
Abstract
Study design
Observational study.
Objectives
To evaluate the prevalence of erectile dysfunction and evaluate the effects of decompressive surgery on erectile dysfunction in cervical spinal stenosis and lumbar canal stenosis patients.
Methods
This observational, prospective analysis enrolled patients aged 18-80 with cervical spinal stenosis and/or lumbar canal stenosis that underwent respective decompressive surgery. The IIEF-5 questionnaire was administered preoperatively, and at 6- and 12-months postoperatively to assess erectile dysfunction severity. The EPIC database was queried to determine any postoperative complications and document prominent erectile dysfunction risk factors.
Results
Of 79 patients included in the analysis, 42 (53.2%) completed the IIEF-5 at 6 months, and 62 (78.5%) completed it at 12 months. Eighteen had cervical stenosis only, 54 had lumbar stenosis only, and 7 had both. 72% (18/25) of cervical stenosis patients and 83.6% (51/61) of lumbar stenosis patients had erectile dysfunction preoperatively according to IIEF-5 responses. The average preoperative IIEF-5 score indicated significant presence of erectile dysfunction for both the cervical and lumbar stenosis groups. No significant differences were identified in IIEF-5 score deltas from pre- to both postoperative periods. The presence of erectile dysfunction in both the cervical and lumbar stenosis groups was not significantly associated with the presence of any documented risk factors.
Conclusions
Our results suggest no significant improvement in overall erectile function postoperatively for patients with preoperative erectile dysfunction. This is important to address during patient counseling for decompression surgery candidates with cervical spinal stenosis and/or lumbar canal stenosis to manage expectations.
Keywords
Introduction
Spinal stenosis is a pathological narrowing of the spinal canal that predominantly impacts middle-aged and elderly populations.1,2 It is known to be associated with several neurological deficits, including erectile dysfunction (ED). At present, there is a paucity of studies in the medical literature that have explored the prevalence of ED in cervical canal stenosis (CSS) and lumbar canal stenosis (LCS) patients, as well as the response to ED regarding surgical treatment for these conditions. Despite this, prior studies have shown that certain decompressive spinal surgeries for other back and spine-related conditions may improve ED.1,3-10 Given the current discrepancies in the literature pertaining to the efficacy of surgical intervention with regards to ED, the present study aimed to evaluate ED both before and after cervical decompression surgery for CSS, and before and after lumbar decompression surgery for LCS. Findings may provide clinicians with greater insight regarding any expected benefits of surgical intervention, which enables detailed counseling and informed partnered decision making with patients to manage expectations pre- and postoperatively.
Methods
Patient Sample
The study population was drawn from patients aged 18-80 who presented to the Cleveland Clinic between July 2016 and October 2018 with cervical spinal stenosis (ICD10 M48.02) and/or lumbar canal stenosis (ICD10 M48.06) with non-traumatic spine disease and/or acute cord compression, who were to undergo cervical spine fusion or direct decompression surgery for CSS, or lumbar spine fusion or direct decompression surgery for LCS. IRB approval was received for study number 16-263 (ActivityId 317023), and verbal consent was obtained for participation in the study from all participants. The requirement for written consent was waived based on the study involving no risk or additional cost to the patient, surgeon, or staff as well as involve no alteration of care to the patients in any way.
Indications for surgery included cervical spinal stenosis and/or lumbar canal stenosis secondary to degenerative changes, disc herniation, and spondylolisthesis. The symptoms of unilateral radiculopathy and/or foraminal stenosis were discerned from those of myelopathic symptoms secondary to complete cervical or lumbar canal stenosis both via the context of the patient’s history of symptoms as well as the physical exam. Criteria for symptomatic cervical spinal stenosis included canal stenosis at cervical levels as seen on MRI or CT myelography, with symptoms of cervical myelopathy and/or radiculopathy. Criteria for symptomatic lumbar canal stenosis included canal stenosis at lumbar levels as seen on MRI or CT myelography, with symptoms of neurogenic claudication reported from the patient’s history. All imaging was reviewed by senior spine surgeons to determine the presence of canal stenosis. Patients undergoing both multi-level and single-level fusion were included. Patients with known risk factors for ED were also included. These risk factors included smoking/alcohol use status, diabetes mellitus, existing neuropathy, hypertension, cerebrovascular accident, chronic obstructive pulmonary disease, ischemic heart disease, prior-diagnosed organic erectile dysfunction, benign prostate hypertrophy, reported depression/anxiety, and renal impairment. Additional risk factors for ED included medications that may contribute towards ED, which were also documented.
Any patient younger than 18 years or greater than 80 years of age was excluded.
Primary Outcome
The mean international index of erectile dysfunction (IIEF-5) questionnaire was used to investigate erectile dysfunction severity. The IIEF-5, also called the Sexual Health Inventory for Men (SHIM) survey, is a 5-item self-reported questionnaire widely used as a diagnostic tool for evaluating the presence and severity of erectile dysfunction.4,11 The IIEF-5 questionnaire was validated as a diagnostic tool by Rosen et al (1999) based on an analysis of 1152 male patients, classifying the extent of ED as severe (5 to 7), moderate (8 to 11), mild to moderate (12 to 16), mild (17 to 21), and no ED (22 to 25). 11 Siddiqui et al (2013) provided two-year prospective results using the IIEF-5 and reported scores of less than 21 as having ED, further categorizing into mild ED (16 to 20), moderate ED (11 to 15), and severe ED (10 or less). 4 The IIEF-5 was administered preoperatively, and at 6- and 12-months postoperatively for the present study, with a score of 20 or less on the IIEF-5 considered indicative of ED.
The EPIC database was queried to retrieve medical charts from follow up visits consistent with the study sample and to determine any adverse outcomes or complications associated with the surgical procedure. All subjects were de-identified after chart review, and existing patient data was collected and managed using REDCap electronic data capture tools hosted at the Cleveland Clinic Foundation. 12 REDCap (Research Electronic Data Capture) is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources.
Covariates
The following existing data were extracted from each patient chart: age, gender, BMI, reported depression, anxiety, smoking/alcohol use status, potential ED-contributory medications, and medical comorbidities that may contribute to ED. Additionally, level(s) of stenosis, level and extent of decompression, year of fusion or decompression, length of hospital stay, units of blood transfused (if any), intraoperative complications noted, and time to follow-up were extracted from the medical records.
Data Analysis
Patient and clinical characteristics were summarized using descriptive statistics, stratified by surgery type (CSS, LCS) and by whether the patient had ED according to the IIEF-5 cutoff score of 20. A power analysis was performed prior to enrollment of patients. Using half of the standard deviation (4.0) of the baseline preoperative IIEF-5 score reported in Siddiqui et al as an estimate of minimal clinically significant change, we estimated that the proposed study would require at least 34 patients to detect change in IIEF-5 score of 2 points with 80% power.4,13 Thus, we sought to enroll 34 patients in each of the CSS and LCS groups. Comparisons were made using two-sample t-tests or Mann-Whitney U tests for continuous variables and Fisher’s exact test for categorical variables. Within each of the CSS/LCS groups, the prevalence of ED was determined by computing the proportion of patients with a pre-surgery IIEF-5 score of 20 or less. A 95% confidence interval was computed using the exact binomial method. To determine whether patients improved in IIEF-5 score from pre-surgery to 6- and 12-month follow-up, we fit separate mixed-effects linear regression models for each of the CSS and LCS groups. The dependent variable was IIEF-5 total score, and time was included as a fixed-effect independent variable, treated as categorical (pre-surgery, 6-month post-surgery, 12-month post-surgery). A random effect for patient was included. There were some patients who had both CSS and LCS. These patients were included in the analyses for each group. We also explored whether the number of levels operated on was associated with change in IIEF-5 total score. To do so, we added number of levels (1, 2, 3+) to the mixed-effects models as well as an interaction term between number of levels and time. Plots of the interaction terms were created for visualization. All computations were performed in R, version 4.0.3 (R Foundation, Vienna Austria). All tests were two-sided and P-values less than .05 were considered statistically significant.
Results
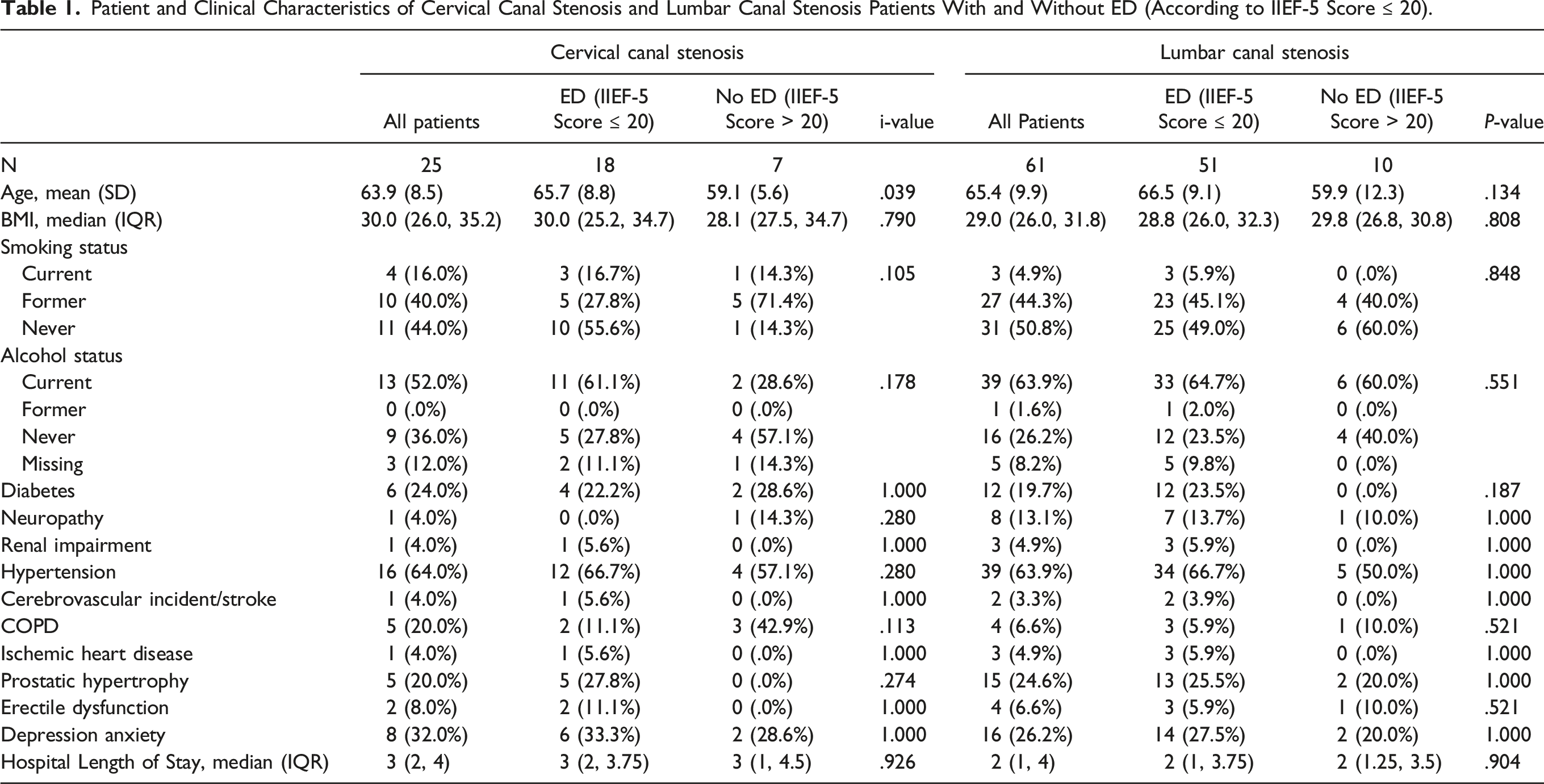
Patient and Clinical Characteristics of Cervical Canal Stenosis and Lumbar Canal Stenosis Patients With and Without ED (According to IIEF-5 Score ≤ 20).
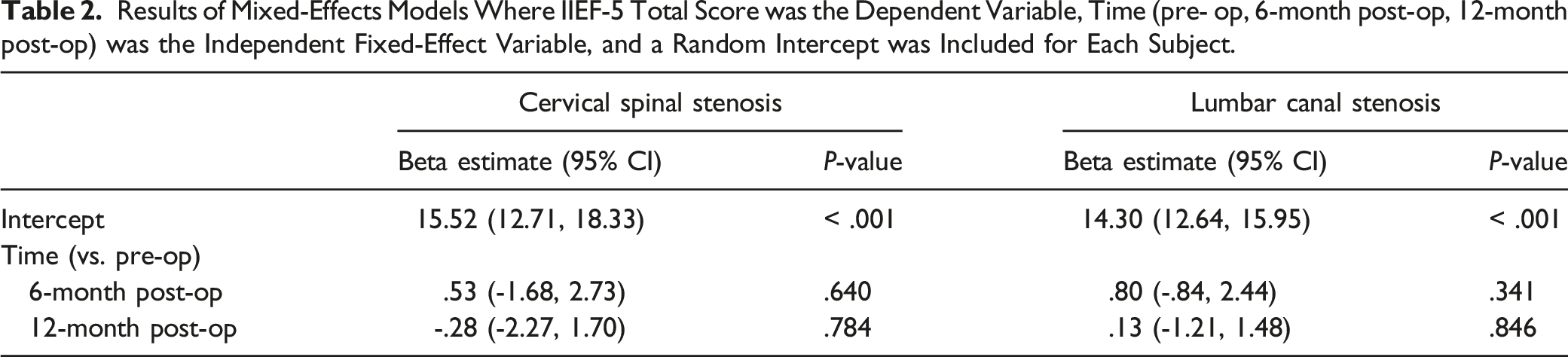
Results of Mixed-Effects Models Where IIEF-5 Total Score was the Dependent Variable, Time (pre- op, 6-month post-op, 12-month post-op) was the Independent Fixed-Effect Variable, and a Random Intercept was Included for Each Subject.
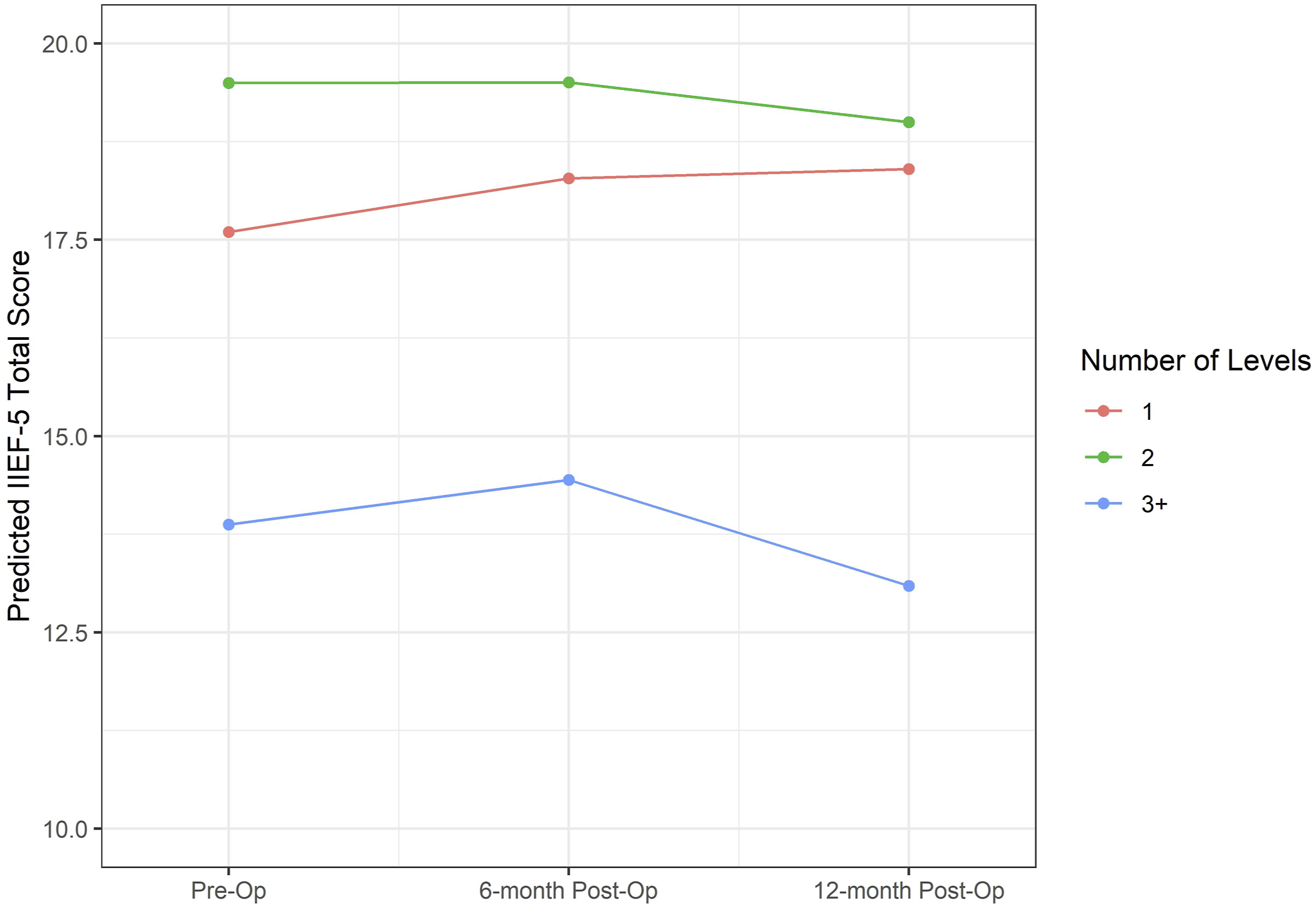
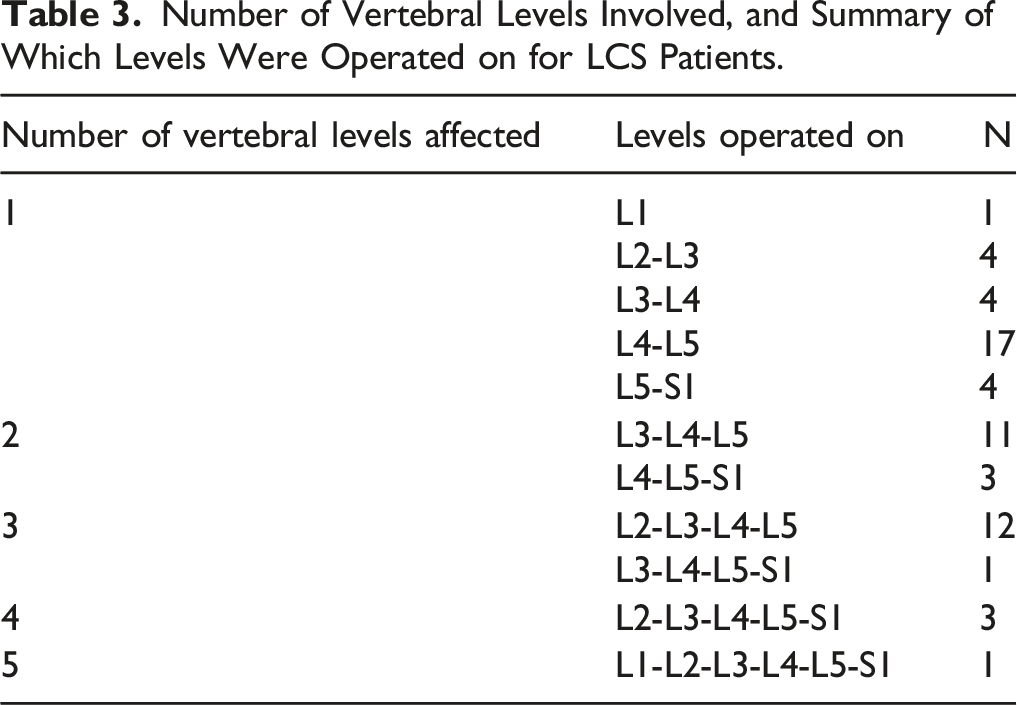
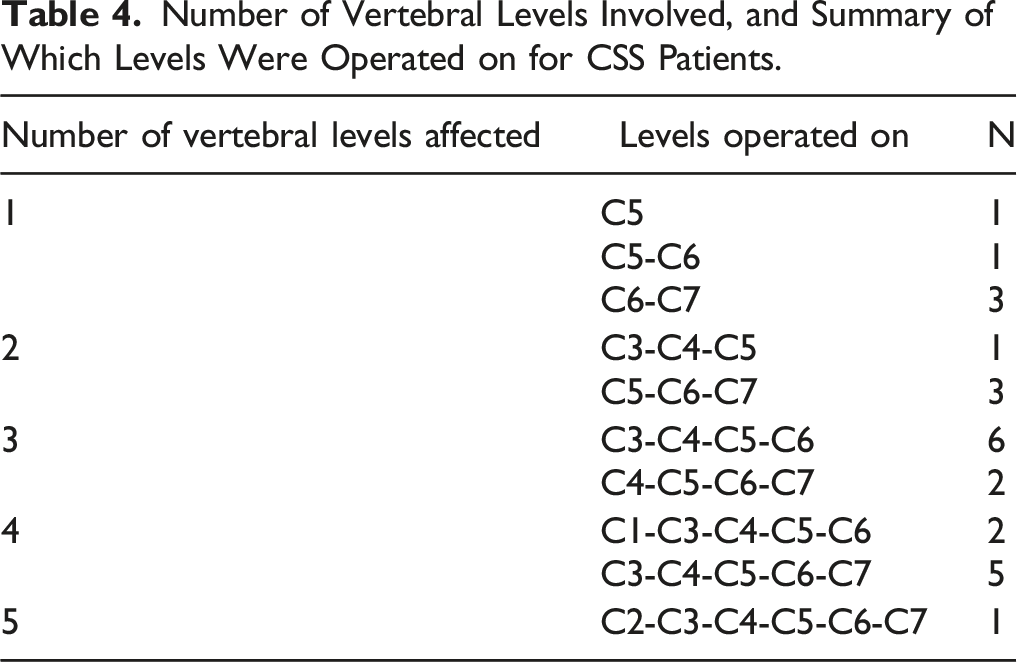
Figures 1 and 2 show mean predicted IIEF-5 total scores estimated by the mixed-effects models that included number of spinal levels involved and the interaction between number of levels and time (preoperative, 6-months postoperative, 12-months postoperative) for LCS and CSS patients, respectively. In all cases, the change from pre-surgery to 6- or 12-months post-surgery either increased or decreased in score by less than one point. Descriptive tables enumerate the total number of vertebral levels, and specific levels involved for all patients in the LCS (Table 3) and CSS (Table 4) groups. These results also demonstrated no significant change over time in IIEF-5 score based on the number of spinal levels involved during operation. Mean predicted IIEF-5 total scores for LCS patients based on mixed effects model where IIEF-5 total score is the dependent variable and the fixed-effect independent variables are time, number of levels (1, 2, 3+), and an interaction between number of levels and time. Mean predicted IIEF-5 total scores for CSS patients based on mixed effects model where IIEF-5 total score is the dependent variable and the fixed-effect independent variables are time, number of levels (1, 2, 3+), and an interaction between number of levels and time. Number of Vertebral Levels Involved, and Summary of Which Levels Were Operated on for LCS Patients. Number of Vertebral Levels Involved, and Summary of Which Levels Were Operated on for CSS Patients.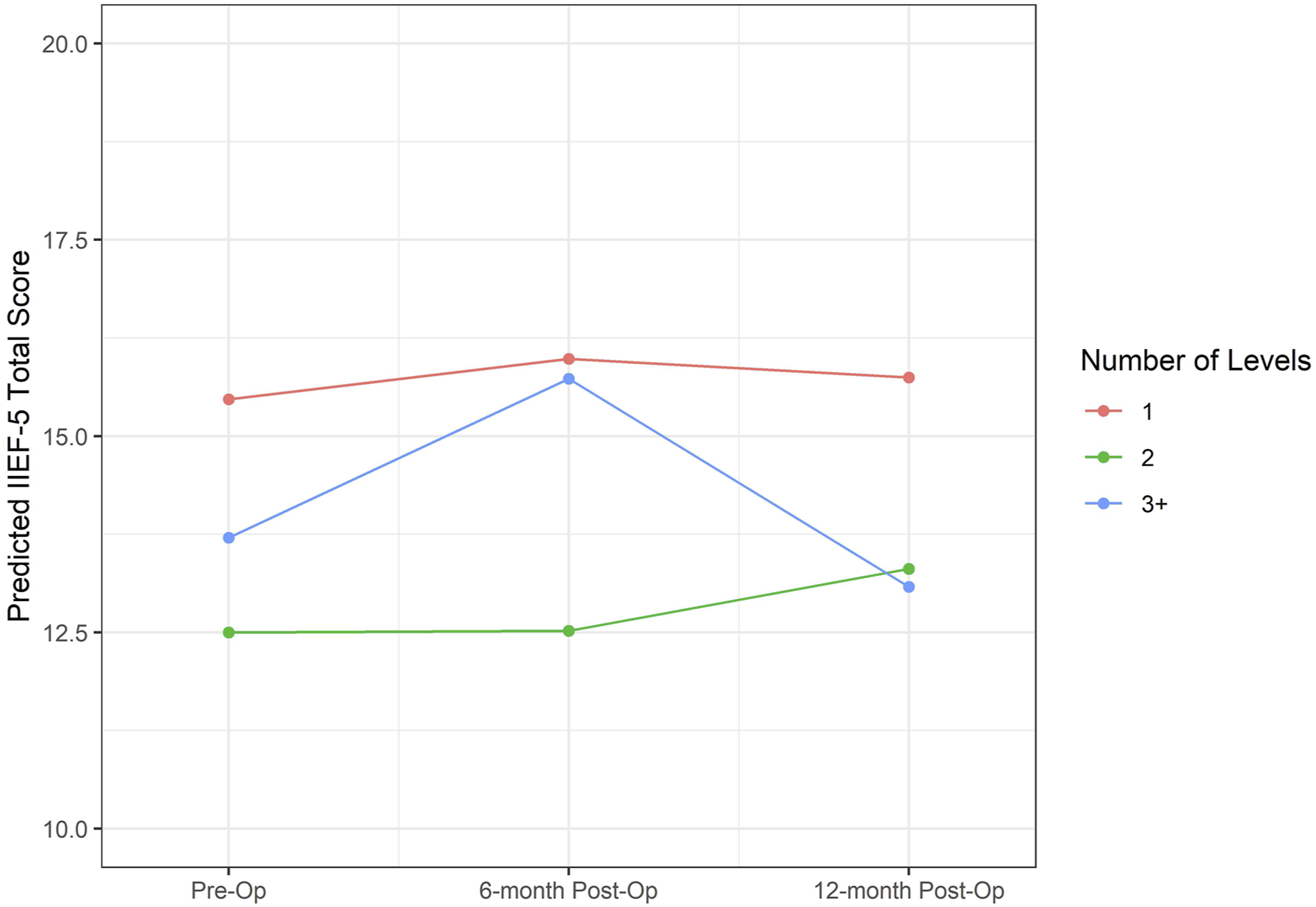
Discussion
Anatomically, LCS results in compression of efferent, pro-tumescent, parasympathetic fibers within the cauda equina. 3 Sympathetic fibers exiting the spinal canal above the level of maximal stenosis are not compressed, and thus imbalance may exist between pro-erectile signals and antagonistic sympathetic signals. Although poorly understood, reports also exist of LCS resulting in an excitable sacral center that may engender involuntary reflexogenic erection.14-18 Large analyses such as that of the Spine Patient Outcomes Research Trial (SPORT) 2010 have found that LCS patients treated surgically with decompressive laminectomy had improved health-related quality of life indices and pain scores following treatment.19,20 However, current literature, including the SPORT 2010 analysis, did not report the effect of this surgical treatment on ED among LCS patients. Similarly, studies on cervical spondylotic myelopathy (CSM; a common sequelae of CSS) report various motor, sensory, and bladder and bowel dysfunctions, as well as sexual dysfunction that can result from spinal stenosis or injury of cervical levels.3,21 Results of the 2013 AO Spine North American Prospective Multi-Center Study showed that surgical decompression for CSM is associated with improvement in functional, disability-related, and quality-of-life outcomes. However, this study also did not assess the effect of surgical decompression on ED among CSM patients, nor can the findings be directly extrapolated to cervical canal stenosis. 22
A handful of studies have explored facets of ED response to invasive interventions in the context of spine pathology associated with stenosis, including Hagg et al (2006). 5 This prospective study involving 264 patients (mean age 43, range 25-64 years) followed over two years found that those treated surgically for chronic low back pain reported significantly improved overall sexual function and sexual enjoyment relative to those randomized to non-surgical treatment. A case study by Choy et al (1999) found that two patients (mean age 33.5, range 25-42) regained erectile function after laser disc decompression for ED associated with herniated disc disease. 6 Three prospective studies by He et al (2006), Zhu et al (2008), Qian et al (2010) with mean follow up times between 11.8-16 months involving 22 (mean age 56.3 years, range 43-72), 22, and 19 (mean age 48.8) patients respectively described an improvement in ED following surgical decompression for CSM, however, these studies were limited by small sample sizes of less than twenty-five patients each.7,9,10 The first retrospective case series examining the role of ED in 197 patients (mean age 63 years, range, 33-74) with spinal stenosis with latest follow up at 9.7 months was carried out by Gempt et al (2010) and found a significant improvement in ED following decompressive surgery for LCS. 3 However, a small prospective study by Siddiqui et al in 2012 and 2013 involving 61 patients (mean age 38.4 years (SD = 7.0; range, 20-49) followed up at 6 months, and 56 patients followed up at 2 years respectively found that while there was overall improvement in mean visual analogue scale (VAS) scores for back and leg pain, Oswestry Disability Index, and North American Spine Society score for neurogenic symptoms at 2 years (P < .01), the mean international index of erectile dysfunction (IIEF-5) scores were not significantly different.4,8
Along the same vein, the results of statistical analysis for the present study indicate that there was no significant change in the degree of ED as measured via standardized 5-item IIEF-5 questionnaire responses from the preoperative to postoperative periods for patients with CSS nor LCS. The significance of this finding is that while the degree of ED may improve for a small proportion of patients following decompression surgery for cervical or lumbar stenosis, a significant proportion of patients with ED would not be expected to see a significant clinical improvement in their ED from decompression surgery alone, regardless of smoking/alcohol use status, BMI, and the presence of common medical comorbidities. This is reflective of the fact that several contributing factors influence both the presence and degree of ED which may be predominantly associated with vascular pathways, neural pathways, or both.23-29 Any aberration along the tumescence pathway can lead to ED, including pathology of the sacral preganglionic parasympathetic fibers and nervi erigentes which govern nitric oxide release from the cavernous nerve that initiates tumescence, or the maintenance of erection which is secondary to nitric oxide release from vascular endothelial cells.3,4,17,23-25 With regards to vascular etiologies, hypertension has been identified as a co-diagnosis in 35-40% of men with ED, and hyperlipidemia has been identified in about 42% of men with ED.23-25 Undiagnosed diabetes is 20-28% more likely in men with ED compared to men with normal erections, and the severity of ED is positively correlated with the length of time having diabetes.23-25 Obesity is associated with an up to 50% increase in risk of ED compared to the general population and is also associated with improvement or even resolution of ED following aggressive weight loss.23-25 Similarly, smokers that quit may experience up to 25% improvement in ED after 1 year, and those that continue to smoke experience increased severity of ED in a direct dose-response relationship.24,27 Common conditions that impact ED from a neurologic standpoint include heavy alcohol use, which is associated with an increased risk of ED secondary to direct nerve toxicity in a direct dose-response relationship.24,27 Individual neurologic conditions can also precipitate ED, such as Multiple Sclerosis or Parkinson’s disease, via direct disruption of neurologic pathways.23,28,29 The neurologic-psychiatric and neurologic-hormonal axes are also implicated in ED, as performance anxiety, stress, depression, and hypogonadism are also strongly associated with ED, with the incidence of depression in men with ED being almost three times greater compared to men without ED.23-25,27,30 Considering this, the present outcome of this study is not surprising when accounting for the distribution of other possible etiologies, and is notable that while direct spinal cord compression may be associated with the onset or progression of ED, its correction alone was not significantly associated with improvement in ED.
This study has certain limitations, including a relatively lower 6-month follow up survey response pool compared to the preoperative and 1-year postoperative response pools. We intended to have at least 34 patients in each of the CSS and LCS groups at this time point, but in total, we had 61 LCS patients and 25 CSS patients. Thus, we were underpowered in the CSS group secondary to time delays associated with management transition in the study, and concurrent lack of patient response. However, all changes in score were below the clinically significant change threshold of 2 points, indicating that lack of power was not the only reason for lack of statistically significant results. Another limitation is that it is possible that the degree of ED correlates with the degree of cord injury; this variable could not be meaningfully standardized to include an assessment in this study and no classification system was used to score central canal stenosis for additional stratification on data analysis. A third limitation is that the duration of dysfunction as well as the associated symptoms of claudication were not assessed other than based on patient reported histories, and thus may include patients with other potential sources of claudication-like symptoms such as undiagnosed vasculitis. The region of the cord involved in compression (ie, ventral vs dorsal) as well as surgical approach were also not assessed; these factors may potentially contribute to the degree of ED and/or postoperative improvement, and ideally would be preemptively stratified for in future studies.
Despite these limitations, this study addressed the concern of assessing a cohort of older patients, which extrapolates to align more so with the general population that suffers from ED. Compared to previous studies evaluating ED in relation to LCS and/or CSS, this study also included a larger sample size, and preoperative vs postoperative assessment of ED to help avoid recall bias. The results of this study are important for clinicians to consider when counseling patients with CSS and/or LCS that have concurrent (or concern for development of) ED. Accounting for this information will improve preoperative partnered decision making with patients who may be considering decompression surgery to manage expectations with regards the impact of this intervention on ED.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.