
Abstract
Study Design:
Cadaveric study.
Objective:
To evaluate accuracy, radiation exposure, and surgical time of a new robotic-assisted navigation (RAN) platform compared with freehand techniques in conventional open and percutaneous procedures.
Methods:
Ten board-certified surgeons inserted 16 pedicle screws at T10–L5 (n = 40 per technique) in 10 human cadaveric torsos. Pedicle screws were inserted with (1) conventional MIS technique (L2–L5, patient left pedicles), (2) MIS RAN (L2–L5, patient right pedicles), (3) conventional open technique (T10–L1, patient left pedicles), and (4) open RAN (T10–L1, patient right pedicles). Output included (1) operative time, (2) number of fluoroscopic images, and (3) screw accuracy.
Results:
In the MIS group, compared with the freehand technique, RAN allowed for use of larger screws (diameter: 6.6 ± 0.6 mm vs 6.3 ± 0.5 mm; length: 50.3 ± 4.1 mm vs 46.9 ± 3.5 mm), decreased the number of breaches >2 mm (0 vs 7), fewer fluoroscopic images (0 ± 0 vs 108.3 ± 30.9), and surgical procedure time per screw (3.6 ± 0.4 minutes vs 7.6 ± 2.0 minutes) (all P < .05). Similarly, in the open group, RAN allowed for use of longer screws (46.1 ± 4.1 mm vs 44.0 ± 3.8 mm), decreased the number of breaches >2 mm (0 vs 13), fewer fluoroscopic images (0 ± 0 vs 24.1 ± 25.8) (all P < .05), but increased total surgical procedure time (41.4 ± 8.8 minutes vs 24.7 ± 7.0 minutes, P = .000) while maintaining screw insertion time (3.31.4 minutes vs 3.1 ± 1.0 minutes, P = .650).
Conclusion:
RAN significantly improved accuracy and decreased radiation exposure in comparison to freehand techniques in both conventional open and percutaneous surgical procedures in cadavers. RAN significantly increased setup time compared with both conventional procedures.
Introduction
Surgical techniques have evolved from open surgery to minimally invasive surgery (MIS), in an effort to decrease surgical site exposure, reduce blood loss and complications, and shorten recovery time and hospital stay. 1,2 Advancements in computer-aided navigation (CAN) and robotic technologies have the potential to improve accuracy of screw placement in comparison to freehand methods 3 and to reduce excessive radiation exposure resulting from repetitive intraoperative fluoroscopy. 4 -7 Robot-assisted navigation (RAN) platforms (SpineAssist/Renaissance/Mazor X, Mazor Robotics Ltd, Caesarea, Israel; ROSA, Medtech SA, Montpellier, France; and ExcelsiusGPS, Globus Medical, Inc, Audubon, PA) use 3-dimensional (3D), real-time patient data mapped via computed tomography (CT) registration, which is displayed on a monitor, allowing for the intraoperative navigation of surgical instruments using a camera system. As a result, the location of instruments and implants relative to the patient is known.
In the present study, researchers examined a novel, freestanding RAN platform with a floor-fixable base, rigid robotic arm, and software for preoperative planning, allowing for active RAN and passive freehand navigation of pedicle screw insertion (ExcelsiusGPS, Globus Medical, Inc; Figure 1). The robotic arm aligns with the desired trajectory and allows for visualization of patient anatomy, instruments, and implants. Unlike CAN platforms that only provide a 3D map of bony anatomy and instruments, the software allows for comprehensive screw planning (Figure 2). Once desired trajectories are planned using the software, the robotic arm is activated by the user and moves to that location based on real-time tracking of percutaneously placed reference markers affixed to the patient’s bony anatomy. The distal end of the robotic arm incorporates a guide tube to interface with navigated instruments, which have reflective markers to allow real-time tracking similar to freehand navigation.
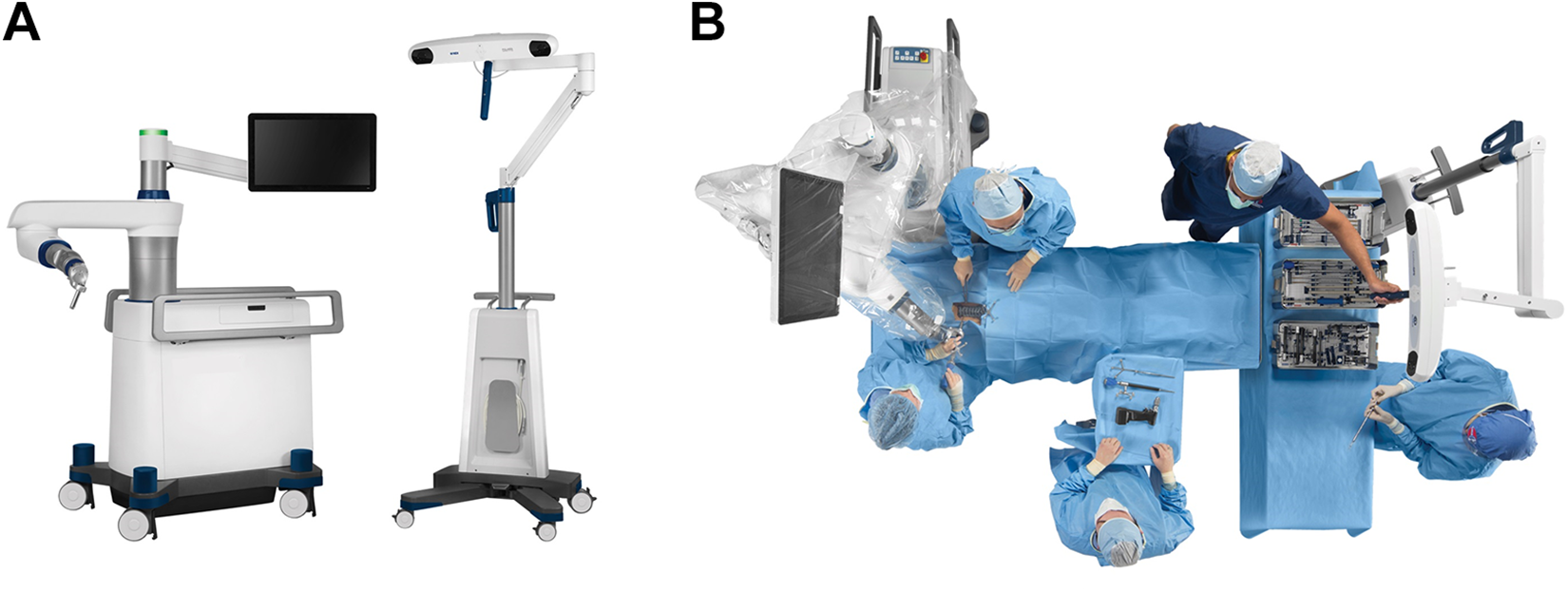
Representative photographs of (A) novel, freestanding RAN platform (ExcelsiusGPS, Globus Medical, Inc) with a floor-fixable base, rigid robotic arm, and navigation camera, and (B) simulated operating theater layout used in the present study.
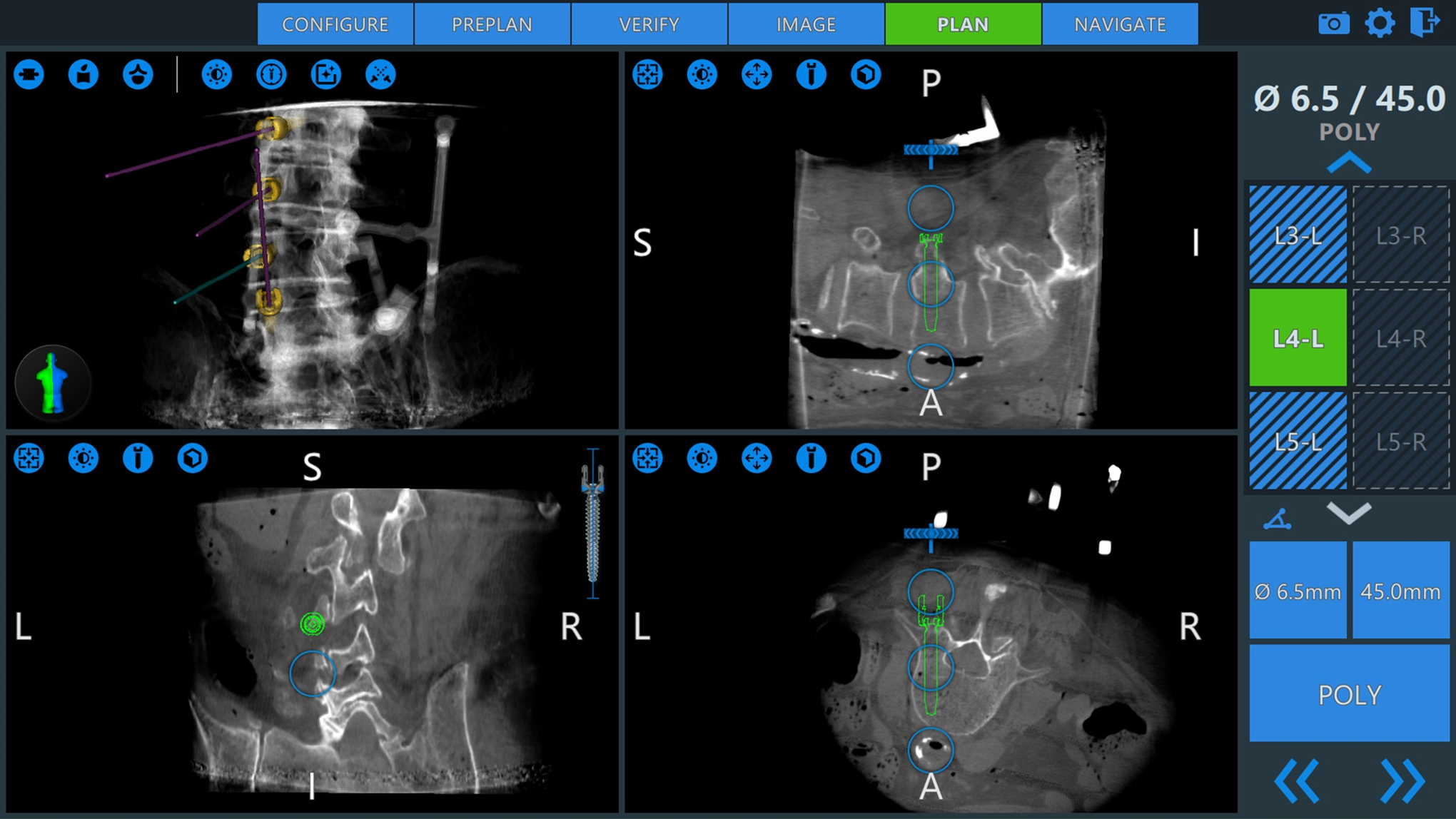
Representative screenshot of the preoperative planning step displaying the proposed diameter, length, and orientation of unilateral pedicle screws in the sagittal, axial, coronal, and a synthetic 3D rendering. L and R indicate anatomic left and right, respectively; S, superior; I, inferior; A, anterior; P, posterior.
To the authors’ knowledge, there are limited comparative studies on conventional and RAN procedures. Furthermore, inherent differences between RAN systems, such as (1) the use of K-wires; (2) bed-mounted, spinous process mounted, or floor-fixable frames; or (3) use of preoperative CT, intraoperative CT, or intraoperative fluoroscopy, necessitate the validation of each RAN platform. As such, the present study investigates pedicle screw accuracy, radiation exposure, and simulated operative times of conventional open and MIS techniques, as well as open and MIS techniques using a RAN platform in a cadaveric setting.
Methods
Specimen Preparation
Ten unembalmed human torsos were used in this investigation (age: 64.4 ± 8.0 years; sex: 9 males, 1 female). Specimens were selected based on radiography to exclude specimens with spinal trauma, malignancy, or fractures. All specimens were stored at −20°C until testing.
Surgical Reconstruction
Ten orthopedic or neurologic surgeons (n = 5 each) were selected for the study. Surgeons possessed a variety of clinical experience ranging between 2 and 23 years (7.1 ± 6.1 years). Robotic or navigation experience varied (55.8 ± 35.5 cases total) and primarily included use of either SpineAssist/Renaissance (Mazor Robotics Ltd) or StealthStation (Medtronic, Minneapolis, MN). Each surgeon performed 4 experimental procedures that required insertion of 16 pedicle screws (n = 4 per procedure). CREO MIS and CREO AMP Threaded screw systems were used (Globus Medical, Inc). All clinicians were instructed to follow the Weinstein trajectory when placing each screw, 8 parallel to the superior endplate, and occupying approximately 60% to 75% of the vertebral body in the sagittal plane. Treatment groups included MIS lumbar surgery (conventional fluoroscopic and RAN) and open thoracolumbar surgery (conventional and RAN; Table 1).
Procedural Steps for Technique Treatment Groups Included in the Time Measurement.
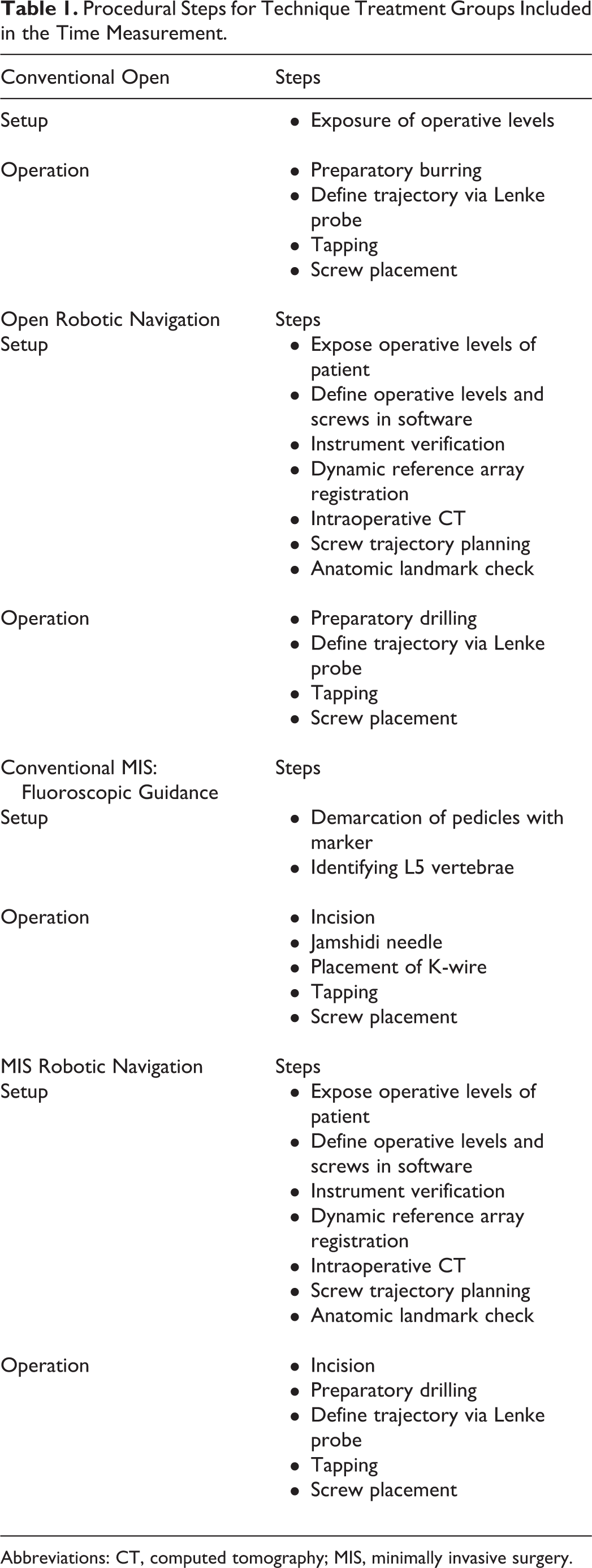
Abbreviations: CT, computed tomography; MIS, minimally invasive surgery.
The conventional open technique began with a superficial incision and exposure of the posterior elements; preparatory burring was used to penetrate the cortical bone (Table 1). A Lenke probe was used to define a trajectory. While preoperative CT of the specimen was not provided, fluoroscopy was available for trajectory planning and screw size selection. A ball-tipped probe or “pedicle sounder” was available to verify the trajectory. For the conventional MIS technique, procedural steps included the use of fluoroscopy to demarcate the pedicles, incise superficial tissue, and define the screw trajectories with Jamshidi needles and K-wires (Table 1); only one surgeon used biplanar fluoroscopy. Preoperative planning and screw size selection was determined with fluoroscopy and measurements from the K-wire.
The investigated RAN system (ExcelsiusGPS, Globus Medical, Inc) included a frameless, floor-mounted base (with attached monitor) and navigation camera system (Figure 1). The RAN system is compatible with preoperative CT, intraoperative CT (as used in the study), or 2D fluoroscopy workflows. The navigation camera tracks patient movement (including breathing or acts executed by the surgeon) with the help of a patient reference array (PRA). The PRA was affixed to the iliac crest with a 4-pronged post, although it is also possible to secure to the spinous process with a clamp; a surveillance marker was affixed to the contralateral iliac crest to monitor potential movement of the PRA. Intraoperative CT was performed (slice thickness of 0.833) 9 (O-Arm, Medtronic, Minneapolis, MN) while a registration pattern (dynamic reference base [DRB]) was affixed to the PRA and was carefully removed following the CT scan; registration of the bony anatomy is possible by tracking the position of the DRB and PRA with the navigation camera. Following registration and screw planning, the robotic arm positioned itself (once activated by the surgeon) in line with a planned trajectory and a custom scalpel was inserted in the guide tube to release the posterior tissue. The fiducial markers and integrated instruments/implants provide a K-wireless approach for direct real-time visualization of all instruments and navigated screw placement through the rigid robotic arm.
Before using RAN, surgeons were briefed on the platform, preoperative planning software, and instruments for approximately 30 minutes by a clinical specialist on the day of the study. No surgeon had prior experience using this RAN. The surgical setup for robotic navigation required more steps than conventional surgery (Table 1), including mounting a PRA, conducting an intraoperative CT scan, and screw trajectory planning. Following percutaneous PRA and surveillance marker insertion, all staff exited the room during intraoperative CT. Surgeons then planned the trajectories at the desired slice (ie, vertebral level) and adjusted the screw diameter and length as they deemed appropriate. Following planning of the screws, the surgeon would confirm placement in the sagittal, coronal, and axial planes, and in the volumetric rending of the spine and screw on the monitor (Figure 2). Last, the surgeons inserted all screws, with the real-time instrument/implant trajectory displayed on the specimen images along with the planned screw allowing the user to confirm the desired trajectory and insertion of the screw to the desired depth.
Measurement Endpoints
Experimental Operative Time
Data was collected separately for platform setup times and operative times. Operative steps uniformly involved the insertion of a drill followed by a Lenke probe, tap, and driver. The exact workflow for each procedure is described in Table 2.
Detailed Summary of Major (Grade ≥C) Pedicle Breaches.
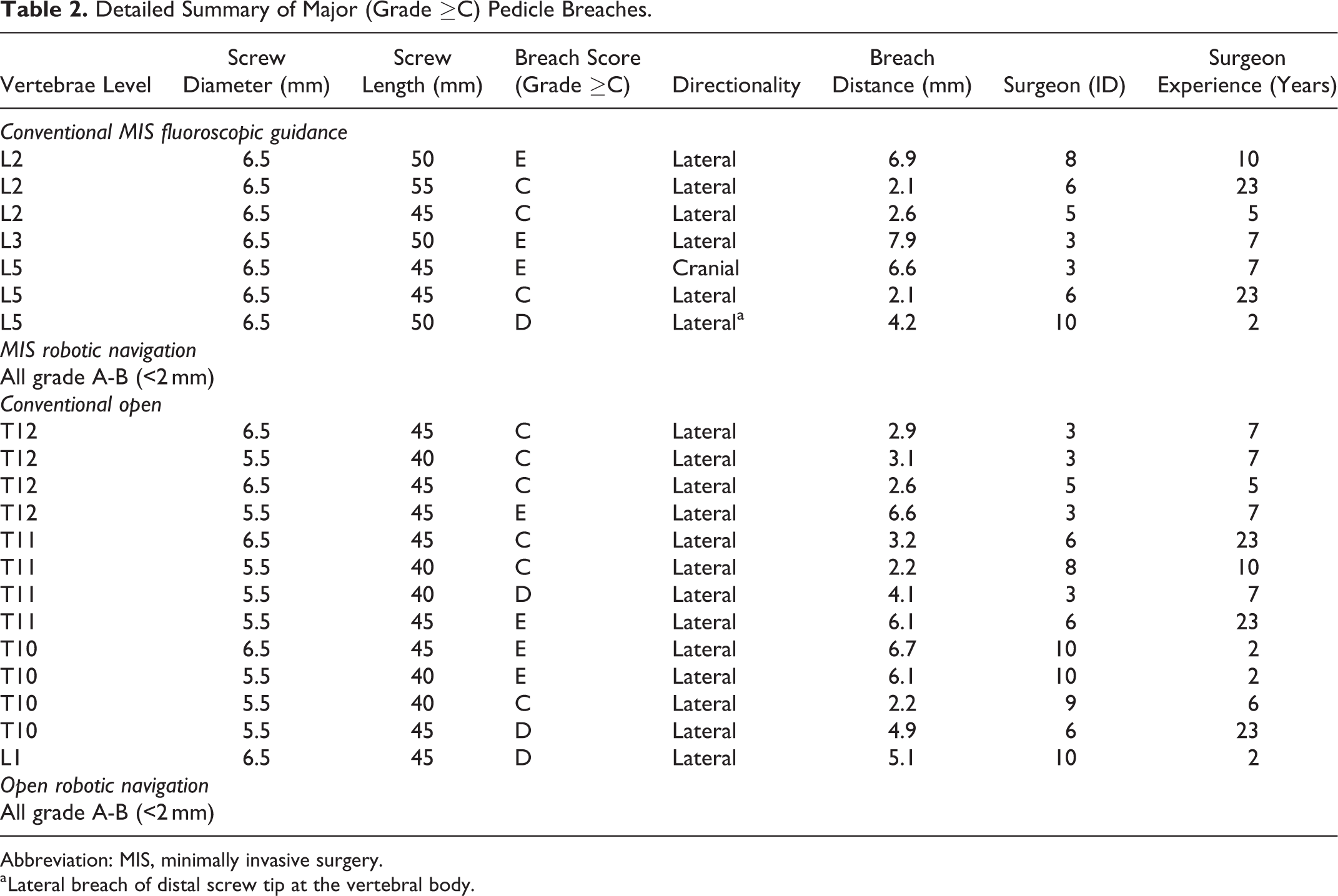
Abbreviation: MIS, minimally invasive surgery.
a Lateral breach of distal screw tip at the vertebral body.
Pedicle Screw Accuracy
Following screw placement, operative levels were disarticulated. Lateral and axial images of disarticulated vertebrae were taken. Radiographic films were reviewed and used for breach measurements, and were graded A to E according to a Gertzbein and Robbins 10 classification system: Grade A, in the pedicle; Grade B, perforation <2 mm; Grade C, ≥2 mm but <4 mm; Grade D, perforations ≥4 mm but <6 mm; and Grade E, perforations ≥6 mm. Breaches classified as Grade B (<2 mm) were considered minor, based on safety criterion outlined by Kim et al. 11 The direction of cortical violation was also recorded.
Accuracy of the RAN screw placement was compared with the screw plan for both RAN treatment groups. Each screw’s planned position, trajectory, length, and diameter was exported in the coordinate system of the initial intraoperative CT. The planned trajectory and CT were then superimposed with the postoperative CT using custom software. Intraoperative and postoperative CT scans were aligned manually until the bony edges matched in 3 orthogonal slice views. The differences encountered with the preplanned screw were measured relative to screws in the postoperative CT using a custom software. Linear differences were measured in the medial-lateral, cranial-caudal, and anterior-posterior distances of the screw tip and head (mm), while angular differences were measured in medial-lateral and cranial-caudal angles (°). Examples of custom software interface are displayed in Figure 3.
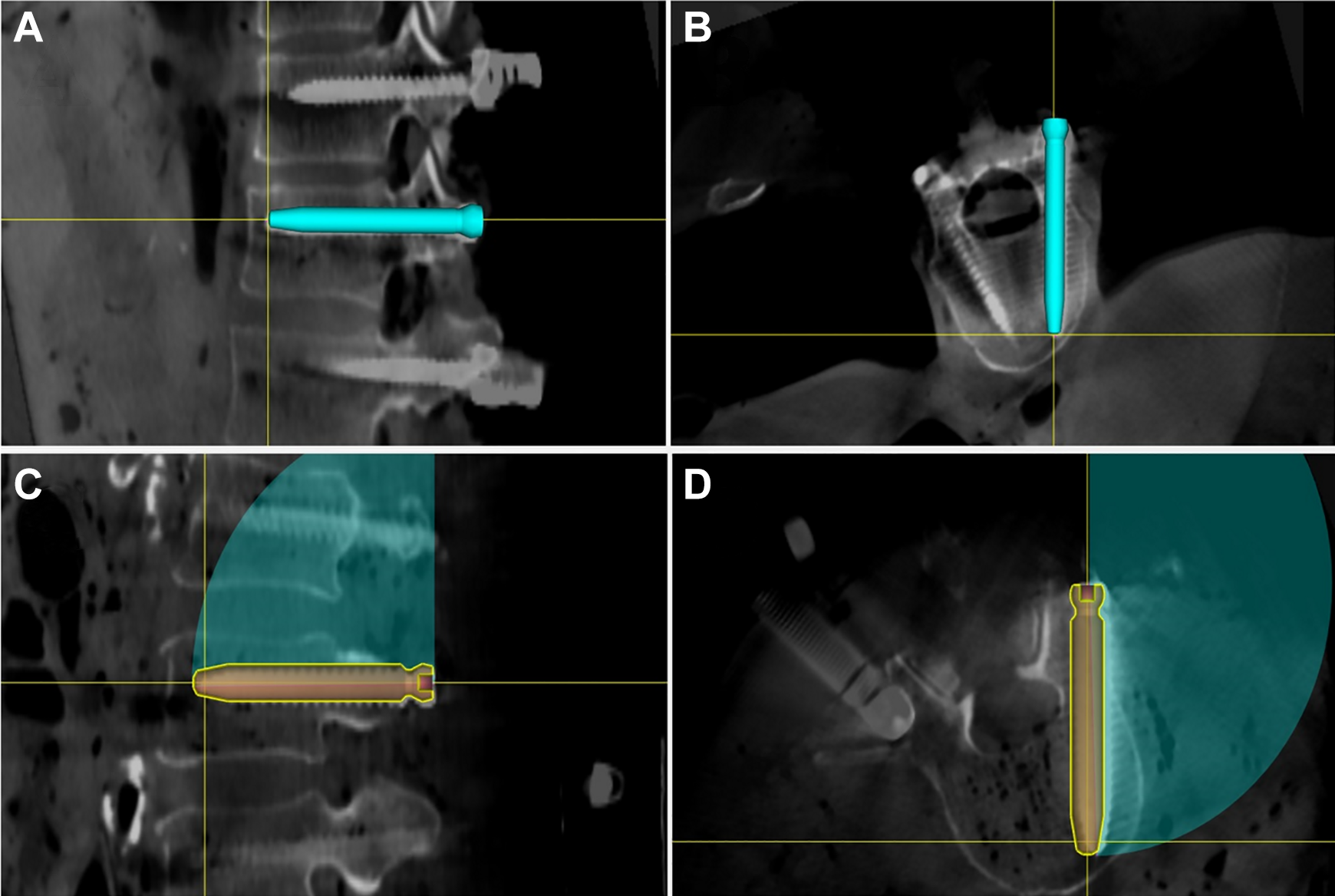
Intraoperative CT with screw CAD trajectory superimposed on the postoperative CT using custom software. The top images (A, B) display the T12 tip in comparison to the actual screw tip, while the bottom images (C, D) display the screw angulation of the planned trajectory in comparison to the placed screw.
Fluoroscopy
The number of fluoroscopic images required for each operative technique was recorded as a proxy for the radiation exposure to the surgeon, and did not include intraoperative CT (surgeon stepped out of the lab).
Statistical Analysis
Statistical analysis was performed using IBM SPSS Statistics software (SPSS v22, IBM Corp, Armonk, NY). Direct group comparisons included (1) MIS conventional fluoro-guided versus MIS RAN techniques in the lumbar spine (L2-L5) and (2) conventional open fluoro-guided versus open RAN techniques in the thoracolumbar spine (T10-L1). Comparisons of results for screws placed used in the lumbar versus thoracolumbar regions were not performed due to pedicle morphological differences—specifically isthmus size 12 —that has been shown to affect breach rates 13 between the thoracic and lumbar spine. Independent t tests were performed on all continuous data sets to assess the differences in operation times, fluoroscopic images captured, and screw dimensions between the test groups. A Wilcoxon rank-sum test was used to assess differences in breach classification, the ordinal data set qualifying screw trajectory accuracy. Statistical significance was defined as P < .05.
Results
Experimental Operative Time
A summary of experimental operative time with significant relationships between pedicle screw insertion using the RAN versus conventional open and MIS freehand techniques is presented in Figure 4A-C and Table 4. Conventional MIS required 36.0 ± 7.0 minutes (setup, 5.7 ± 4.2 minutes; insertion of screws, 30.3 ± 8.1 minutes), averaging 7.6 ± 2.0 minutes per screw when excluding setup time. Alternatively, MIS with RAN required 32.6 ± 3.5 minutes (setup, 18.4 ± 3.5 minutes; insertion of screws, 14.3 ± 1.4 minutes), averaging 3.6 ± 0.4 minutes per screw when excluding setup time. Use of RAN significantly increased the setup time required for the MIS technique (P < .001). Per screw, the use of RAN significantly decreased the duration of screw insertion (P < .001). Overall surgical time was not significantly different between procedures (P = .196).
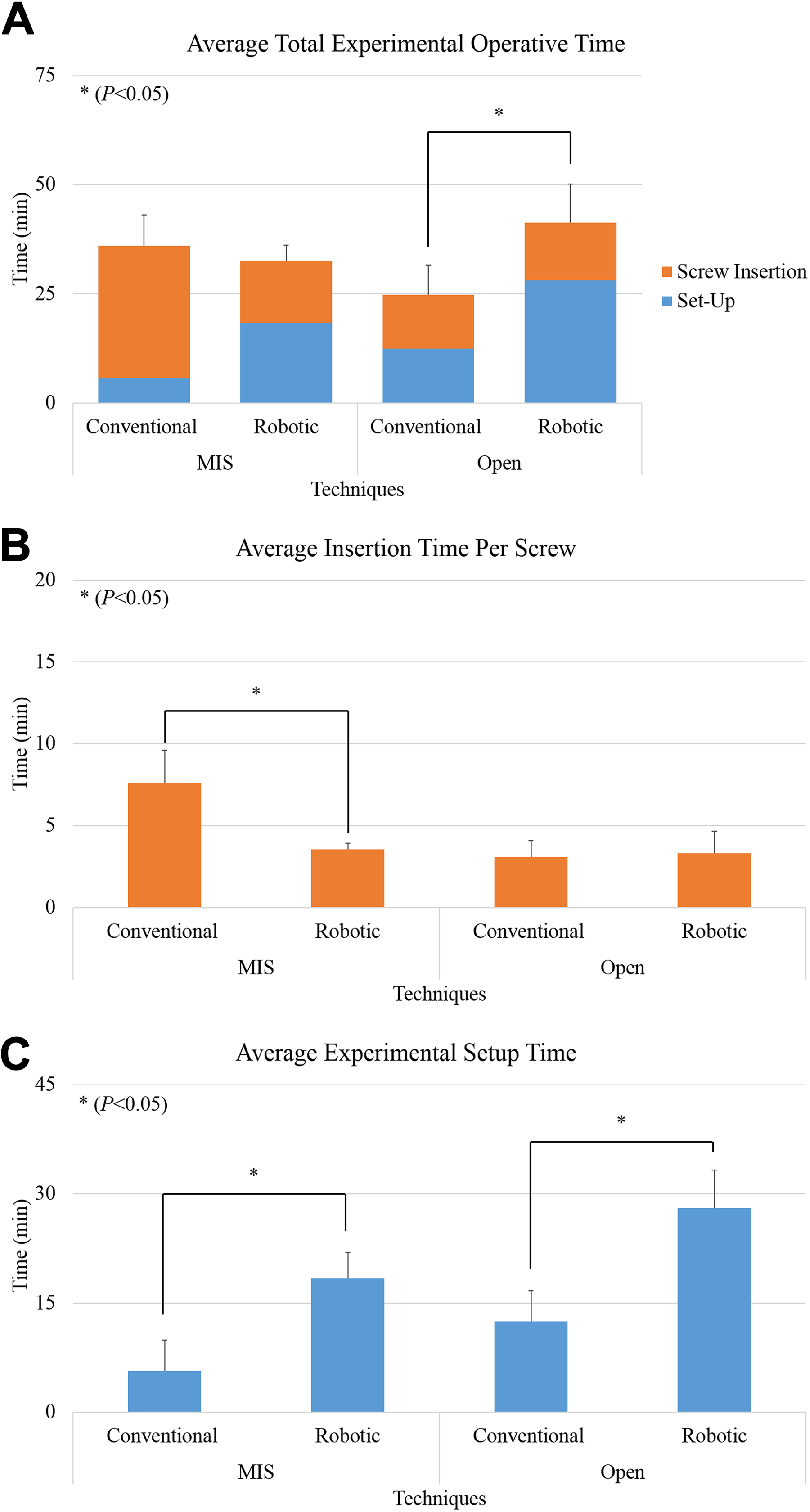
(A) Average time to perform experimental operation, (B) average time per screw insertion, and (C) average setup time.
Robotic Navigation Group Planned Versus Screw Placement Accuracy.
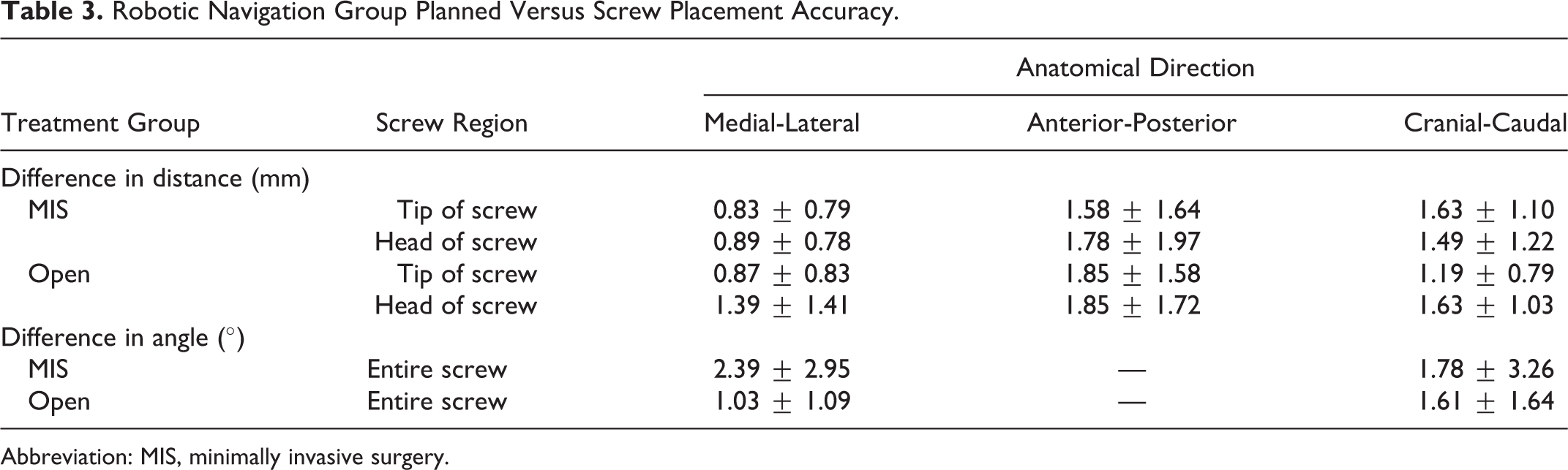
Abbreviation: MIS, minimally invasive surgery.
Surgical Technique Results Comparisons.
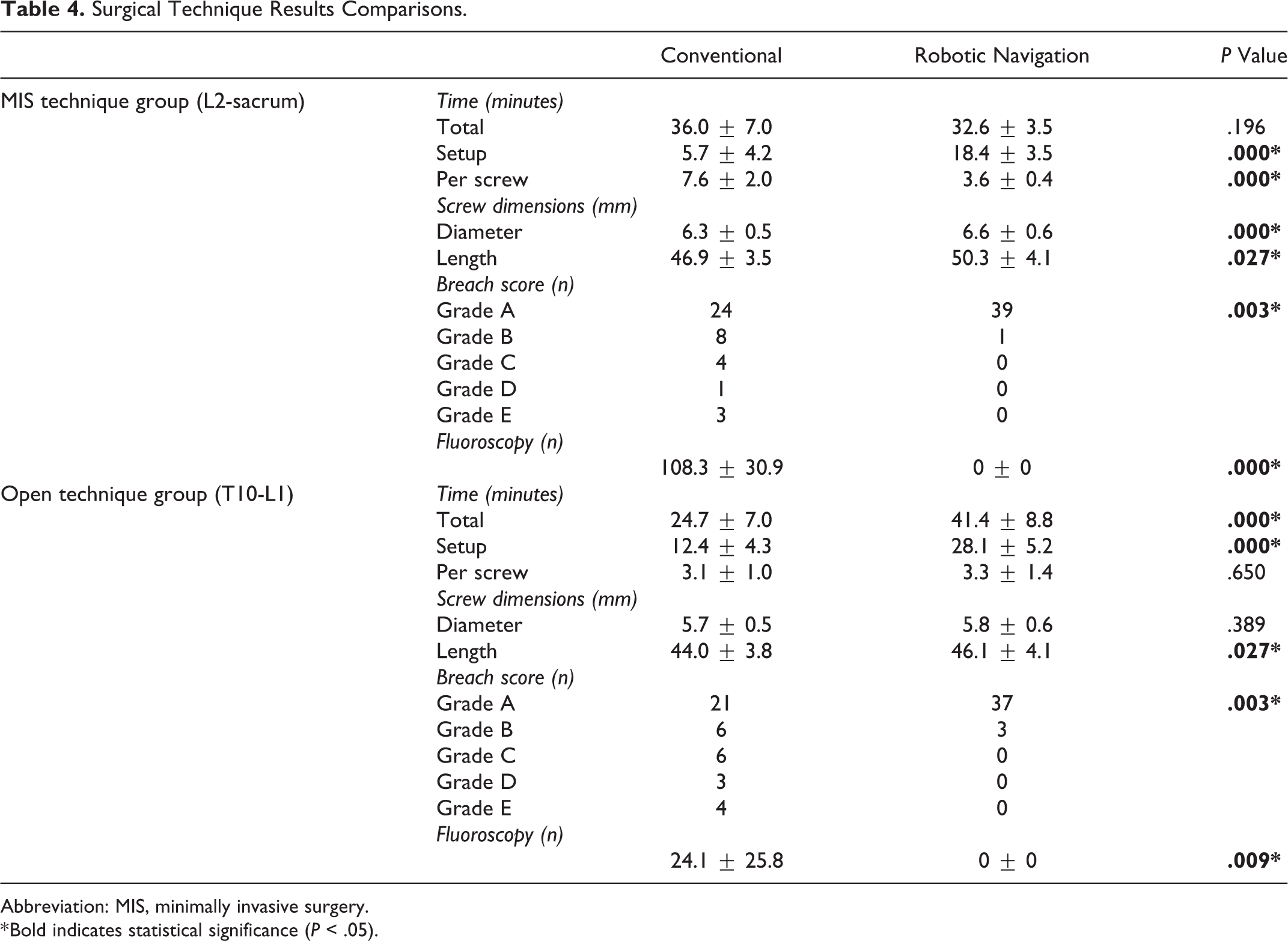
Abbreviation: MIS, minimally invasive surgery.
* Bold indicates statistical significance (P < .05).
The conventional open technique required 24.7 ± 7.0 minutes (setup, 12.4 ± 4.3 minutes; insertion of screws, 12.3 ± 4.1 minutes), averaging 3.1 ± 1.0 minutes per screw when excluding setup time. Alternatively, the open technique with RAN required 41.4 ± 8.8 minutes (setup, 28.1 ± 5.2 minutes; insertion of screws, 13.3 ± 5.4 minutes), averaging 3.3 ± 1.4 minutes per screw when excluding setup time. Setup of the RAN platform was 2.3 times longer than the conventional open technique (P < .001), significantly increasing total experimental operative time (P < .001); no significant differences were observed between insertion times per screw (P = .650).
Pedicle Screw Accuracy
A summary of breach rates (percentage; Figure 5), a summary of observed breaches (Table 3), and absolute numbers of breaches for MIS and open techniques (Table 4) are presented. The conventional MIS technique resulted in 24 screws (60%) placed in the pedicle; 8 screws (20%) resulted in a minor breach (Grades B). Major breaches of Grade C (4 screws, 10%), Grade D (1 screw, 2.5%), and Grade E (3 screws, 7.5%) were observed. Alternatively, the MIS RAN technique resulted in 39 screws (97.5%) placed in the pedicle, with 1 screw (2.5%) resulting in a minor breach. In the open procedures, the conventional technique resulted in 21 screws (52.5%) placed in the pedicle; 6 screws (15%) resulted in a minor breach (Grade B). Major breaches of Grade C (6 screws, 15%), Grade D (3 screws, 7.5%), and Grade E (4 screws, 10%) were observed. Alternatively, the MIS RAN technique resulted in 37 screws (92.5%) placed in the pedicle, with 3 screws (7.5%) resulting in a minor breach. Regardless of MIS or Open procedures, RAN significantly reduces the number of pedicle breaches compared with conventional techniques (both P = .003). Significant differences in screw lengths (44.0 ± 3.8 mm vs 46.1 ± 4.1 mm, P = .027) were observed between conventional and RAN open techniques, but not differences in screw diameter (5.7 ± 0.5 mm vs 5.8 ± 0.6 mm, P = .389).
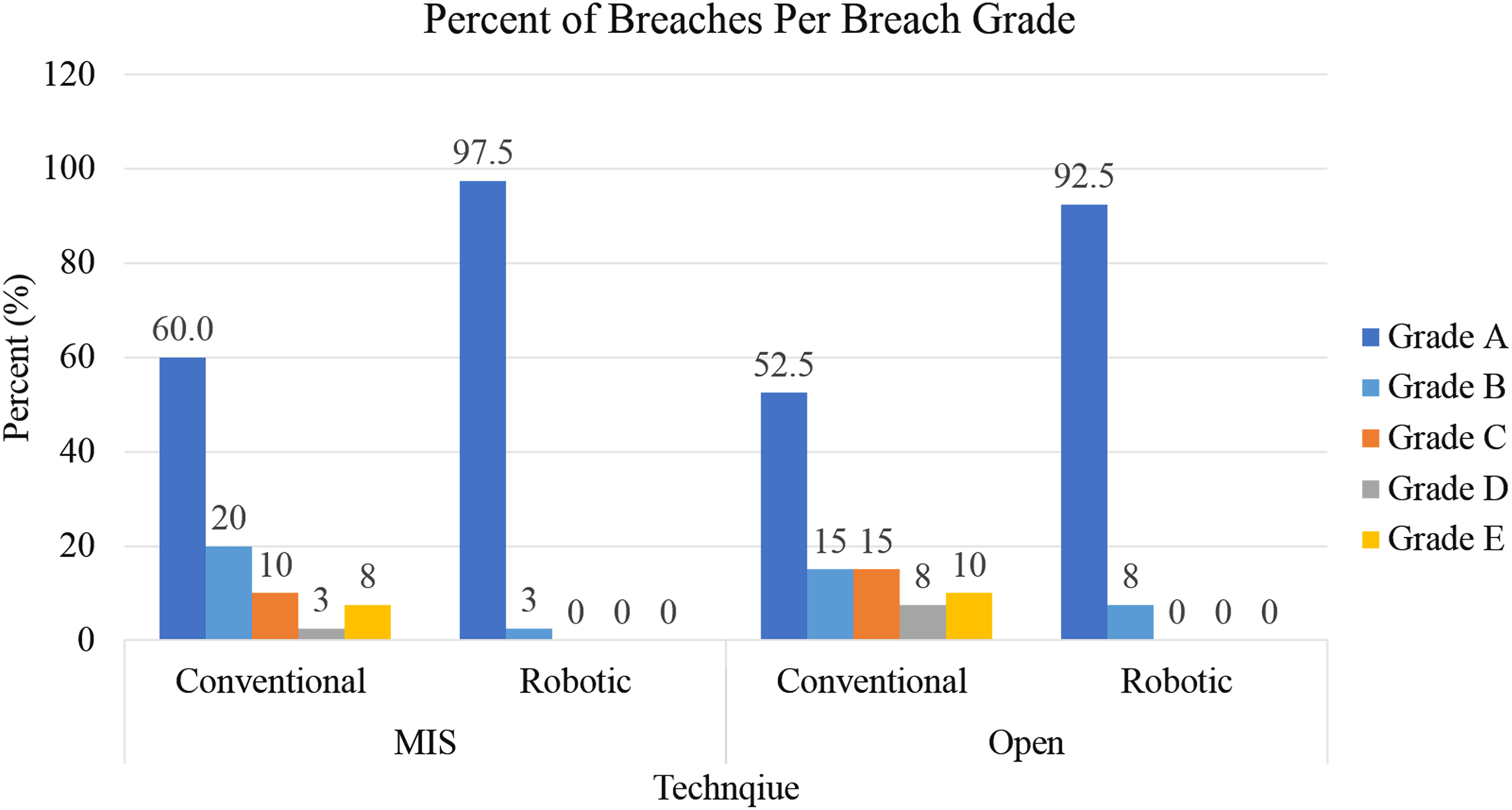
Rate of pedicle breach per breach grade. Grade A, in the pedicle; Grade B, perforation <2 mm; Grade C, ≥2 mm but <4 mm; Grade D, perforations ≥4 mm but <6 mm; and Grade E, perforations ≥6 mm.
Robotic Planning Versus Screw Placement Accuracy
A summary of the average displacement (mm) and angular (°) differences is presented for the MIS and open RAN treatment groups (Table 3).
Fluoroscopy
The experimental insertion using a conventional MIS technique exposed the surgeon to an average of 108.3 ± 30.9 fluoroscopic images, while the conventional open technique required 24.1 ± 25.8 fluoroscopic images. RAN, regardless of the technique, exposed the surgeon to zero fluoroscopic images through the duration of the experimental procedure (P < .001 and P = .009), compared with conventional MIS and open techniques, respectively.
Discussion
Pedicle screw and rod fixation is the gold standard for spinal fusion. 14 A systematic review by Gelalis et al 15 reported pedicle screw misplacement rates of 0.1% to 31% using the freehand technique, 15% to 72% with the aid of fluoroscopy, 0% to 11% using CT navigation, and 8% to 19% using fluoroscopy-based navigation. Iatrogenic damage of neurological structures and reduced biomechanical fixation manifesting as failed hardware are two consequences of screw malposition. 16,17 The present study investigated a novel RAN platform, and a summary of time, radiation exposure, and accuracy comparisons to conventional MIS and open techniques is presented (Table 4).
The investigated RAN system significantly increased setup time compared with conventional MIS due to draping, instrument verification, anatomy registration, and screw trajectory planning (18.4 ± 3.5 vs 5.7 ± 4.2 minutes), but significantly reduced time per screw (3.6 ± 0.4 vs 7.6 ± 2.0 minutes); overall, total procedure time was slightly less for the RAN procedure (32.6 ± 3.5 vs 36.0 ± 7.0 minutes). Use of RAN during an open procedure significantly increased setup time compared with the conventional technique, as the conventional method only required exposure of the posterior elements (28.1 ± 5.2 vs 12.4 ± 4.3 minutes); time per screw was time neutral between the RAN and non-RAN techniques (3.3 ± 1.4 vs 3.1 ± 1.0 minutes); thus, the total procedure time was significantly higher for the RAN procedure (41.8 ± 8.8 vs 24.7 ± 7.0 minutes).
Direct comparison to clinical investigations is difficult due to inconsistencies between the open and MIS techniques used (which may include additional decompression); conflicting average operative times are reported in the literature. Hyun et al 4 report identical operative times between RAN and open freehand techniques (208.5 minutes each). Kantelhardt et al 5 found that the use of RAN moderately increased operative time in comparison to freehand (65.2 vs 52.9 minutes per screw, P > .05); statistical equivalence was also reported by Solomiichuk et al 18 (264 vs 226 minutes, P > .05). Alternatively, Ringel et al 19 found that RAN significantly increased surgical time in comparison to a conventional open technique (95 vs 84 minutes); preoperative planning required an additional 24 minutes. Similarly, Lonjon et al 6 report a significant increase in total time in comparison to freehand (209 vs 336 minutes). Near significant differences between screw insertion speed across repeated use of RAN suggest some learning curve with the technology. 20
Breaches were also quantified (Grades A-E) in accordance with the literature. 4,6,18,19,21 -27 Screw malposition as described by Kim et al 11 found deviations of 0 to 2 mm to be clinically insignificant; 2 to 4 mm, probably safe; and greater than 4 mm, questionably safe. In the present study, conventional MIS and open techniques resulted in an overall breach rate (>2 mm) of 20% and 32.5%, respectively, within the ranges reported by Gelalis et al 15 ; 19 of 20 breaches occurred laterally, a trend in agreement with reported literature. 3,15
Rates of major breaches (>2 mm) varied between 0% to 7.6% and 0% to 15.6% in cadaveric 21,28 and clinical 1,4 -6,18,19,22 -27,29 -31 investigations of RAN systems. Fujishiro et al 28 and Hyun et al 4 observed no major breaches, in agreement with the present study. However, comparisons between RAN and non-RAN procedures have produced mixed results. Lieberman et al 21 report MIS RAN moderately reduced breach rates compared with conventional MIS in a cadaveric model (7.6% vs 13.5%). Molliqaj et al 25 observed MIS RAN significantly reduced breach rates compared with conventional MIS in a clinical setting (6.6% vs 11.1%); however, Hyun et al 4 found a negligible improvement with use of MIS RAN even though no major breaches were observed (0% vs 1.4%). Solomiichuk et al 18 report similarly negligible differences between RAN and non-RAN placement of percutaneous screws, albeit higher breach rates due to the focus on metastatic spinal disease (15.6% vs 16.3%). Alternatively, Kantelhardt et al 5 report minimal improvement in breach rate in MIS and open RAN compared with open freehand technique (6.0% and 4.6% vs 8.5%). In a study conducted by Ringel et al, 19 use of RAN significantly increased major breach rates compared with the freehand technique (15% vs 7%). Last, Laudato et al 30 observed no significant differences in major breaches between freehand (6.4%), CAN (4.2%), or RAN (4.7%) techniques. In the present study, the use of RAN significantly reduced major breach rates compared with conventional open and MIS procedures.
Key differences between RAN systems previously reported should be noted. The most investigated RAN system, SpineAssist/Renaissance, is a hexapod system that attaches to the patient’s spine by (1) a spinous process clamp and K-wires affixed to the adjacent spinous process (SP), (2) a T-shaped platform fixed by K-wires affixed to the cranial SP and iliac, and (3) a platform fixed to a cranial SP with a K-wire and caudally attached to the operating table by a “bed mount.” The aforementioned system is only compatible with a preoperative CT workflow and requires fluoroscopic images for registration. The small robotic arm positions a guiding tube along the trajectory and clinicians then use fluoroscopy to assist insertion of the drill, K-wire, and screw to the desired depth without the aid of real-time visualization or navigated instruments. Alternatively, ROSA (Zimmer Biomet, Warsaw, IN) includes a floor-fixable mobile base with robotic arm, and a mobile navigation camera. Intraoperative CT is used to register anatomy to the PRA and plan screw trajectories; the robotic arm supports tools needed to position a guiding tube, drill, and K-wire. Following insertion of the K-wire, a navigated axial guide enables real-time visualization/navigation of pedicle screw depth.
Differences between RAN designs and imaging workflows may influence screw accuracy and sensitivity to pathologies that may obfuscate registration. Specific to RAN design, screw misplacement due to instability of the K-wire fixation, and therefore the RAN platform, has been reported for both “patient-mounted” 21,29,32 and “bed-mounted” 19,25 configurations. The stability of the platform solely depends on the bone quality of the spinous process or iliac crest. Additionally, screw malposition has been attributed to motion of the PRA, and subsequent loss of registration, to RAN systems that do not attach directly to the patient and utilize a PRA. 22 Precise registration of the bony anatomy is critical, and is widely noted as a limiting issue with RAN systems dependent on the preoperative CT workflow requiring intraoperative planar fluoroscopy for registration. High body mass index (>35-40 mg/kg2), 29,32 poor bone quality, 13,19 high-degree curvature deformities, 13 metastatic disease, 29 and previously placed hardware 32 have been attributed to obfuscating bony anatomy, thus reducing registration precision, and contributing toward screw misplacement. Regardless of RAN design/workflow, screw misplacement most commonly resulted from skiving of either the guide tube or drill. 6,19,21,22,26,28,29,33 Both the guide tube and drill bit are designed to anchor at the bony entrance point of the screw; however, most entrance points for pedicle screws are on the slope of the lateral aspect of the facet joint. The increased facet slope in the upper thoracic spine 29 or due to facet joint hypertrophy 19 has been associated with skiving and subsequent screw misplacement; high drilling pressure is also associated with skiving. 33
While the current study used an intraoperative CT workflow to avoid the pitfalls of preoperative CT and the need for planar fluoroscopic registration, the investigated RAN system possesses several unique features to avoid the limitations of PRA motion and instrument skiving. 34 Exclusive to the system, a surveillance marker was percutaneously inserted contralateral to the PRA to track motion of the PRA; the clinician would be alerted that the registration may be no longer valid if displacement between the 2 objects occurs. Furthermore, the PRA was designed to include a spring-loaded detented hinge that, should the PRA be accidentally hit, would allow the array to return to its original position. Additionally, the RAN system possesses a multi-axis load cell positioned between the guide tube and robotic arm to detect any forces or torques caused by skiving, or deflection of the tip of the tool/guiding tube in contact with the bone, and will alert the clinician in real-time. Last, drill bit design may also affect skiving and subsequent accuracy. Traditional orthopedic drill bits include a fluted design with a pointed tip that may be susceptible to sliding across the facet when force is applied. Alternatively, the investigated RAN system includes a side-cutting squared-off drill bit, similar to bits used when machining metal or wood when the approach angle is not perpendicular to the surface. When using a side-cutting bit, the bit must be sharp, and high rotational speed and low thrust is recommended. 34
Intraoperative deviation of the screw trajectory from the planned trajectory is a concern that is unique to RAN platforms. In the present study, the average deviation of the screw head was 0.87 to 1.19 mm in the axial, sagittal, and coronal planes using the open navigation technique; and 0.83 to 1.63 mm with MIS RAN (Table 3). While deviations are within the range of previous investigations, direct comparisons are difficult due to alternative metrics describing the deviation. Fujishiro et al 28 observed average deviations of the screw entry point and depth at 30 mm in the axial plane (0.64 mm and 0.63 mm, respectively) and sagittal plane (0.77 mm and 0.80 mm, respectively). Alternatively, Devito et al 23 reported average positional error [(deviation at entry + tip)/2] of 1.2 mm and 1.1 mm in the axial and sagittal plane, respectively. Nevertheless, minimizing deviation from the preoperative planned trajectory greatly depends on proper drilling and avoidance of skiving. 28
In addition to significantly decreased breach rates compared with non-RAN procedures, the use of RAN enabled the use of larger pedicle screws (in diameter and length; Table 4). These differences may be attributed to access to, and use of, intraoperative CT for the surgical planning of pedicle screws in the RAN treatment group. Preoperative CT is commonly used for pedicle measurements or surgical planning and would likely minimize differences in screw dimensions observed in the present study.
Finally, ionizing radiation exposure experienced by the clinician and staff is a key concern, particularly with MIS techniques. 35 The current investigation found use of RAN significantly reduced radiation compared with open and MIS non-RAN procedures. The overall results are in general consensus with published literature. 4 -7 Hyun et al 4 found that use of RAN decreased radiation from 13.3 seconds/screw to 3.5 seconds/screw when compared with open freehand. However, the benefits of RAN were not observed by Ringel et al (1.9 vs 1.9 minutes), due to the dependency of the RAN platform used (SpineAssist/Renaissance) on K-wires and fluoroscopic registration. The presently investigated RAN platform does not require K-wires for screw insertion, and was used with intraoperative CT, thus removing the need for fluoroscopic registration or confirmation of screw depth.
While the present study successfully characterized simulated operative time, pedicle screw accuracy, and radiation exposure of a novel RAN system to conventional non-RAN techniques, several limitations should be noted. Cadaveric specimens used excluded spinal trauma, malignancy, or fractures that would otherwise affect the accuracy of conventional and RAN procedures; exclusion of such specimens was due to an inability to produce torsos exhibiting similar pathologies. The lack of randomization between the order of screw placement, open/MIS and RAN/non-RAN procedures, and spinal regions may have introduced bias. The order of screw placement (conventional MIS, RAN MIS, open conventional, and open RAN) was selected to eliminate the influence of (1) placed RAN MIS screws on conventional MIS placement and (2) visualization of the open technique on MIS screw placement. While randomization between open and MIS techniques in the lumbar and TL spine would have allowed for comparisons between the spine regions, the lumbar region is the most prominent site of degeneration 36 and, presumably, use of MIS technologies. Additionally, differing preferences of the participating surgeons, or experience favoring either open or MIS techniques, or RAN or non-RAN procedures, may have affected screw size selection, breach rates, or simulated operative times, and should be considered a limitation.
Conclusions
The present healthy cadaveric study demonstrated that the novel RAN platform and planning software significantly improved pedicle screw accuracy and decreased clinician fluoroscopic radiation exposure compared with conventional techniques. The RAN platform decreased overall experimental operative time over conventional MIS; setup time significantly increased, yet screw insertion time for the navigation group was significantly lower. In the open technique, the RAN platform significantly increased overall and setup experimental operative time, but was time-neutral during screw insertion. Further investigation in cadavers with spinal trauma, malignancy, or fractures that would otherwise affect results is warranted.
Footnotes
Authors’ Note
The robotic navigation platform (ExcelsiusGPS, Globus Medical, Inc, Audubon, PA) and pedicle screws (CREO, Globus Medical, Inc) examined in this study are FDA-approved for the application described within.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors would like to disclose that this study was performed at Globus Medical, Inc (GMI), using its 6-degrees-of-freedom motion simulator. Cadaveric specimens and related materials were provided by GMI, at which JAH, MMH, NRC, and BSB are employees. Author RRP reports support for travel to meetings for this study or other purposes from GMI; is a paid consultant for GS Medical, Medtronic, MizuhoOSI, and ZimmerBiomet; has grants from GMI, Medtronic, SpineGuard, ZimmerBiomet, and Boston Scientific; and is employed by Epiom, Haider Biologics, and Xenco. Authors ARV, RKW, SRS, PGP, VWC, WPS, RDP, and SD have no conflicts of interest to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.