
Abstract
Study design
Diagnostic accuracy study.
Objectives
Previous studies have reported the clinical application of the Vertebral Bone Quality (VBQ) scores for assessing bone density in operative lumbar spine patients. We aim to explore whether the method could be modified and applicable for patients undergoing cervical spine surgery.
Methods
Adult patients receiving cervical spine surgery for degenerative diseases between September 2020 and March 2022 with non-contrast T1-weighted MRI and DEXA were included. Correlation between cervical VBQ scores and DEXA T-scores was analyzed using Pearson’s correlation. Student’s t test was used to present the discrepancy between the VBQ of patients with normal bone density (T ≥ -1.0) and patients with osteopenia/osteoporosis (T < -1.0). Statistical significance was set at P < .05.
Results
Eighty-three patients (20 patients with T ≥ -1.0 vs 63 patients with T < -1.0 ) were included. Significant difference was found between the cervical VBQ between groups (2.99 ± .79 vs 3.80 ± .81, P < .001). Interclass correlation coefficient for inter-rater reliability was .82 (95% CI: .70-.93) and .91(95% CI: .84-.97) for intra-rater reliability. The area under the ROC curve was .78 (95% CI: .65-.90). The DEXA T-score of the femoral neck, total hip and the lowest DEXA T-score were found to be significantly correlated with the cervical VBQ score according to Pearson correlation analysis (P < .001).
Conclusions
This is the first study to apply the VBQ method to assess the bone density in preoperative cervical spine patients. Cervical VBQ scores were significantly correlated with DEXA T-score. With an overall accuracy of .78, the radiation-free and cost-effective method could be a potential tool for screening patients with osteopenia and osteoporosis before surgery.
Introduction
It is well recognized that bone quality plays an important role in cervical spine fusion surgery due to its impact on biomechanical properties such as the screw pullout strength, insertional torque and loading strength of the vertebrae.1,2 Poor quality has been reported to be associated with suboptimal surgical outcomes including construct failure, pseudarthrosis, cage subsidence, and need for revision.3-7
The current guideline recommends that men ≥ 70 years old and women ≥ 65 years old should receive bone mineral density (BMD) measurement with dual-energy X-ray absorptiometry (DEXA), which is the current gold standard. 8 For surgical patients, screening for low BMD has been recommended by surgeons to achieve better surgical outcomes. 9 Surgeons could determine the optimal surgical scheme and fixation according to the acquired BMD, generally via DEXA.5,10 With an increasing average lifespan of whole population, spine surgeons nowadays could encounter increasing number of elder patients, who may require surgery in cervical spine and have poor bone quality at the same time.
However, a survey including 114 spine surgeons showed that only 44% of them arranged the preoperative DEXA scan for patients before instrumented fusion surgery although the majority of patients were elders. 11 Another study has found a low adherence rate to the guideline as few as 27% for eligible patients. 12 Thus, a large number of patients receiving spine surgery do not have accessible BMD data. Additionally, errors might exist during DEXA scan for patients with vascular calcification, obesity and some other situations.13-15 Besides, the DEXA scan data was commonly based on the femoral or lumbar spinal images, which might be inconsistent with the regional bone quality of the cervical spine in some situations.
Due to the aforementioned reasons, some researchers have sought to study novel alternative assessment measurements based on data acquired during the routine preoperative evaluation for spine surgery. 13 The vertebral bone quality (VBQ) was a recently described technique for assessing BMD with an 81% accuracy in identifying osteopenia and osteoporosis by taking advantage of the preoperative lumbar spine T1-weighted (T1W) MRI. 9 VBQ has become a practical tool for lumbar spine surgery given that previous studies have found the correlation between the VBQ score and DEXA T-scores and the prediction value of the VBQ score regarding postoperative complications.4,9,16-18 The method was cost-effective and radiation-free with fair diagnostic value.
However, to date, whether the VBQ method based on cervical spine MRI is applicable for preoperative BMD assessment before cervical spine surgery remains to be a simple but significant issue, given that previous studies mainly focused on the application of VBQ using lumbar spine MRI images in patients with lumbar spinal disorders. To best of our knowledge, there were no previous studies that attempted the VBQ method in cervical spine. From the theoretical perspective, the logic and science behind VBQ is strong due to using the non-contrast T1W signal intensity (SI) to reflect the fatty infiltration of trabecular bone. Therefore, we aimed to explore whether the similar easy-to-use method could be applied to assess the BMD in patients with preoperative cervical spine MRI.
Method
Patient Sample
The study referred to the method introduced by Ehresman et al. and we modified it according to cervical spine (details of the measurement would be introduced within the The flow diagram of the patients inclusion process.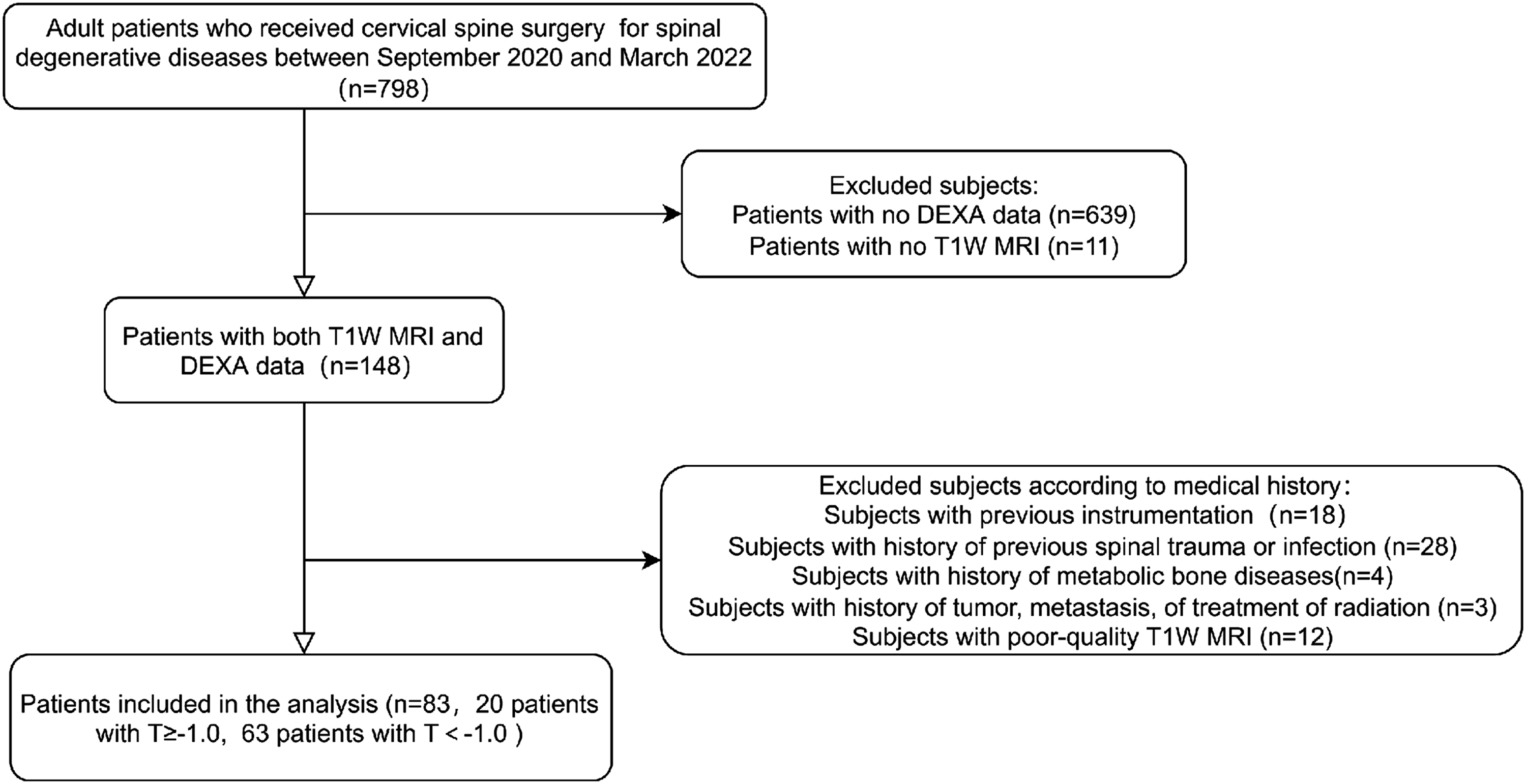
Cervical Vertebral Bone Quality Score Calculation
Taking the cervical spinal anatomy and convenience of measuring into consideration, we modified the VBQ calculation method raised by Salzmann et al. applied in the lumbar spine.
13
The cervical VBQ scores were calculated based on the MRI T1W images included in the current study. As Figure 2 shows, to acquire the cervical VBQ, the regions of interest (ROI) were placed within the medullary portions of vertebrae from C2 to C7 on the mid-sagittal MRI T1W slice through the GE PACS Centricity system. With regard to the detailed method on placing ROI, Salzmann et al. introduced that the elliptical ROI was placed 3 mm from the perimeter of the vertebral body.
13
However, in the cervical spine, we attempted to maximize the inclusion of vertebral body cancellous bone surrounded by the black cortical shell on T1W as Schilling described.
5
This attempt was one of the modifications applied in the current study, which was distinguished from the original method described by Ehresman et al.
13
There were 2 reasons for our measuring without 3 mm margin from the perimeter: (1) most importantly, the cortical bone presents no or very low signal intensity which was legible and enabled us to include the cancellous bone by observing the signal; (2) meanwhile, the cervical vertebral cortical shell was reported to be .285 ± .02 mm
19
, so 3 mm from the perimeter of the vertebral body might make the acquired VBQ scores less representative due to increasing exclusion area. It should be noted that regions such as bone islands or sclerotic changes were avoided within the ROI field. Subsequently, the C2-7 average SI (SIC2-C7) values were obtained by averaging the SI of each vertebra. To adjust for the intrinsic differences between the baseline existing across different scanners, when calculating the lumbar VBQ, previous studies adopted the SI of cerebral spinal fluid (CSF) for standardization given that CSF possesses relatively stable signal and has almost constant composition across people.
9
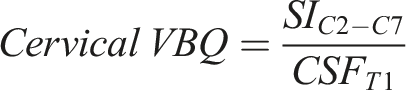
Another modification in our method is that the average ROI SI of the CSF at the upper T1-level on mid-sagittal MRI T1W slice was chosen as the means of standardizing. For lumbar spine, researchers generally choose to measure the SI of CSF at a medial lumbar level such as L3.9,18 In this study, the purpose of choosing the upper T1-level instead of C3 or C4 is to avoid the measuring difficulty and potential errors due to the presence of the intumescentia cervicalis and the possible spinal compression caused by degenerative tissues at C3-C7 in patients with degenerative diseases, and thus to acquire a relatively heterogeneous value by measuring the SI of CSF at upper T1-level. The parasagittal image would be used if the scoliotic changes lead to incapability of placing the ROI for certain vertebrae on the mid-sagittal T1W images. When the averaged SIs of the C2-C7 vertebrae and upper T1-level CSF (CSFT1) were acquired, the cervical VBQ could be calculated according to the following formula: Illustration on the cervical vertebral bone quality calculation process.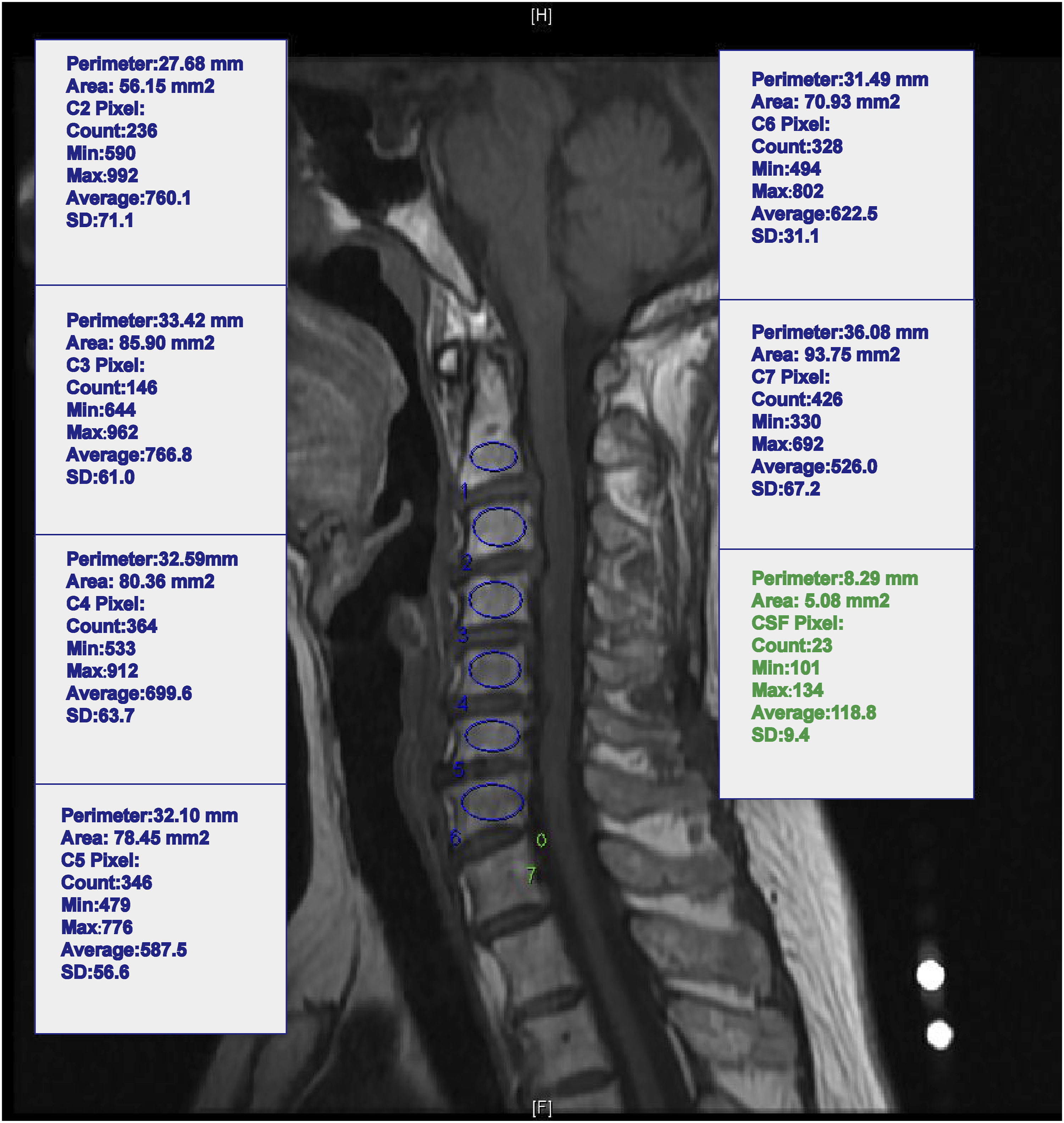
The measuring procedure was accomplished independently by 2 researchers (the first author and the co-first author) who were blinded to the information of patients and the 2 authors finished two-time measurements. Besides, to rule out the brand of MR scanner and tesla setting as the potential confounders, VBQ from various brands and tesla settings were recorded and compared using Kruskal-Wallis tests as well(See Supplementary Table 1).
Statistical Analysis
All data were recorded with Microsoft Excel and analyzed using SPSS Statistics version 21.0 (IBM Corp. Armonk, NY, USA) and Graphpad prsim 9 (GRAPHPAD SOFTWARE, LLC, California, USA). Continuous variables were described as mean ± standard deviation (SD). Normality tests with regard to the continuous variables of demographic data, DEXA T-score, and cervical VBQ score were performed via Statistics version 21.0 (IBM Corp. Armonk, NY, USA). During the comparison progress between the patients with osteopenia/osteoporosis and normal BMD, student’s t tests were used for continuous variables which were approximately normally distributed and the Mann–Whitney U tests were performed for variables with nonnormal distribution. Chi-Square test was used to compare the percentage. Receiver operating characteristic (ROC) analysis was performed to calculate the area-under-curve (AUC) of the cervical VBQ score as a predictor of osteopenia/osteoporosis. The Youden Index was applied to obtain satisfied cutoff cervical VBQ value for diagnosis. The multivariate linear regression (backward elimination technique) was performed to explore the predictive effects of all recorded demographic data and VBQ on DEXA T-Score. The ‘Simple linear regression’ (univariate linear regression) module of Graphpad prsim 9 (GRAPHPAD SOFTWARE, LLC, California, USA) was performed to acquire the detailed formula and statistical significance. The correlation between the DEXA T-score and cervical VBQ score was analyzed with Pearson correlation. Meanwhile, the Pearson correlation coefficient (r) was calculated by applying the ‘Correlation’ module of Graphpad prsim 9 (GRAPHPAD SOFTWARE, LLC, California, USA). The interclass correlation coefficient (ICC) with 95% confidence interval (CI) was used to calculate the intra-rater reliability and inter-rater reliability between 2 independent researchers. Based on previous literature, we regarded ICC less than .40 as poor, .40-.59 as fair, .60-.74 as good, and greater than .75 as excellent. 20 Statistical significance was set at P < .05. Meanwhile, PASS 15 Software (PASS Software, Rijswijk (ZH), The Netherlands) was used to confirm the power of tests and ROC analysis.
Results
Diagnosis Value of the Cervical Vertebral Bone Quality Scores
Demographics and Cervical VBQ Scores of the Patients.
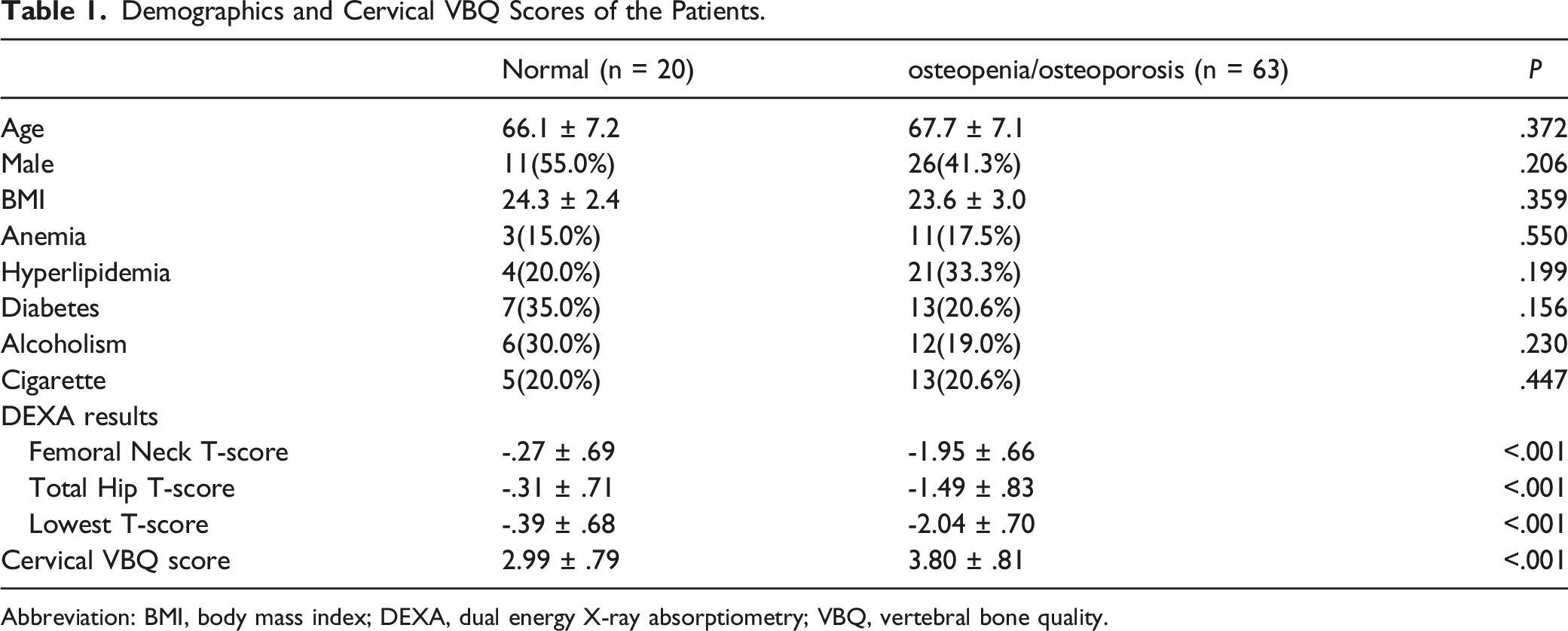
Abbreviation: BMI, body mass index; DEXA, dual energy X-ray absorptiometry; VBQ, vertebral bone quality.
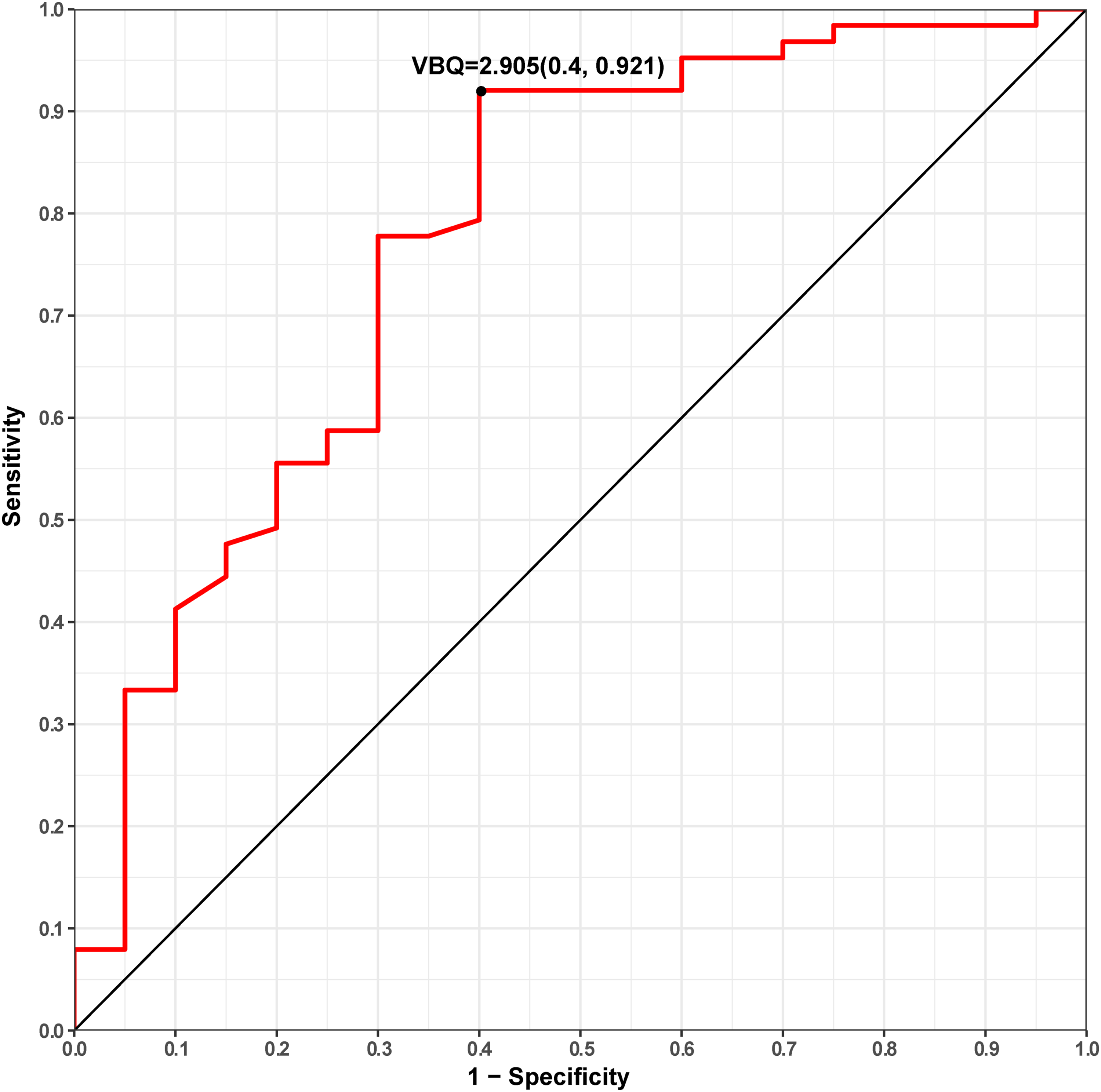
Receiver operating characteristic (ROC) curve showing the sensitivity and specificity.
Correlation Between the Cervical Vertebral Bone Quality Score and DEXA T-Score
Correlation between the Cervical VBQ Scores and DEXA T-Score.

Abbreviation: DEXA, dual energy X-ray absorptiometry; VBQ, vertebral bone quality.
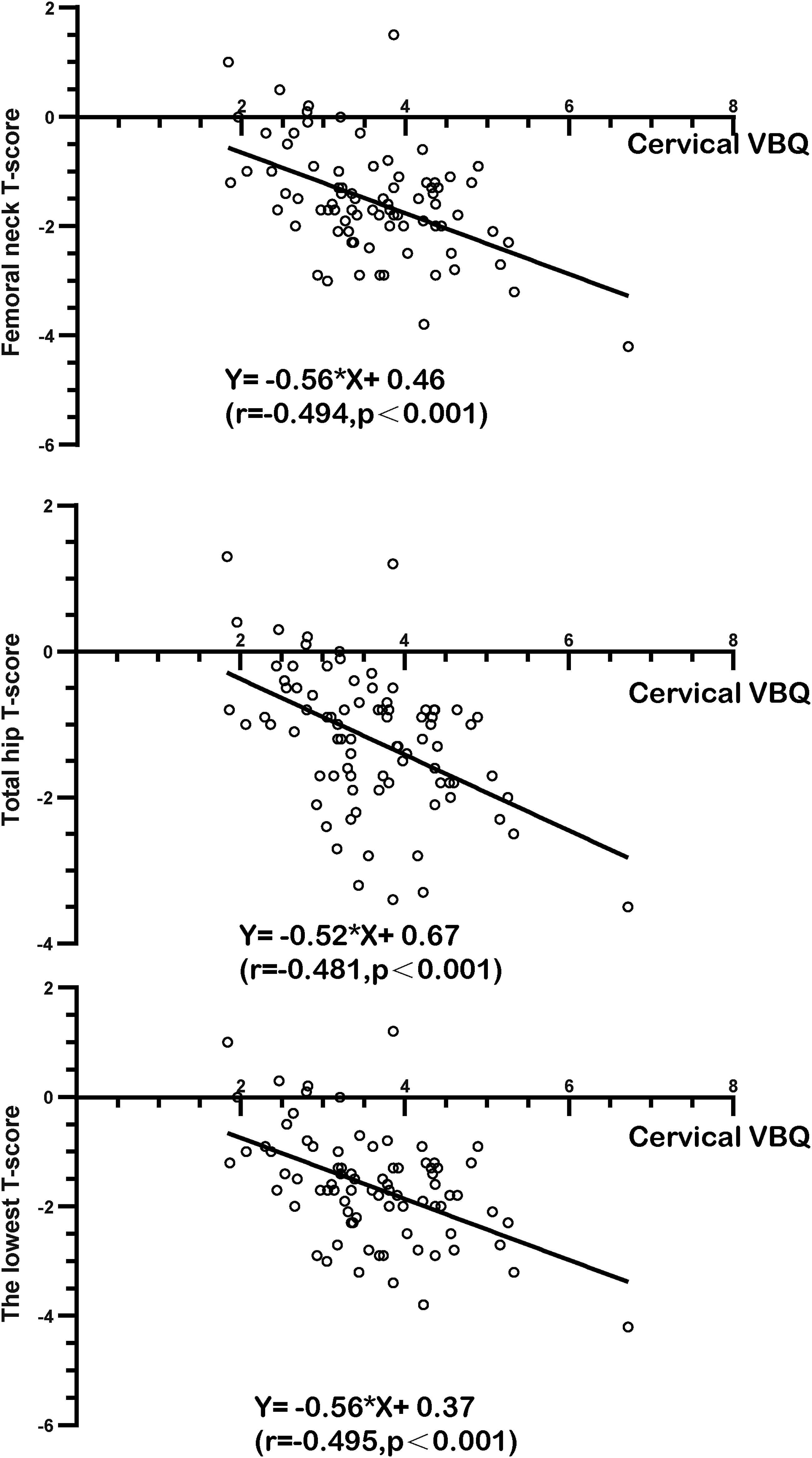
Linear regression and correlations between the cervical vertebral bone quality (C-VBQ) scores and DEXA T-Score.
Discussion
The evaluation of the bone quality has drawn increasing attention in spine surgery due to the worldwide social aging process. Low bone quality (osteopenia/osteoporosis) was found to be a risk factor leading to construct failure including screw pull-out and cage subsidence as the bony elastic modulus and strength decreased.21,22 Furthermore, former literature found that low bone mineral density was associated with slower and less reliable fusion.23-25 And the low bone quality was generally associated with a higher risk of fractures in various positions in human body under certain stress.
To achieve better surgical outcomes, proper evaluation on the bone quality could aid in determining medical management such as augmenting fixation using proper types of fixations or cement augmentation and applying perioperative osteogenic medicines.25,26 Although measuring the BMD has been recommended by guidelines and some spine surgeons, the gap between the initial guideline and actual adherence in practice existed.11,12 The inclusion process of the current study also reflected this phenomenon to some extent. On the one hand, the low adherence rate attributed to some surgeons’ lack of conception of preoperative BMD evaluation. On the other hand, this was potentially due to some intrinsic defects of DEXA method including requiring extra examination procedure, more radiological exposure, and higher medical cost. Meanwhile, some symptoms such as gait difficulty and limbs numbness caused by cervical degenerative diseases would increase the difficulty for some patients to receive the DEXA scan, decreasing their adherence to this exam. Further, the BMD can be overestimated because the DEXA measurement on lumbar spine might be affected by the vascular calcification, surrounding calcified tissue and spinal degenerative tissue, which are quite common in elder people undergoing spine surgery.13,27,28 Therefore, researchers have been exploring additional tools with simplicity and convenience.
The VBQ method was firstly developed by Ehresman et al based on the lumbar T1W MRI images very recently. 9 T1W images have been regarded as excellent diagnosis tool for the pathologic lesions of cancellous bone, which is the main region of hematopoiesis, mineral storage, remodeling and vascularization.5,29,30 The SI change on T1W images due to fatty infiltration of trabecular bone was the primary theoretical basis for method assessing BMD via T1W MRI such as M-score reported by Bandirali et al. 31 To address the issue that baseline differences in SI exist between various scanners, Ehresman et al innovatively applied the SI of CSF for standardization. Their initial research has proved a good accuracy of 81% of the method. And more recently, the method has been applied in many aspects in lumbar spine surgery and proved its satisfying efficacy on prediction of fragility fractures in at-risk patients, indicating bone quality in patients with degenerative disease or vertebral compressive fractures.4,9,13,17,18
However, there are no previous studies answering whether the VBQ method could be performed in cervical spine. To best of our knowledge, the current study is the first study to investigate and verify the application of modified VBQ technique before cervical spine surgery. We thought that a possible explanation towards this gap was that the uncertainty whether the CSF SI could be recorded in cervical spine MRI. Inspired by the result reported by Li et al. that the VBQ scores calculated by L2 CSF and L3 CSF were similar. 18 Due to a relatively homogeneous SI of CSF, 9 as an attempt, we chose the T1-level CSF as the target taking cervical spine anatomy into consideration as well. Our practice found that it was not that difficult to acquire the T1-level CSF by zooming the images and drawing ROI avoiding the spinal cord. The results in the current study also proved a significant correlation between the DEXA T-score and cervical VBQ with good inter-rater and intra-rater reliability. Possibly, the VBQ concept might be extended to be performed in thoracic spine in the future. More importantly, the AUC of the ROC curve indicated an overall accuracy over .78. By determining the cut-off value as 2.90, a sensitivity of .92 was found in the study. This sensitivity provided support for the application of the method on screening the patients with osteopenia and osteoporosis, helping surgeons decrease the risk and improve the surgical outcomes. These findings were comparable to the results reported by Ehresman et al based on lumbar spine MRI. 9 Admittedly, an altered cut-off could be determined according to the purpose of doctors during the clinical practice.
As described by previous studies, the VBQ method has several advantages with regard to its application in clinical practice.9,18 Because it was based on the data of MRI that most patients undergoing spine surgery would routinely receive before the surgery, it could lead to higher clinical screening rates in an economic-efficient and radiation-free way for patients. For surgeons, the method was easy to understand and perform using the PACS system, which broaden the application of the method. The case in Figure 2 could be taken as an instance, where the patient is a 64-year-old female lady without known medical record of osteoporosis. However, obvious fatty infiltration was found on T1W MRI and a high VBQ score of 5.56 indicated the low bone quality, which was later confirmed by femoral neck DEXA T-Score of -3.2. The successful identification of the poor bone quality provided evidence for us to adopt more fixation points and perioperative anti-osteoporotic medications. Last, from a theoretical aspect, the cervical VBQ score could have another superiority. For patients receiving spine surgery, it could perform better in reflecting the regional bone quality in cervical spine and could provide more accurate bone quality of the surgical field given that the DEXA T-score was acquired on lumbar spine or femur. Although this assumption was reasonable theoretically, it remains to be verified through further study.
We have to admitted that the current study has some limitations. First, as we stated in the Method part, we applied the elliptical tool to place the ROI region, but the tool has limit on its shape and direction so that more cancellous bone could be included by using more powerful ROI tool such as ImageJ software. But if more powerful ROI measurements such as manual-drawing polygon was used, the whole process might be more time-consuming and require extra software, which might affect the inter-rater and intra-rater reliability. Convenience and simplicity are advantages of the current VBQ method so this might be a trade-off for users between the simplicity and accuracy. Second, as Ehresman et al stated in their study, the current study focused on patients undergoing cervical spine surgery and this might lead to potential selection bias because patients with severe osteoporosis were less likely to be admitted to hospital for surgery. 9 Third, although the results of the study were comparable to its use in lumbar spine, all subjects involved in this study were Chinese, which could affect the generalizability of the study. Meanwhile, although the results of the study were satisfying, it should be noted that at present MRI scans were generally done in supine position so that the results might not entirely reflect the states in other positions. Last, despite that the science under the VBQ method is robust and a few papers from different institutions proved its efficacy, its application in cervical spine still requires future reconfirmation involving more institutions, larger sample size and clinical feedback when surgeons try the method.
Conclusion
In this study, we firstly modified and applied the VBQ method to assess the BMD in operative cervical spine patients based on the preoperative cervical spine MRI. The DEXA T-score of the femoral neck, total hip and the lowest DEXA T-score were found to be significantly correlated with the cervical VBQ score. A significant difference could be found between the cervical VBQ of patients with normal BMD and patients with osteopenia/osteoporosis. The ROC curve indicated that the cervical VBQ score can be a potential tool which is convenient and cost-effective for surgeons to screen the patients with osteopenia and osteoporosis based on the routinely available data of patients before the cervical spine surgery.
Supplemental Material
Supplemental Material - Preoperative Assessment of Bone Density Using MRI-Based Vertebral Bone Quality Score Modified for Patients Undergoing Cervical Spine Surgery
Supplemental Material for Preoperative Assessment of Bone Density Using MRI-Based Vertebral Bone Quality Score Modified for Patients Undergoing Cervical Spine Surgery by Weibo Huang, MD, Zhaoyang Gong, MM, Chaojun Zheng, MD, Yu Chen, MD, Xiaosheng Ma, MD, Hongli Wang, MD, and Jianyuan Jiang in Global Spine Journal
Supplemental Material
Supplemental Material - Preoperative Assessment of Bone Density Using MRI-Based Vertebral Bone Quality Score Modified for Patients Undergoing Cervical Spine Surgery
Supplemental Material for Preoperative Assessment of Bone Density Using MRI-Based Vertebral Bone Quality Score Modified for Patients Undergoing Cervical Spine Surgery by Weibo Huang, MD, Zhaoyang Gong, MM, Chaojun Zheng, MD, Yu Chen, MD, Xiaosheng Ma, MD, Hongli Wang, MD, and Jianyuan Jiang in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from Excellent Talent Training Award Program of Huashan Hospital, Fudan University.
Authors Note
All authors certify that this manuscript is a unique submission and is not being considered for publication, in part or in full, with any other source in any medium.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.