
Abstract
Study Design
Systematic review and meta-analysis.
Objective
Poor bone quality is a major risk factor for complications after cervical spine surgery. The MRI-based cervical vertebral bone quality (C-VBQ) score is a reliable tool for assessing bone quality. This study systematically evaluates, for the first time, the predictive value of C-VBQ for cage subsidence risk in cervical spine surgery patients using meta-analysis.
Methods
We conducted a comprehensive search of relevant literature in electronic databases up to October 16, 2024, to systematically assess the quality of included studies. Publication bias was evaluated by comparing C-VBQ between groups and calculating pooled sensitivity, specificity, and summary receiver operating characteristic (SROC) curves.
Results
7 studies involving 681 patients were included. Using the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) tool, the studies were deemed high quality with low risk of bias. High C-VBQ scores were significantly associated with fusion subsidence, with a pooled odds ratio of 2.98 (95% CI: 1.68-5.30). The C-VBQ cut-off value was 2.94 ± 0.32, and the combined sensitivity and specificity for diagnosing postoperative complications were 0.78 and 0.87, respectively, with an area under the curve of 0.90 (95% CI: 0.87-0.92).
Conclusion
In patients undergoing degenerative cervical spine surgery, higher C-VBQ scores were significantly associated with an increased risk of cage subsidence. The C-VBQ score is a reliable tool for preoperative bone quality assessment and serves as an independent predictor of cage subsidence risk following cervical spine surgery.
Keywords
Introduction
Anterior cervical discectomy and fusion (ACDF) and anterior cervical corpectomy and fusion (ACCF) are common treatments for cervical spondylosis, primarily aimed at decompressing the spinal cord by removing intervertebral discs and bone remnants.1-3 However, poor preoperative bone quality may increase the risk of instrumentation-related complications, with cage subsidence being the most prevalent. 4 The incidence of reduced bone quality or osteoporosis has been reported to be as high as 65.2% among patients undergoing spinal fusion surgery. 5 Consequently, accurate preoperative assessment of bone quality is widely recognized as essential for preventing postoperative complications, guiding rehabilitation, and promoting early functional recovery. 4
Dual-energy X-ray absorptiometry (DXA) is widely used by orthopedic surgeons to assess preoperative bone quality in the spine. 6 However, a survey of over 100 spine surgeons indicated that only 44% of patients routinely underwent DXA before spine surgery. 7 Recently, Ehresmann et al. 8 proposed an MRI-based vertebral bone quality (VBQ) score as an alternative to DXA, with numerous studies confirming significant correlations between VBQ scores, DXA T-scores, and quantitative CT (QCT) bone mineral density (BMD) values.9-11 Subsequently, Soliman et al. 12 developed the cervical VBQ (C-VBQ) based on the lumbar VBQ score, which has shown significant correlation with the lumbar VBQ and demonstrated predictive value for postoperative cage subsidence in cervical spine surgery patients.13-15
However, the predictive value of the C-VBQ score for the risk of postoperative cage subsidence has not been systematically evaluated. This study therefore conducted a comprehensive meta-analysis to assess the role of C-VBQ in predicting postoperative cage subsidence in patients undergoing cervical spine surgery, providing a scientific basis for its clinical application.
Materials and Methods
Search Strategy and Screening
We conducted a comprehensive literature search (up to October 16, 2024) across the English-language databases PubMed, Embase, and Web of Science, as well as the Chinese-language databases China National Knowledge Infrastructure (CNKI) and China Biology Medicine (CBM). This systematic review targeted original studies investigating C-VBQ scores as predictors of fusion subsidence following degenerative cervical spine surgery. Our search strategy included the keywords: vertebral bone quality, VBQ, vertebral bone quality score, VBQ score, bone quality, subsidence, cage subsidence, magnetic resonance imaging, MRI, cervical, and spine.
After excluding duplicates, 2 authors independently screened all studies by title and abstract, followed by a full-text review of potentially eligible studies for further assessment. Disagreements were resolved through discussion until a consensus was reached. Clinical studies examining the effect of the C-VBQ score on cage subsidence after cervical spine fusion were included. Studies were excluded if they met any of the following criteria: study design unrelated to assessing C-VBQ’s effect on cage subsidence, focus on lumbar or thoracic VBQ, incomplete outcome data, or review articles.
Currently, there is no universally accepted definition or standardized method for calculating cage subsidence in the cervical spine. 16 Most studies define cage subsidence as a loss of ≥3 mm in the height of the fused segment.12,14,15,17
C-VBQ Score Measurements
The C-VBQ score was calculated according to the method described by Soliman et al..
12
Appropriate regions of interest (ROIs) were placed in the C3-C6 vertebrae and the C2 cerebrospinal fluid (CSF) in the median sagittal image of the non-contrast T1-weighted MRI of the cervical spine, as shown in the sagittal slices in Figure 1. The mean signal intensity (SI) within each ROI was recorded, and the C-VBQ score was subsequently calculated by dividing the SI of the C3-C6 vertebrae by the SI of the C2 CSF, using the following formula: Example of measurement of C-VBQ score based on sagittal unenhanced T1-weighted MRI of the cervical spine with a measured C-VBQ score of 2.96.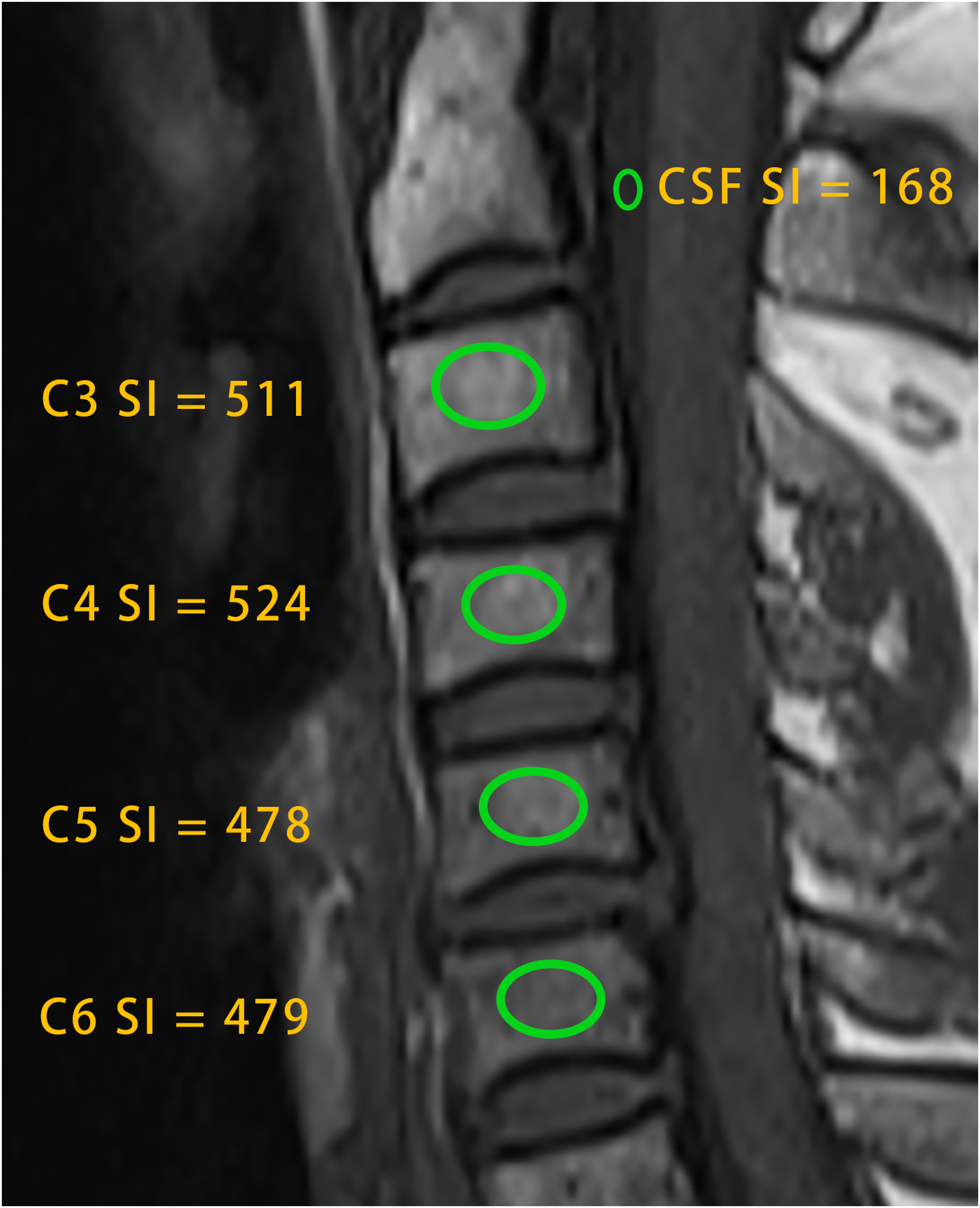

The calculation principle of the C-VBQ score is similar to that described in the original study by Ehresmann et al.. 8 Specifically, the degree of fat infiltration in trabecular bone of osteoporotic patients is correlated with increased MRI T1 SI. 18 Due to inherent signal differences across various MRI devices, CSF was chosen as the reference standard for VBQ scoring. CSF provides a stable and homogeneous signal, which effectively minimizes the bias caused by device-specific signal variations. 8 By using the CSF signal to calibrate the vertebral SI, baseline signal differences can be accounted for, ensuring the accuracy of the scoring method. 19
It is important to note that the C3-C6 vertebrae have limited space anterior to the spinal cord, as well as potential pathological factors (eg, disc herniation), 12 which may introduce signal heterogeneity. In contrast, the CSF space at the C2 level is more stable and consistent, facilitating precise placement of ROIs and providing a reliable signal reference.
Data Extraction
Two authors comprehensively reviewed all publications, focusing on study design, quality assessment, and outcome data. In cases of disagreement, a third author was consulted to ensure consistency. Outcome data included the incidence of cage subsidence, the odds ratio (OR), and the number of true-positive, false-positive, false-negative, and true-negative cases for diagnosing cage subsidence, as well as mean C-VBQ scores for group comparisons. Logistic regression analysis was used to calculate ORs with 95% confidence intervals. To assess the validity of C-VBQ as a diagnostic tool, an experimental group (patients who developed cage subsidence) was compared with a control group (patients who did not develop subsidence).
Assessment of Methodological Quality
We employed the Quality Assessment of Diagnostic Accuracy Studies 2 (QUADAS-2) tool to systematically evaluate the methodological quality of the included studies. 20 This tool is designed to identify major sources of bias in test accuracy evaluations and focuses on 4 key domains: patient selection, index test, reference standard, and flow and timing. A risk-of-bias assessment was conducted for each of these domains. Two lead authors independently performed the assessment, with a third author consulted to resolve any disagreements. Responses to the fourteen core questions were recorded as “yes,” “no,” or “unclear.” A “yes” response to all signaling questions within a domain indicated a low risk of bias, whereas a “no” response to any signaling question suggested potential bias. The “unclear” option was used only when data were insufficient to make a definitive judgment.
Statistical Analysis
All data were analyzed using RevMan 5.4.1 (Thomson Research Soft, Carlsbad, CA, USA) and Stata 17.0 (Stata Corp., College Station, TX, USA). For continuous variables, the mean ± standard deviation was reported, and OR with 95% confidence intervals (CI) were used to calculate the pooled risk of complications. Heterogeneity was assessed using chi-square and I2 tests. Subgroup and sensitivity analyses were also conducted to explore potential sources of heterogeneity. The following parameters, along with their 95% CIs, were calculated: sensitivity, specificity, positive likelihood ratio (PLR), negative likelihood ratio (NLR), diagnostic odds ratio (DOR), and the area under the curve (AUC) of the pooled summary receiver operating characteristic (SROC) curve. The optimal diagnostic cut-off value was determined based on the Youden index. Publication bias was assessed using Deeks’ funnel plot, with P < 0.05 indicating statistical significance.
Results
Characteristics of the Included Studies
Figure 2 illustrates the step-by-step literature review process. Based on the inclusion and exclusion criteria, we ultimately included 7 retrospective cohort studies, with patient characteristics detailed in Table 1. Five studies were conducted in China, and 2 were conducted in the United States, with a total of 681 patients enrolled (212 of whom experienced cage subsidence). The mean patient age was 55.09 years, 50.5% of patients were female, and the mean body mass index (BMI) was 24.72 kg/m2. ACDF was performed in 5 studies,12,14,21-23 while ACCF was performed in the remaining 2 studies.15,17 These studies used 3 different types of cage, which could be potential sources of heterogeneity: the cervical plate system (CPS),12,23 the zero-profile cage (ZPC),21,22 and the titanium mesh cage (TMC).15,17 Step-by-step literature review procedure. Characteristics of the Including Studies.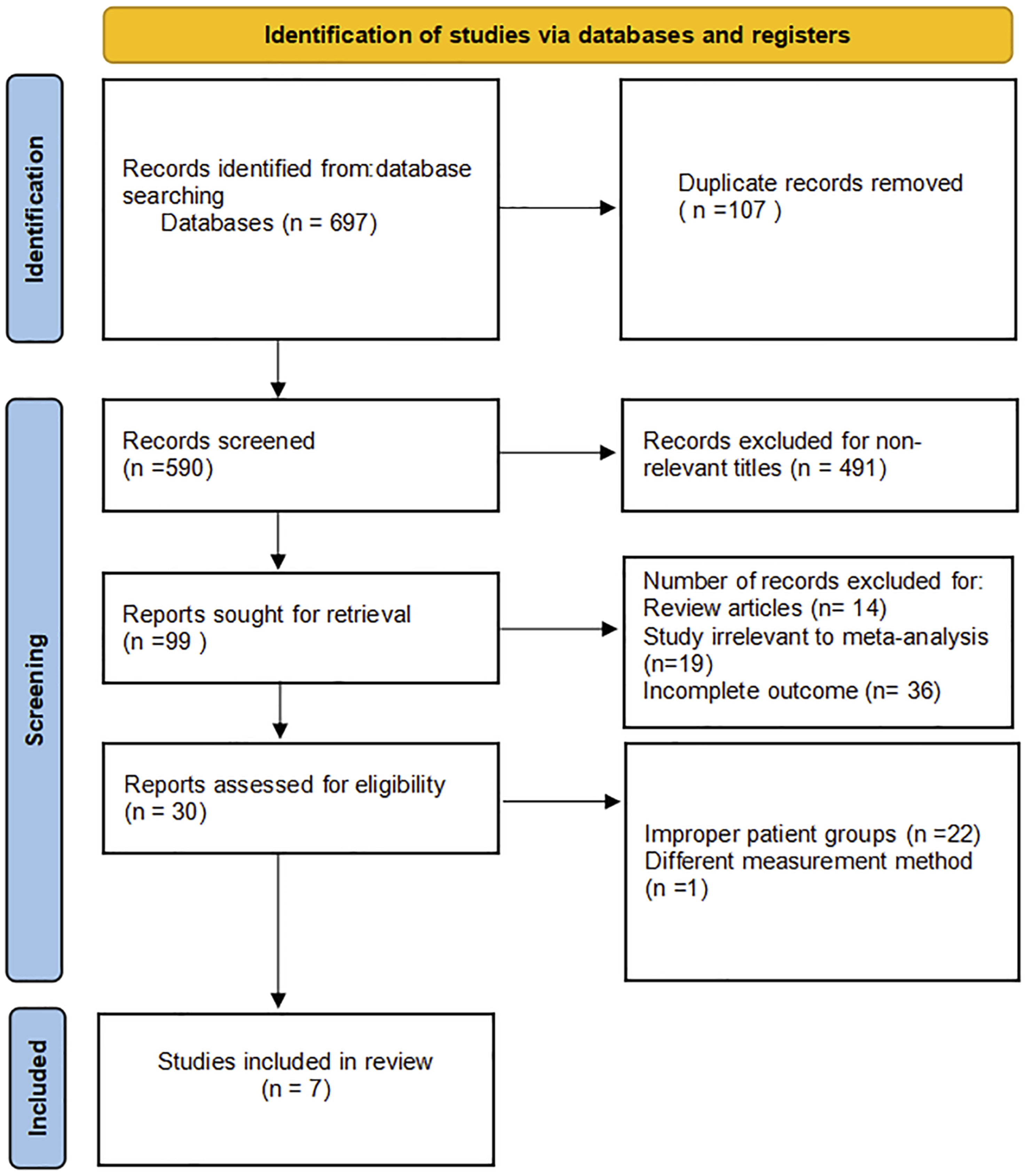

Quality of the Included Studies
A graphical summary of the methodological assessment using the QUADAS-2 tool based on 7 studies is presented in Figure 3(A)and(B). Most studies demonstrated a low risk of bias in terms of patient selection, index test, reference standard, and flow and timing. Some studies did not provide sufficient information to assess how the experimental outcomes were interpreted against the gold standard, resulting in potential bias. Overall, the studies included in this meta-analysis had low concerns regarding applicability. QUADAS-2 quality assessment; A represents the overall result; B represents the results of individual studies.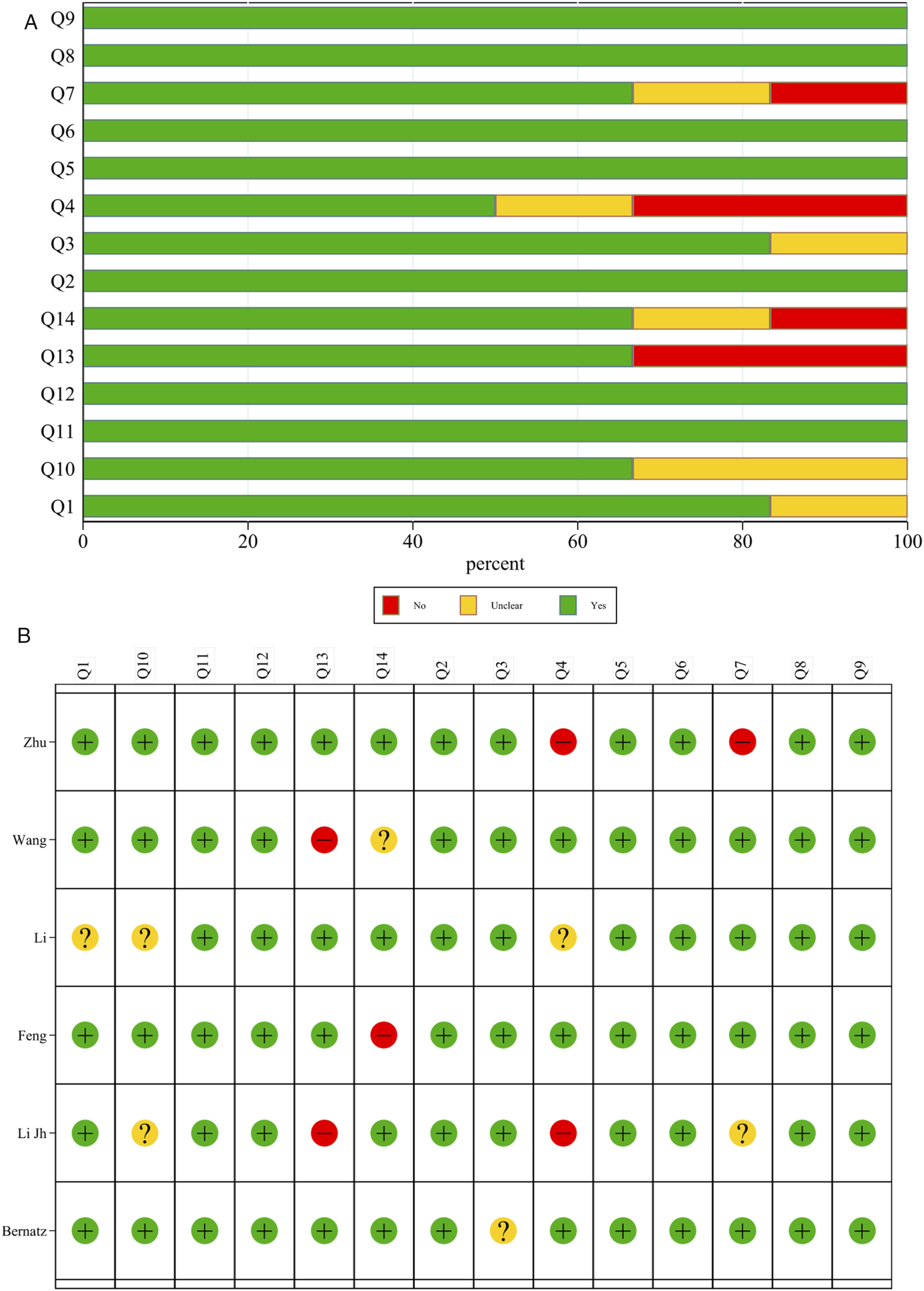
Control of Confounding Factors in Cage Subsidence
Of the 7 original studies included, 5 controlled for confounding factors that may influence cage subsidence through multifactorial logistic regression analysis. Specifically, 3 studies included age, gender, smoking history, and surgical segment as confounders in their analyses12,15,21; 1 study considered age, cage tilt angle, and placement depth 17 ; and another controlled for age alone. 22 The remaining 2 studies did not incorporate C-VBQ in their multifactorial analysis.14,23 Additionally, some studies performed univariate analyses of follow-up time17,21,22 and fusion status17,21 without controlling for confounders. Only 1 study noted that the procedure was performed by an experienced spine surgeon. 17
C-VBQ Scores Were Higher in the Postoperative Cervical Cage Subsidence Group
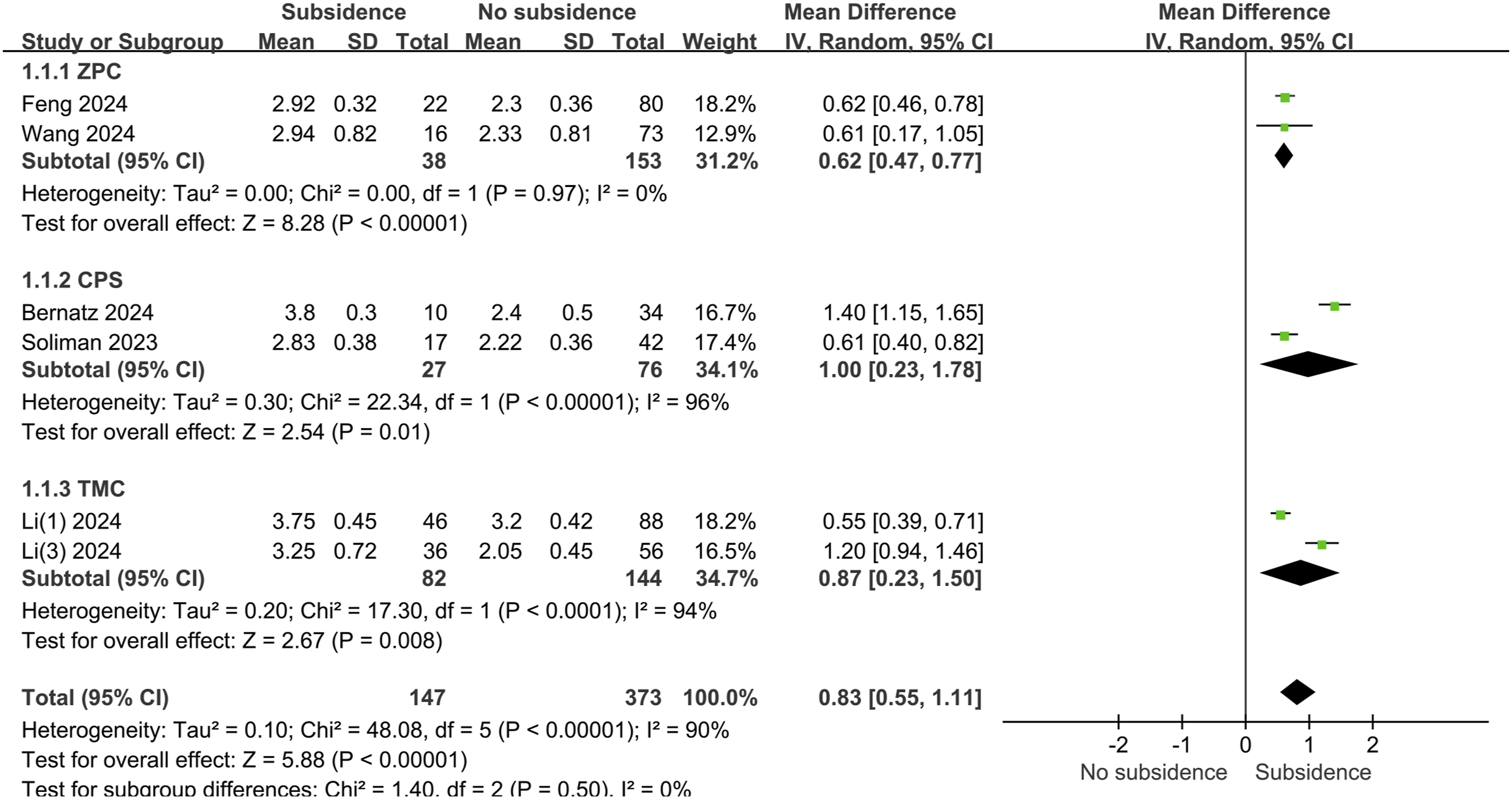
As shown in Figure 4, cage subsidence was reported in 7 studies, comprising a total of 681 patients. The overall incidence of cage subsidence was 31.1% (212/681). VBQ scores were significantly higher in the subsidence group compared to the control group (mean difference, 0.85; 95% CI, 0.61-1.09; P < 0.001; I2 = 89%; random-effects model). In a subgroup analysis by surgical approach, 2 studies investigated ACCF, involving 226 patients. The overall incidence of postoperative cage subsidence was 36.3% (82/226), and C-VBQ scores were significantly higher in the subsidence group compared to the control group (mean difference, 0.87; 95% CI, 0.23-1.50; P < 0.001; I2 = 94%; random-effects model). Two studies involving ACDF included 455 patients, with a postoperative subsidence rate of 28.6% (130/455), and C-VBQ scores were significantly higher in the subsidence group compared to the control group (mean difference, 0.85; 95% CI, 0.56-1.14; P < 0.001; I2 = 88%; random-effects model). No differences were observed between subgroups (P = 0.96, I2 = 0%), indicating that the surgical approach had no significant effect on VBQ scores. Additionally, a subgroup analysis of different cage types, as shown in Figure 5, revealed no significant differences between the cages (P = 0.50). Forest map of vertebral quality scores analyzed by type of surgery. SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom; ACDF, anterior cervical discectomy and fusion; ACCF, anterior cervical corpectomy and fusion. Forest map of vertebral quality scores analyzed by cage type. CPS, cervical plate system; ZPC, zero-profile cage; TMC, titanium mesh cage; SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom.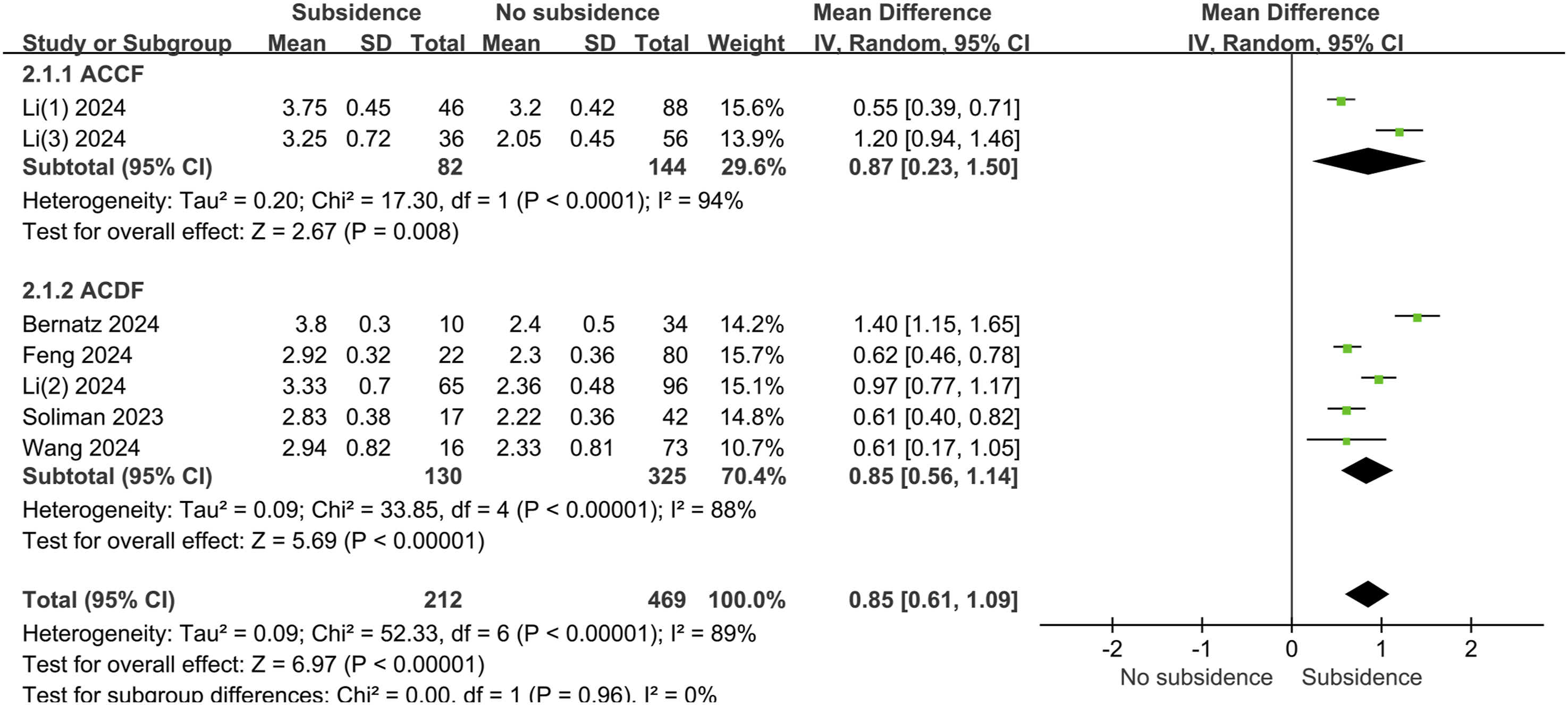
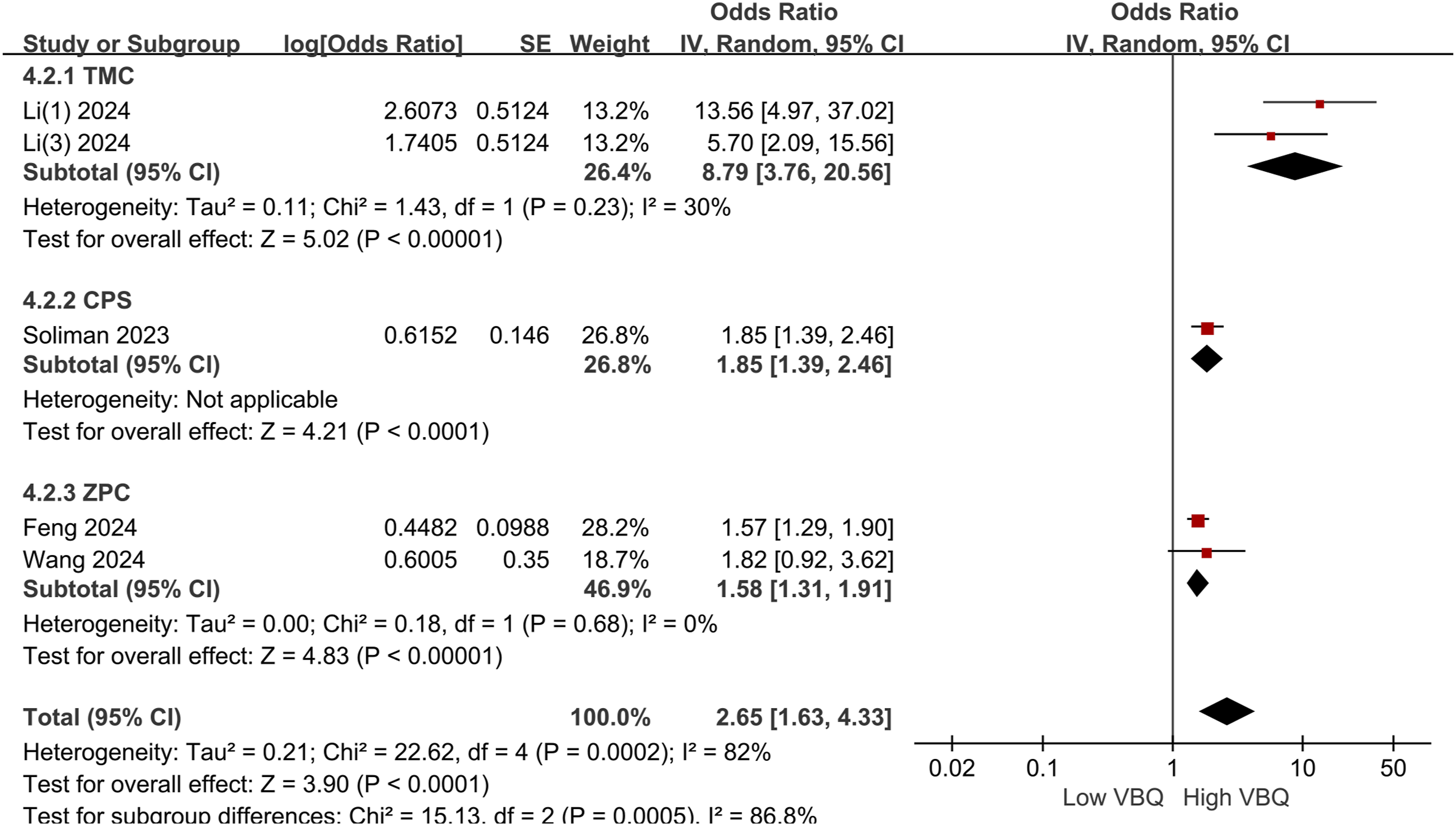
Analysis of Risk Factors for Postoperative Cage Subsidence Associated with High C-VBQ
High C-VBQ scores were identified as a significant risk factor for cage subsidence following cervical spine fusion surgery (Figure 6). The pooled OR for high C-VBQ scores and cage subsidence was 2.98 (95% CI, 1.68-5.30; P < 0.001; I2 = 91%; random-effects model). In the subgroup analysis by surgery type vs cage type, no significant difference was observed between the surgery subgroups (P = 0.53), while a significant difference was found between the cage type groups (P < 0.001; I2 = 86.8%; random-effects model), suggesting that cage type may contribute to the heterogeneity in this study (Figure 7). Overall, patients undergoing cervical spine surgery with high C-VBQ scores were more likely to experience cage subsidence. High C-VBQ risk analysis by surgical approach subgroup analysis. SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom; ACDF, anterior cervical discectomy and fusion; ACCF, anterior cervical corpectomy and fusion. High C-VBQ risk analysis by fusion type. CPS, cervical plate system; ZPC, zero-profile cage; TMC, titanium mesh cage; SD, standard deviation; IV, inverse variance; CI, confidence interval; df, degrees of freedom.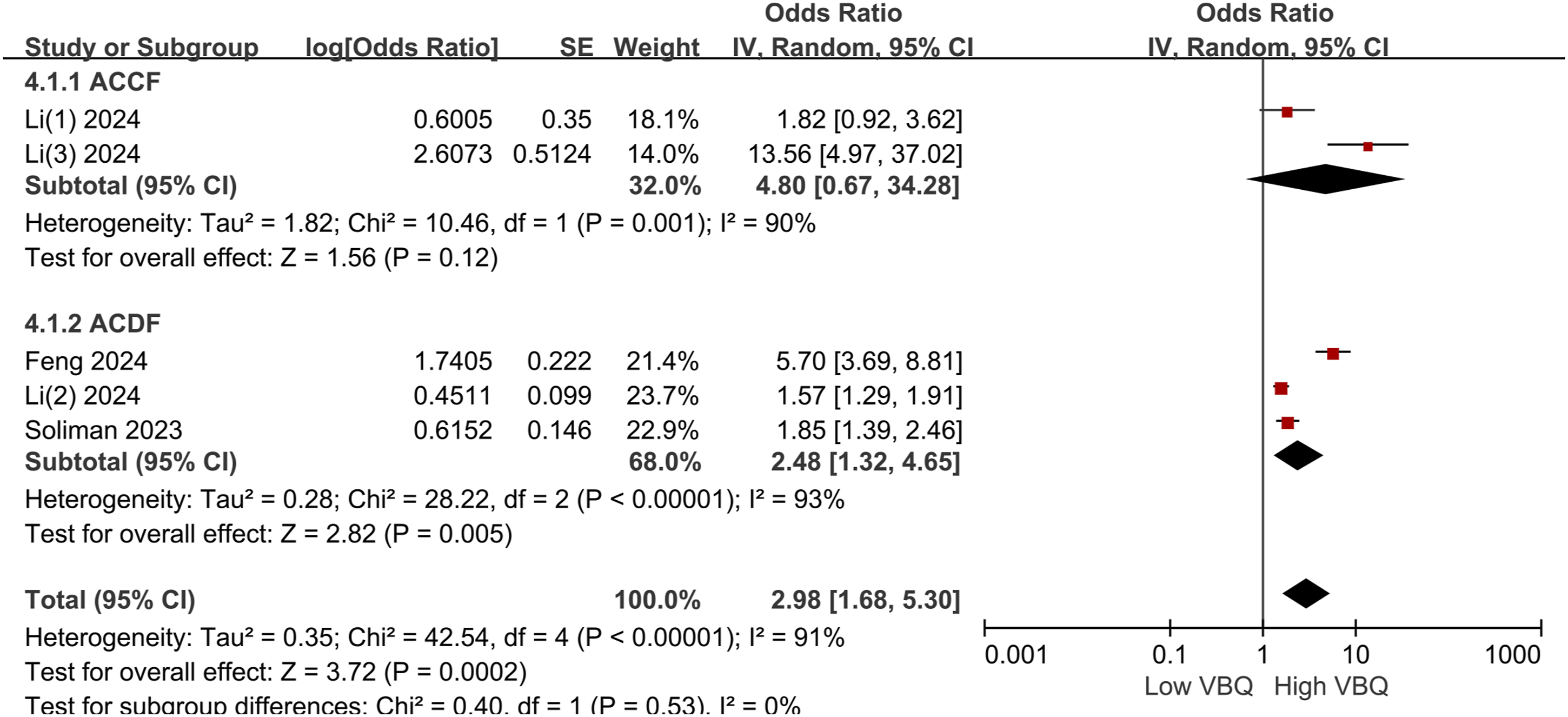
Diagnostic Value of High C-VBQ for Postoperative Cage Subsidence
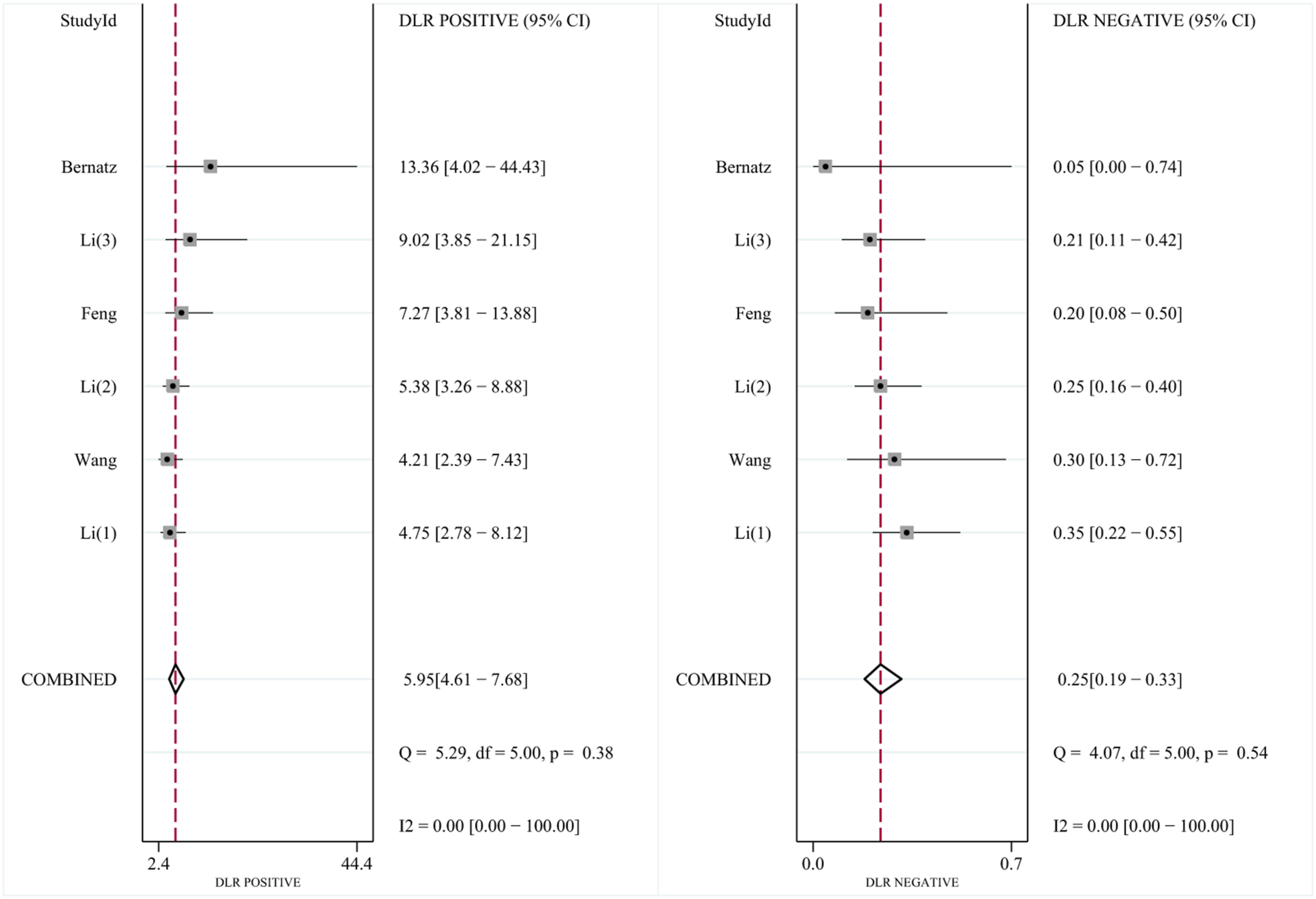
As shown in Figure 8(A), six studies assessed the diagnostic sensitivity and specificity of C-VBQ scores in 195 patients with cage subsidence and 622 controls. The C-VBQ cut-off values ranged from 2.68 to 3.45, with a mean of 2.94 ± 0.32. The sensitivity and specificity reported in these studies ranged from 69.60% to 100% and 82.10% to 94.10%, respectively. The pooled sensitivity and specificity were 0.78 (95% CI, 0.72-0.83) and 0.87 (95% CI, 0.83-0.90), respectively. The pooled PLR was 6.0 (95% CI, 4.6-7.7), the NLR was 0.25 (95% CI, 0.19-0.33), and the DOR was 24 (95% CI, 15–37) (Figure 9). The SROC curve for the overall diagnostic accuracy of the C-VBQ score is shown in Figure 8(B), with an AUC of 0.90 (95% CI, 0.87–0.92) for high C-VBQ scores used to diagnose cage subsidence after cervical spine surgery. A represents a forest map of sensitivity and specificity estimates of high vertebral mass scores for post-cervical fusion sink. B shows the SROC curve of the high VBQ score used to diagnose the fusion sink. C shows the funnel plot used for publication bias detection. Results of a high vertebrae mass score, as output by STATA, assessing fusion apparatus subsidence after cervical surgery.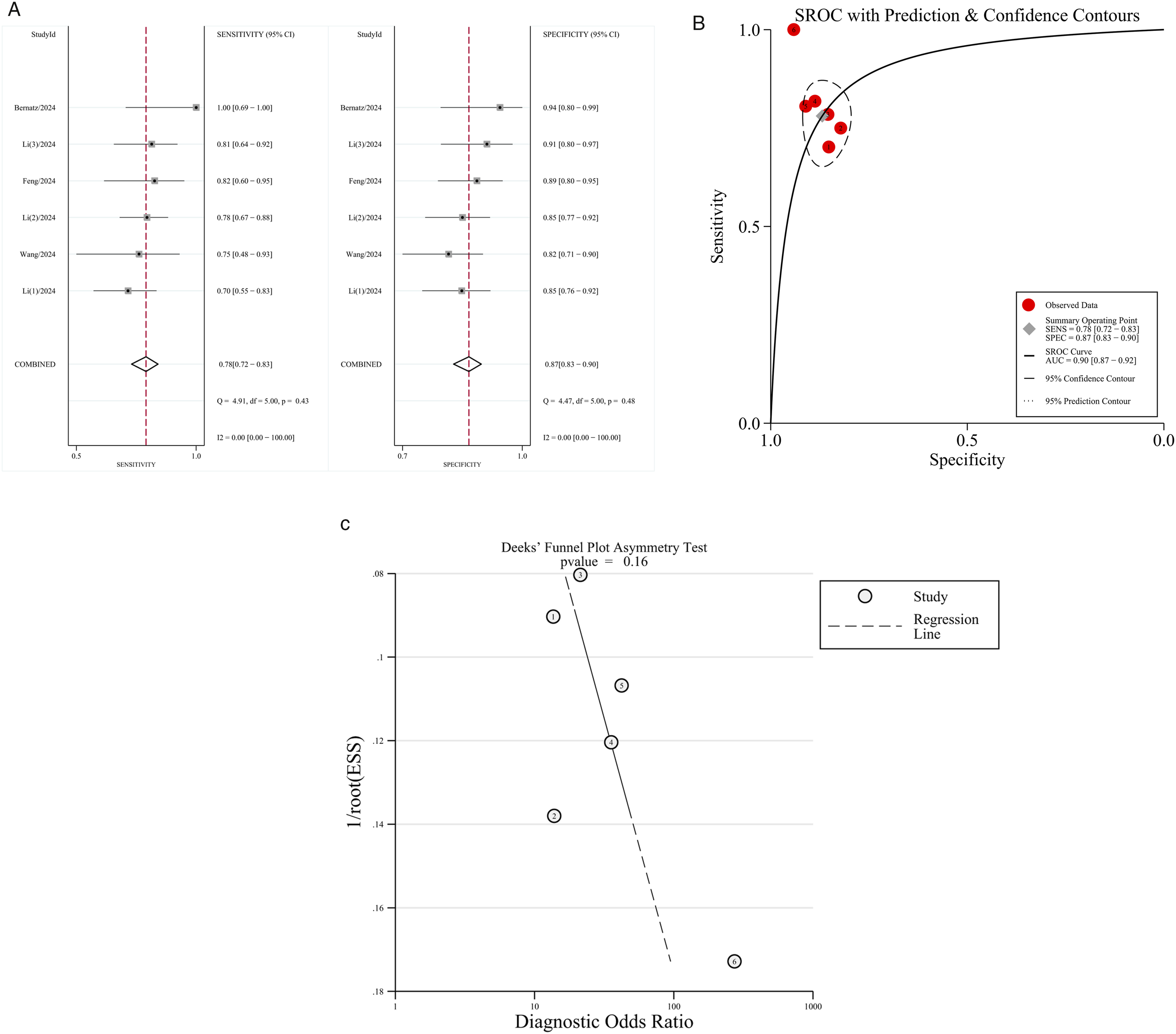
Publication Bias
Figure 8(C) displays a Deeks funnel plot for high C-VBQ scores used in diagnosing postoperative cage subsidence, showing minimal risk of publication bias (P > 0.1). Likelihood ratios and post-test probabilities were applied to evaluate clinical utility, as they indicate the probability of postoperative cage subsidence in patients with positive or negative test results. With a pre-test probability set to 50%, a positive test result yields a post-test probability of 86%. When the negative likelihood ratio is set to 0.25, the post-test probability of a negative test result decreases to 20% (Figure 10). A nomogram for diagnosing cage subsidence.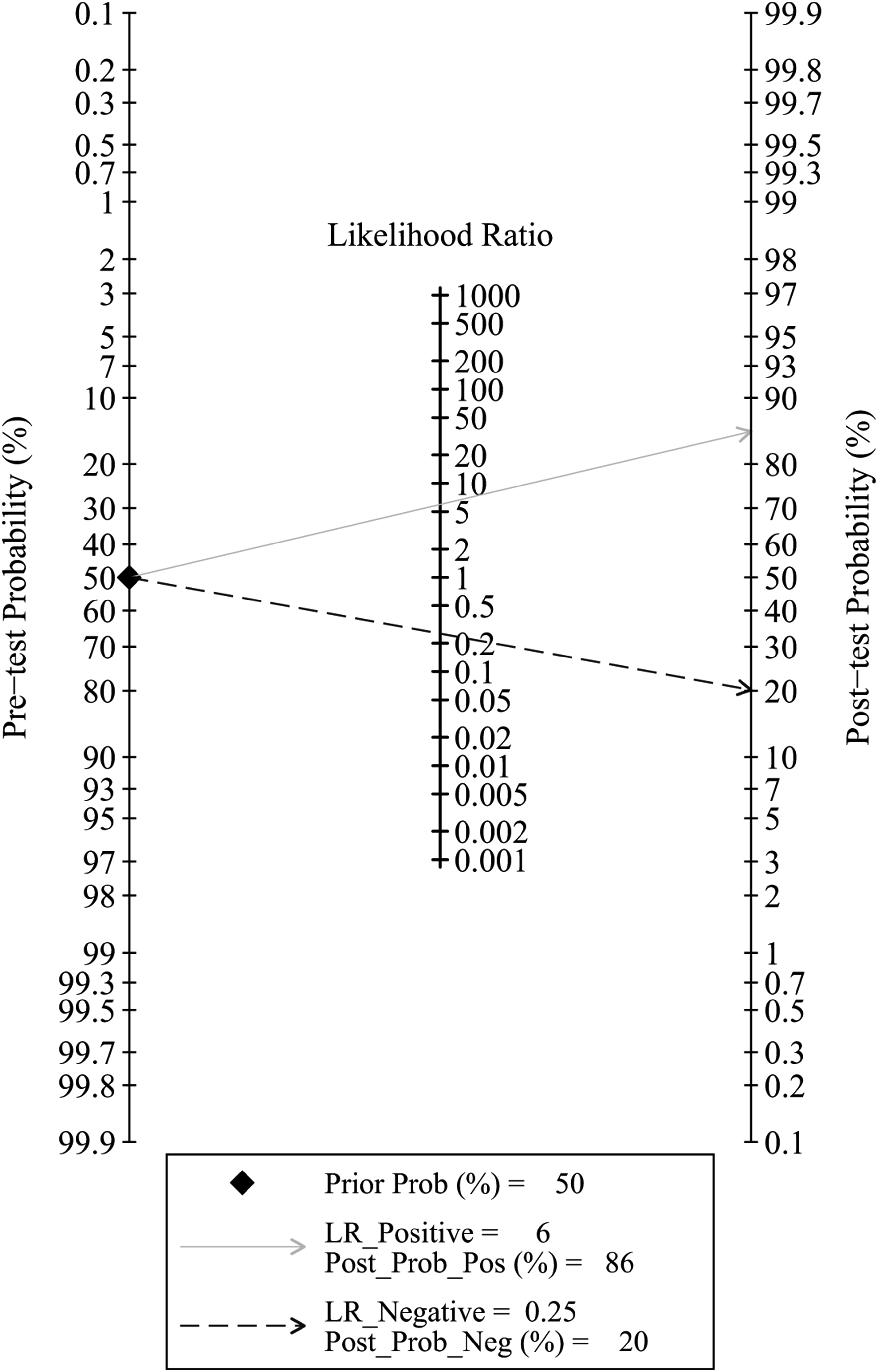
Discussion
This meta-analysis aimed to evaluate the potential value of C-VBQ scores in predicting cage subsidence following cervical fusion surgery. After analyzing data from 7 studies involving 681 patients, we found a significant association between higher C-VBQ scores and cage subsidence. Risk factor analysis revealed that patients with higher C-VBQ scores were at a significantly increased risk of postoperative cage subsidence (OR = 2.98). When the C-VBQ cutoff value was set at 2.94 ± 0.32, the diagnosis of postoperative cage subsidence showed a pooled sensitivity of 0.78 and specificity of 0.87, with an AUC of 0.90 (95% CI, 0.87-0.92). Based on these findings, we propose that the C-VBQ score could be used to identify patients at high risk for cage subsidence, enabling clinicians to implement timely interventions to prevent related postoperative complications. These results provide additional support for incorporating the C-VBQ score into postoperative management and suggest its potential role in risk screening and preoperative assessment to optimize clinical outcomes.
VBQ Score in Preoperative Bone Quality Assessment of the Spine
Studies have shown that poor preoperative bone quality has been shown to be a key factor affecting cage subsidence.12,14 Therefore, in order to achieve better surgical outcomes, surgeons should pay close attention to the preoperative bone quality of their patients and take timely interventions to achieve a good clinical prognosis. 24 Currently, DXA is the gold standard used to assess preoperative bone quality in patients undergoing spinal surgery. 6 However, degenerative spinal lesions can affect the accuracy of T-scores measured by DXA 25 and its low use in the preoperative spine 7 makes this method limited in practical application. In contrast, QCT can more accurately measure the volumetric density of cancellous and cortical bone through the use of calibrated body moulds and specialised software, and studies have shown that its results are more correlated with the patient’s true bone density. 9 However, because QCT requires specialised equipment and analysis tools, it is currently only used in a few health care settings.
In recent years, Ehresman et al. 8 developed a lumbar VBQ score based on lumbar MRI T1-weighted imaging, demonstrating a strong correlation with DXA T-scores and QCT findings. 9 Since osteoporosis increases bone marrow fat infiltration in cancellous bone, which appears as a high signal on T1-weighted imaging, a higher VBQ reflects more severe osteoporosis. The primary advantage of the VBQ scoring system is its ability to assess bone quality using existing MRI images, thereby avoiding the need for additional tests, radiation exposure, or increased medical costs.
Although the VBQ score has been extensively studied in the lumbar spine, research on its application in cervical spine surgery remains relatively limited. To address this gap, Soliman et al. 12 expanded the clinical application of VBQ by developing the C-VBQ for the cervical spine. This score showed a strong positive correlation with the lumbar VBQ (r = 0.757), 13 with comparable diagnostic value for preoperative osteoporosis assessment in cervical spine surgery patients (AUC = 0.78). Thus, the VBQ score, as an innovative tool for assessing bone quality, shows considerable potential in the diagnosis of osteoporosis.
Despite the promising applications of the VBQ score, its widespread clinical adoption faces several challenges. Research has shown that VBQ scores are influenced by a range of physiological and technical factors, such as ethnic variations, lipid levels, dietary habits, and differences in the magnetic field strength of MRI devices.26,27 These factors contribute to inconsistencies in VBQ scores across different populations and devices. Future studies should focus on optimizing the standardization of the VBQ scoring process to overcome these limitations and explore its potential in combination with other diagnostic tools to enhance early screening and improve the accuracy of osteoporosis diagnosis.
C-VBQ Predicts Postoperative Cage Subsidence
Cage subsidence is among the most common complications related to internal fixation in cervical spine surgery, 28 with incidence rates reported as high as 79.7% and 83% following ACCF and ACDF surgeries, respectively.29,30 Cage subsidence results in a loss of intervertebral height, which can lead to adverse outcomes such as nonunion, segmental kyphotic deformity, adjacent segment degeneration, and significant impacts on surgical success and patient quality of life. 31
In the present study, our combined results confirmed that high C-VBQ was significantly associated with interbody fusion device subsidence (OR = 2.98). In addition, C-VBQ had a good role in predicting fusion device subsidence when the C-VBQ cut-off value was 2.94, with a pooled sensitivity and specificity of diagnosis of 0.78 and 0.87, respectively, and a combined AUC of 0.90. Therefore, if patients with poor bone quality can be identified in a timely manner preoperatively and their surgical and therapeutic regimens adapted, this would help to reduce the risk of postoperative cervical spine fusion device subsidence, thereby improving the patients’ prognosis. For example, intraoperative use of bone cement increases the stability of the fusion system construct. 32 For patients who do not require emergency surgery or need to wait for surgery, starting osteoporosis medication 6 months before surgery may be another effective way to control the risk of fusion subsidence if close follow-up and appropriate patient education are available. 33
Analysis of Risk Factors for Cage Subsidence after Cervical Spine Surgery
Several studies have identified additional risk factors that influence cage subsidence following cervical spine surgery, beyond the C-VBQ. Age and gender, for instance, are common confounders.34-36 Older patients may face a higher risk of subsidence due to conditions such as osteoporosis, while postmenopausal women often have lower bone mass, which also increases their risk. Reduced disc height is another significant factor affecting fusion device subsidence. 37 A lower disc height may result in inadequate support, leading to concentrated load and an elevated risk of subsidence. The tilt angle and placement depth of the fusion device have also been shown to impact subsidence. 38 Improper alignment or depth placement can cause uneven stress distribution, thereby contributing to subsidence. Additionally, intraoperative factors such as excessive distraction and correction can negatively affect the stability of the fusion device, 39 potentially leading to subsidence. A larger cross-sectional area of the cage increases its contact area with the surrounding endplate, which provides more efficient axial load transfer and enhances segmental stability.36,40,41 Multi-segment surgery increases the surgical burden and operative complexity, potentially resulting in uneven postoperative stress distribution and fusion instability, thus raising the risk of subsidence. 35 Endplate damage decreases the contact area between the cage and the vertebral body, leading to uneven load distribution and inadequate support, which can destabilize the fusion and increase the likelihood of subsidence or deflection. 42 Finally, the length and placement of screws directly influence the fixation strength. Inaccurate screw placement or angulation can cause uneven stress distribution, impairing the long-term stability of the fusion and raising the risk of subsidence. 43 Therefore, these factors should be carefully considered and optimized during surgery to minimize postoperative complications and the risk of subsidence.
Sources of Heterogeneity
Statistical heterogeneity among the included studies was high. Subgroup analysis indicated that the heterogeneity stemmed from variations in VBQ values and the types of cage used. Despite adjustments for CSF signals, discrepancies in C-VBQ values persisted across the studies. For instance, in the study by Zhu et al., 17 the c-VBQ scores for the settling and control groups were 3.75 ± 0.45 and 3.20 ± 0.42, respectively, while in the study by Li et al., 15 the scores for the sedentary and control groups were 3.25 ± 0.72 and 2.05 ± 0.45, respectively. Additionally, the area under the ROC curve showed wide variation in the VBQ cutoff values, ranging from 2.68 to 3.45, with a mean value of 2.94 ± 0.32. Despite efforts to reduce heterogeneity, it could not be fully eliminated, so a random-effects model was applied. However, in the diagnostic experiment, the 6 included studies demonstrated good homogeneity, with an I2 of zero for both combined sensitivity and specificity, suggesting that the C-VBQ score provides reliable results and strong agreement when predicting fusion subsidence.
Limitations and Future Researches
To our knowledge, this is the first study to systematically summarize the value of the C-VBQ score in predicting the risk of cage subsidence in patients undergoing cervical spine surgery. However, several limitations should be considered when interpreting the results. First, the included studies were all retrospective cohort studies, which are prone to selection bias and may lead to an overestimation of the diagnostic advantage ratio. Second, the study population primarily consisted of middle-aged and elderly patients undergoing cervical spine surgery, and the study sites were limited to China and the United States, which may restrict the generalizability of the findings to younger, healthier individuals or populations in other regions. Third, there was significant clinical and statistical heterogeneity among the included studies, particularly in cage types, and despite efforts to address this, heterogeneity could not be fully eliminated, necessitating the use of a random-effects model. Fourth, the VBQ thresholds varied across the included studies, ranging from 2.68 to 3.445, with a mean value of 2.94, and the optimal threshold remains to be further investigated. Fifth, due to the limited number of studies included, the predictive value of the C-VBQ score for prognostic indicators such as proximal junctional kyphosis and reoperation has not been sufficiently explored, warranting further investigation. Sixth, the exclusion of unpublished data may introduce publication bias. Therefore, all findings from this review should be interpreted with these limitations in mind. Finally, some of the included studies did not adequately control for all relevant confounders, potentially affecting the accuracy and generalizability of the results. Although the C-VBQ demonstrated independent predictive value in some studies, the reliability of these findings was limited due to incomplete control of confounders.
Future studies should be prospectively designed and more comprehensively control for these confounders to more accurately assess the predictive effect of C-VBQ on fuser subsidence. Currently, C-VBQ scores are primarily based on T1-weighted imaging. However, the potential predictive value of C-VBQ scores derived from T2-weighted or STIR imaging remains unclear, warranting further investigation into the validity of C-VBQ scores from different imaging modalities for predicting postoperative risk.
Conclusion
In summary, this study systematically evaluated the diagnostic utility of the C-VBQ score in predicting interbody fusion subsidence following cervical spine surgery through meta-analysis. Results indicated that the C-VBQ score effectively predicts the risk of interbody fusion subsidence. Given its ease of measurement, radiation-free nature, and broad applicability, the C-VBQ score holds promise for widespread clinical use. We recommend that the C-VBQ score be considered for identifying patients at high risk of interbody fusion subsidence prior to cervical spine surgery, facilitating preoperative assessments and enabling individualized surgical planning with appropriate preventive measures. Nonetheless, further prospective studies and better control of additional confounders are needed to validate the effectiveness of C-VBQ in this field and optimize its clinical application.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Project of Health Commission of Sichuan Province (23LCYJ032); the Clinical Scientific Research Fund Project of Chengdu Medical College and the Third Affiliated Hospital of Chengdu Medical College (23LHPDZYB20); the Research Fund Project of Chengdu Medical College and the Chengdu Seventh People’s Hospital (2022LHJYZD-03); Sichuan Province medical research project plan (S23035); Sichuan medical youth innovation research project (Q23058).