
Abstract
Study Design
Prospective cohort study.
Objectives
In spine surgery, accurate screw guidance is critical to achieving satisfactory fixation. Augmented reality (AR) is a novel technology to assist in screw placement and has shown promising results in early studies. This study aims to provide our early experience evaluating safety and efficacy with an Food and Drug Administration-approved head-mounted (head-mounted device augmented reality (HMD-AR)) device.
Methods
Consecutive adult patients undergoing AR-assisted thoracolumbar fusion between October 2020 and August 2021 with 2 -week follow-up were included. Preoperative, intraoperative, and postoperative data were collected to include demographics, complications, revision surgeries, and AR performance. Intraoperative 3D imaging was used to assess screw accuracy using the Gertzbein-Robbins (G-R) grading scale.
Results
Thirty-two patients (40.6% male) were included with a total of 222 screws executed using HMD-AR. Intraoperatively, 4 (1.8%) were deemed misplaced and revised using AR or freehand. The remaining 218 (98.2%) screws were placed accurately. There were no intraoperative adverse events or complications, and AR was not abandoned in any case. Of the 208 AR-placed screws with 3D imaging confirmation, 97.1% were considered clinically accurate (91.8% Grade A, 5.3% Grade B). There were no early postoperative surgical complications or revision surgeries during the 2 -week follow-up.
Conclusions
This early experience study reports an overall G-R accuracy of 97.1% across 218 AR-guided screws with no intra or early postoperative complications. This shows that HMD-AR-assisted spine surgery is a safe and accurate tool for pedicle, cortical, and pelvic fixation. Larger studies are needed to continue to support this compelling evolution in spine surgery.
Keywords
Introduction
Accurate pedicle screw placement is crucial to achieving stable posterior fixation and avoiding complications in spinal surgery. There is growing interest in the use of augmented reality (AR) navigation in spine surgery as an alternative to the current approaches: traditional navigation, robotic-guidance, fluoroscopic-guidance, and freehand.1-7 Augmented reality systems are capable of projecting patient anatomy directly onto the surgical field, eliminating the need for the surgeon to break line-of-sight with the patient while operating. Prior AR studies in spine surgery have shown potential in decreasing intraoperative radiation exposure to operating room staff. 8 Several versions of AR are described in the literature, including systems that incorporate a head-mounted device (HMD) in the surgical workflow. 9 To date, only one HMD-AR system has received FDA approval, granted in December 2019.
There are limited in vivo studies demonstrating the safety, efficacy, and accuracy of HMD-AR navigation when used in spine surgery. Prior studies have shown that AR-guided navigation systems are simple to integrate into modern operating rooms with limited disruptions in traditional workflow and higher screw placement accuracy than traditional freehand techniques.9-12 The purpose of this study is to provide an early experience safety profile and accuracy rating of HMD-AR-guided posterior instrumentation in a cohort of patients undergoing thoracolumbar spinal fusion by 3 fellowship-trained spine surgeons novice to AR technology. We hypothesized that intra- and postoperative complication rates, revision rates, and screw accuracy would be comparable to traditional freehand, fluoroscopic-guided, and robotic-guided techniques without a learning curve.
Methods
Study Design and Patient Selection
This is an IRB-approved prospective observational study of adult patients (age 18–76) undergoing AR-navigated thoracolumbar fusion surgery between October 2020 and August 2021 at a multi-surgeon, single institution (Advarra Pro00042720, 5/16/2020). Surgeries were performed by 3 board certified spine surgeons using the only FDA-approved AR system for spine surgery, xvision-Spine (XVS) system (Augmedics, Ltd, Philadelphia, PA). All 3 surgeons in this study were experienced with other guidance techniques, including fluoroscopy, navigation and robotics, and were able to begin utilizing the HMD-AR system after only 2–3 hours of training with cadavers and demonstration models. All patients signed informed consent and a notice of privacy practices prior to surgery.
Data Collection
Preoperative patient demographic information, Charlson Comorbidity Index (CCI), and smoking status, was collected using electronic questionnaires. Intraoperative data was collected using case report forms (CRFs) and included: complications, radiation time/dose, number of screws revised due to misplacement, estimated blood loss (EBL), surgical time, and adverse events. In-hospital data included: postoperative complications, revisions, and length of stay. Postoperative data collected at 2 weeks included: medical and surgical complications and revision rates.
Intraoperative 3D imaging was performed following instrumentation. The AR-placed screws were graded for accuracy using the highly cited Gertzbein-Robbins (G-R) grading scale by two fellowship-trained spine surgeons and one independent neuroradiologist. 13 A modified G-R grading scale was used to grade S2AI screw accuracy, which reflects screw deviation from the ideal trajectory; a screw breach was defined as perforation of cortical bone resulting in any portion of the screw protruding outside the confines of the pelvis: Grade A screws had 0 mm breach, grade B screws had less than 3 mm breach, grade C screws had 3–6 mm breach, and grade D screws had greater than 6 mm breach.14,15
All analyses were performed using IBM SPSS V 27.0 (Armonk, New York). Descriptive statistics are presented as frequencies (percentages) or means and standard deviations.
Results
Patient Characteristics
Patient Characteristics.
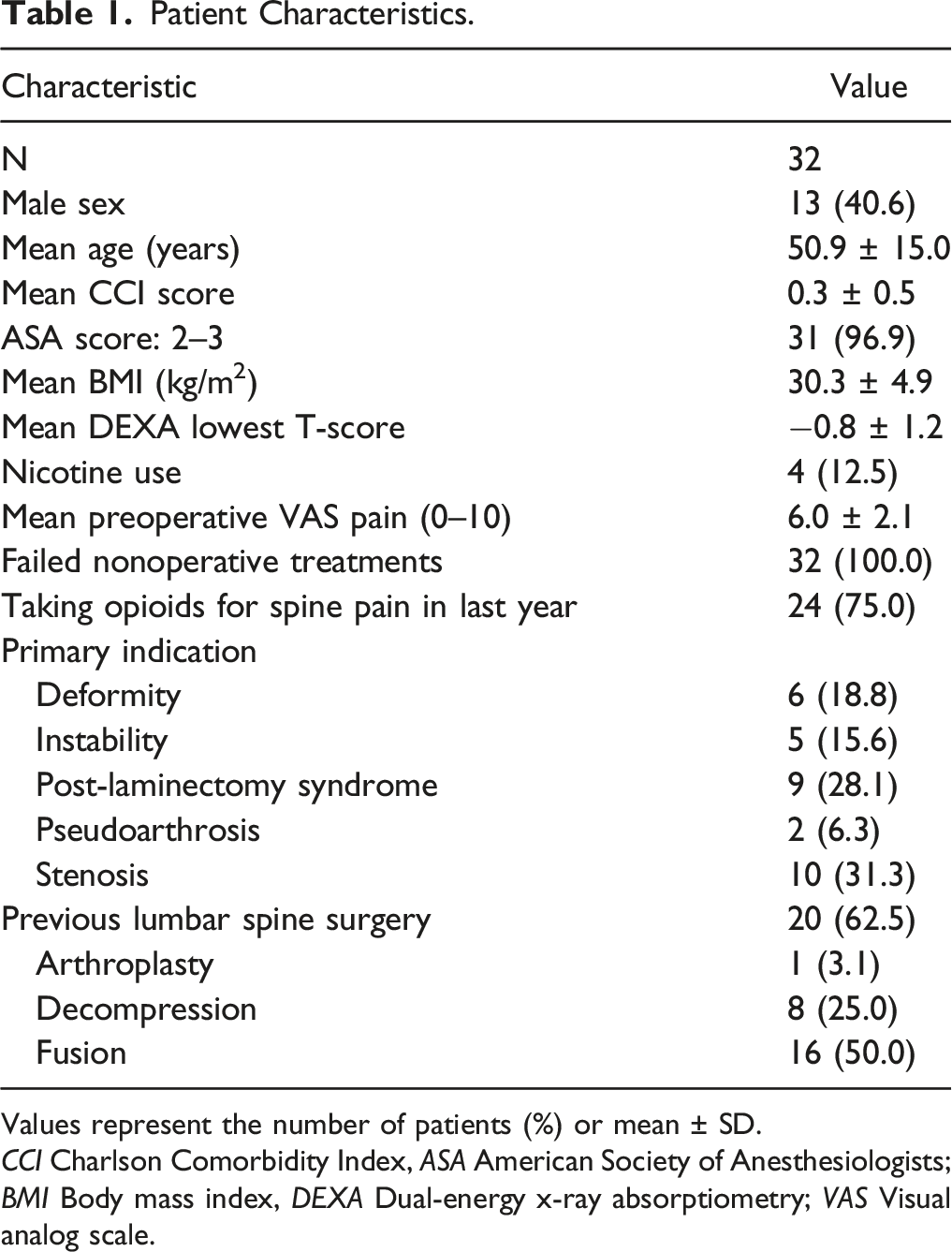
Values represent the number of patients (%) or mean ± SD.
CCI Charlson Comorbidity Index, ASA American Society of Anesthesiologists; BMI Body mass index, DEXA Dual-energy x-ray absorptiometry; VAS Visual analog scale.
Surgical Details
Surgical Details.
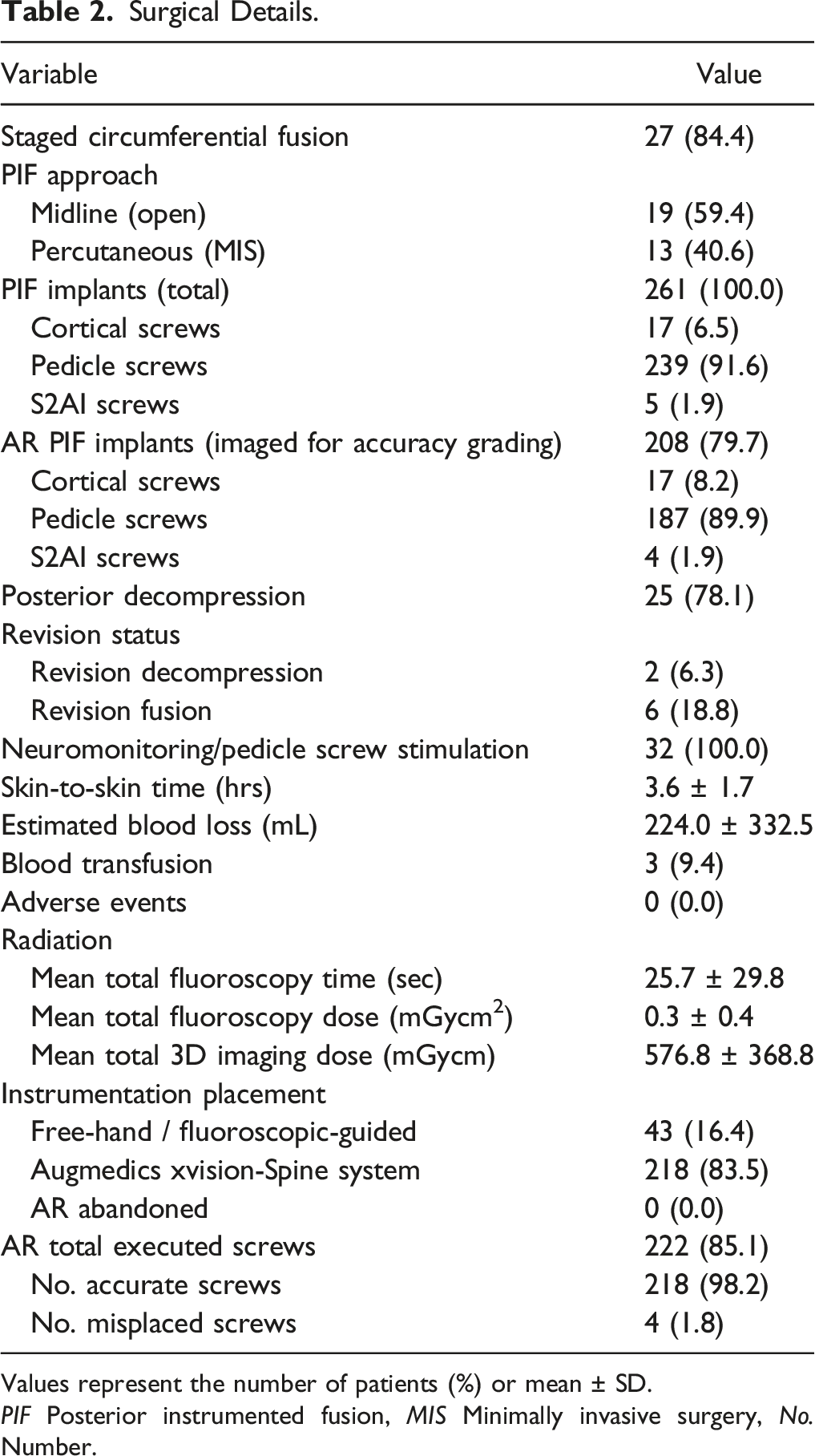
Values represent the number of patients (%) or mean ± SD.
PIF Posterior instrumented fusion, MIS Minimally invasive surgery, No. Number.
Accuracy Grading and Complication and Revision Rates
Accuracy Grading.
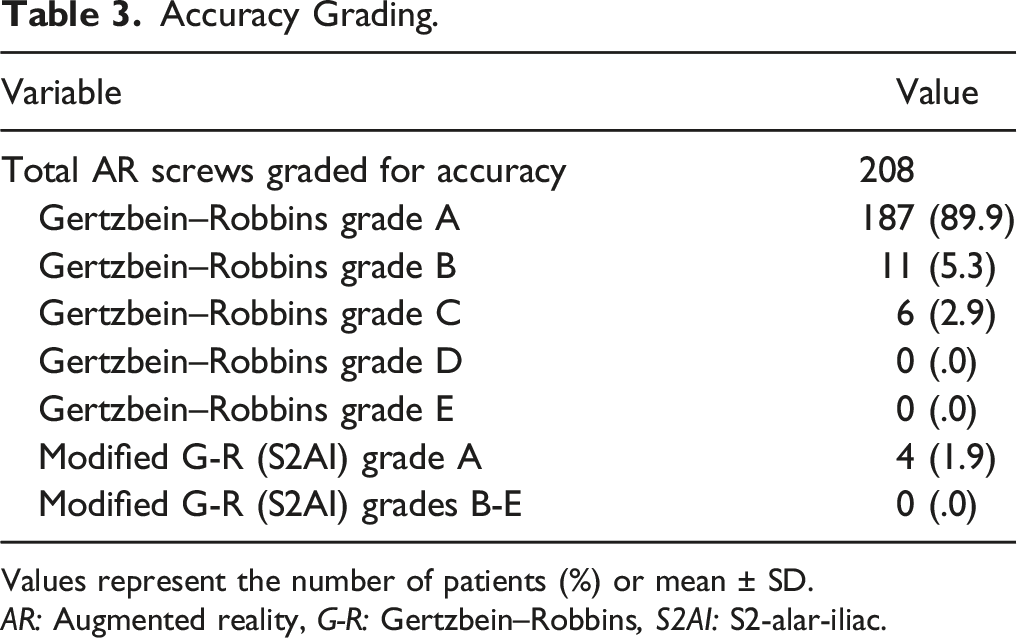
Values represent the number of patients (%) or mean ± SD.
AR: Augmented reality, G-R: Gertzbein–Robbins, S2AI: S2-alar-iliac.
Complications and Revision Rates.
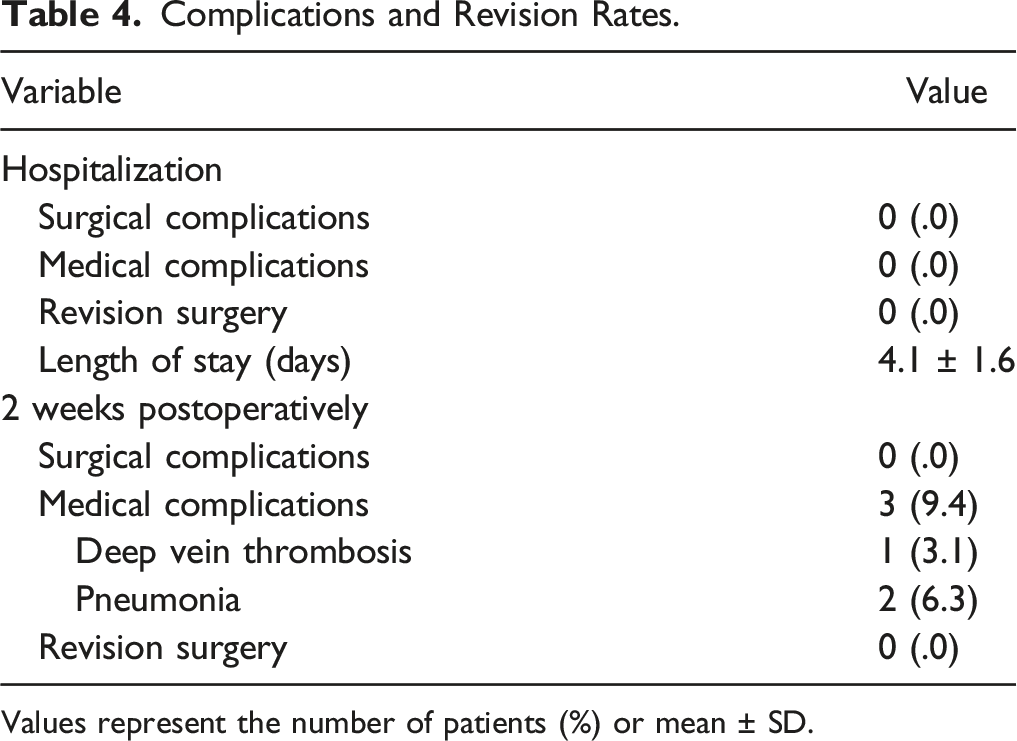
Values represent the number of patients (%) or mean ± SD.
Discussion
To the best of our knowledge, this study has the largest sample size to date reporting complication and accuracy rates for AR-assisted posterior instrumented thoracolumbar fusions using a HMD. We report an overall screw accuracy rate of 97.1% (Gertzbein-Robbins Grade A or B) for 208 AR-placed thoracic, lumbosacral, and pelvic screws. While there were 3 medical complications, no intraoperative or postoperative surgical complications occurred, and no patients required early revision surgery within a 2 -week period.
Head-mounted AR devices have been shown in preliminary studies to be effective during cannulation and pedicle screw placement.16-18 HMD-AR has also been found to have excellent pilot hole placement rates in both novice and experienced surgeons, as well as significantly reduced breach rates in AR-placed screws compared to screws placed freehand in a laboratory setting.
19
In our in vivo study, only 4 out of 222 planned AR screws were considered misplaced as defined by pedicle screw stimulation of less than 10 mA. In two separate instances, a slight medial breach was determined by intraoperative CT imaging, these screws were removed and revised using the same HMD-AR technology. Figure 1 depicts an example of a slight medial breach that was revised using HMD-AR. Two other screws were found to have similar medial or lateral breaches and revised freehand at the surgeon’s discretion. Overall, these results coupled with the prior experience of the surgeons demonstrate that HMD-AR technology is highly effective in real-world scenarios without a significant learning curve using the technology. (a) Axial O-arm image prior to instrumentation used for AR registration demonstrating small right L2 pedicle (b) Axial O-arm image during instrumentation demonstrating slightly medial right L2 pedicle screw (c) Axial O-arm image at the completion of instrumentation demonstrating right L2 pedicle screw repositioned laterally.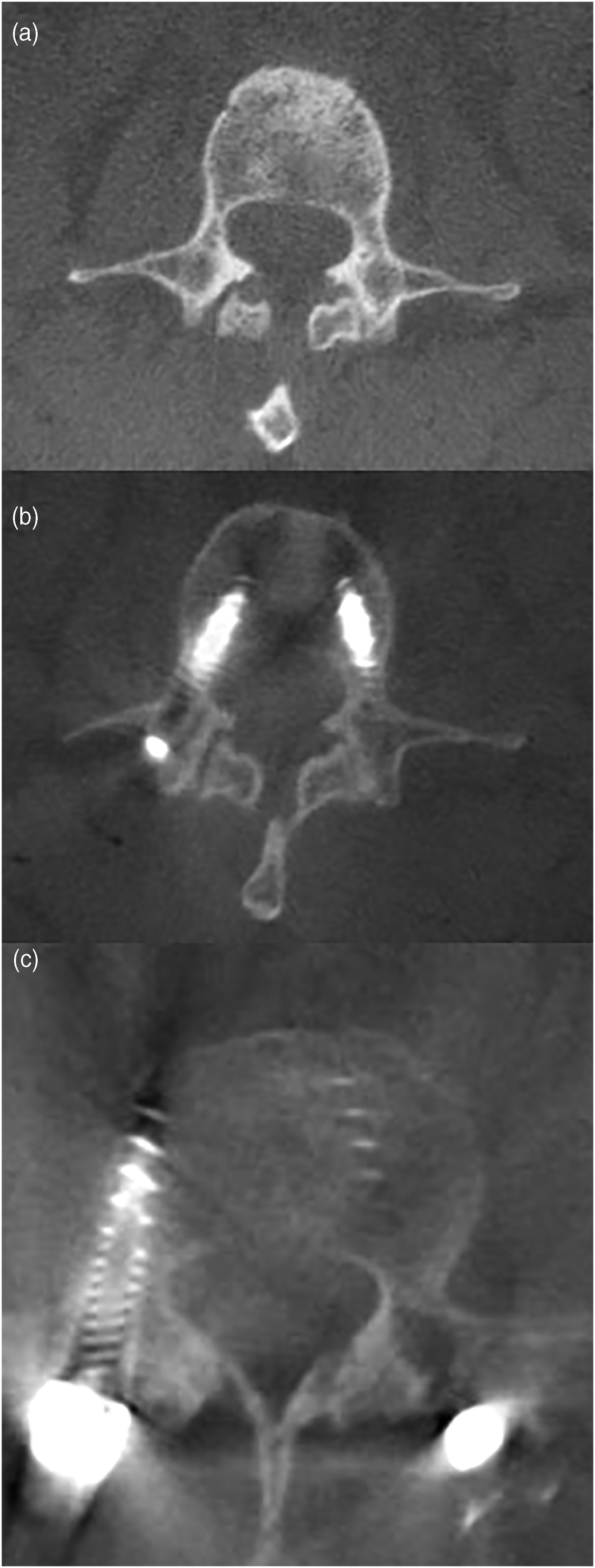
As spine surgery has evolved from utilizing traditional freehand and fluoroscopic-guided techniques to 3D imaging technologies such as navigation, robotics, and AR navigation, this paper aims to contribute our initial experience with and evaluation of AR technology. A recent meta-analysis in patients aged 4–22 found an overall complication rate of 5.84% for pedicle screws placed using various techniques: conventional freehand, modified freehand, and image-guided. 20 In the MIS reFRESH study by Good et al., at 1 year postop, the Hazard Ratios for complications and revision surgeries was 5.8 and 11.0 times higher, respectively, in the fluoroscopic-guided group than the robotic-guided group. 21 The retrospective analysis by Yahanda et al. showed excellent results in their cohort of 9 patients undergoing HMD-AR-guided percutaneous placement of 63 screws with no intra- or postoperative complications or revision surgeries up to the most recent follow up (which was not specifically defined, but was at least beyond the hospitalization period). 22 Similarly, we did not encounter any surgical complications or early revision surgeries in the intraoperative or immediate postoperative period. Our results compare favorably to the current literature and suggest that AR-assisted surgery has a low complication rate that is comparable to the current methods for screw placement assistance.
Studies evaluating pedicle screw accuracy often use the Gertzbein–Robbins (G-R) grading scale and consider G-R grades A or B clinically accurate, represented by a pedicle screw with 2 mm of a cortical breach or less.22,23 Several studies have attempted to characterize the accuracy of screws placed using AR technology. In a cadaveric study, Burstrom et al. reported a screw accuracy rate ranging from 97.4% to 100% based on screw diameter and Yahanda et al. reported 100% accuracy in vivo (63 screws) using the G-R grading system.22,23 In a larger cohort of 20 patients and 253 AR-guided screws using a monitor display, Elmi-Terander et al. reported a G-R accuracy rate of 94.1%. 24 Our unique study reports a similar screw accuracy rate (97.1%) with 3 spine surgeons using a head-mounted display and executing pedicle, cortical, and pelvic fixation. This is comparable to that reported in the literature for robotic-guided systems, where accuracy ranges from 97.9% to 100%, suggesting AR technology is a compelling alternative.25-28
The main limitation of this study is the 2-week length of follow-up. Although the primary aim of this paper was to measure intraoperative screw placement accuracy a secondary aim was to report on early complications and revision surgeries which can be affected by duration of follow-up. While our sample size is certainly the largest to date, larger multi-center studies will further characterize screw accuracy under a variety of conditions with different operators. The authors of this study intend to report further follow-up data to determine the long term complication and revision rates for patients undergoing AR-assisted screw placement.
Conclusion
This study reports on the safety and accuracy of 218 HMD-AR-guided screws in 32 patients with an overall Gertzbein–Robbins accuracy of 97.1%. There were no surgical complications or revision surgeries during the 2 -week postoperative period, suggesting that AR-guided screw placement is safe and accurate. While the results of our study show that AR is a compelling evolution in navigation for screw placement, further multi-center studies with larger sample sizes have greater potential to identify superiority to traditional techniques.
Footnotes
Declaration of Conflicting Interests
The author(s) declared following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Research Ethics Statement
This study was approved by a centralized IRB, Advarra, on May 16th (Pro00042720). This study was conducted in accordance with the 1964 Helsinki Declaration, its amendments, and other equivalent ethical standards. All study participants or their legally authorized representative signed written informed consent, included in the Notice of Privacy Practices, for study enrollment and publication prior to surgery.