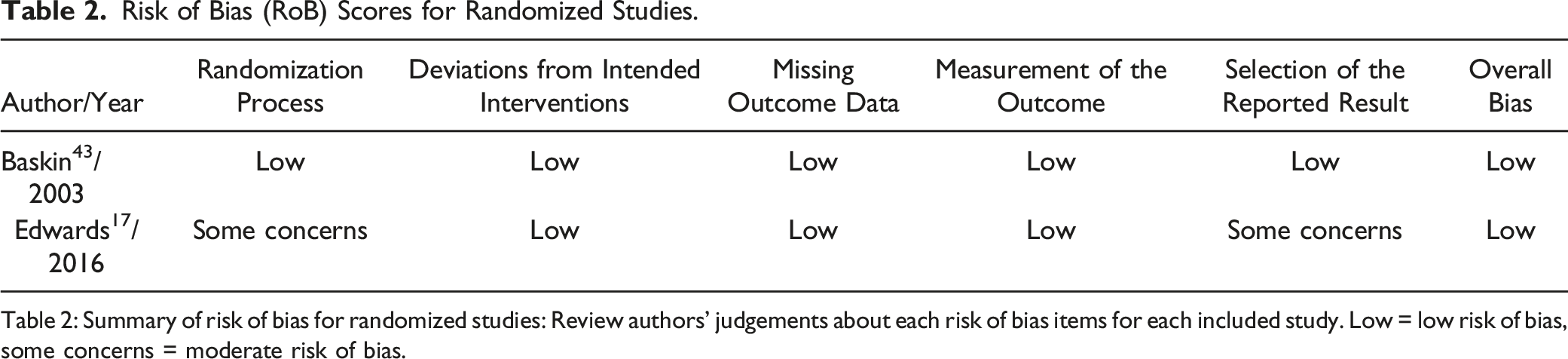
Table 2: Summary of risk of bias for randomized studies: Review authors' judgements about each risk of bias items for each included study. Low = low risk of bias, some concerns = moderate risk of bias.
Characteristics of Included Studies
Characteristics of Included Studies.
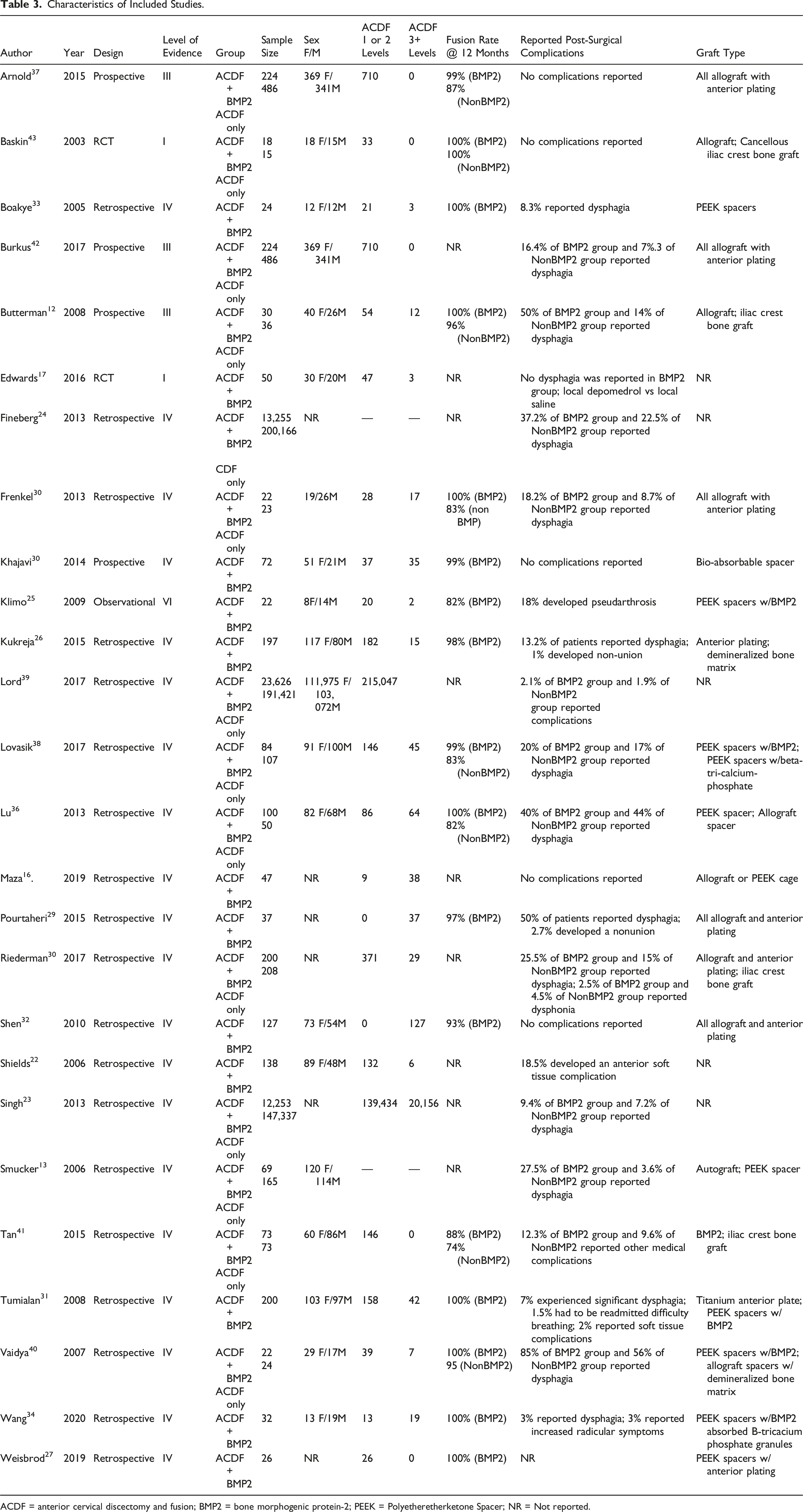
ACDF = anterior cervical discectomy and fusion; BMP2 = bone morphogenic protein-2; PEEK = Polyetheretherketone Spacer; NR = Not reported.
Dysphagia/Dysphonia
Eighteen studies12,22–24,26,28–31,33,36,38–40,42,43 reported on the incidence of dysphagia or dysphonia. For the purposes of this review we defined dysphagia as inadequate neural control or the impairment of soft tissue or bony structures involved in any part of the swallowing process, or patient-reported swallowing difficulties; and defined dysphonia as the impairment of voice production or altered voice quality due to structural and/or functional causes, or patient-reported hoarseness. Ten studies12,23,24,30,35,36,38–40,42 were included in the meta-analysis of dysphagia or dysphonia rate, representing a total of 589,673 patients (BMP2, n = 49,815; nonBMP2, n = 539,858). Meta-analysis showed that the BMP2 group (RR = 1.39, CI 95% 1.18 - 1.64, p = <.001) is at a 40% increased risk to develop dysphagia or dysphonia than the nonBMP2 group Incidence of dysphagia/dysphonia.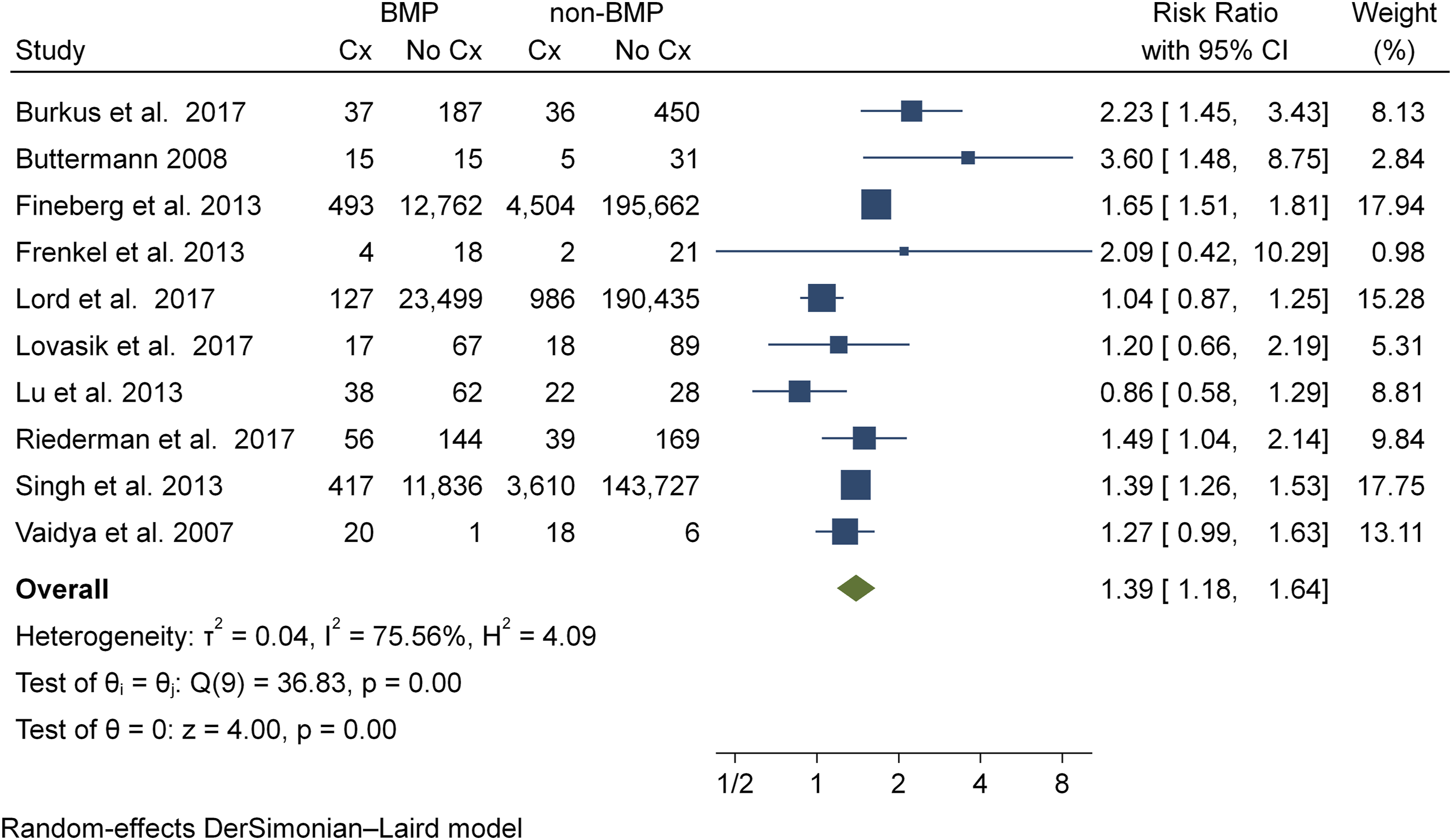
Anterior Soft Tissue Complication
Twenty-five studies12,16,22–26,28–43 reported on complications within our grouped category of anterior soft tissue complications, which included any occurrence of dysphagia, dysphonia, hematoma, seroma, or wound complication. Thirteen studies12,23,24,30,35–43 were included in the meta-analysis of anterior soft tissue complication rates, representing a total of 590,562 patients (BMP2, n = 50,130; nonBMP2, n = 540,432). Meta-analysis showed that the BMP2 group (RR = 1.43, CI 95% 1.25 - 1.64, P = <.001) is at a 40% increased risk to develop an anterior soft tissue complication than the nonBMP2 group. Statistical assessment for heterogeneity was found to be high (I2 = 70.4%) (Figure 3). Incidence of anterior soft tissue complications.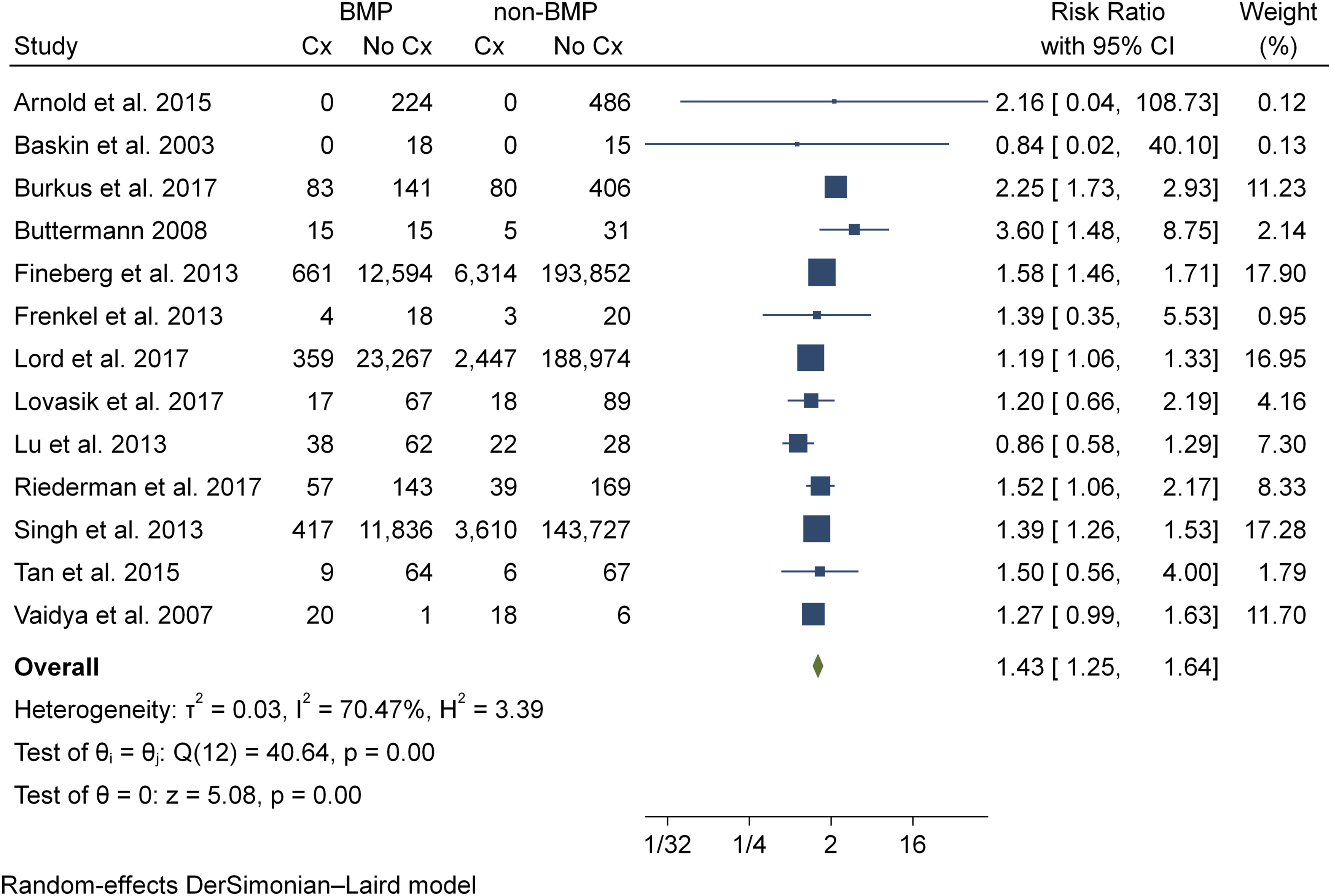
Nonunion
Six studies22,26,28,35,42,43 reported on the incidence of non-union. Three studies35,42,43 were included in the two-armed meta-analysis of non-union rate, representing a total of 788 patients (BMP2, n = 264; nonBMP2, n = 524). Meta-analysis showed that the BMP2 group (RR .5, CI 95% .23 - 1.13, P = .09), showed a 50% reduction in risk to develop a nonunion and demonstrated a trend towards statistical significance (Figure 4). Statistical assessment for heterogeneity was found to be negligible for all meta-analyses (I2 = .00%). Incidence of non-union.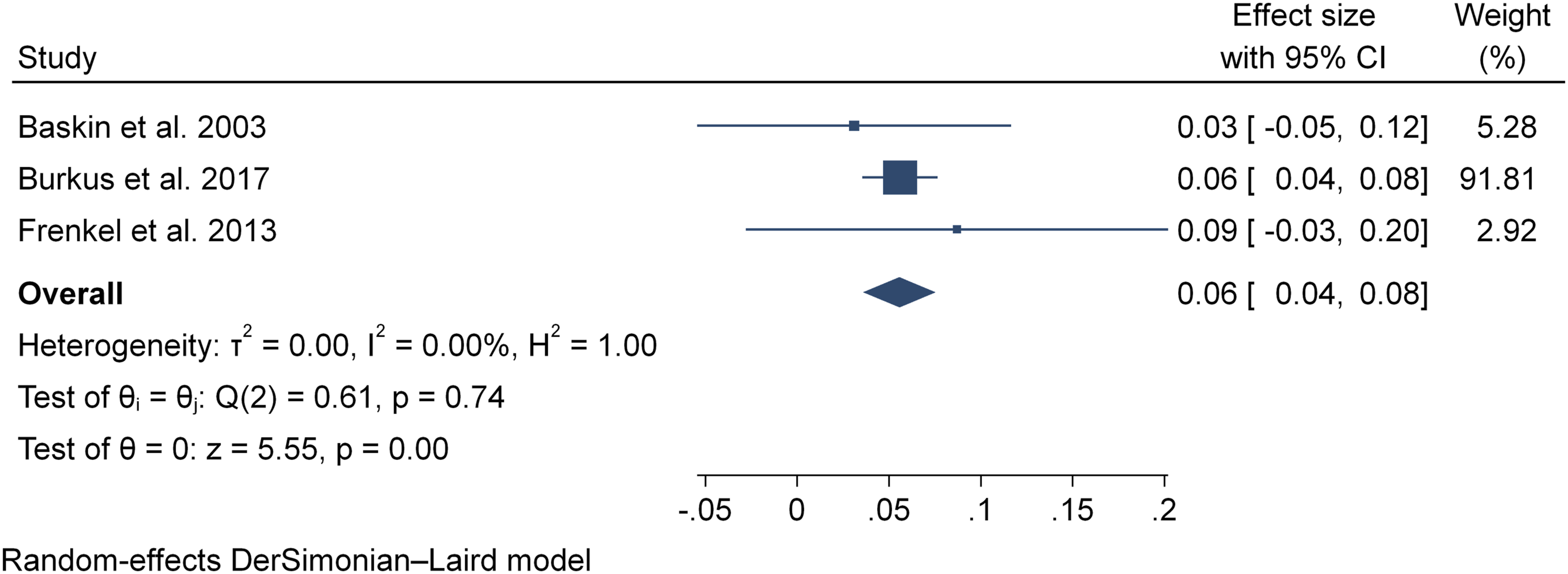
New Neurologic Deficit
Eleven studies24–26,28,30,33,35,39,42,43 reported on the incidence of neurological deficit. Six studies24,30,35,39,42,43 were included in the meta-analysis of neurological deficit rate, representing a total of 429,664 patients (BMP2, n = 37,345; nonBMP2, n = 392,319). Meta-analysis showed that the BMP2 group (RR = 1.06, CI 95% .82 - 1.37, P = .66) was no more at risk to develop neurological deficit than the nonBMP2 group. Statistical assessment for heterogeneity was found to be low (I2 = 29.5%) (Figure 5). Incidence of new neurologic deficit.
Medically Related Complications
Seven studies16,24,28,30,33,41,42 reported on the incidence of neurological deficit. Four studies24,30,41,42 were included in the meta-analysis of medically related complications, representing a total of 214,682 patients (BMP2, n = 13,752; nonBMP2, n = 200,930). Meta-analysis showed that the BMP2 group (RR = 1.32, CI 95% 1.06 – 1.66, P = .013) is at a 30% risk increase for development of a neurological deficit vs the nonBMP2 group. Statistical assessment for heterogeneity was not found to be low (I2 = 23.8%) (Figure 6). Incidence of medically related complications.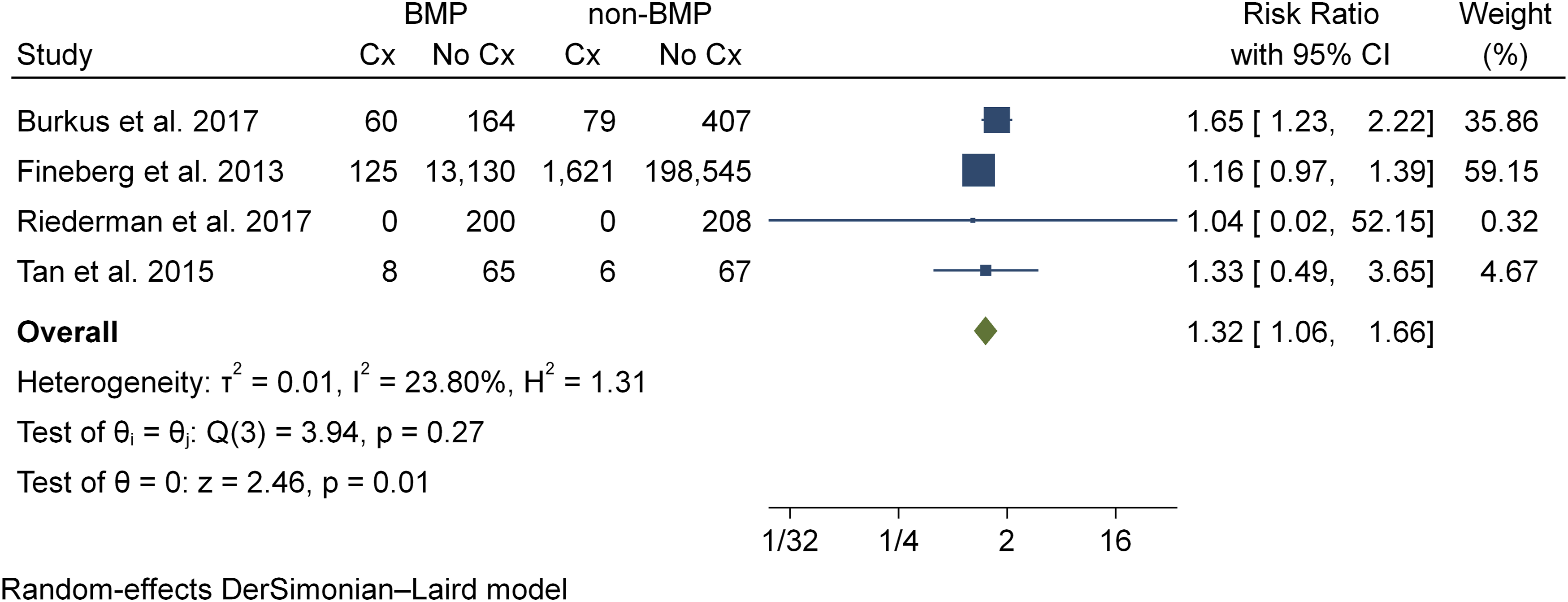
Additional Medical Complications
Eleven studies24,25,29–33,35,37,42,43 reported complications that did not fall into the categories noted above. Five studies24,30,37,42,43 were included in the meta-analysis of other complications, representing a total of 215,282 patients (BMP2, n = 13,921; nonBMP2, n = 201,361). Meta-analysis showed that the BMP2 group is at a 50% risk increase for development of additional medical complications vs the non BMP2 group (RR1.53, CI 95% .98 - 2.38, P = .06) and trended towards statistical significance. Statistical assessment for heterogeneity was found to be moderate (I2 = 58.9%) (Figure 7). Incidence of additional medical complications.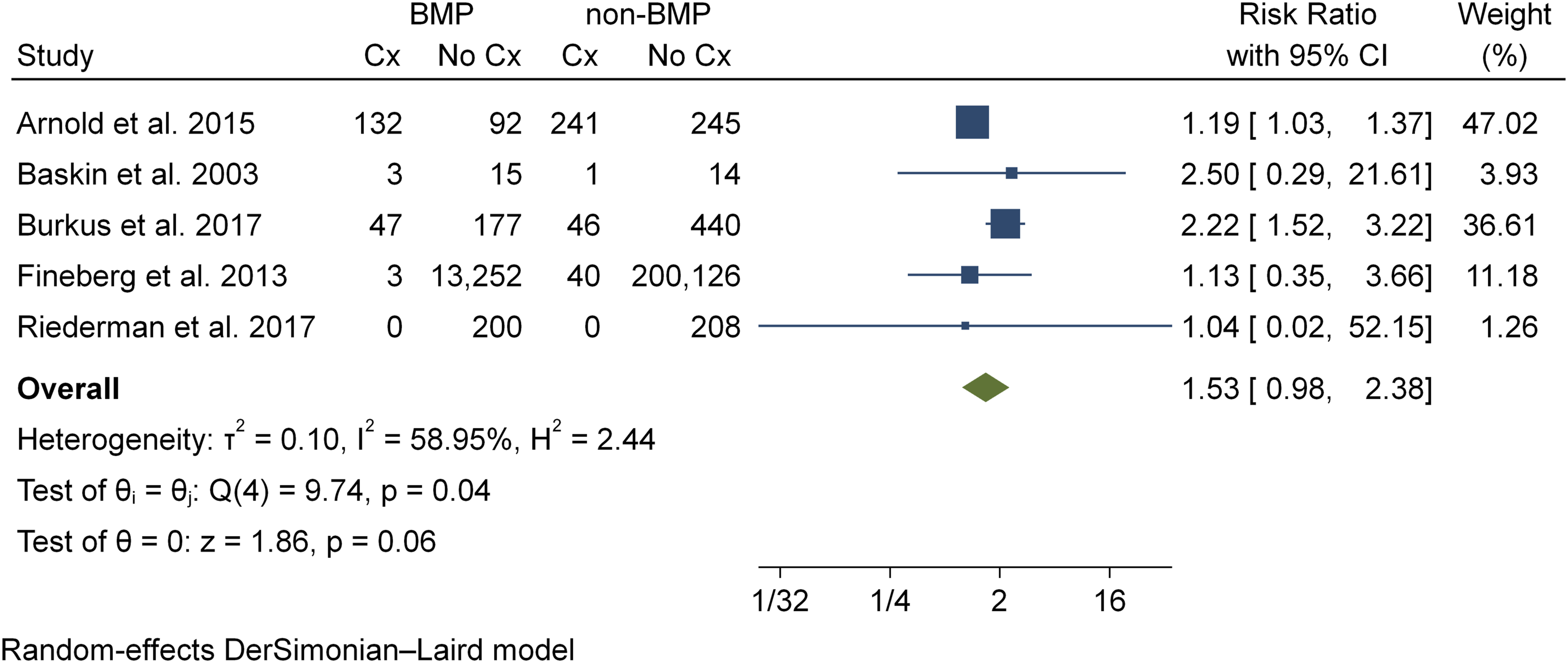
Impact of Dosage on Fusion Rates
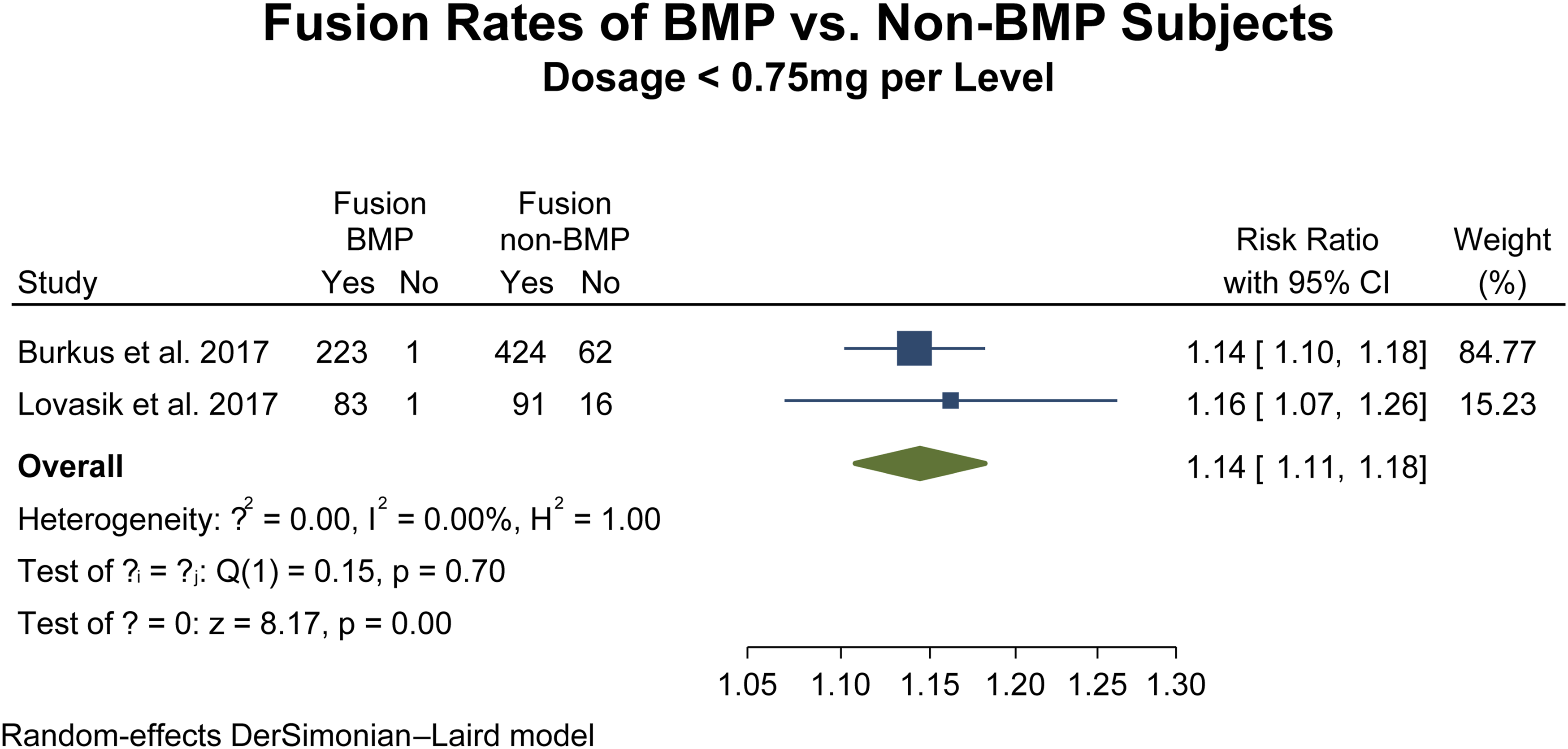
Seven studies12,35–37,40,41,43 were included in the two-armed meta-analysis of fusion rates with BMP dosages greater than 75 mg, representing a total of 1196 patients (BMP2, n = 489; nonBMP2, n = 707). Meta-analysis showed that the BMP2 group (RR 1.10, CI 95% 1.04 – 1.16, p = <.001), showed a 10% increase in union rates (Figure 8) while two studies38,42 were included in the two-armed meta-analysis of fusion rates with BMP dosages less than 75 mg, representing a total of 901 patients (BMP2, n = 308; nonBMP2, n = 593). Meta-analysis also showed that the BMP2 group (RR 1.14, CI 95% 1.10 – 1.18, p = <.001), showed a 10% increase in union rates (Figure 9). Statistical assessment for heterogeneity for both analyses were found to be negligible (I2 = .00%). Fusion rates with >75 mg BMP dosage. Fusion rates with <75 mg BMP dosage.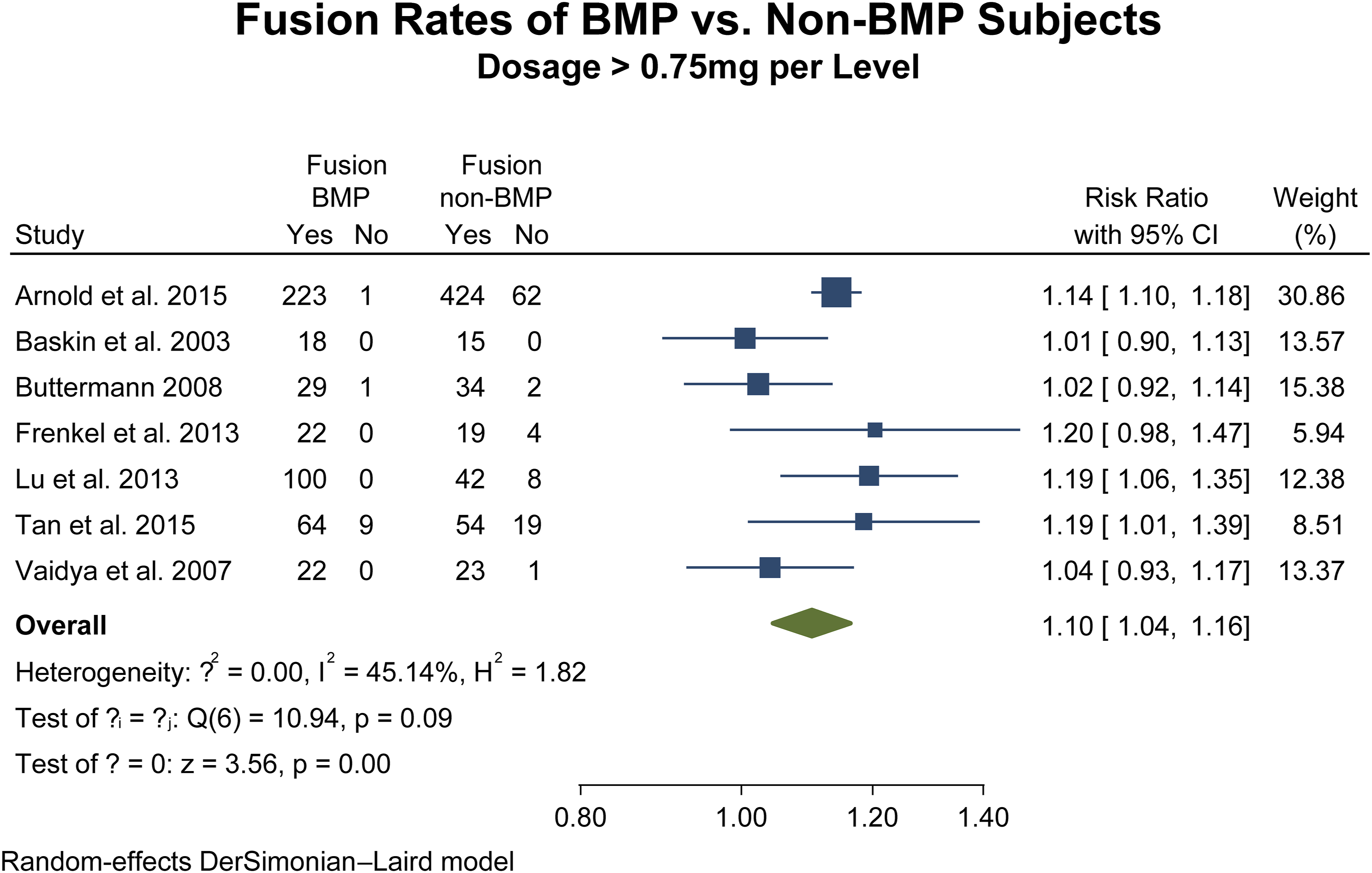
Impact of Dosage on Complication Risk
Substantially fewer studies reported on complications related to dosing. With the available patient numbers, there was no significant difference in the incidence of dysphagia/dysphonia, anterior soft tissue complications, new neurologic deficits, medically related complications, or other complications between those with or without BMP2, either for doses above or below .75 mg/level (P = >.05 for each comparison).
Discussion
The purpose of this review and meta-analysis was to determine the comparative complication rates amongst patients with and without BMP2 use in anterior cervical fusions. Overall, bony union rates were reportedly high, but many studies reported an increased risk of dysphagia/dysphonia or anterior soft tissue complications. There were no significant differences in the incidence of new neurologic deficits or medical complications. Several of these findings merit further discussion.
For surgeons interested in using BMP2 in anterior cervical applications, the most concerning adverse event has been severe swelling which can result in dysphagia or airway compromise. 13 Due to concern over this specific complication, the FDA issued a warning recommending against the use of BMP2 in anterior cervical surgery. 9 The results of the current study indicate that dysphagia and dysphonia were much more common in patients who received BMP2 (RR = 1.39). It is worth noting that dysphagia and dysphonia are different disease processes, but given the reported variability in definition across the available clinical studies, 44 we chose to combine them for this analysis. Similarly, in our combined analysis of all anterior soft tissue complications, the BMP2 cohort was also at significantly higher risk (RR = 1.43). Some studies reported similar overall rates of dysphagia, but even so the severity of dysphagia was typically worse in the BMP2 group with more readmissions and higher validated outcome scores.36,38 This result fits with multiple reports which appeared in the mid 2000’s expressing similar concerns. 13 Some authors have investigated steroids as a method to reduce severe dysphagia,16,29 whereas others have advocated for using very low dose BMP2, 29 each with reportedly favorable results. We did attempt a secondary analysis on the dosage of BMP2 used, and no difference in dysphagia incidence was noted with dose changes. However, this secondary analysis was limited by lower patient numbers. Thus, our study design does not allow us to definitively assess the efficacy of dosage or other interventions to mitigate the risk of anterior swelling complications, but it seems reasonable for surgeons to take additional precautions in anterior cervical cases where BMP2 is used.
Fusion rates after 1 and 2 level ACDF are generally high, with nonunion typically occurring in less than 5% of cases regardless of the graft material. 3 In contrast, the nonunion rate for multi-level ACDF is typically much higher, with rates as high as 38% in some series. 7 Thus, some authors have advocated for using BMP2 in patients who are at high risk for non-union, particularly multi-level cases.9,36 In this study, the two-armed statistical analysis found that the use of BMP was associated with a 50% reduction in nonunion risk (RR = .5, P = .09). However, there were only three published studies with two treatment arms, which limits the statistical power of the two-armed analysis, and this result did not reach statistical significance. These results largely confirm prior studies which have shown very high rates of fusion with BMP2 in multiple spinal applications.9,45 These results were maintained in the sub-analysis of patients who received at least .75 mg/level of BMP2 (RR = 1.10), and also of those who received less than .75 mg/level (RR = 1.14), both of which had higher fusion rates than patients without BMP2, and in the sub-analysis the result did reach statistical significance. It would seem reasonable that if BMP2 is to be used in an anterior cervical application, that it be reserved for patients who are at particular risk of nonunion. We did attempt a secondary analysis on the number of fusion levels (2+ and 3+ levels) associated with non-unions, however this was not feasible as insufficient patient numbers (statistical power) and limited published studies precluded any meaningful analysis.
In this study, there was no difference in the incidence of general medical complications or in the incidence of new neurologic deficits between the BMP2 and non-BMP2 cohorts. The molecular mechanism of BMP2 is such that it induces multiple pro-inflammatory pathways that act locally at the site of application. 46 Thus, the relative absence of increased medical or systemic complications is consistent with the known activities of the protein. However, numerous animal studies have indicated that BMP2 can induce significant inflammatory and morphologic changes in neural tissue. 47 Thus, some authors have expressed concern that BMP2 could increase the risk of radiculitis or neural injury, particularly in lumbar applications.47,48 Our study design did not have the ability to specifically identify radiculitis as a complication, but incidence of new neurologic deficit does not appear to increase when BMP2 is used.
This analysis does carry some weaknesses. Specifically, while the increased incidence of anterior seroma/hematoma and dysphagia/dysphonia has been widely reported with BMP2, some authors have argued that mitigating strategies such as decreasing the dosage or using topical steroids might reduce these risks. Our analysis does not allow us to comment on whether or not these mitigating strategies would be successful. In addition, the dosage of BMP2 has been reportedly linked to complication incidence. However, dosages used across these studies were quite varied, and our analysis cannot definitely evaluate the impact of dosing on BMP2 related complications. We did attempt a sub-analysis of complications divided according to dose of BMP2 used, but no significant differences are identified and this sub-analysis was limited by small patient numbers. Although ectopic bone formation has been reported as a complication in lumbar surgeries using BMP2, it was not widely reported in the studies examined here and we cannot report on its incidence in cervical cases. Lastly, while it is clear that 1 and 2 level ACDF has a lower complication rate than multi-level procedures, the heterogeneity of the included studies meant that it was not possible to do a meta-analysis of these sub-categories.
Conclusion
In summary, this meta-analysis identified a high rate of union when BMP2 was used in anterior cervical fusions, but confirmed the previously widely reported concerns regarding increased rates of dysphagia and anterior soft tissue complications. Surgeons who choose to use BMP2 may wish to reserve implementation for cases with a high risk of non-union, and should be aware of the risk of catastrophic airway compromise.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This supplement was organized and financially supported by AO Spine through the AO Spine Knowledge Forum Degenerative, a focused group of international spine experts.
Ethical Approval
This paper is exempt from IRB review as it is not human subjects research.