
Abstract
Study Design
Biomechanical cadaveric study.
Objectives
Multi-rod constructs maximize posterior fixation, but most use a single pedicle screw (PS) anchor point to support multiple rods. Robotic navigation allows for insertion of PS and cortical screw (CS) within the same pedicle, providing 4 points of bony fixation per vertebra. Recent studies demonstrated radiographic feasibility for dual-screw constructs for posterior lumbar spinal fixation; however, biomechanical characterization of this technique is lacking.
Methods
Fourteen cadaveric lumbar specimens (L1–L5) were divided into 2 groups (n = 7): PS, and PS + CS. VCF was simulated at L3. Bilateral posterior screws were placed from L2–L4. Load control (±7.5Nm) testing performed in flexion-extension (FE), lateral bending (LB), axial rotation (AR) to measure ROM of: (1) intact; (2) 2-rod construct; (3) 4-rod construct. Static compression testing of 4-rod construct performed at 5 mm/min to measure failure load, axial stiffness.
Results
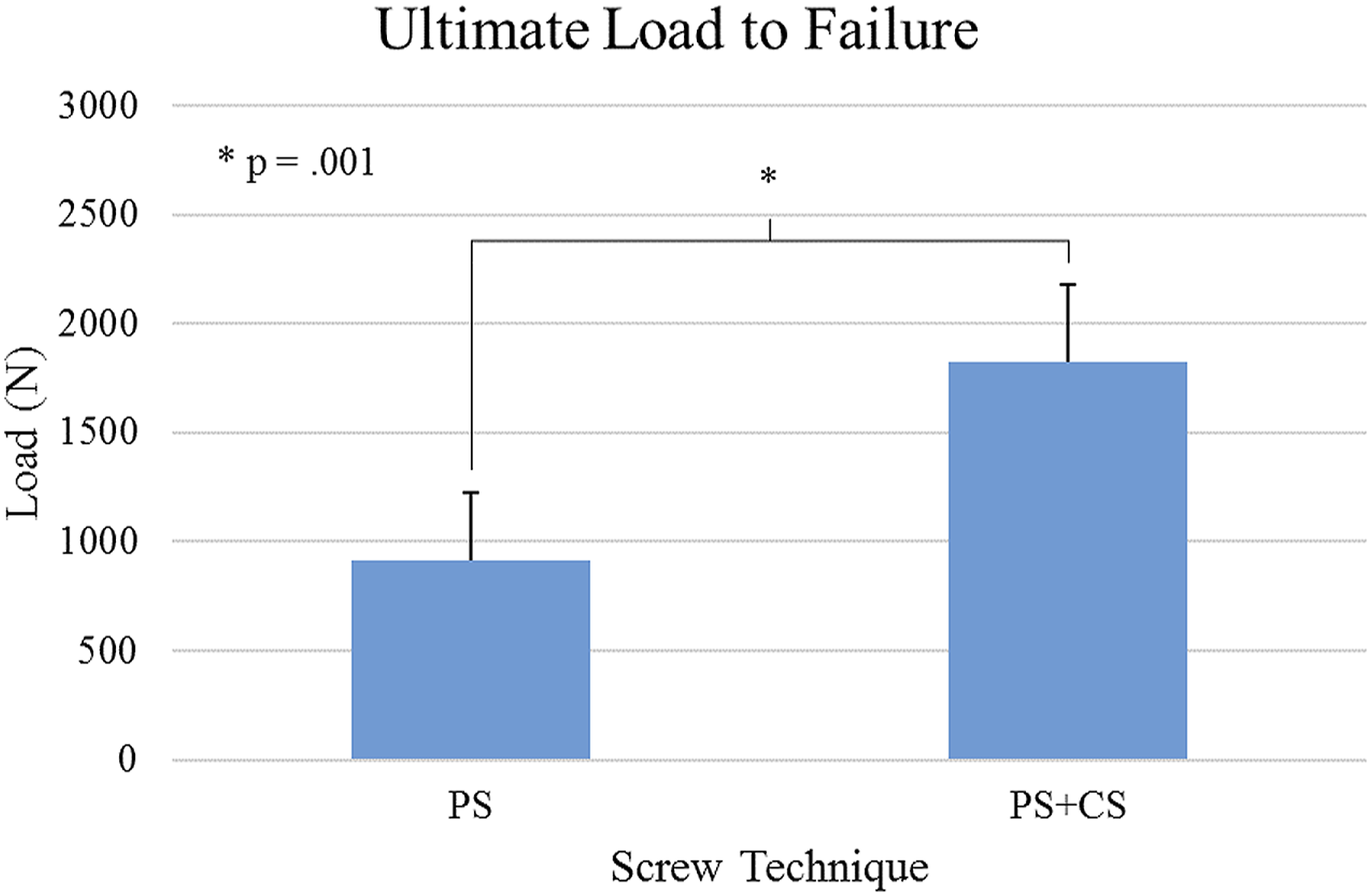
Four-rod construct was more rigid than 2-rod in FE (P < .001), LB (P < .001), AR (P < .001). Screw technique had no significant effect on FE (P = .516), LB (P = .477), or AR (P = .452). PS + CS 4-rod construct was significantly more stable than PS group (P = .032). Stiffness of PS + CS group (445.8 ± 79.3 N/mm) was significantly greater (P = .019) than PS (317.8 ± 79.8 N/mm). Similarly, failure load of PS + CS group (1824.9 ± 352.2 N) was significantly greater (P = .001) than PS (913.4 ± 309.8 N).
Conclusions
Dual-screw, 4-rod construct may be more stable than traditional rod-to-rod connectors, especially in axial rotation. Axial stiffness and ultimate strength of 4-rod, dual-screw construct were significantly greater than rod-to-rod. In this study, 4-rod construct was found to have potential biomechanical benefits of increased strength, stiffness, stability.
Keywords
Introduction
Despite improvement of spinal implants and techniques, risk of failure persists for transpedicular fixation, especially in cases of osteopenic bone, where decreased mineral density strongly influences pullout strength. 1 In patients undergoing transpedicular fixation, failure requires pedicle screw revision. 2 Several methods are proposed to improve screw fixation, including cement augmentation,3,4 or adding satellite rods to the primary construct,5,6 thus increasing stability.
Adding satellite rods to create 4-rod constructs improves stability, 6 alleviates primary rod strain,7,8 and increases fatigue resistance. 9 This study proposes a new 4-rod surgical technique utilizing 4 posterior screws per vertebral level, accomplished by placing pedicle and cortical screws in the same vertebra. Both cortical and traditional pedicle screws, used separately, provide effective stabilization of lumbar spinal fusions. They have shown equivalent biomechanical stability through kinematics, pullout strength, and toggle testing.10–13 Further, both trajectories achieve similar fusion rates and improvements in pain amelioration and functional status. 14
Since these screws follow different trajectories, it may be feasible to insert them simultaneously in 1 pedicle. Utilizing both trajectories in 1 pedicle has been investigated as a possible revision strategy. In a human cadaveric study, Calvert et al 12 used cortical screws to replace failed pedicle screws, and vice versa, and found both revisions retained adequate construct stiffness and pullout strength. In a small case series (n = 5), Rodriguez et al 15 used navigation to place cortical screws in pedicles already treated with pedicle screws to extend constructs without removing primary implants in adjacent segment disease cases, finding this a successful revision strategy. Matsukawa et al 16 used finite element modeling to simulate combined traditional and cortical trajectory pedicle screws, demonstrating increased fixation strength compared to traditional techniques. A case study from Ueno et al 17 reported on a 64-year-old woman with severe scoliosis and osteoporosis who were treated with a dual-screw technique to address increased risk for correction loss and pseudarthrosis. The patient experienced an uneventful postoperative course; 14-month follow-up confirmed solid fusion.
Despite promising prior cadaveric, finite element, and limited clinical results, additional studies are needed to investigate using this dual pedicle screw technique to achieve a 4-rod construct. To the authors’ knowledge, a thorough cadaveric investigation of the biomechanics and strength of such a construct does not exist. A dual-screw, 4-rod system has potential biomechanical advantages over 2-rod or traditional 4-rod satellite systems. Instead of relying on rod-to-rod connectors, which distribute the load of 4 rods spanning a motion segment across 2 fixation points, this technique distributes load across 4 fixation points. The present study addresses this gap in literature by testing stability of the dual-screw, 4-rod technique in an osteopenic vertebral compression fracture model (VCF). It was hypothesized that a dual-screw, 4-rod construct would demonstrate increased biomechanical stability and ultimate load-to-failure compared to 4-rod constructs achieved with traditional bilateral pedicle screws and rod-to-rod connectors.
Methods
Specimen Preparation
Fourteen fresh-frozen osteoligamentous human cadaveric lumbar spines (L1–L5) were tested. Each donor’s medical history was examined to exclude trauma, malignancy, or metabolic disease that might compromise the lumbar spines’ biomechanical properties. Specimens were radiographed in both anteroposterior (AP) and lateral planes to ensure absence of fractures, deformities, disc narrowing, and any metastatic disease. Paravertebral musculature was carefully denuded, avoiding disruption of spinal ligaments, joints, or discs. Dual-energy X-ray absorptiometry scans were obtained in the coronal plane with a Lunar Prodigy Scanner 8743 (GE Medical Systems, Madison, WI, USA), using a water-bath protocol. 18 All specimens were double-wrapped in plastic bags and stored at −20°C until tested. Specimens were fixed proximally (L1) and distally (L5) with a 1-to-1 mixture of Bondo® Body Filler and fiberglass resin (Bondo MarHyde Corp, Atlanta, GA, USA).
Creation of Vertebral Compression Fracture
An injury model was selected to mimic naturally occurring, high-energy VCFs through transmission of a heavy axial load dropped from above the specimen. The technique was based on Bartanusz et al,
19
described as follows: The level of burst fracture (L3) was weakened using a power drill to create 1/8” holes through the vertebral body. To allow for a controlled burst fracture of only the level of interest. A custom-built drop tower was used to guide the axial load onto the specimen.19,20 Multiple axial drops of a 45lb weight from 30 inches created the VCF at L3 (Figure 1). Example of radiographs before (left) and after (right) creation of VCF at L3.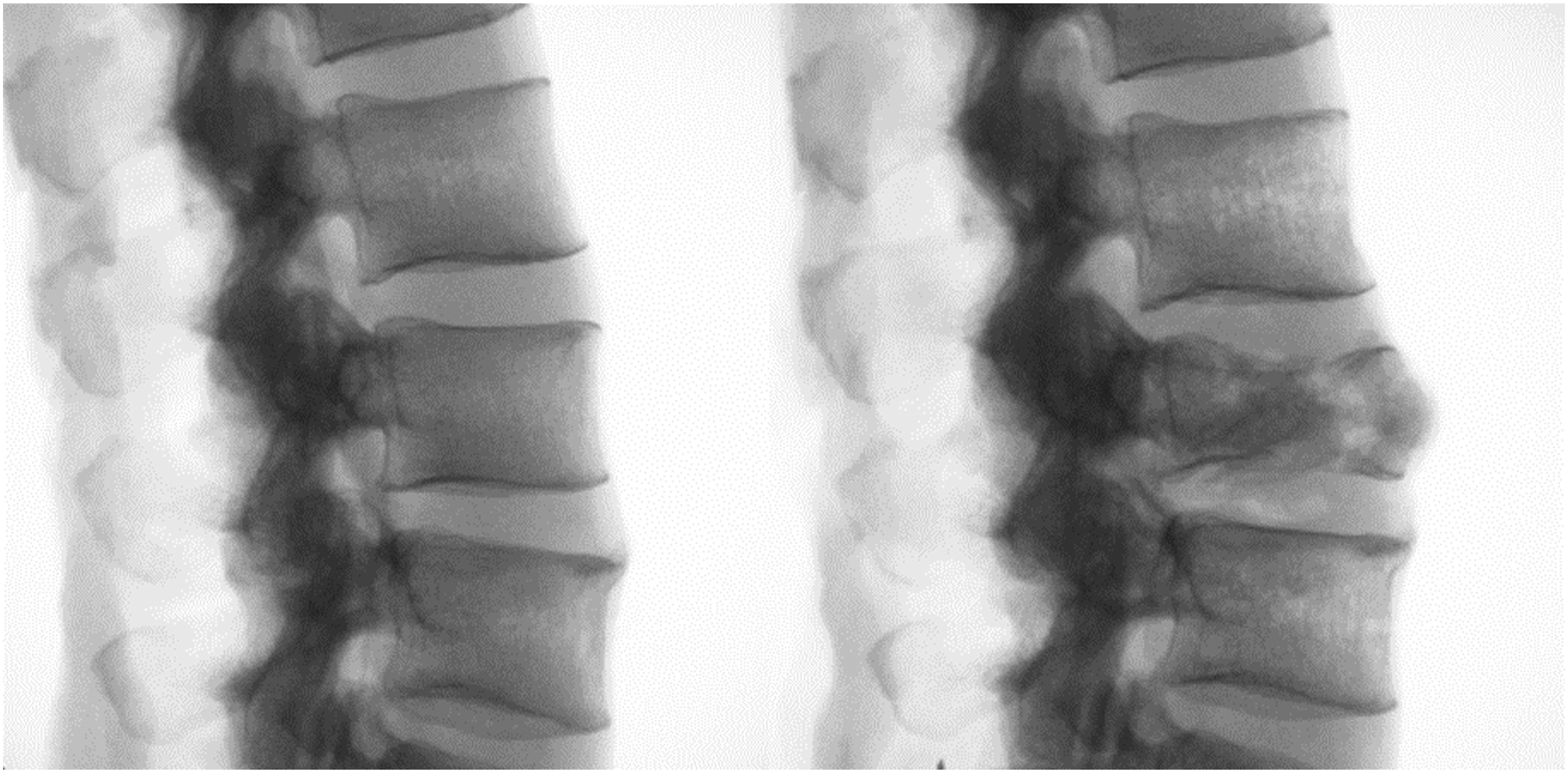
Surgical Technique and Constructs
Following VCF creation, specimens were separated into equal groups (n = 7) with similar average bone mineral density (P = .824): pedicle screws only (PS) and pedicle screws with cortical screws (PS + CS). T-scores of PS and PS + CS groups were -2.2 ± 1.3 and -2.1 ± .6, respectively. Specimens were bilaterally stabilized with pedicle screws from L2–L4 in each group. To ensure proper screw placement, a robotic guidance and navigation system (Excelsius GPS®, Globus Medical, Inc, Audubon, PA, USA) was utilized, with an intraoperative computed tomography (CT) scanner (O-Arm® Intra-operative 2D/3D Imaging System, Medtronic, Inc, Minneapolis, MN). Screws were placed through a rigid robotic arm that aligned precisely to planned trajectories. (Figure 2). Specimens in both groups were tested as 2-rod and 4-rod constructs. Example of robotic planning of traditional pedicle and cortical bone trajectory screws within the same lumbar pedicles.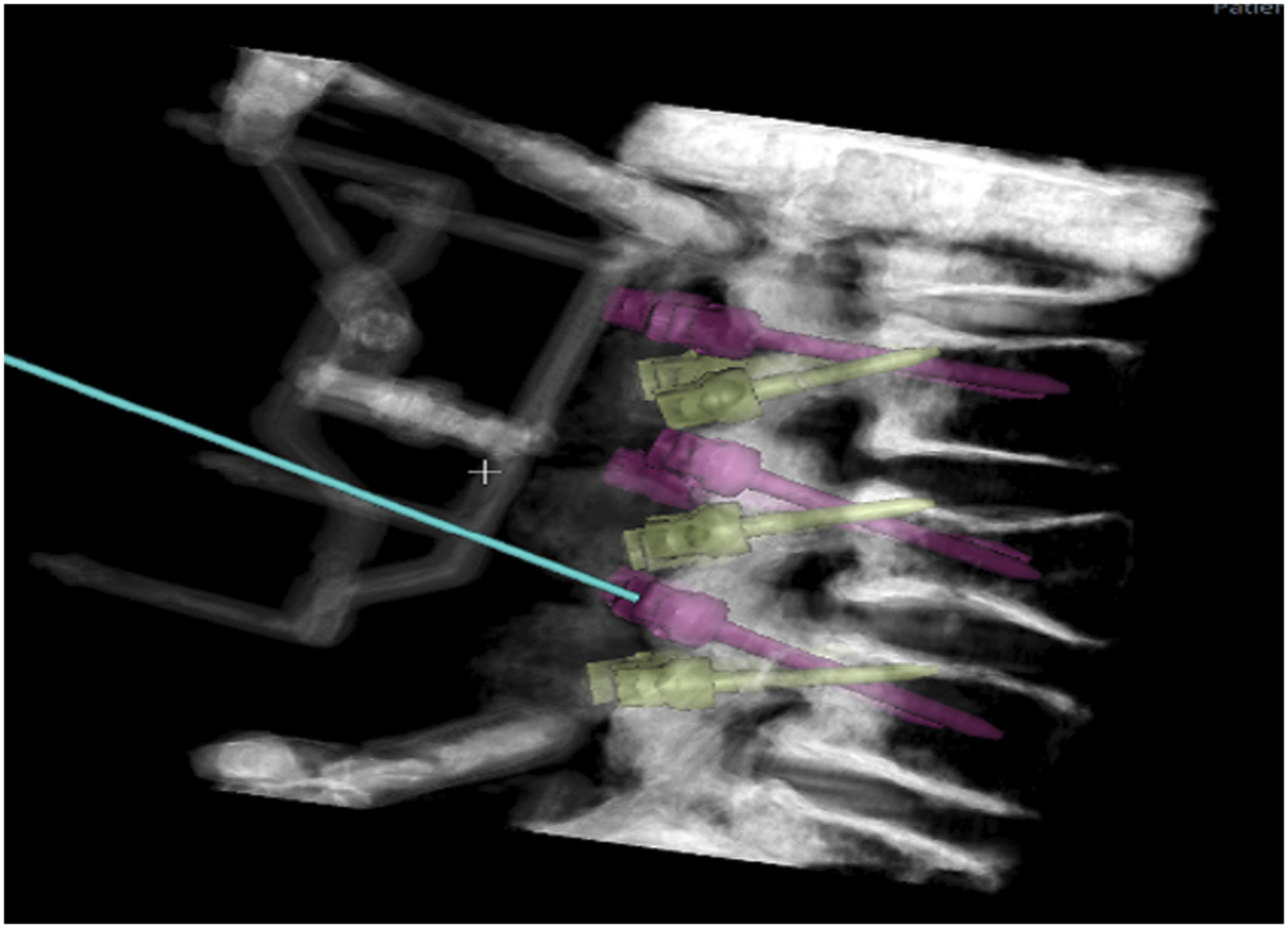
Pedicle Screw Group
Pedicle screws (CREO® Stabilization System, Globus Medical, Inc) were inserted using the Weinstein “lateral-to-medial-converging” PS technique (Figure 3).
21
Screw size was determined by specimen anatomy. An intraoperative CT scan was used to check for pedicle breaches. For the 2-rod construct, 5.5 mm-diameter longitudinal titanium-aluminum-vanadium (TAV) rods were placed bilaterally spanning L2–L4. For the 4-rod construct, rod-to-rod connectors were used to connect primary pedicle screw rods to additional satellite 5.5 mm-diameter TAV rods bilaterally. Example axial radiographs of screw trajectories of the PS (left) and PS + CS (right) groups.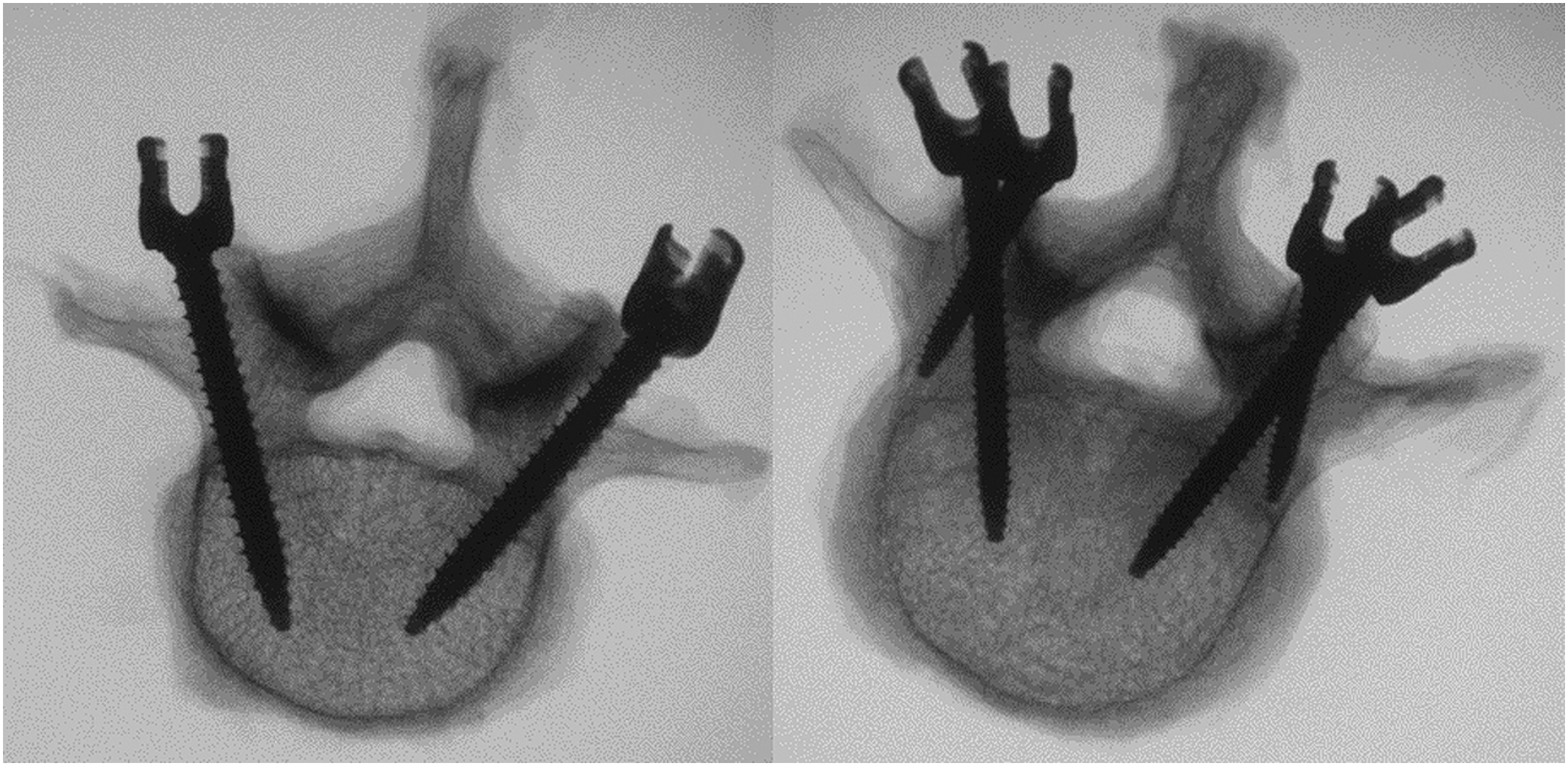
Pedicle Screw + Cortical Screw Group
Dual outer diameter (DOD) cortical screws (CREO MCS® Stabilization System, Globus Medical, Inc.) were inserted first, using a modified Roy-Camille “straight ahead” technique. 22 The starting point for cortical screws was at the intersection of horizontal and longitudinal lines bisecting the transverse process and facet joint, respectively. This point was medial to that of the pedicle screw. Cortical screws were angled cranially toward the superior vertebral endplate (Figure 3). All cortical screws were 5.0-4.0 mm in diameter and 35 mm in length.
Pedicle screws were inserted second, again using the Weinstein “lateral to medial converging” PS technique. 21 Compared to the PS group, the entry point of pedicle screws in the PS + CS was placed more superiorly the trajectory was angled slightly caudally. These differences in starting point and trajectory were necessary to allow room in the pedicle for cortical screw placement. Pedicle screw size was determined by specimen anatomy and space left in the pedicle following cortical screw placement. An intraoperative CT scan was used to check for pedicle breaches. For the 2-rod construct, longitudinal 5.5 mm-diameter TAV rods were placed bilaterally only in pedicle screws, spanning L2–L4. For the 4-rod construct, additional 5.5 mm-diameter TAV rods were placed in cortical screws bilaterally, spanning L2–L4.
Multidirectional Testing
Range of motion (ROM) was evaluated using a custom-built 6 degrees-of-freedom (6DOF) machine (Figure 4) and motion analysis software (Optotrak Certus® Northern Digital Inc, Waterloo, Canada). Cranial (L1) and caudal (L5) portions of the specimen were mounted to the 6DOFsimulator. The spine was subjected to pure, unconstrained bending moments directed in flexion-extension (FE), lateral bending (LB), and axial rotation (AR) by 3 cephalad stepper motors supported by near-frictionless air bearings. A load control protocol of ±7.5 Nm was applied at a velocity of 1.5°/s.
23
Each of 3 test constructs for both groups – (1) intact, (2) 2-rod, and (3) 4-rod – underwent 3 loading/unloading cycles in each direction of bending with data analysis based on the final cycle to allow for tissue viscoelasticity. Plexiglas markers were fixed to L1, L2, L4, and L5 vertebral bodies to track specimen motion using the motion analysis system, which superimposes coordinate systems of 2 adjacent rigid bodies to determine relative Eulerian rotations in each plane, with .1 mm accuracy and .01 mm resolution. Relative motion was calculated between proximal (L2) and distal (L4) ends of the surgical construct. ROM data were averaged and normalized to average intact ROM for each group. Example photographs of multidirectional testing on L2–L4 specimen (left) and quasistatic axial testing of 4-rod PS + CS construct (right).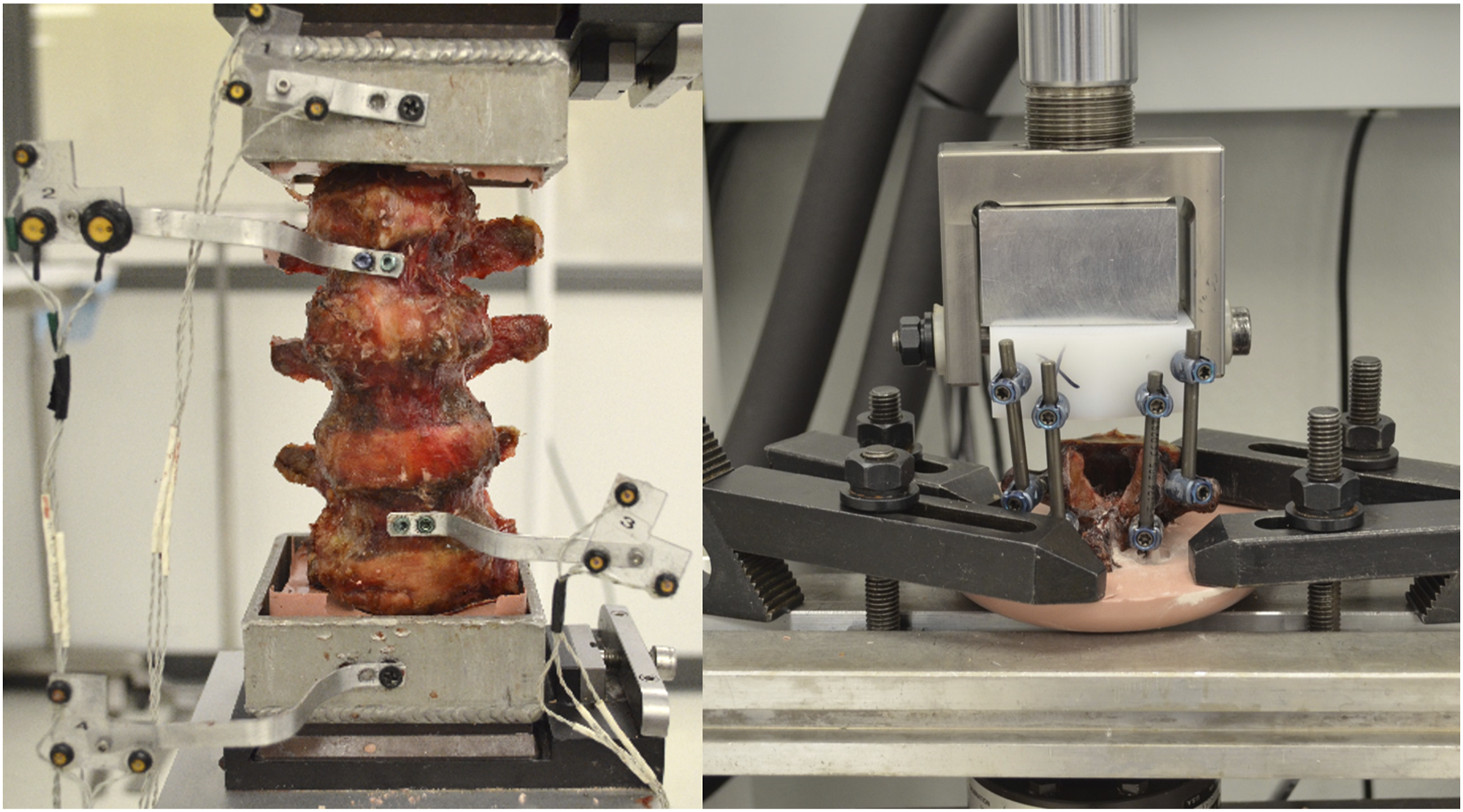
Static Compression
Following ROM testing, the L2 vertebra was disarticulated from the specimen. Using a setup similar to methodology used by Jiang et al, 24 each L2 vertebra was used for quasistatic compression testing of the 4-rod construct using an MTS Bionix® 858 Test System (MTS Systems Corporation, Eden Prairie, MN, USA). An ultra-high-molecular-weight polyethelene (UHMWPE) block was attached to the actuator such that it could only translate axially, and not rotate. Four pedicle screws were inserted into the UHMWPE block so 4 5.5 mm-diameter TAV longitudinal rods could be attached. In the PS group, 2 of these rods were connected to L2 pedicle screws. Two additional rods were attached to primary rods, with rod-to-rod connectors. In the PS + CS group, 2 rods were connected to L2 pedicle screws and 2 rods were connected to L2 cortical screws (Figure 4). Screw-to-screw distance between L2 and UHMWPE screws was approximately 65 mm. Quasistatic loading was applied axially until failure at a 5 mm/min rate. Failure load and axial stiffness for each specimen were recorded and used for data analysis.
Statistical Analysis
Statistical analysis was performed using IBM SPSS® Statistics (SPSS® v24, IBM Corp, Armonk, NY, USA). Outliers, whose values were greater or less than the data median by at least 1.5x the interquartile range were excluded. A mixed-model analysis of variance with repeated measures and Bonferroni post hoc analysis was performed to assess the main effects of screw technique (PS vs PS + CS) and rod construct (intact vs 2-rod vs 4-rod) on normalized ROM, and any interactions between these main effects. When interactions of main effects was significant, differences in normalized ROM between screw technique and differences in normalized ROM between rod constructs tested within each treatment group were also assessed. An independent t-test was used to analyze differences between PS and PS + CS groups in axial stiffness and failure load of 4-rod constructs. Significance for all tests was defined as P < .05.
Results
Specimen Age, Height, Weight, and Pedicle Dimensions (Mean ± StDev).

Raw ROM of Intact, 2-rod, and 4-rod Constructs.

Screw technique had no significant effect on FE (P = .516), LB (P = .477), or AR (P = .452). There was, however, interaction between screw technique and rod construct for normalized AR ROM (P = .025). Significant differences between and within test groups in AR are shown in Figure 5. There were no significant interactions between treatment group and test construct for FE (P = .247) or LB (P = .599). ROM normalized to intact, of the rod constructs for the PS and PS + CS treatment groups.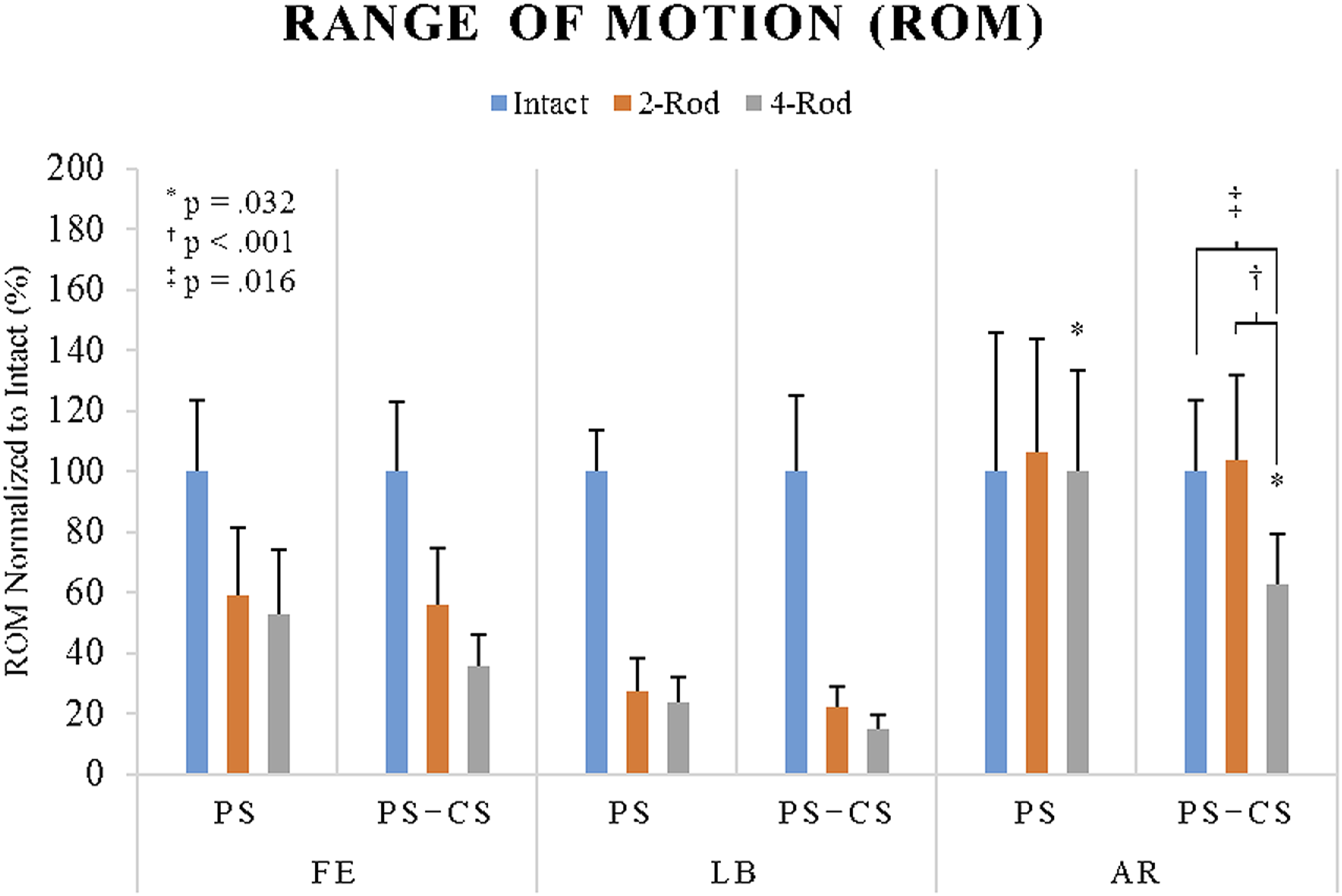
Static compression testing revealed significant differences in axial stiffness and failure load between PS and PS + CS screw techniques in 4-rod constructs (Figures 6 and 7). Stiffness of the PS + CS group (445.8 ± 79.3 N/mm) was significantly greater (P = .019) than the PS group (317.8 ± 79.8 N/mm). Similarly, failure load of the PS + CS group (1824.9 ± 52.2 N) was significantly greater (P = .001) than the PS group (913.4 ± 309.8 N). Axial stiffness of 4-rod construct for PS and PS + CS groups as determined by quasistatic loading on a single vertebra. Ultimate load to failure of 4-rod construct for PS and PS + CS groups as determined by quasistatic loading on a single vertebra.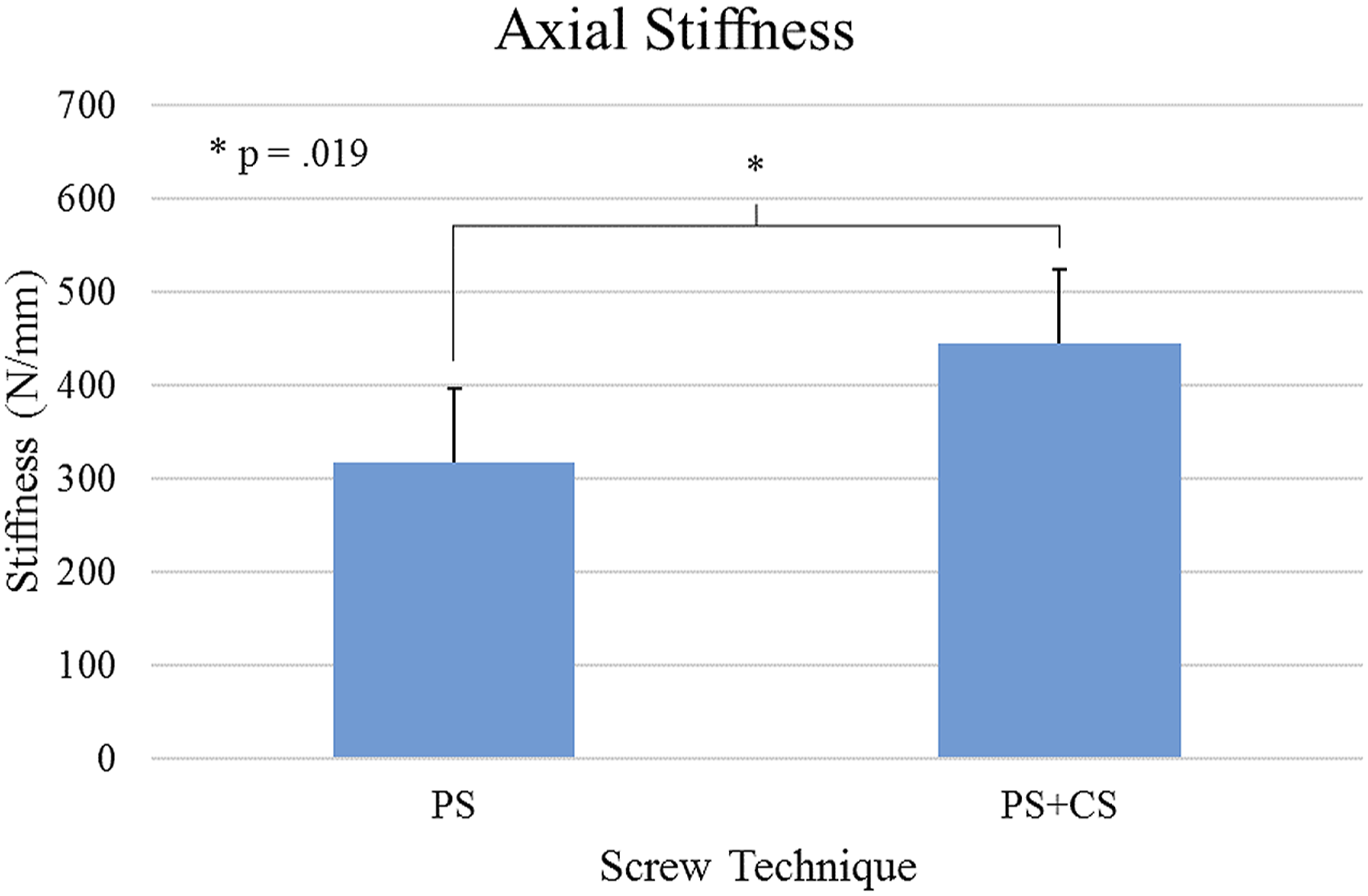
Discussion
While traditional pedicle screws are the most commonly used method for posterior spinal fusion, implant failure can occur. The cortical bone trajectory offers an alternative technique with biomechanical properties comparable to traditional pedicle screws. 10 Use of cortical screws in conjunction with traditional pedicle screws is novel. With limited clinical evidence of its use, the dual-trajectory technique remains untested but offers possibilities of improved support and stability.15,17
One purpose of this investigation was to evaluate feasibility of a dual-screw technique within a vertebral compression fracture cadaveric model. Mullin et al 25 assessed feasibility of placing both a traditional pedicle screw and cortical screw at all lumbar levels using 3-dimensional spinal navigation system and were able to successfully implement this technique in 70% of pedicles without prior fixation, and 40% of pedicles with pre-existing traditional pedicle screws. In this study, authors successfully used robotic guidance and navigation to plan and place both traditional pedicle and cortical screws in the same lumbar pedicle in all tested pedicles, including those of the upper lumbar spine. There were no incidences of a screw breaching the pedicle or the vertebral body.
Another aim of this study was to evaluate biomechanical stability, strength, and stiffness of a 4-rod construct achieved using the dual-screw technique. Four-rod constructs in spinal fusions have been previously investigated in a variety of clinical applications. Several authors have investigated 4-rod constructs achieved with rod-to-rod connectors for primary and satellite rods to reduce risks of rod failure following pedicle subtraction osteotomy.5–9,26 However, none of these studies achieved their 4-rod construct by utilizing 4 screws per vertebral level, as performed in the present study.
Across both screw techniques, both 2- and 4-rod constructs significantly reduced FE and LB motion compared to intact. This study showed that 4-rod constructs, independent of if achieved with a dual-screw construct or rod-to-rod connectors, provided more biomechanical stability than 2-rod constructs, although this was only statistically significant in AR for PS + CS group. Motion of 2-rod constructs did not differ between PS and PS + CS groups, as these constructs are largely the same, with only small differences in starting point and trajectory of their traditional pedicle screws. The PS + CS group 4-rod construct was more rigid than the PS group’s. This difference was only statistically significant in AR. Results suggest that a 4-rod construct using dual-screw technique may be more biomechanically stable than 4-rod constructs relying on rod-to-rod connectors.
The present study’s quasistatic compression testing results appear to align with previous studies, as ultimate strength and stiffness of 4-rod constructs were considerably greater than 292.1N-633.4 N ultimate strength and 23.7 N/mm–38.0 N/mm stiffness of 2-rod pedicle screw constructs tested in a similar method by Stanford et al. 27 Since traditional pedicle and cortical screws follow different trajectories, a dual-screw construct effectively doubles fixation points, increasing total screw purchase and providing more resistance to failure. In the present study, ultimate load-to-failure of 4-rod construct using a dual-screw technique was approximately 100% greater than the similar construct created with rod-to-rod connectors. Four-rod construct axial stiffness in PS + CS was also approximately 40% greater than the PS group.
The present study had several limitations common with cadaveric testing. Sample size was limited due to the cost and availability of cadaveric specimens that met all criteria the study. Pure bending moments were applied to assess ROM; however, without in vivo muscle forces and axial loading of the spine, this may not be representative of true physiological bending. Further, while the authors believe the VCF model used to simulate high-energy compression fracture to be a sufficient representation of instability caused in such a fracture, it is possible that the model is not completely representative of VCFs seen clinically. The authors also acknowledge that most VCF injuries do not require surgical intervention, but the model was selected to produce a consistent, repeatable injury across all specimens. Finally, all specimens were male, with large pedicles to ensure appropriate placement of 2 screws. Dual-screw technique feasibility may limited by patient anatomy; however, this was beyond the present study’s scope.
Further cadaveric testing could be useful to elucidate additional biomechanical knowledge of the 4-rod, dual-screw construct. Future studies may investigate this technique’s feasibility across varying patient anatomy, more unstable fracture types or pathologies, or in thoracic and cervical pedicles, which would greatly increase the number of clinical scenarios where this technique may be used. Dynamic specimen bending over time could be useful in understanding the 4-rod, dual-screw construct’s resistance to fatigue. Further, feasibility of robotic guidance and navigation to assist in inserting cortical bone trajectory screws into cadavers with pre-existing, unplanned pedicle screws could be investigated as a potential revision technique.
Conclusions
This study evaluated feasibility and biomechanical stability, strength, and stiffness of a novel dual-screw, 4-rod construct achieved through placement of a traditional pedicle and cortical screw in the same pedicle. The dual-screw technique was successfully completed in all lumbar pedicles tested using robot-assisted guidance and navigation. The dual-screw, 4-rod construct may be more stable than a 4-rod construct achieved with traditional rod-to-rod connectors, especially in axial rotation, where this difference was statistically significant. Finally, axial stiffness and ultimate strength of the 4-rod, dual-screw construct was significantly greater than the comparable rod-to-rod construct. This study found the dual-screw, 4-rod construct to have potential biomechanical benefits of increased strength, stiffness, and stability. Further research is needed to assess this technique’s safety and efficacy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by Globus Medical, Inc.