
Abstract
Study Design
Retrospective cohort study.
Objectives
To assess the impact of Enhanced recovery after surgery (ERAS) protocols on peri-operative course in adult cervical deformity (ACD) corrective surgery.
Methods
Patients ≥18 yrs with complete pre-(BL) and up to 2-year (2Y) radiographic and clinical outcome data were stratified by enrollment in an ERAS protocol that commenced in 2020. Differences in demographics, clinical outcomes, radiographic alignment targets, peri-operative factors and complication rates were assessed via means comparison analysis. Logistic regression analysed differences while controlling for baseline disability and deformity.
Results
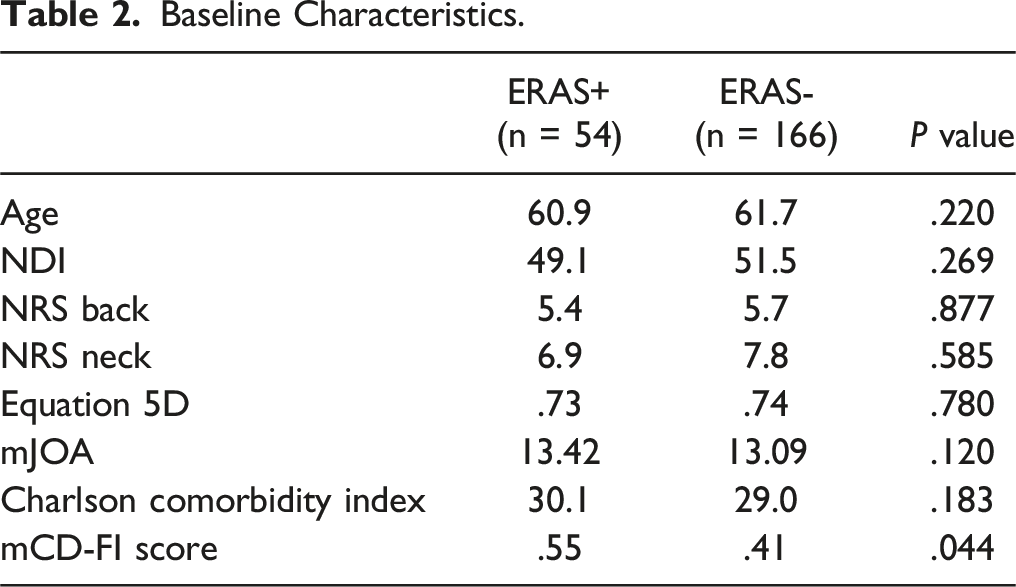
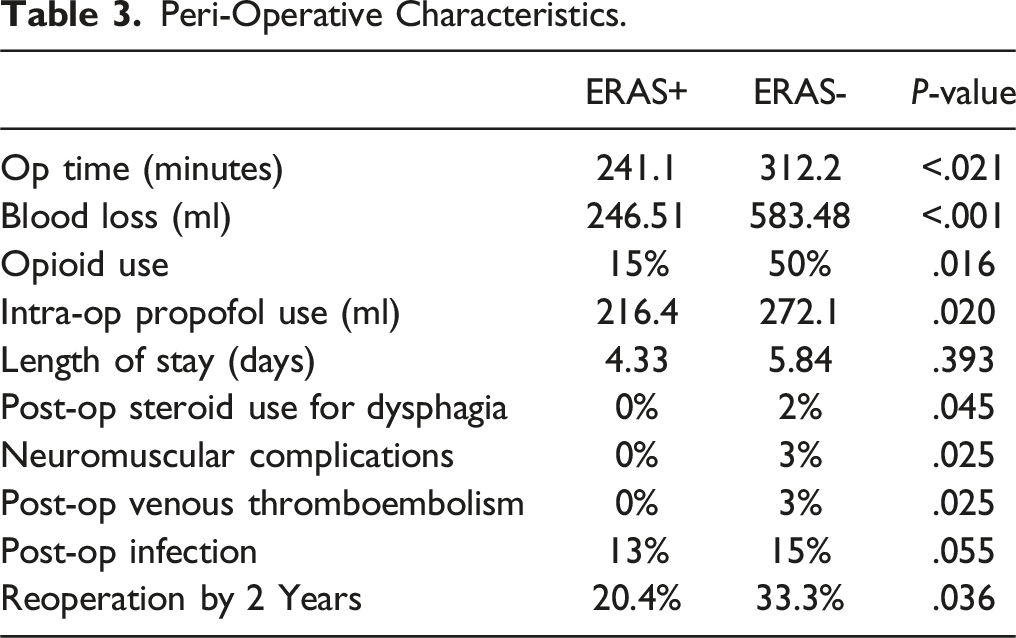
We included 220 patients (average age 58.1 ± 11.9 years, 48% female). 20% were treated using the ERAS protocol (ERAS+). Disability was similar between both groups at baseline. When controlling for baseline disability and myelopathy, ERAS- patients were more likely to utilize opioids than ERAS+ (OR 1.79, 95% CI: 1.45-2.50, P = .016). Peri-operatively, ERAS+ had significantly lower operative time (P < .021), lower EBL (583.48 vs 246.51, P < .001), and required significantly lower doses of propofol intra-operatively than ERAS- patients (P = .020). ERAS+ patients also reported lower mean LOS overall (4.33 vs 5.84, P = .393), and were more likely to be discharged directly to home (χ2(1) = 4.974, P = .028). ERAS+ patients were less likely to require steroids after surgery (P = .045), were less likely to develop neuromuscular complications overall (P = .025), and less likely experience venous complications or be diagnosed with venous disease post-operatively (P = .025).
Conclusions
Enhanced recovery after surgery programs in ACD surgery demonstrate significant benefit in terms of peri-operative outcomes for patients.
Introduction
Enhanced recovery after surgery (ERAS) protocols are a combination of pre and post-operative approaches to optimizing care with a multidisciplinary, multimodal lens that accelerates recovery after major surgery. 1 The idea of ERAS was first introduced in 2001, and applied to laparotomy procedures in general surgery, where it was shown to reduce post-operative pain and hospital length of stay (LOS). 2 Despite the introduction of ERAS in all major surgical fields, the efficacy of ERAS in the field of spine surgery, particularly in the context of adult cervical deformity (ACD) procedures has yet to be widely studied. 3 The goals of ERAS implementation include minimizing the surgical stress response, reducing LOS, decreasing post-operative complications and associated healthcare costs, and improving the overall patient experience. 4 With regard to spine surgery, the bulk of ERAS implementation and literature has focused on outcomes following lumbar spine procedures. 5 For example, Kim et al found that an ERAS pathway for patients undergoing thoracolumbar deformity surgery was associated with reduced LOS, without adverse collateral effects on short-term morbidity and complication. 6
Adult cervical deformity is a complex spinal condition that can cause significant disability, pain, and reduced quality of life. Correction of ACD involves extensive and invasive surgical intervention, with instrumentation and fusion to correct spinal alignment and improve stability. 7 These surgeries are known to have relatively high associated morbidity rates, prolonged hospitalization, significant postoperative pain, and elevated costs. 8 This may interfere with the suitability of ACD surgery to ERAS protocols. Nonetheless, given that ERAS has the potential to improve patient outcomes and satisfaction from a variety of different angles; such protocols could undoubtedly be beneficial to ACD patients. To our knowledge, no previous work has examined the deployment of ERAS protocols in a population of patients undergoing surgical correction for ACD. We hypothesized that patients treated using an ERAS protocol would have a lower hospital LOS, decreased peri-operative complications, and reduced pain requirements over the course of 2 years following surgery.
Methods
Data Source and Study Design
This is a retrospective study of a prospectively collected, single-center database involving ACD patients enrolled between 2012 and 2021. Institutional Review Board (IRB) approval was obtained prior to patient enrollment and all patients provided informed consent. The requirements for dataset enrollment and the means by which data were collected, stored and accessed have been published previously.9-11 This dataset has been used to examine various aspects of clinical care and health policy around the treatment of patients with ACD.9-11 The inclusion criteria for the present study investigation consisted of operative cervical deformity patients with complete radiographic and health related quality of life (HRQL) data collected preoperatively and at 2-years postoperatively.
Data Collection and Radiographic Assessment
Standardized data collection forms assessed patient demographics, surgical parameters, and comorbidities at initial presentation. Health related quality of life metrics were collected via patient surveys at baseline and at multiple scheduled follow-up time points. HRQL measures consisted of the Neck Disability Index (NDI), Numeric Rating Scale for the Neck (NRS-Neck), Numeric Rating Scale for the Back (NRS-Back), Euro-QOL 5-Dimension Questionnaire (EQ5D) and modified Japanese Orthopaedic Association (mJOA) assessment. In this work, we set the minimally clinically important difference (MCID) for the mJOA at 2 based on published values. 12 The MCID for Neck Disability Index was set at 15; double the published MCID value because our NDI score was collected on a 0-100 scale as opposed to 0-50. 13 The EQ-5D MCID was set as .1 in line with previous publications.14,15
Lateral spine radiographs were used to assess radiographic parameters at baseline and at scheduled follow-up intervals. All images were analyzed with SpineView® (ENSAM, Laboratory of Biomechanics, Paris, France).16-18 Spinopelvic radiographic parameters assessed included pelvic tilt (PT: the angle between the vertical and the line through the sacral midpoint to the center of the 2 femoral heads), the mismatch between pelvic incidence and lumbar lordosis (PI-LL), and the sagittal vertical axis (SVA: C7 plumb line relative to the posteriosuperior corner of S1). Cervical spine parameters assessed included cervical lordosis [C2-C7 angle], T1 slope [T1S], McGregor’s Slope [MGS], and chin-brow vertical angle [CBVA].
Classification of Cervical Deformity
Preoperative cervical deformity severity was assessed using the Ames CD classification. This system consists of a cervical deformity descriptor that identifies the apex of the deformity, and 5 modifiers. 19 Patients were assigned a cervical deformity descriptor based on radiographic review and were stratified by deformity severity for each of the 5 modifiers.
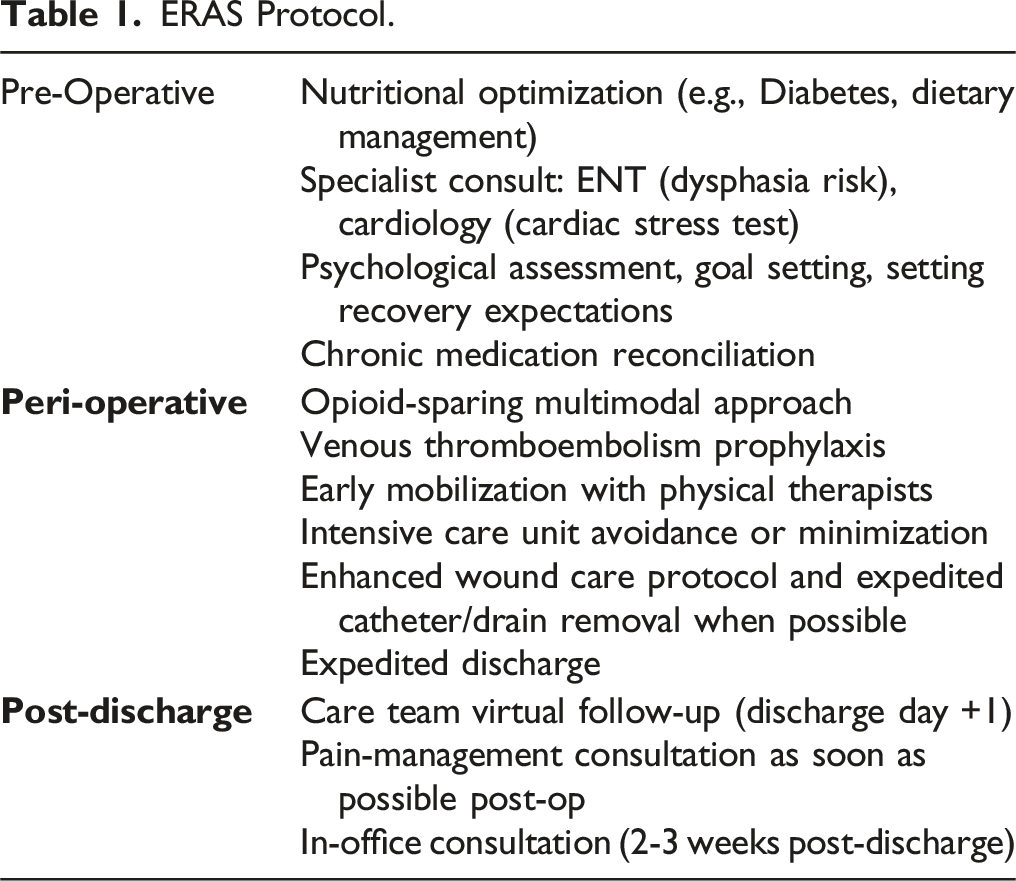
Cohort Selection and ERAS Protocol
ERAS Protocol.
Statistical Analysis
Collected data were assessed via means comparison analyses with regards to demographics, clinical data, complications, and health-related quality of life metrics. The primary outcomes were LOS, peri-operative complications and pain medication requirements. Logistic regression analyses controlling for baseline deformity and disability were used to analyze differences between patients, with the incorporation of ERAS protocols within treatment as the primary predictor. Statistical analyses were performed using SPSS 24.0 software (IBM, Armonk, NY). Statistical significance was set at .05.
Results
Cohort Overview
Baseline Characteristics.
Surgical Descriptors
In terms of surgical characteristics, mean levels fused were 5.3 ± 3.3, mean estimated blood loss (EBL) was 733.3 ± 820.5 mL, and mean operative time was 337.7 ± 201.4 min. By surgical approach, 18.1% of patients underwent anterior-only approach, 49.3% posterior-only, and 31.3% combined. The most common upper instrumented vertebra (UIV) was C3 and most common lower instrumented vertebra (LIV) was T1. 67.4% of patients underwent an osteotomy as part of their index procedure. Surgical approach (anterior, posterior or combined) was similar between ERAS+ and ERAS-. There were no differences between both groups with regards to minimally-invasive screw fixation (ERAS+ 53% vs ERAS- 48%, P = .052).
Cervical Deformity Severity and Ames Classification
Preoperatively, Ames modifier breakdown by severity was as follows: For cSVA, 88.1% of the cohort were non-pathologic, while 11.9% had a moderate deformity. By TS-CL, 25.4% of patients had no deformity, 11.6% had moderate deformity, and 63.0% had a severe deformity. Examining the Horizontal Gaze modifier, 21.1% had no deformity, 52.1% moderate deformity, and 26.8% severe deformity. By SVA, 91.8% of patients were non-pathologic and 8.2% had severe deformity. By myelopathy severity (as measured via mJOA score), 9.7% of the cohort had no myelopathy, 26.2% had mild, 35.0% had moderate, and 29.1% had severe myelopathy.
Peri-Operative Differences: ERAS+ vs ERAS-
Peri-Operative Characteristics.
Complications Analysis
In terms of complications, ERAS+ patients were less likely to require steroids after surgery (OR: .33, 95% CI: .25-.6, P = .045) for radiculopathy or postoperative pain, were less likely to develop neuromuscular complications overall (OR: .2, 95% CI: .1-.5, P = .025), and less likely to experience venous complications or be diagnosed with venous disease post-operatively (P = .025).
Discussion
Enhanced recovery after surgery protocols have gained significant attention in recent years as a standardized approach to improve peri-operative outcomes in patients undergoing major surgery. The current study expands upon our understanding of ERAS implementation in spine surgery, specifically in patients undergoing corrective surgery for ACD. Our study demonstrates that the application of ERAS in patients undergoing surgery for ACD is associated with meaningful reductions in pain and opioid utilization, complications, operative time, and hospital LOS. Our work is the first we are aware of to demonstrate the positive benefits of ERAS implementation in a series of patients undergoing complex correction of ACD.
ERAS+ patients at baseline had lower rates of opioid utilization. Spine surgery has been rated as one of the most painful procedures, and the risk of chronic pain and postoperative opioid utilization and dependence is a significant issue. 20 Integral to an effective ERAS protocol is pre-operative counseling and education regarding pain control. Education on the risks and benefits of opioid use, the importance of using them sparingly and only when acutely necessary should be communicated to the patient at length. Additionally, multimodal analgesia is a key component of ERAS protocols. 21 Enhanced recovery after surgery protocols emphasize the routine use of multimodal analgesic regimens to improve pain control and reduce opioid consumption, consisting of such regimens as acetaminophen, COX-2 inhibitors, gabapentin, muscle relaxants, local anesthetic infusion (epidural or intravenous), and lower morphine-milligram-equivalent opioids. 22 The use of such modalities in our study helped reduce post-operative pain and reduce opioid consumption. Many studies have demonstrated that patients with a history of chronic opioid use experience a greater severity of acute pain and slower post-operative resolution of pain.22-24 Addressing pain and decreasing opioid utilization post-op cannot be overstated, as higher pain scores affect long term HRQL measures, cause decreased satisfaction, and further contributes to the ongoing opioid epidemic. 25 Smith et al studied an ERAS program on lumbar spine fusion patients and found that multimodal analgesia as part of the ERAS pathway had a significant decrease in postoperative opioid and rescue antiemetic use. 24 Chang et al also found that patients who received multimodal pain therapy as part of a standardized ERAS undergoing lumbar fusion had a significant decline in the consumption of opiates post-operatively. 26
Patients enrolled in the ERAS protocol experienced a shorter hospital LOS and were more likely to be discharged home. A shorter LOS signifies a quicker recovery from surgery, generally means that the patient tolerated the procedure well, and imparts cost savings to both the patient and hospital system. Debono et al investigated selected patients before and after ERAS protocol implementation for anterior cervical decompression and fusion, and found that LOS was significantly reduced after ERAS implementation, with no increase in rates of readmission or major complications. 21 This is in accordance with our current study. Structured and detailed counseling preoperatively, including expectation management and planning for safe discharge prior to the surgery were key components of our protocol. Smith et al similarly compared patients before and after implementation of an ERAS program and contrary to our study, found that there was no significant difference in postoperative pain scores or hospital LOS between groups. 24 They also measured compliance with post-operative ERAS principles including early ambulation with physical therapy, and early foley catheter removal, and found that compliance was poor. This could certainly account for the nonsignificant findings, given that physical therapy and post-operative mobilization are keystones of early discharge home and decreasing LOS.
A shorter LOS and higher proportion of patients being discharged home in the ERAS+ cohort is likely attributable in part to the role of physical therapy in the ERAS protocol, which emphasized early ambulation in conjunction with pre-operative counseling on the importance of rapid post-op mobilization. 27 Though our study did not measure ambulation distances with physical therapy, patients in their ERAS+ group were discharged home significantly earlier, and anecdotally noted to ambulate over greater distances once discharged home. Patients should be encouraged to mobilize as soon as they are able, in order to counteract the stress responses and adverse physiologic effects associated with surgery and subsequent prolonged bed rest. 28 Such responses include increased insulin resistance, muscle atrophy, reduced pulmonary function, impaired tissue oxygenation and increased risk of venous thromboembolism. 21 For lumbar fusion patients specifically, Ferrel et al found that patients ambulating at least 30 feet on post-operative day 0 had a significant reduction in hospital LOS. 29
Our study also demonstrated that ERAS+ patients experienced less peri-operative complications. Complications after ACD surgery include dysphagia, recurrent laryngeal nerve palsy, respiratory insufficiency, radiculopathy, and hematoma. 30 Oropharyngeal dysphagia and airway edema are the most common complications following ACDF surgery. 31 Studies have found a significant effect of dexamethasone on improvement of swallowing function and decreased airway edema perioperatively.32,33 It is impressive therefore that ERAS+ patients had both decreased post-operative complications including airway edema and dysphagia, and were less likely to require peri-operative dexamethasone. It is possible that the reduction in post-operative complications may be attributable to peri-operative and intra-operative aspects of the ERAS protocol. One of the tenets of ERAS protocols is the inclusion of minimally invasive surgical (MIS) techniques wherever possible. Minimally invasive surgical techniques can be beneficial in minimizing damage to adjacent muscular and neurovascular structures, which can potentially reduce risk of airway edema, vascular injuries, and overall post-operative complications. 34 The MIS technique espoused by ERAS protocols can also account in part for the significant differences in intra-operative aspects of ERAS+ patients shown in our study, including reduced propofol use, decreased blood loss, and decreased operative time.
Enhanced recovery after surgery protocols also incorporate prophylactic measures to counter post-operative venous complications such as deep venous thrombosis or wound haematomas. The use of compression stocking devices and routine administration of low molecular weight heparin intra- and post-operatively were used in ERAS+ patients, similar to previous studies.22,35 Additionally, shorter operative times, minimally invasive techniques, and pre-operative optimizing all help to reduce the risk of post-operative venous complications.
Enhanced recovery after surgery protocols emphasize the importance of managing body homeostasis during surgery, including managing blood loss, normovolemia, and normothermia; in order to decrease the risk of peri-operative complications.22,36 Managing fluctuations in blood pressure and decreased operative times help to account for the decreased propofol use in our study. Reductions in operative times seen in our study are in accordance with numerous studies on ERAS protocols in spine surgeries.4,34 The reason for decreased operative times is likely multifactorial regarding ERAS implementation and decreased operative time itself can help to explain the reductions in LOS, complications, decreased blood loss, and decreased propofol use seen in our study.
We appreciate limitations inherent to the current work. Foremost, this is a retrospective study with potential for selection and indication bias that cannot be fully addressed or controlled for even with the current study design. With the single-center patient population used in this study, there may also be indiscernible factors influencing peri-operative outcomes, including clustering at the provider and institutional levels. There is also an aspect of a restricted sample, given that just ∼25% of our substrate population was treated using an ERAS protocol. It also remains difficult to accurately assess the magnitude of pre-operative opioid use because of the high variability of dosing regimens and vagaries around reported use at the level of the individual. Given these shortcomings, our findings should be viewed as both proof of concept and instructive to current clinical practice. Further validation in larger samples with more robust clinical variation and exhaustive data collection is necessary to validate our putative results and a pre-requisite to more definitive recommendations.
Conclusions
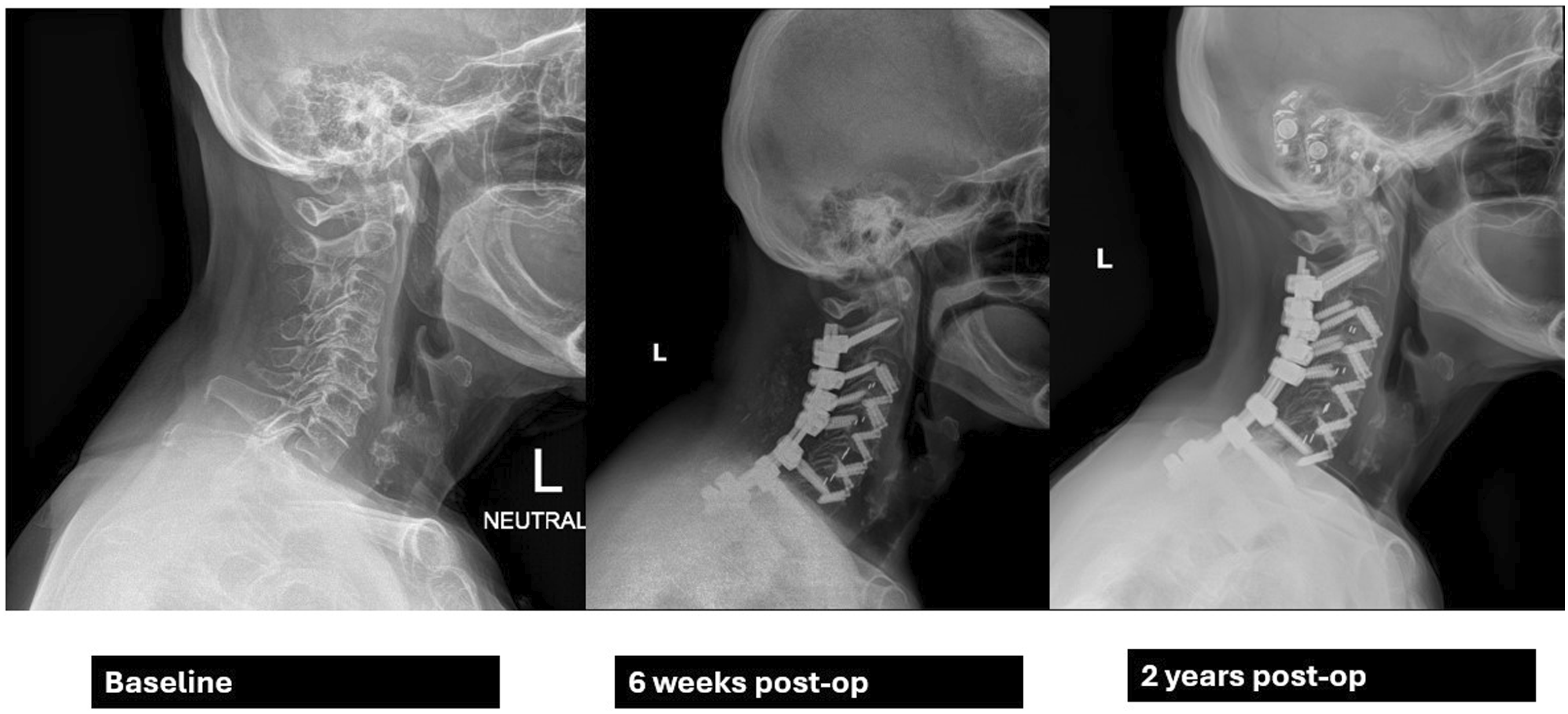
Enhanced Recovery After Surgery programs in ACD surgery demonstrate substantive benefits in terms of lower operative times, reduced LOSs, diminished opioid requirements and anesthetic dosing, as well as lower rates of post-operative morbidity. For ERAS-eligible patients, such protocols appear to have a positive impact on patient HRQL, clinical outcomes, and healthcare costs in the context of high-intensity invasive procedures such as ACD corrective surgery (Figure 1 and 2). 63 year old man. History of right-sided neck pain and spasms after sustaining work-related injury 6 years prior. Symptoms were unresolved with conservative measures and progressively worsened with time, leading to spondylolisthesis and C7-T1 herniation. The patient was unable to undergo ERAS protocols due to severity of symptoms and moderate-to-severe frailty. Underwent C3-C7 ACDF, C3 and C6-T1 partial corpectomy, C4 & C5 corpectomy, and C3-T1 posterior cervical fusion, and was discharged 8 days post-op. He continued to use opioids intermittently. At 2 years post-op he was displaying signs of distal junctional kyphosis and had redeveloped pain symptoms. 74 year old female progressive, atraumatic severe neck pain with radiation into right upper extremity and right upper limb weakness. Patient undertook full ERAS protocols, and underwent C3-C7 ACDF, partial corpectomy C3-C7 and C2-T2 posterior cervical fusion, and was discharged 3 days post-op. Also underwent interval L5-S1 ALIF with L2-Pelvis posterior fusion. Patient reported discontinuing opioids 3 days after discharge. At 2 years post-op, radiographic alignment was still maintained without evidence of DJK.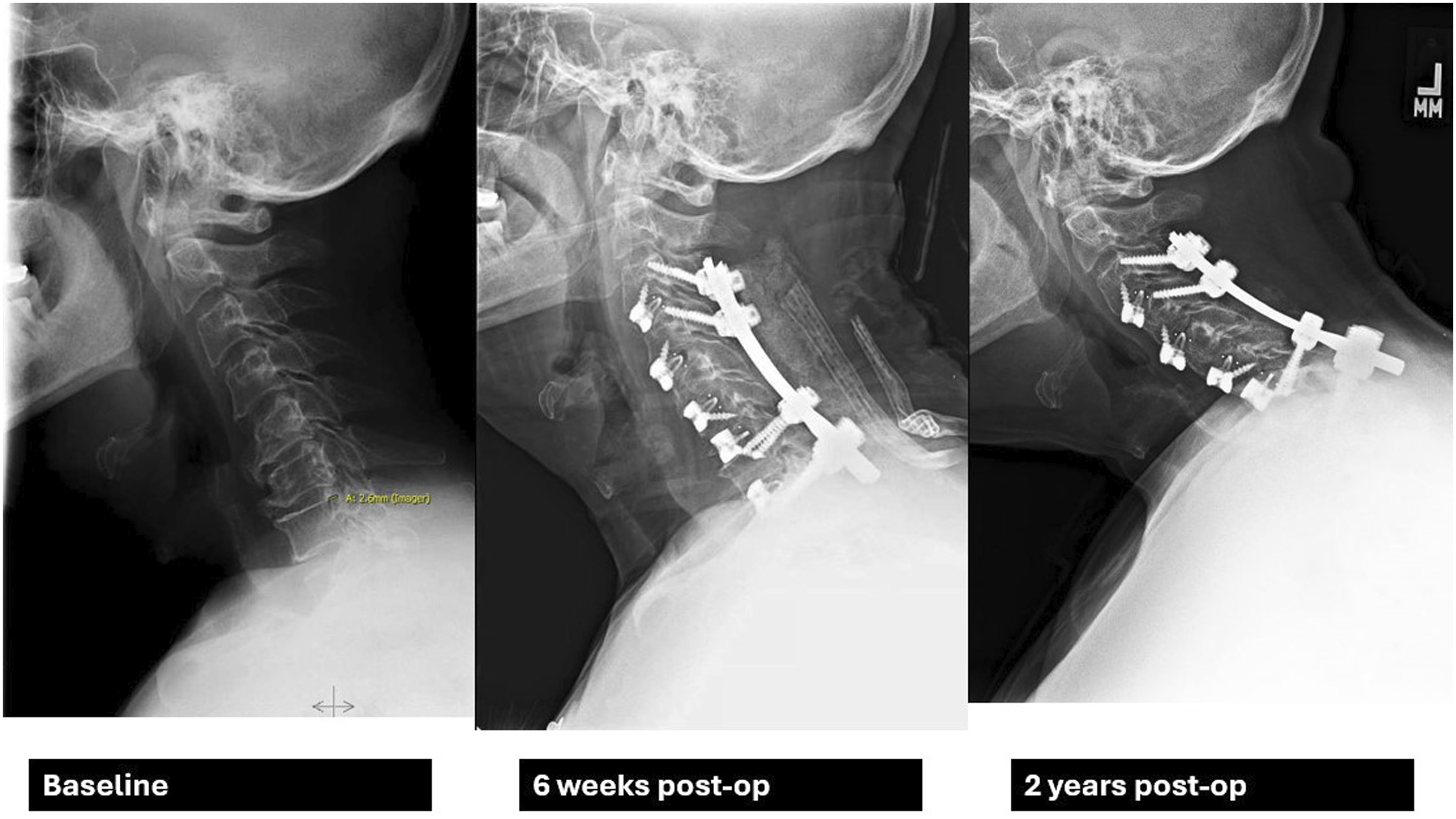
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
Informed Consent
Informed consent was obtained from each patient prior to enrollment.