
Abstract
Study Design
Retrospective cohort study
Objectives
The purpose of this study is to compare patient-reported outcome measures (PROMs) for patients undergoing one-to three-level lumbar fusion using robotically assisted vs freehand pedicle screw placement.
Methods
Patients who underwent either robotically assisted or freehand pedicle screw placement for one-to three-level lumbar fusion surgery from January 1, 2014 to August 31, 2020 at a single academic institution were identified. Propensity score matching was performed based on demographic variables. Clinical and surgical outcomes were compared between groups. Recovery Ratios (RR) and the proportion of patients achieving the minimally clinically important difference (%MCID) were calculated for Oswestry Disability Index, PCS-12, MCS-12, VAS Back, and VAS Leg at 1 year. Surgical outcomes included complication and revision rates.
Results
A total of 262 patients were included in the study (85 robotic and 177 freehand). No significant differences were found in ΔPROM scores, RR, or MCID between patients who underwent robotically assisted vs freehand screw placement. The rates of revision (1.70% freehand vs 1.18% robotic, P = 1.000) and complications (.57% freehand vs 1.18% robotic, P = .546) were not found to be statically different between the 2 groups. Controlling for demographic factors, procedure type (robotic vs freehand) did not emerge as a significant predictor of ΔPROM scores on multivariate linear regression analysis.
Conclusions
Robotically assisted pedicle screw placement did not result in significantly improved clinical or surgical outcomes compared to conventional freehand screw placement for patients undergoing one-to three-level lumbar fusion.
Keywords
Introduction
Pedicle screws are used as an adjunct in spinal fusion surgery to add additional support and stiffness across the fusion construct through their ability to stabilize all 3 columns of the spine. 1 Posterolateral lumbar fusion rates with freehand pedicle screws have been shown to be as high as 85% with acceptable outcomes and excellent patient satisfaction.2,3 Safe and accurate screw placement is of significant importance, as the consequences of screw misplacement can result in a wide range of iatrogenic injuries, ranging from pedicle blow-out fractures to dural tears and permanent neurologic injury.4,5,6 In order to minimize the error of screw misplacement, navigated robotically assisted spine surgery systems have been designed to increase the accuracy of pedicle screw placement while simultaneously limiting the associated surgical footprint. 6 The proposed benefits of robotic surgery include reduced radiation exposure, soft tissue damage, patient lengths of stay, complication rates, and time in the operating room compared to traditional freehand pedicle screw placement.7-11
Conversely, adoption of new technologies is not without its associated costs. These costs include the obvious financial burden associated with acquiring the surgical platform, but also must take into account the costs to both patients and surgeons during the adoption phase. 10 A previous investigation noted a surgeon learning curve of approximately 30 cases for robotically assisted screw placement to avoid malposition when converting from freehand screw placement. 12 The adoption of any new technologies must justify the large buy-in and requires analysis into whether the increased accuracy and safety associated with robotic-assisted navigation translates to improved clinical outcomes for patients. Accordingly, the present study compares patient-reported outcomes, as well as complication and revision rates, for patients undergoing one-to three-level lumbar fusion using robotically assisted vs freehand pedicle screw placement.
Materials and Methods
Patient Selection and Demographic Data
Upon obtaining Institutional Review Board (IRB#19.508) approval, a retrospective cohort study was conducted on patients having undergone one-to three-level lumbar fusions at a single academic center between January 1, 2014 and August 31, 2020. Waiver was granted for patient informed consent as a minimal risk research study. Standardized Query Language (SQL) was used to identify patients over the age of 18 years who received one-to three-level lumbar fusion surgery regardless of lumbar fusion technique. Exclusion criteria included any patient who underwent decompression surgery without fusion, revision surgery, surgical intervention for an infectious, traumatic, or oncologic diagnosis, and patients with less than 1 year of follow-up. Cohorts were then grouped based upon the use of robotically assisted pedicle screw placement (robotic) or traditional freehand pedicle screw placement (freehand). Robots used for assisted pedicle screw placement included the Globus ExcelsiusGPS® robot (Audubon, PA) and Medtronic Mazor Robotics Renaissance® Guidance System (Minneapolis, MN). Robots were utilized by 1 of 4 fellowship trained spine surgeons ranging from 8 years to greater than 20 years of operative experience. Traditional freehand pedicle screw placement was performed by 1 of eleven fellowship trained spine surgeons ranging from 5 years to greater than 20 years of operative experience. Choice of pedicle screw instrumentation in the freehand group was at the discretion of the surgeon. Exposure and decortication of transverse processes with bone grafting was used to achieve fusion in both groups.
Matching
Patient demographics and surgical case characteristics (procedure type, revisions, and complications) were obtained via SQL search and manual chart review. Data obtained included age, sex, body mass index (BMI), and the number of levels fused. For all patients meeting the inclusion and exclusion criteria, patients who received freehand screw placement were matched 2:1 to those who received robotic screw placement using propensity score matching technique. This was done by a logistic regression model based on age, sex, and BMI to account for potential confounding covariates. Model diagnostics include evaluation of mean percent difference.
Patient-Reported Outcomes
Baseline and postoperative patient-reported outcome measures (PROMs) were gathered at 1 year (10.5–13.5 months) for each patient. Patient-reported outcome measures collected included Oswestry Disability Index (ODI), Physical Component and Mental Component Scores of the Short Form-12 Health Survey (PCS-12 and MCS-12, respectively), and Visual Analogue Scale Back (VAS Back) and Leg (VAS Leg) pain scores. Recovery ratios (RR) and the proportion of patients achieving the minimally clinically important difference (%MCID) were calculated to determine the extent to which patients benefitted from each surgical intervention (freehand vs robotic). Recovery Ratios was defined as ΔPROM/[(“Optimal” PROM—baseline PROM)], using a score of “0” as “optimal” for ODI,VAS Back, and VAS Leg, and a score of “100” as “optimal” for PCS-12 and MCS-12. 13 The %MCID was calculated based on the following MCID thresholds for meaningful improvement: ODI: 8.2, MCS-12: 10.1, PCS-12: 2.5, VAS Back: 2.2, VAS Leg: 5.0. 14
Statistical Analysis
Standard descriptive statistics including proportions, means, and 95% confidence intervals were reported for patient demographics and outcomes data. Differences in demographic characteristics were compared using Pearson chi-square (χ2) test or Fisher’s exact test for categorical variables, as appropriate. Sample means between the 2 groups were compared using a parametric independent-samples t-test or a nonparametric Mann–Whitney U test, as appropriate. Secondary analysis included multiple linear regression to determine whether demographic characteristics and procedure type (freehand vs robotic) were predictors of change in PROM scores. All radiographic measurements were conducted on Sectra Workstation IDS7 18.2 (Sectra AB; Linköping, Sweden). For all analyses, P-values less than .05 were considered statistically significant. All statistical analyses were performed using RStudio (Version 1.3.1073-1, RStudio, Inc., Boston, MA).
Results
Patient Demographics
Demographics of Cohort.
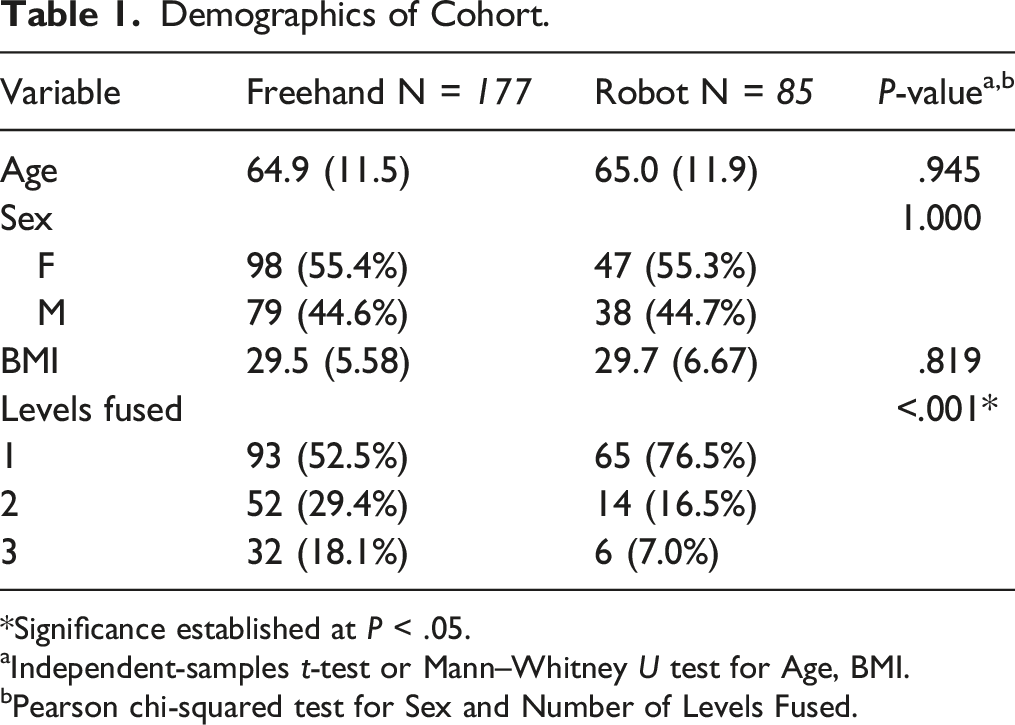
*Significance established at P < .05.
aIndependent-samples t-test or Mann–Whitney U test for Age, BMI.
bPearson chi-squared test for Sex and Number of Levels Fused.
Patient-Reported Outcomes
Patient-Reported Outcomes.
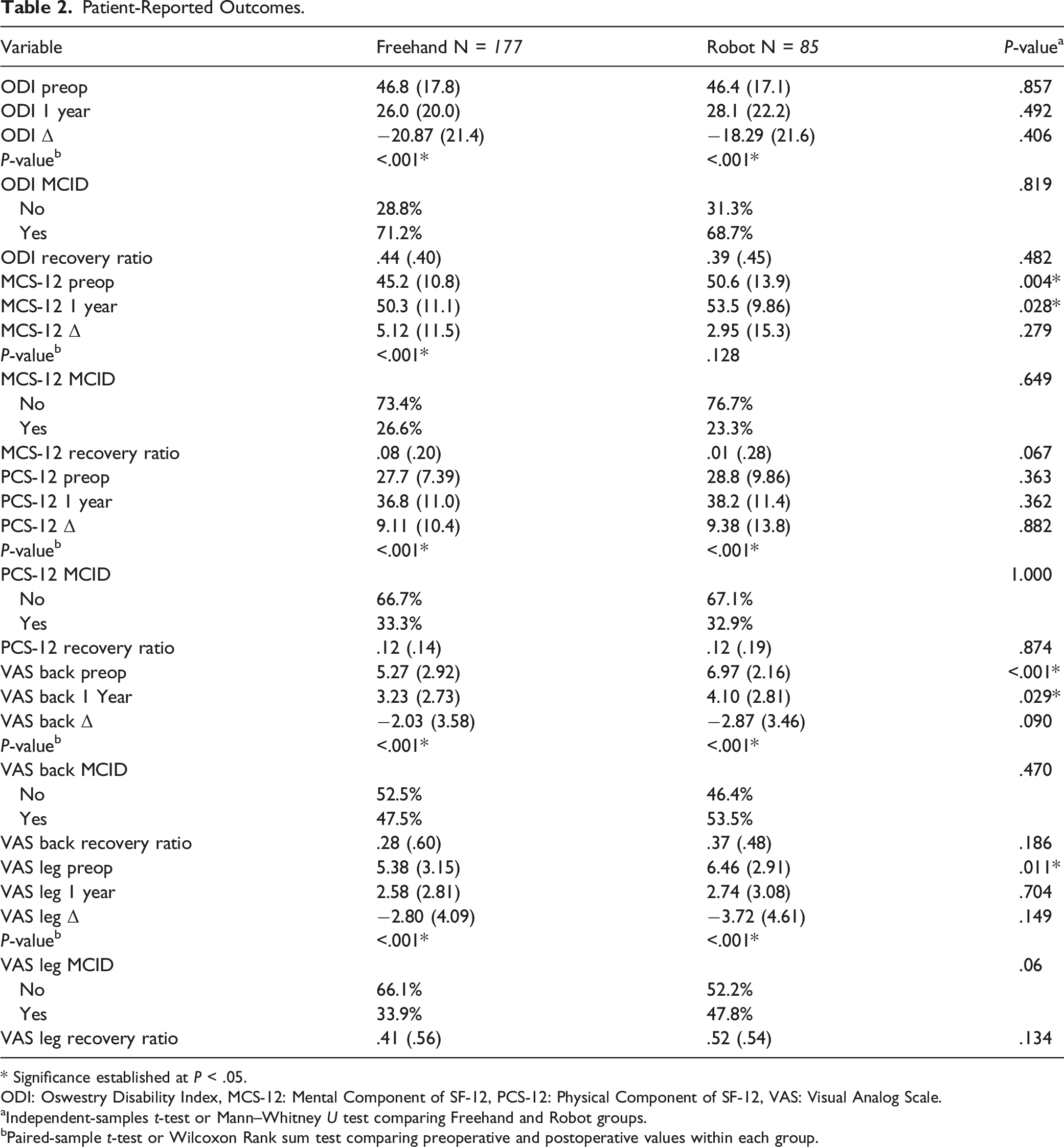
* Significance established at P < .05.
ODI: Oswestry Disability Index, MCS-12: Mental Component of SF-12, PCS-12: Physical Component of SF-12, VAS: Visual Analog Scale.
aIndependent-samples t-test or Mann–Whitney U test comparing Freehand and Robot groups.
bPaired-sample t-test or Wilcoxon Rank sum test comparing preoperative and postoperative values within each group.
Multiple Linear Regression of Procedure Type and Δ Patient Outcome Scores.
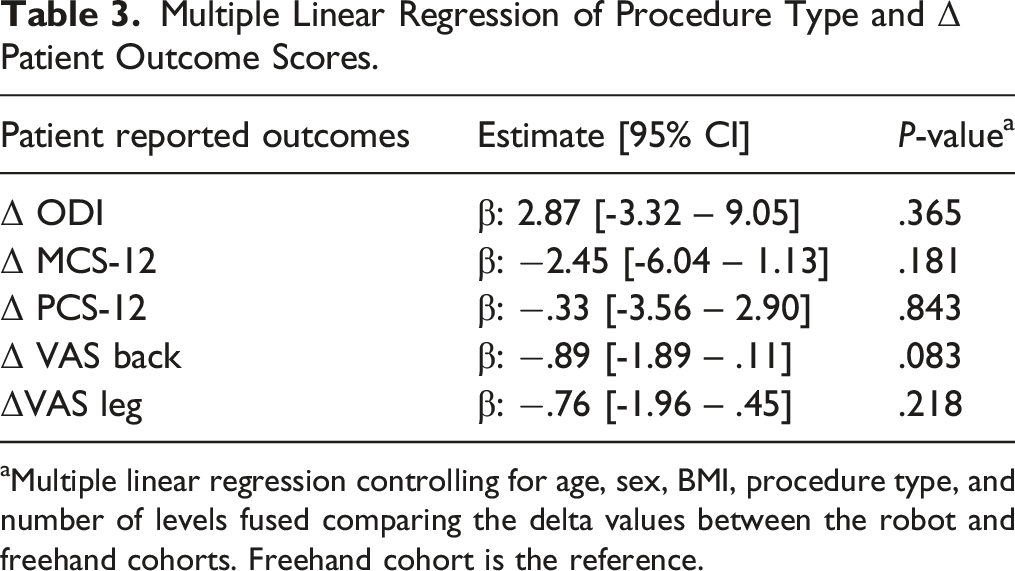
aMultiple linear regression controlling for age, sex, BMI, procedure type, and number of levels fused comparing the delta values between the robot and freehand cohorts. Freehand cohort is the reference.
Revisions and Complications
Complications and Revisions Within 1 year.
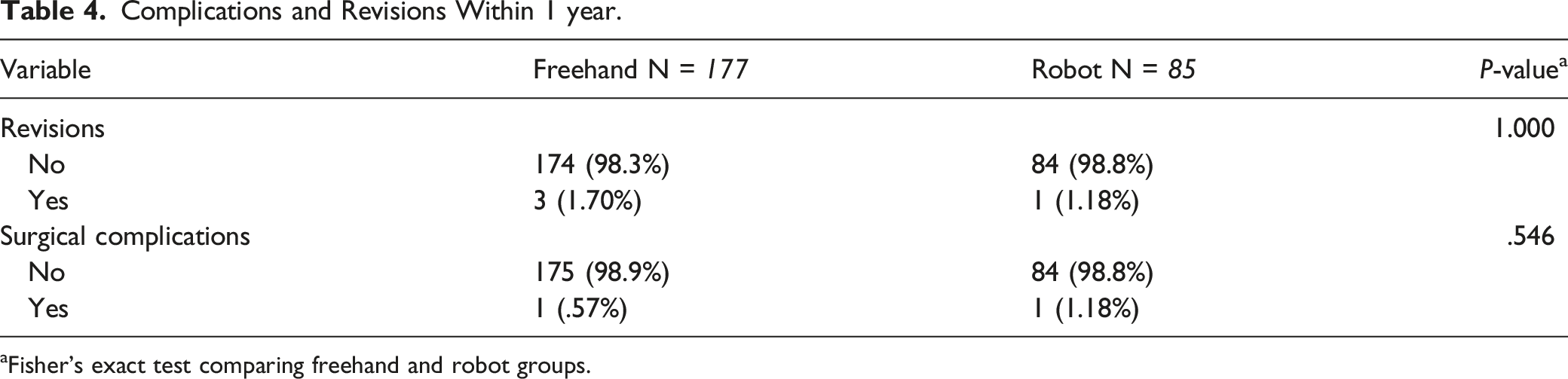
aFisher’s exact test comparing freehand and robot groups.
Discussion
The tolerance required to accurately place pedicle screws without breeching the pedicle wall allows for an error of approximately 1 mm of translation from the ideal starting point at the central pedicle axis and 5 degrees of angulation away from the central pedicle axis on average. 15 With such a low tolerance for error, emphasis has been placed on improving the techniques of screw placement to help increase accuracy. 1 With its ability to provide real-time intraoperative stereotactic guidance, some studies have indicated that robotically assisted pedicle screw placement results in increased accuracy while decreasing radiation exposure, complication rates, operative time, and recovery time.7-11,16,17 However, the adoption of any new technology requires high initial costs, both financial and temporal. It is prudent to justify the adoption of a robotic surgical platform as the associated costs are not amortized. It is unknown whether the advantages of robotically assisted surgery translate into clinically significant benefits for patients. Therefore, the aim of this study was to compare patient-reported outcomes for patients undergoing one-to three-level lumbar fusion using robotically assisted vs freehand screw placement.
Few studies have compared patient clinical outcomes after robotic vs freehand pedicle screw placement.17-20 In 2 published randomized controlled trials comparing radiographic and clinical outcomes of 37 patients undergoing robotic and 41 patients undergoing freehand screw placement in the setting of posterior lumbar interbody fusion (PLIF), no significant differences in clinical outcomes were found between groups at 1 and 2 years, respectively.20,21 Prior studies have shown equal rates of revisions and complications between robotically assisted and freehand pedicle screw insertion.8,18,22,23 Taken together, these findings suggest the touted benefits of robotically assisted pedicle screw fixation may not translate clinically for patients, corroborating the findings of our study. On both univariate and regression analysis, no difference was found for any clinical outcome measures between freehand vs robotically assisted pedicle screw insertion.
Studies have also compared robotic vs freehand surgery with regards to patient length of stay, estimated blood loss, and procedural duration. A randomized controlled trial of 60 patients receiving either robotic (n = 30) or freehand (n = 30) pedicle screw placement for lumbar fusion found patients receiving robotic surgery had a significantly shorter average length of stay (6.8 days vs 9.4 days, P = .020), 8 which has been attributed to the minimally invasive nature of robotic surgery. 24 Multiple studies, both prospective and retrospective, have demonstrated significant decreases in estimated blood loss when comparing robotic to freehand screw placement. 17 Despite these advantages, the clinical outcomes as reported by patients were no different between groups, underscoring the lack of clinical relevance of these often cited surgical outcome measures.
When evaluating surgical workflow, additional studies have shown that robotic screw placement is associated with decreased procedural time.11,25 Previous literature supports a learning curve for robotic surgery with regards to pedicle screw accuracy, but also underscores the need for surgical workflow optimization during the early adoption phase.26-31 Workflow optimization is often best accomplished by repetition of less complex surgeries including fewer levels of fusion, which may explain the difference in the number levels fused between groups found in our study. Additionally, preoperative computed tomography (CT) templating used with robotically assisted screw placement has been shown to decrease intraoperative X-ray exposure to the surgical team and staff. 32 However, it should be noted that with preoperative or intraoperative CT imaging for navigated pedicle screw placement, patients receive a greater mean radiation dose than those whose screws are placed freehand (1071 ± 447 mGy-cm vs 391 ± 53 mGy-cm). 33
As healthcare systems transition to value-based reimbursement, it is important to investigate outcomes affecting both the quality and cost of healthcare delivered. The current study found no significant differences in the improvement of patient-reported outcomes or rates of revision and complications between groups. However, one must also consider the value added from avoiding revision surgery for pedicle screw misplacement. Our results highlight the improved accuracy associated with robotically assisted pedicle screw placement, with 1 patient in the freehand group requiring revision for symptomatic inferior L5 pedicle screw breach.17,34,35 Given the low incidence of screw misplacement in our study (.56% of freehand patients) and the lack of significant difference in revision rates between groups, a larger analysis is required to further substantiate these findings. When examining the literature, previous studies demonstrate disparate similar results regarding complication and revision rates between robotic vs freehand pedicle screw placement.8,18,22,23 In a retrospective study of 520 lumbar fusion cases, no differences were observed in the rate of postoperative complications between robotically assisted vs freehand pedicle screw placement. 23 These results have been corroborated by multiple randomized controlled trials for lumbar fusion, which demonstrate no differences in rates of complications or revisions between patients in the robotic arm vs the freehand arm.8,18 Altogether, the results suggest that patient outcomes after surgery are unlikely to be dependent on the technique used for placement of screws, but are more importantly associated with the success of the fusion performed.
The financial costs of adopting a robotically assisted navigation platform are worth noting. The total price of the Globus ExcelsiusGPS® robot (Audubon, PA), 1 of the robots used to perform the lumbar fusion in this study, is approximately $1.5 million (at the time of this study) when including the robotic base, arm, and end effector necessary to perform surgery. 36 Another platform, the Medtronic Mazor X Stealth Robot® (Minneapolis, MN), can be acquired without charge if the surgeon uses Medtronic pedicle screws. Given the results of this study, this option may be reasonable for an adaptable spine surgeon, as there is no current evidence to suggest that utilizing a single company’s pedicle screw over another will influence patient outcomes. Further cost-effective analyses are warranted to investigate if adoption is fiscally responsible.
This study is not without limitations. Its retrospective study design is inherently subject to selection and indication biases. The number of fusion levels was restricted to 3 levels in this study, limiting the study population and subjecting the study to type II errors. However, previous studies have demonstrated that the number of levels in reconstructive lumbar surgery may not significantly impact overall clinical outcomes.37,38 Further research partitioning results based on fusion type and technique (i.e., anterior lumbar interbody fusion (ALIF) or transforaminal lumbar interbody fusion (TLIF) utilizing robotic-assisted pedicle screw placement compared to traditional freehand technique) should be performed to understand if procedure type in combination with robotic-assisted navigation has a differential effect on outcomes. Finally, this study is limited to patient outcomes at 1 year of follow-up. Future studies should investigate the outcomes of robotic spine surgery with longer patient follow-up.
Conclusion
Robotically assisted pedicle screw placement has been reported to increase the accuracy of pedicle screw placement and decrease complication rates, operative time, and recovery time when compared to conventional freehand surgery. However, the present study suggests that these benefits may not translate to meaningful clinical improvements for patients. No significant differences were found between robotic and freehand pedicle screw placement with regards to patient-reported outcomes, surgical complications, or revision rates in a large cohort of matched patients undergoing one-to three-level lumbar fusion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Board Review Statement
This study was approved by the Institutional Review Board at the Thomas Jefferson University Hospital. Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.