
Abstract
Study design
Retrospective case-series study
Objectives
To assess (1) low cone beam CT (CBCT) mediated intraoperative navigation to limit radiation exposure without compromising surgical accuracy, and (2) the potential of intraoperative C-arm CBCT navigation to augment pedicle screw (PS) placement accuracy in AIS surgery compared to pre-surgery CT-based planning.
Methods
The first part involved a prospective phantom study, comparing radiation doses for conventional CT, and standard (6sDCT) and a low dose (5sDCT) Artis Zeego®-imaging. Next, 5sDCT- and 6sDCT-navigation were compared on PS accuracy and radiation exposure during AIS correction. The final part compared surgical AIS deformity correction through intraoperative 5sDCT navigation to a matched cohort treated using conventional pre-surgery CT-scans for navigation. Outcome parameters included operation time, skin dose (SD), dose area product (DAP), intraoperative blood loss, postoperative complications, and PS deviation rates.
Results
The phantom study demonstrated a reduction in radiation for the 5sDCT protocol. Moreover, 5sDCT-imaged patients (n = 15) showed a significantly lower SD (-27.41%) and DAP (-30.92%), without compromising PS accuracy compared with 6sDCT-settings (n = 15). Finally, AIS correction through intraoperative CBCT C-arm navigation (n = 27) significantly reduced screw deviation rates (6.83% versus 10.75%, P = .016) without increasing operation times, compared with conventional CT (n = 37).
Conclusions
Intraoperative navigation using a CBCT C-arm system improved the accuracy of PS insertion and reduced surgery time. Moreover, it reduced radiation exposure compared with conventional CT, which was further curtailed by adapting the low-dose 5sDCT protocol. In short, our study highlights the benefits of intraoperative CBCT navigation for PS placement in AIS surgery.
Introduction
Adolescent idiopathic scoliosis (AIS) is a complex disorder that involves a curvature and rotation deformity of the spine. While its prevalence is estimated at .5%–5.2%, 1 the etiology of AIS remains largely elusive.2,3 Curvature corrections aimed to alleviate disability, reduce neurological risk, and improve patients’ self-image generally involve surgical translation and rotation techniques followed by spinal fixation.4-7 Contemporary correction maneuvers employ instrumentation comprising pedicle screws (PS) to provide a strong fixational force enabling vertebral manipulation and correction maintenance. PS insertion requires meticulous care not to impair adjacent and critical nerve and vasculature structures. Generally, PS placement is attempted following careful preoperative planning, direct visualization, and pedicle probing.8,9 Nevertheless, detection of pedicle breaches remains challenging.
Intraoperative imaging and navigation techniques have become commonplace for instrumented spinal surgeries, including hybrid operating rooms (ORs) with incorporated navigation systems.10,11 (Figure 1) Such floor-mounted C-arm multi-axis robotic cone-beam computed tomography (CBCT) 3D-imaging devices (Figures 1B and 1D) rely on a cone-shaped X-ray beam emitted towards a two-dimensional (2D) detector that is rotated once around the patient, generating complete volumetric data in a single rotation. It is unlike conventional CT scans, which rely on fan-shaped X-ray beams that create slice-by-slice images to construct a stacked 3D image.12,13 As a result, CBCT has been suggested to decrease the amount of radiation exposure compared with conventional CT methods.
17
Intraoperative CBCT also has the potential advantage of enabling direct repositioning of misplaced screws, thereby reducing re-operating rates and postoperative CT scans. Work by Cordemans et al highlighted that intraoperative CBCT allows for accurate measurement of screw misplacement similar to postoperative CT scans in their spinal surgery cohort.
14
Identical conclusions were made by Burström et al.
15
Both studies involved patients undergoing spinal fusion for a range of spinal diseases, including malignancies and trauma. One study by Oba et al
16
specifically examined the potential utility of intraoperative CBCT for AIS corrective surgery. However, they did not compare outcomes with other navigation techniques nor did they record radiation exposure. Illustrative overview of imaging and navigation equipment described in this study. (A) O-arm™ Surgical Imaging System (Medtronic Inc, Memphis, TN, USA; not used), (B) Robotic C-arm system Artis Zeego® (Siemens AG, Forchheim, Germany), (C) StealthStation® S7® (Medtronic, Memphis, TN, USA), and (D) Magnus Operating Table System (Maquet, Rastat, Germany) within a hybrid operating room.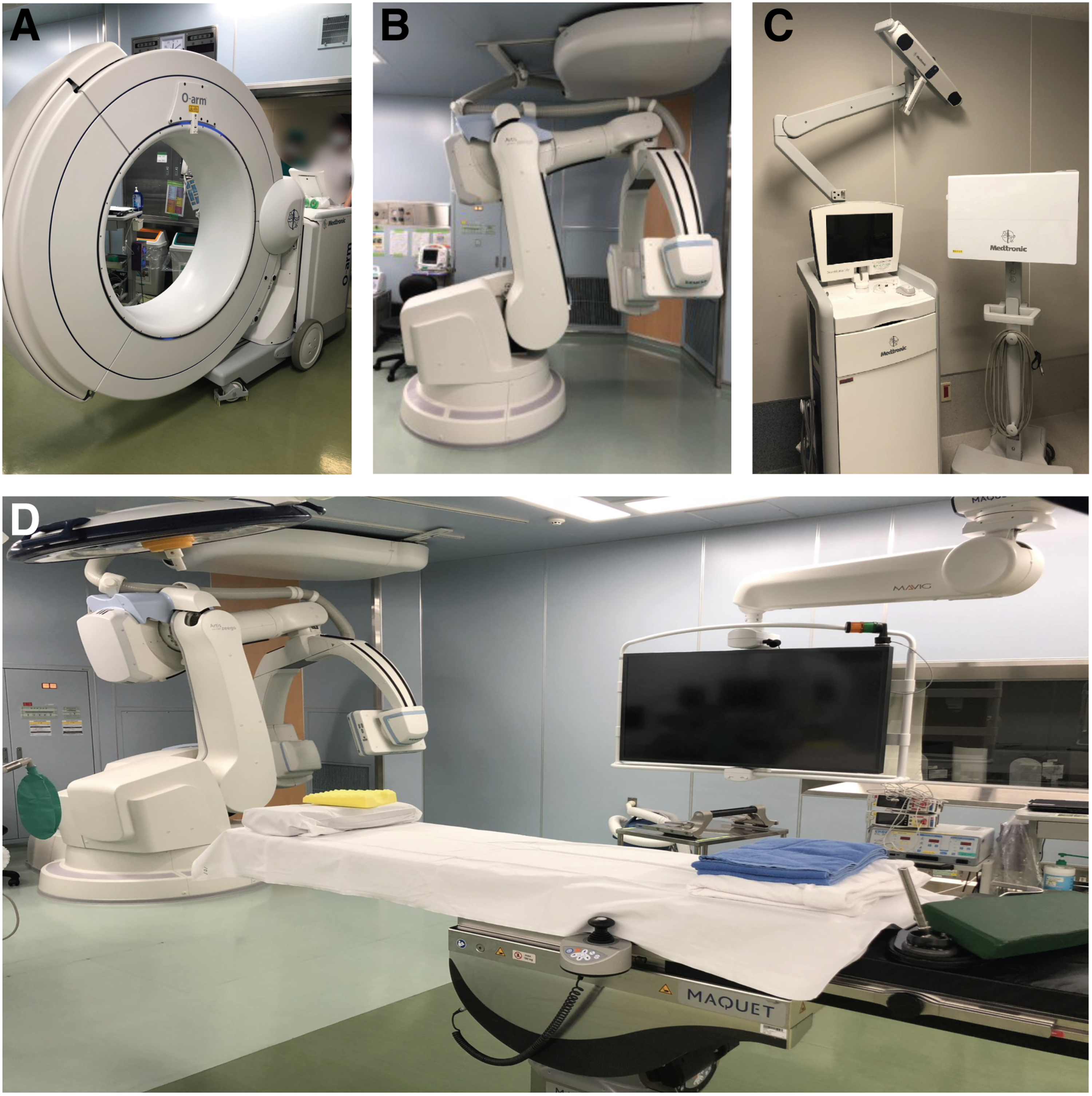
AIS correction engenders a particularly challenging surgical procedure due to the relatively small and abnormally angled pedicles. As such, navigation techniques are ideally examined on AIS patients specifically. Moreover, AIS patients are relatively young individuals, exacerbating potential radiation exposure risks,17,18 although others argue against an overemphasis on this aspect. 19 Considering these limitations of the contemporary literature, by this retrospective study consisting of three separate parts, we aim to (1) validate the potential of a low-exposure protocol for the Artis Zeego® to reduce radiation exposure while maintaining surgical precision, and (2) to examine potential improvements in safety and accuracy of PS insertion for AIS deformity correction guided by intraoperative robotic C-arm CBCT system compared with a matched cohort planned for conventional presurgical CT navigation.
Materials and Methods
Study Design and Patient Selection
All procedures described were performed in accordance with ethical standards directed by and upon approval of our institutional review board and the 1964 Helsinki declaration and its later amendments. (12R-036, 16R-052) Informed consent for analysis of medical records was provided by participants or their respective parent(s) or legal guardian(s). Medical records were screened for AIS patients who underwent posterior (or anterior and posterior) correction and spinal fusion (PSF) from Jan 2015 to Jan 2020. Patient records were eligible if patients were mainly classified as thoracic curve scoliosis (T2–T12) with Lenke type 1 to 3.
The first part of the study aimed to get a general impression of radiation dosage involved in the different imaging settings using in-phantom dose measurements with radiophotoluminescence glass dosimeters (Chiyoda Technol Corporation, Tokyo, Japan). The dosimeters were attached to five locations at thoracic vertebrae level 8 on the back, right and left side, and right and left chest of the phantom (Figure 2A). Effective doses were measured using standard CT equipment (SOMATOM Definition Edge, Siemens AG) and the Artis Zeego® system. Artis Zeego® runs on syngo DynaCT (Siemens AG), which provides a standard 6-second spin (6sDCT) protocol.
17
In our institution, a “low-exposure protocol” has been adapted involving 248 projections during a 5-second spin (5sDCT; see Supplemental Figure 1 for a settings overview). Standard CT, 5sDCT, and 6sDCT imaging measurements were each taken once to evaluate dosimetric readings. (A) Radiophotoluminescence glass dosimeter on anthropomorphic phantom at thoracic vertebrae level 8 (Th8); [1] Right side, [2] Right chest, [3] Left chest, [4] Left side, and [5] Dorsal side. (B) Skin dose (SD) measured at each site using conventional computed tomography (CT), or cone beam CT (CBCT) using 6sDCT or 5sDCT settings.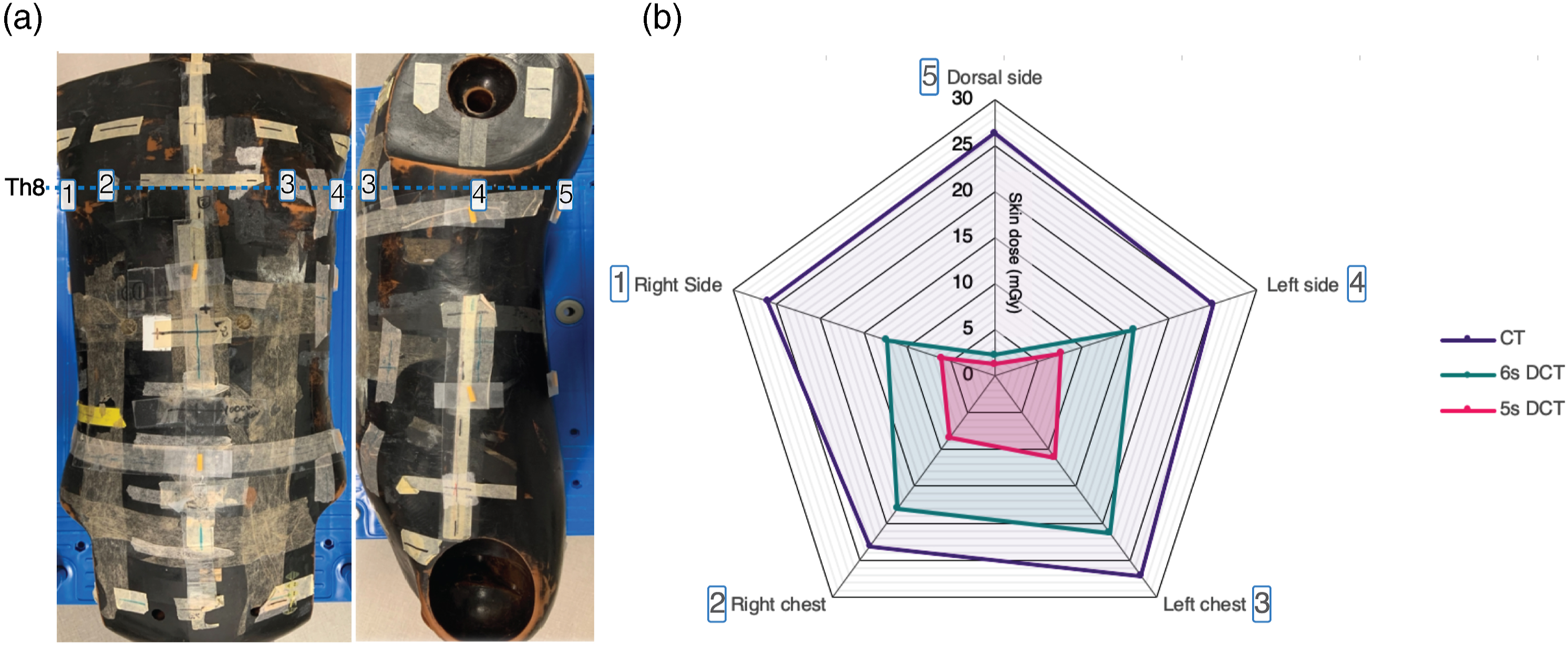
The second part of the study involved the validation of radiation exposure reduction by the 5sDCT protocol while retaining accurate PS placement during AIS surgery. The 5sDCT cohort was compared to a historical AIS patient cohort treated under the 6sDCT navigation settings. Postoperative images to detect PS deviations were obtained through the 5sDCT or 6sDCT settings for the 6sDCT cohort.
To assess improved PS accuracy through intraoperative CBCT navigation, the third study part, included patients that underwent surgical correction using the intraoperative robotic CBCT C-arm with 5sDCT within the hybrid OR (L-group) treated from Jan 2017 to Jan 2020. The cohort was matched to a historical AIS cohort (treated from Jan 2015 to Dec 2016) who underwent similar procedures in a standard OR using pre-surgery CT-scans for navigation (M-group). Cohort matching for both the second and third study parts was based on patient age, height, weight, Lenke type, 20 and Cobb angle.
Surgical Intervention
All surgical procedures were performed by the same spine surgeon. Patients were placed in the prone position during PSF with instrumentation. Generally, two titanium PS were employed per vertebral level, however, if the surgeon considered the pedicle too small or fragile, the insertion could be skipped or PS could be replaced by hooks. Before insertion of the PS, the inferior and superior articular processes within the to-be-fixed range were resected. The hybrid OR encompassed a radiolucent Magnus Operating Table System (Maquet, Rastat, Germany) and a StealthStation® S7® navigation system (Medtronic, Memphis, TN, USA; Figures 1C and 1D). Surgical navigation was performed using surface registration based on the intraoperative CBCT images (L-group; see Video 1 for 3D reconstruction) or the preoperative CT images (M-group; Figure 3A). Comparing navigation images from conventional CT and intraoperative CBCT scan. Pictures represent sagittal and axial views of representative AIS spines (A) pre- and (B) post-surgical instrumented deformity correction. For a representative animation of the CBCT 3D images see Video 1. (CBCT: cone-beam computed tomography, CT: computed tomography). Video 1. Example of spine 3D reconstruction using our 5sDCT CBCT scan technique of spine pre- and post-surgical correction.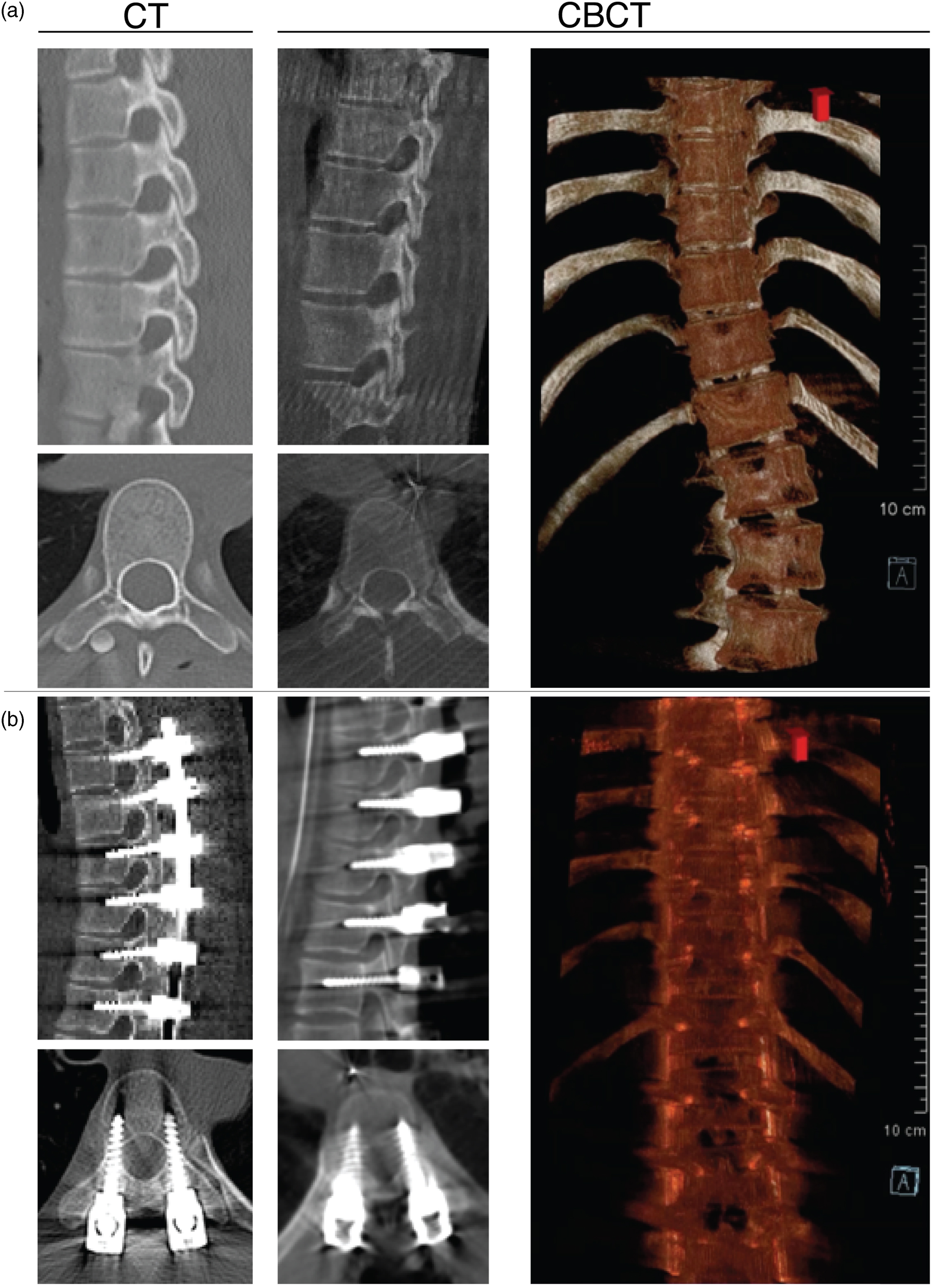
Outcome Parameters
For each patient, standard demographics, preoperative radiographic assessments (i.e., main Cobb angle and Lenke type 20 ), and surgical features were registered. Similarly, screw deviation rates (assessed postoperatively using intraoperatively obtained CBCT-images or postoperative CT images) were evaluated (Video 1). Screw deviations were qualified according to Nakanishi et al 21 with grade 2 or higher being considered violations. Patient records were also examined for serious or severe adverse events up to 2 years following deformity correction, including neurological, vascular, and infectious complications.22,23 Finally, radiation exposure was determined for the 5sDCT, 6sDCT, and L-groups as dose area product (DAP) and skin dose (SD).24-27
Statistical Analysis
All data were collected and processed in Microsoft Excel (Microsoft Co. Ltd, Redmond, WA). Statistical analyses were performed using IBM SPSS Statistics version 23.0 (IBM Corp, Armonk, NY). All values are expressed as mean ± standard deviation unless stated otherwise. Comparisons between patient groups were made using the Mann–Whitney U test or chi-square test. A P value ≤.05 was considered statistically significant.
Results
Part 1: Phantom Dose Measurements
The SD was measured as 25.5 ± 1.6 mGy, 14 ± 7.3 mGy, and 6.9 ± 3.7 mGy in the CT group, 6sDCT, and 5sDCT, respectively (Figure 2B). The SD was higher in the CT group than in the 5sDCT. Moreover, CT showed a clear trend of higher SD compared with the 6sDCT. Minimal radiation was measured at the dorsal side, likely due to the 200° imaging rotation for CBCT compared with the 360° rotation for the CT scan. Overall, both CBCT methods showed a clear SD reduction, with 44.8 ± 29.1% and 72.9 ± 14.2% reduction compared with CT for 6sDCT and 5sDCT, respectively (Supplemental Table 1).
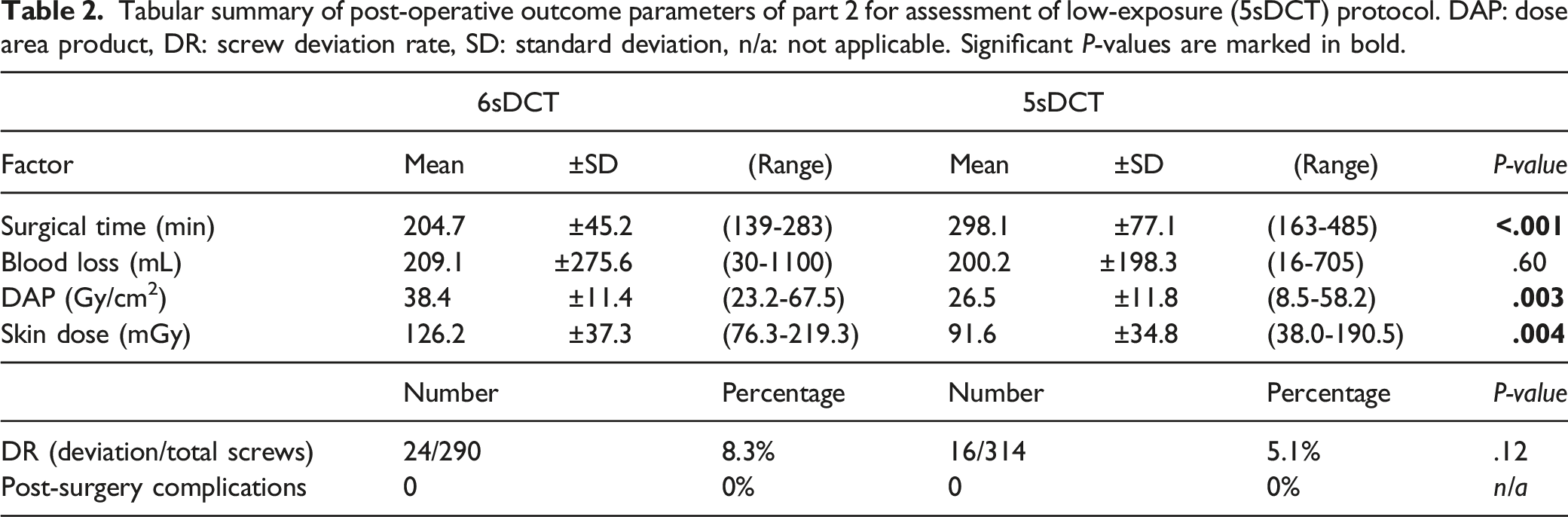
Part 2: 5sDCT Protocol Assessment
Tabular summary of demographic patient characteristics of part 2 included for assessment of low-exposure (5sDCT) protocol.
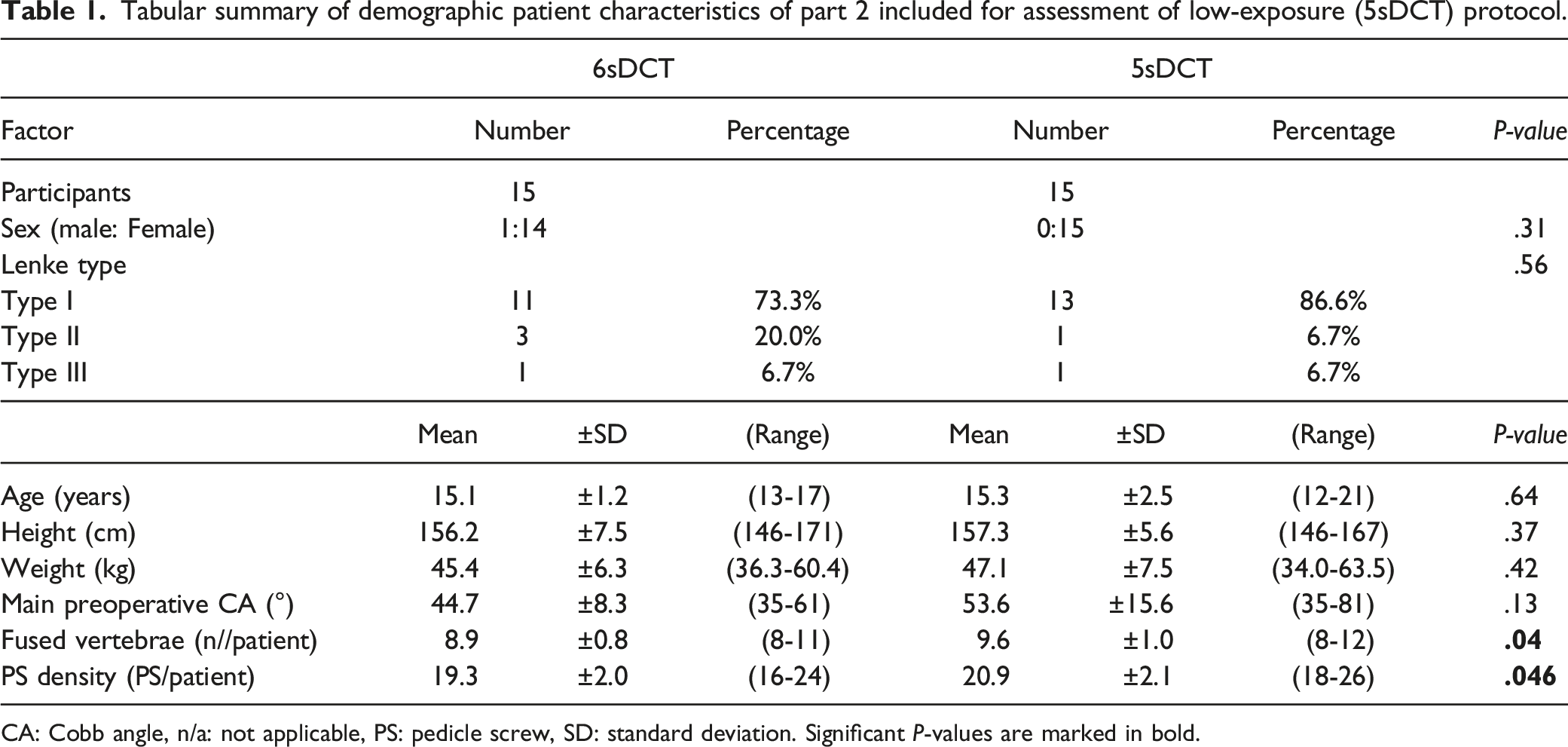
CA: Cobb angle, n/a: not applicable, PS: pedicle screw, SD: standard deviation. Significant P-values are marked in bold.
Tabular summary of post-operative outcome parameters of part 2 for assessment of low-exposure (5sDCT) protocol. DAP: dose area product, DR: screw deviation rate, SD: standard deviation, n/a: not applicable. Significant P-values are marked in bold.
Part 3: Intraoperative CBCT Imaging Compared With Pre-surgery CT Imaging
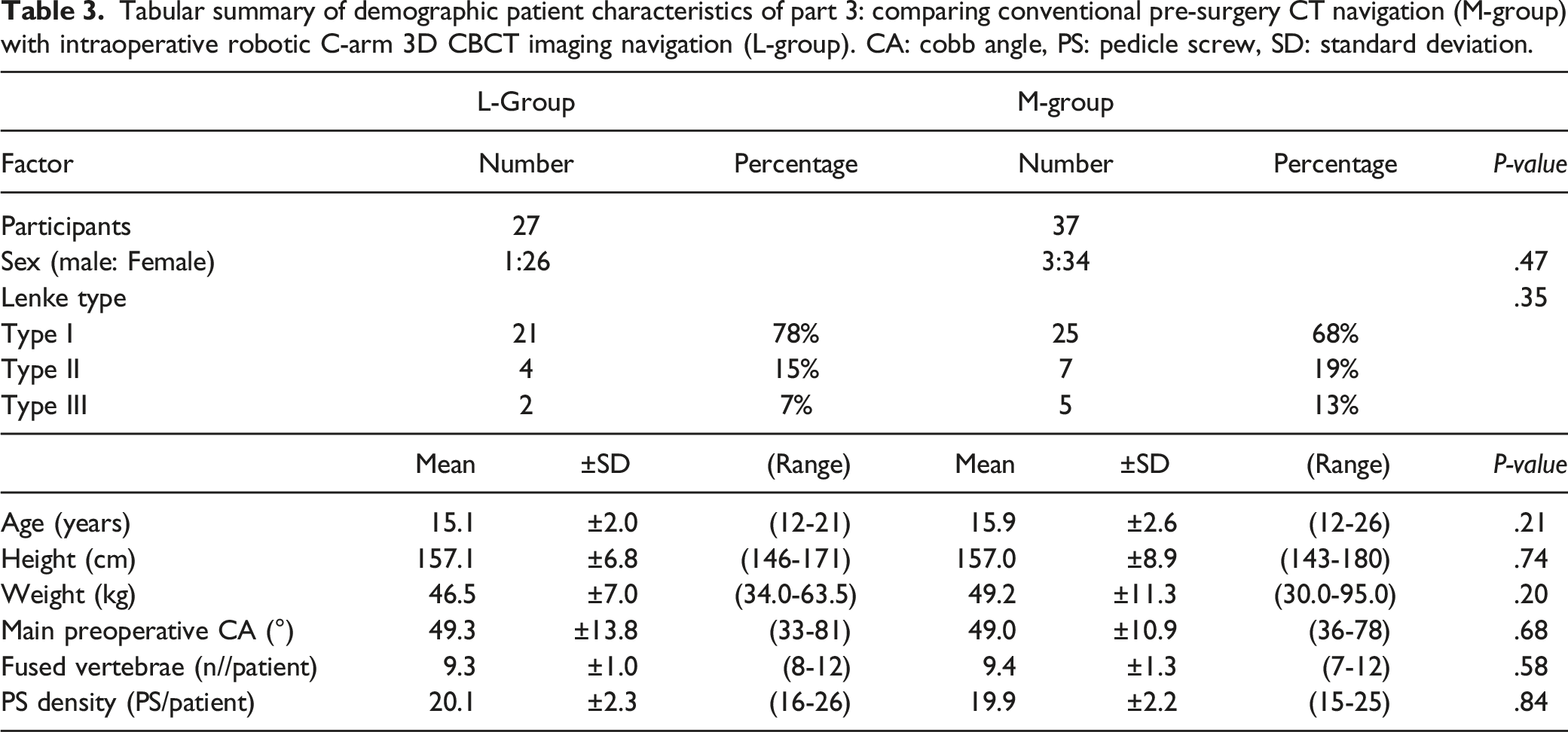
Tabular summary of demographic patient characteristics of part 3: comparing conventional pre-surgery CT navigation (M-group) with intraoperative robotic C-arm 3D CBCT imaging navigation (L-group). CA: cobb angle, PS: pedicle screw, SD: standard deviation.
Tabular summary of post-operative outcome parameters of part 3: comparing conventional pre-surgery CT navigation (M-group) with intraoperative robotic C-arm 3D CBCT imaging (L-group).
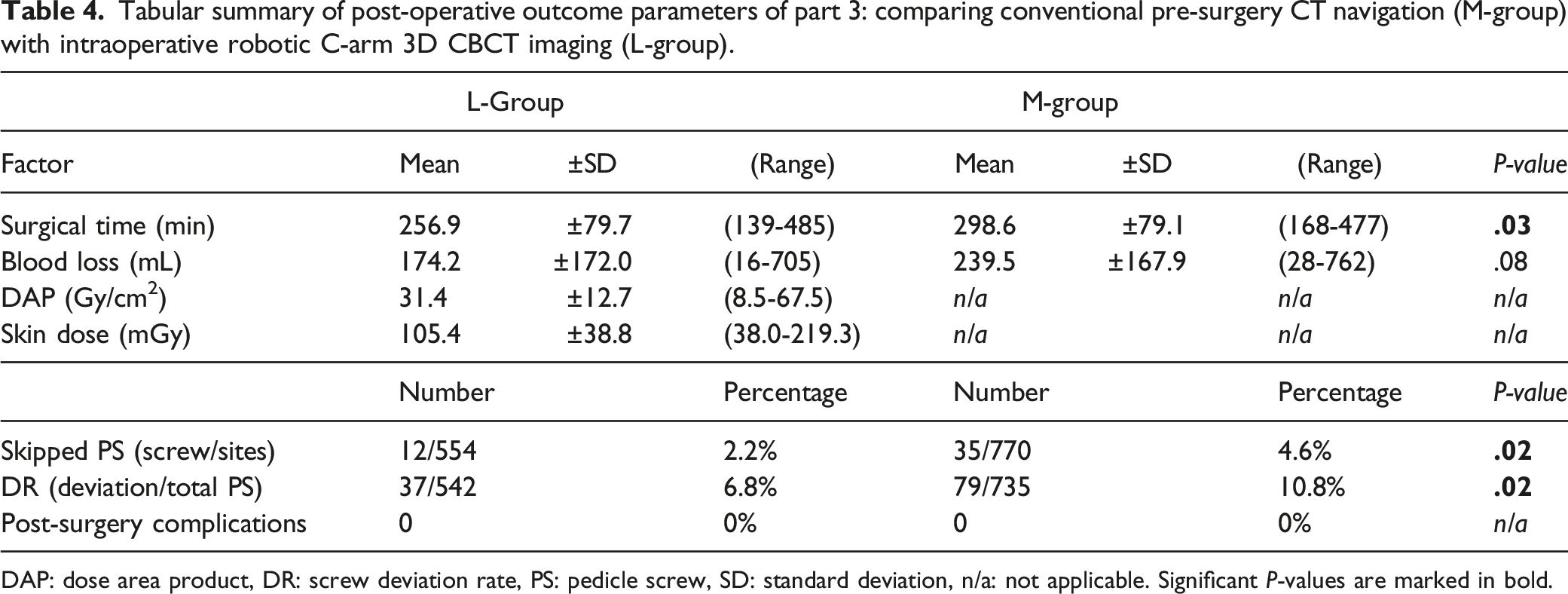
DAP: dose area product, DR: screw deviation rate, PS: pedicle screw, SD: standard deviation, n/a: not applicable. Significant P-values are marked in bold.
Discussion
As surgical navigation with intraoperative CBCT has become more prevalent, concerns have been raised regarding potential surgery time extensions.28-30 Surprisingly, in our study, we found that intraoperative robotic C-arm CBCT actually significantly reduced surgery time. One explanation could be the additional time taken for intraoperative CT scans in the M-group after screw insertion to assess potential screw deviation after corrective manipulation. Notably, however, the surgery time within the L-group could likely be further reduced if we had applied automatic registration instead of manual registration. Our literature review (Supplemental Table 2, for an overview of identified studies) of CBCT-guided PS-based instrumented spinal surgeries suggests that our average time of 260 min is in line with other studies employing intraoperative C-arm imaging. For example, Tajsic et al 31 and Oba et al 16 presented surgery times of 211 min and 236 min respectively. Additionally, the intraoperative CBCT provided lower rates of skipped PS, suggesting the CBCT based navigation offers higher confidence to the surgeon to employ PS insertion than navigation based on pre-operative CT-scans.
It is important to justify and optimize radiation doses. The International Commission on Radiological Protection (ICRP) promotes three principles of radiological protection: justification, optimization, and dose limits. 32 Specifically, the 2011 “ICRP Statement on Tissue Reaction” has set the exposure limit of 20 mSV a year upon the eye lens. 33 Medical workers can take various actions to reduce radiation exposure. For example, surgeons and accompanying staff can be located outside the OR during the imaging process. Moreover, while exposure to patients cannot be avoided, the incidental dosages applied with modern imaging equipment are relatively low and potentially negligible. 19 By contrast, others have emphasized the higher rates of cancer among patients with scoliosis and caution against radiography. For example, a recent metanalysis by Luan et al 18 found that among 3301 patients with general adolescent scoliosis, 532 developed cancer (17.6%) following a period of ≥20 years, compared with 457 cases among 3045 (13.1%) in a control cohort. The authors attributed this increase to radiation exposure during the management of scoliotic deformity. 18 In our view, this assumption is somewhat presumptuous, as the studies included do not directly correlate radiation dose with carcinogenesis or propose alternative hypotheses. 19 Instead, Oakley et al hypothesized that the enhanced cancer rates might be inherent to the scoliotic pathology itself. 19 Noticeably, few reports have examined radiation doses in patients undergoing spinal instrumentation by C-arm CBCT. Cordemans et al reported a DAP of 81.6 Gy/cm2 and SD of 267 mGy, while Kaminski et al reported a DAP of 82.8 Gy/cm2 and SD of 273 mGy, both of which are double the amount measured in our cohort.14,34 Gebhard et al found that iso-C3D-arm-guided spinal fusion resulted in higher doses of 664 mGy. 35 Kobayashi et al 36 measured SD of 401 mGy for AIS surgeries using the O-arm™. These findings suggest that radiation exposure through robotic C-arm CBCT devices tends to be lower than conventional CT. Moreover, considering our suggestion that intraoperative CBCT removes the need for post-correction CT-scans, we conclude that intraoperative CBCT-mediated navigation can reduce radiation exposure during AIS surgery.
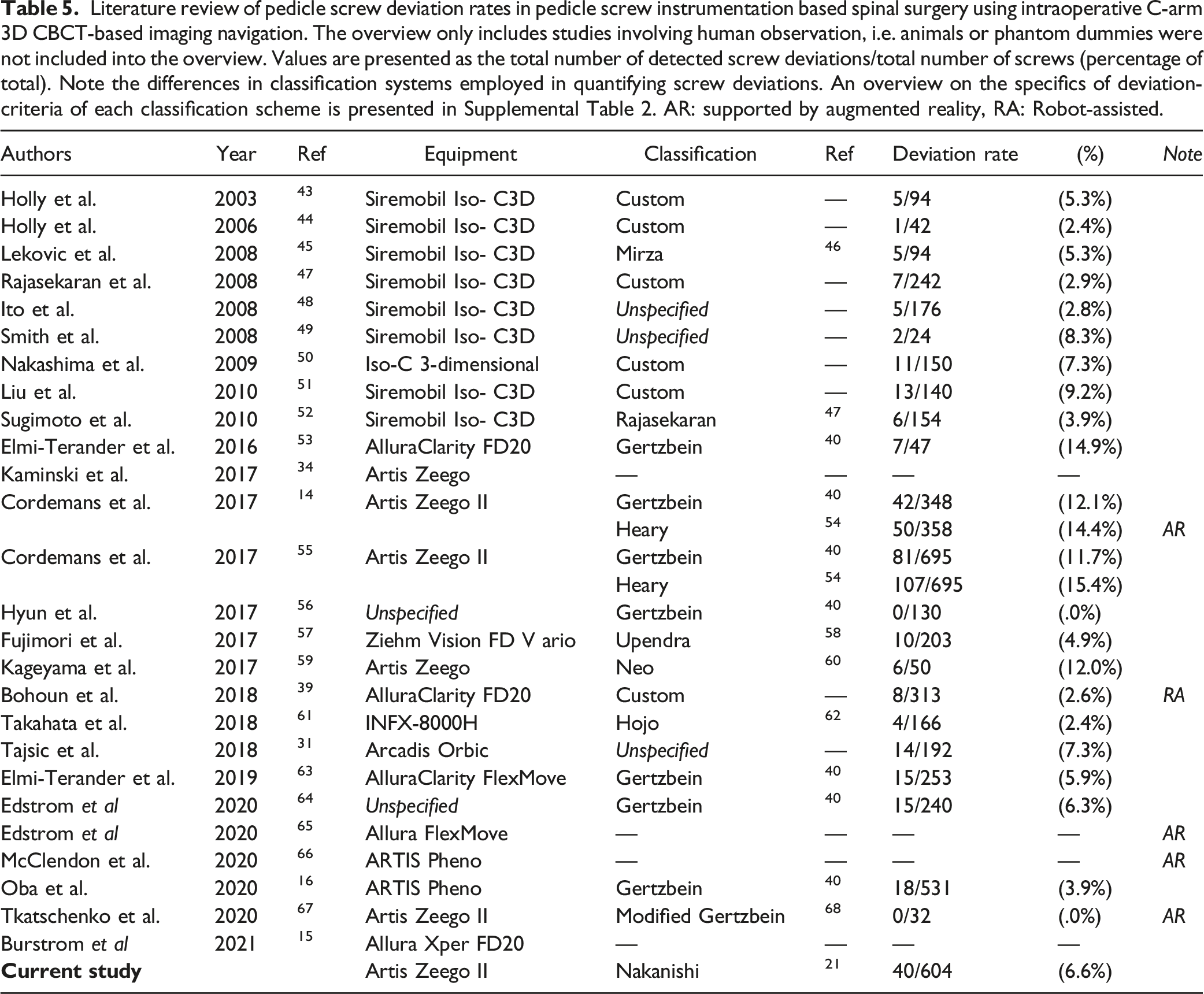
Literature review of pedicle screw deviation rates in pedicle screw instrumentation based spinal surgery using intraoperative C-arm 3D CBCT-based imaging navigation. The overview only includes studies involving human observation, i.e. animals or phantom dummies were not included into the overview. Values are presented as the total number of detected screw deviations/total number of screws (percentage of total). Note the differences in classification systems employed in quantifying screw deviations. An overview on the specifics of deviation-criteria of each classification scheme is presented in Supplemental Table 2. AR: supported by augmented reality, RA: Robot-assisted.
One limitation of our study is that we did not measure the radiation exposure from the preoperative CTs in the M-group and, thus, were unable to directly compare exposure rates between the groups. However, our phantom study revealed a clearly reduced exposure rate for the CBCT techniques. Another limitation is the retrospective and nonrandomized nature of the study. Although case matching was applied, the different periods for each cohort in which the corrections took place might also have affected the outcomes. Moreover, our findings were obtained under specific imaging conditions set at our institute and thus might vary when operated by others. Even so, cumulatively our data and other reports suggest that intraoperative CBCT navigation allows for enhanced PS accuracy, operating time reductions, and a suggested lower radiation exposure. Accordingly, we are of the opinion that these benefits outweigh the likely small risk increase 26 provoked by the low-radiation exposure generated by CBCT. Moreover, future developments in software and equipment, are likely to enable radiation dosage reduction without compromising on resolution and accuracy. These advancements are highly encouraged.
Conclusion
In summary, intraoperative CBCT navigation with a robotic C-arm device for AIS surgery reduced PS deviation rates and radiation exposure compared with conventional preoperative CT-based procedures. Moreover, our low-dose 5sDCT setting was able to reduce radiation dosages significantly without compromising PS accuracy.
Supplemental Material
Supplemental Material - Low Radiation Protocol for Intraoperative Robotic C-Arm Can Enhance Adolescent Idiopathic Scoliosis Deformity Correction Accuracy and Safety
Supplemental Material for Low Radiation Protocol for Intraoperative Robotic C-Arm Can Enhance Adolescent Idiopathic Scoliosis Deformity Correction Accuracy and Safety by Masahiro Tanaka, MD, PhD, Jordy Schol, MSc, Daisuke Sakai, MD, PhD, Kosuke Sako, MD, Kazuyuki Yamamoto, MD, Kensuke Yanagi, MD, Akihiko Hiyama MD, PhD, Hiroyuki Katoh MD, PhD, Masato Sato MD, PhD, and Masahiko Watanabe M in Global Spine Journal.
Supplemental Material
Footnotes
Acknowledgments
We would like to thank Prof. Hiroyuki Kobayashi, M.D., PhD (Department of Clinical Pharmacology, Tokai University School of Medicine, Isehara, Japan) for his support and advice for the statistical analysis, and Natsumi Horikita (Tokai University School of Medicine, Isehara, Japan) for her support in processing and animating the CT-images for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.