
Abstract
Study Design
Systematic review and meta-analysis.
Objective
The aim of this study was to determine the prevalence of asymptomatic cervical spinal cord compression (CSCC) in individuals with lumbar spinal stenosis (LSS).
Methods
A systematic electronic search was conducted in Medline, EMBASE, Scopus, and Web of Science without language restriction, with no starting date limit to June 8, 2023, to define the prevalence of asymptomatic CSCC in symptomatic LSS patients. Asymptomatic CSCC was defined based on radiographic studies. All types of studies were included in the review. Meta-analysis was performed on the reported prevalence of asymptomatic CSCC in LSS.
Results
The database search yielded 10,272 articles. After a full-text review, five studies were included in the final review, comprising a total of 1043 cases. Two studies had a low risk for bias, two moderate, and one estimated to be high risk. The range of prevalence of asymptomatic CSCC in LSS in the five included studies was between 24% and 61%. Meta-analysis on the reported prevalence of asymptomatic CSCC patients with symptomatic LSS demonstrated that the random pooled prevalence was 35% (95% CI: 23 to 48).
Conclusions
Asymptomatic CSCC appears to occur in a high number of patients, with this study noting its presence in one-third of patients with LSS. Based on these findings, we strongly recommend that spine surgeons exercise particular caution during the positioning of patients who are undergoing surgery for lumbar stenosis. Furthermore, it is imperative to monitor individuals with symptomatic LSS closely for any potential signs of emerging myelopathy.
Keywords
Introduction
Degenerative Cervical Myelopathy (DCM) represents a progressive affliction of the spinal cord that may arise from various sources, including mechanical stress or degenerative alterations. 1 The degenerative processes can include osteophytes, disc herniation, enlargement, or ossification of the ligamentum flavum, and translation or instability. 1 A multifactorial interplay of mechanical forces, such as shear, tension, and compression, contribute to a comprehensive understanding of DCM. 2 Individual predispositions, such as age, genetic factors, cardiovascular, gastrointestinal, and neural health, and exposure duration, also have a significant bearing on the susceptibility to spinal cord injury. 2 Symptoms of DCM manifest as pain, numbness in limbs, coordination impairment, balance issues, and bladder complications. 3
A key challenge within the DCM poulation is the accurate diagnosis and prediction of disease progression. 4 The global AO Spine RECODE-DCM initiative, collaborating with multiple stakeholders, aims to create a research toolkit that fosters rapid knowledge acquisition and augments DCM outcomes. 5 These endeavors emphasize the crucial role of early surgical intervention, currently the only disease-modifying treatment available, which can arrest further spinal cord injury and deliver significant benefits, though full recovery may remain elusive.6-9 Optimal surgical outcomes and the prevention of irreversible damage hinge on the early identification of patients exhibiting symptomatic myelopathy. Nevertheless, the inherent surgical risks warrant that in patients with Cervical Spinal Cord Compression (CSCC) lacking symptomatic myelopathy, surgical intervention is discouraged. 8
The occurrence of asymptomatic CSCC varies between 8% and 57%.10-12 Those with CSCC stand at risk for DCM development. In a 4-year study involving 66 asymptomatic CSCC patients, Bednarik et al. discovered that 19.7% manifested clinical DCM symptoms. 13 Spinal stenosis, a condition more prevalent in individuals with smaller spinal canals, arises from degenerative changes, and this degenerative sequence, coupled with resultant canal stenosis, can provoke neuronal compression in both cervical and lumbar regions, a condition known as Tandem Spinal Stenosis (TSS). 14
Tandem spinal stenosis prevalence is reported to range from 7.6% to 60%, with asymptomatic cases, where the patient exhibits no discernible symptoms, found in 23.7%-61.4% of instances.15-18 Recognizing asymptomatic CSCC, which can be present in patients with symptomatic Lumbar Spinal Stenosis (LSS), is important since the condition can evolve into myelopathy.13,19-22 Early diagnosis and thorough follow-ups can benefit CSCC patients. Moreover, during surgical operations, asymptomatic CSCC patients should be carefully positioned and further monitored for any signs of myelopathy.17,23
Appreciating the prevalence of asymptomatic CSCC in symptomatic LSS patients can inform more effective clinical decision-making. In this research, our objective is to define the prevalence of asymptomatic CSCC in patients diagnosed with symptomatic LSS.
Methods
The protocol for this study was registered with PROSPERO (CRD42023430201). 24 The study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) protocol for systematic reviews and meta-analysis. 25 The Ethics Committee of Tehran University of Medical Sciences, approved the study, and the reference number is IR.TUMS.SINAHOSPITAL.REC.1402.003.
Literature Search
An electronic search was conducted to identify research that determined the prevalence of patients with asymptomatic CSCC in patients with symptomatic LSS using Medline, EMBASE, Scopus, and Web of Science with no language restriction, with no starting date limit to June 8, 2023. The search strategy for this study is included in Appendix 1.
Selection Criteria
Studies had to report the prevalence of asymptomatic CSCC in known cases of lumbar stenosis. Asymptomatic was defined as those patients without neck pain, signs or symptoms of myelopathy, and cervical radiculopathy. Radiculopathy was considered arm pain or paresthesia in the dermatomal distribution or muscle weakness relating to the affected nerve. Myelopathic symptoms were defined as neck or upper limb pain, weakness, sensory loss, loss of dexterity, paresthesia, imbalance, falls, and autonomic dysfunction. Studies that met any of the following criteria were excluded: (1) Studies that reported the prevalence of symptomatic CSCC in patients with LSS. (2) Studies that reported asymptomatic cervical and thoracic cord compression in patients with LSS without mentioning separate prevalence for cervical and thoracic cord compression cases. (3) Reviews, case reports, and case series with less than ten patients. (4) Spinal compressions due to non-degenerative, oncologic, or traumatic causes.
Selection Process
Search results were imported to EndNote (X9, Thomason Reuters), duplicates were removed, and two reviewers independently screened titles and abstracts. Any discrepancies between the reviewers were resolved in a session with the senior author. After obtaining the full text of included articles, the full texts were checked against inclusion and exclusion criteria for including studies by two reviewers. Any disagreements were resolved by the senior author.
Data Extraction
A data collection spreadsheet was designed and the following items were extracted from the included studies: authors’ names, publication date, study date, country, study design, sample size, and characteristics, percentage of patients with LSS, percentage of patients with asymptomatic CSCC, BMI, level of lesions, primary lesion type, cervical lesion location, and tandem percentage. Data were extracted and rechecked by two investigators.
Quality Assessment
The ROBINS-I tool was used for risk of bias assessment, as recommended by the Cochrane Handbook for Systematic Reviews of Interventions. 26 This was also done by two independent authors and conflicts were resolved by the senior author. The class of evidence was based on the Journal of Bone and Joint Surgery for studies investigating treatment results for assessing methodological quality. 27
Outcomes
The variable of interest was the prevalence of imaging findings of CSCC in patients with symptomatic LSS that did not have any signs or symptoms of myelopathy or cervical radiculopathy.
Statistical Analysis
We assessed the heterogeneity of the studies with the Chi2 test and the I2 statistics. The “Metaprop” command in Stata was applied for meta-analyses of effect sizes. Random effects model was used to combine the effect sizes. Also, the effect sizes with 95% confidence intervals were plotted. Stata version 14.0 (Stata Corp, College Station, TX) was used for analysis.
Results
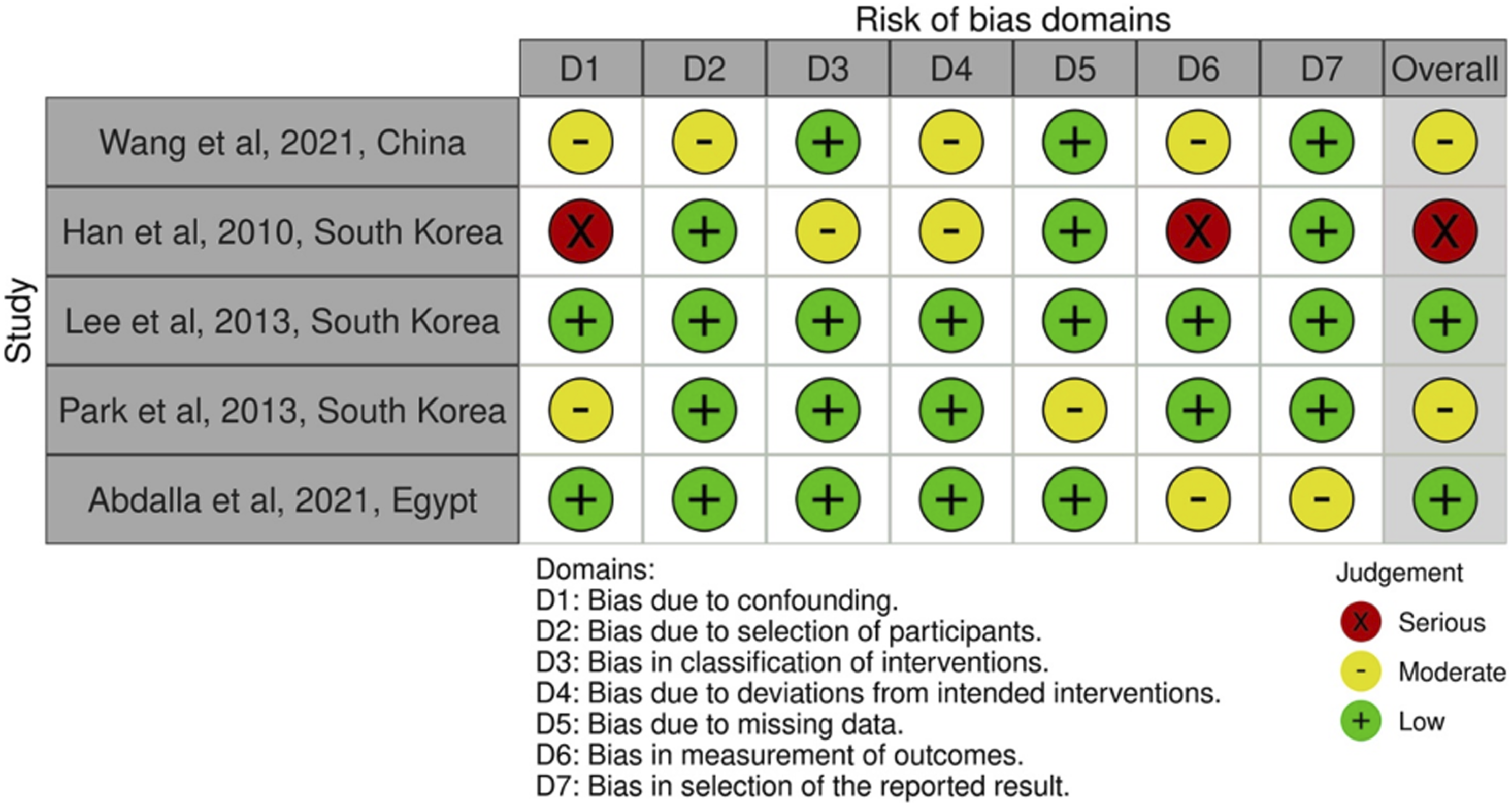
The PRISMA chart of this study is presented in Figure 1. The database search yielded 10,272 clinical cases. After screening relevant titles and abstracts, 28 manuscripts were included for further assessment. After a full-text review of these 28 records, five studies were included in the final analysis. Of these five studies, four were retrospective and one was prospective. In total, there were 1043 cases included. The included study characteristics are presented in Table 1. The ROBIN-I tool was used to assess the risk of bias in the included studies, and the results are presented in Figure 2. Two studies assessed low risk, two moderate risks, and one serious risk for bias. Flowchart of studies based on the PRISMA statement for the prevalence of asymptomatic cervical spinal cord compression in individuals presenting with symptomatic lumbar spinal stenosis. Characteristics of Included Studies. Risk of bias assessment of included studies for the prevalence of asymptomatic cervical spinal cord compression in individuals presenting with symptomatic lumbar spinal stenosis.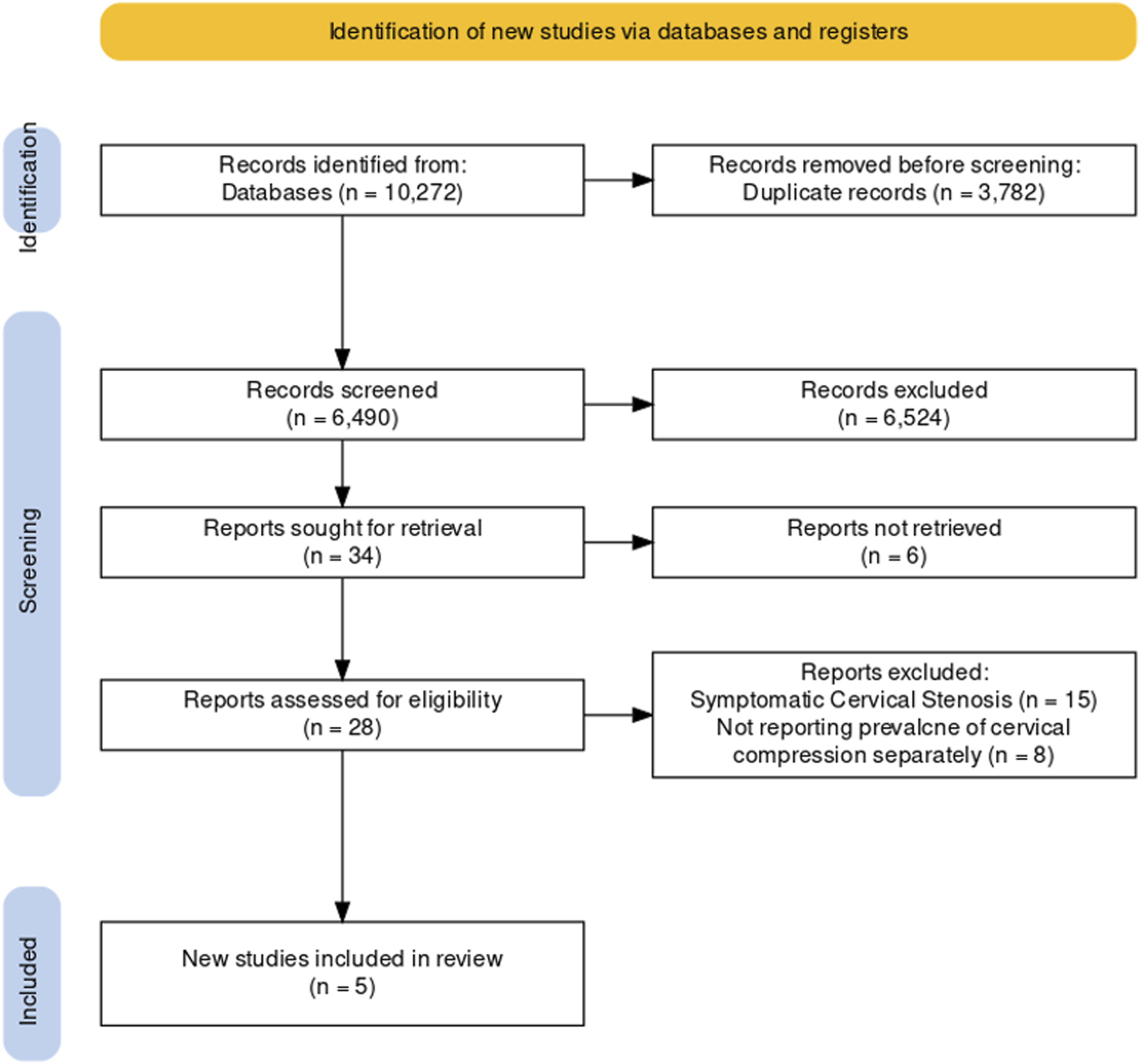
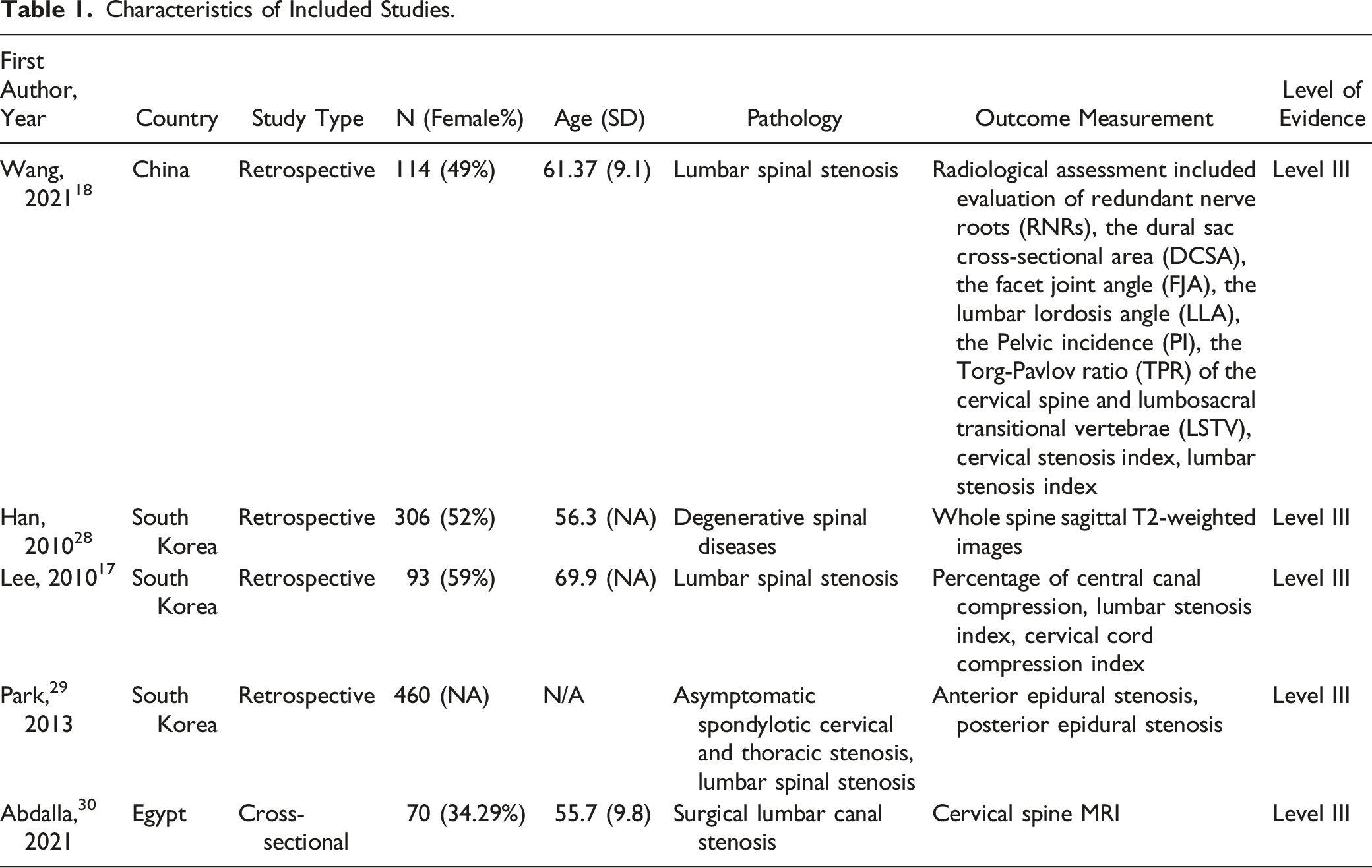
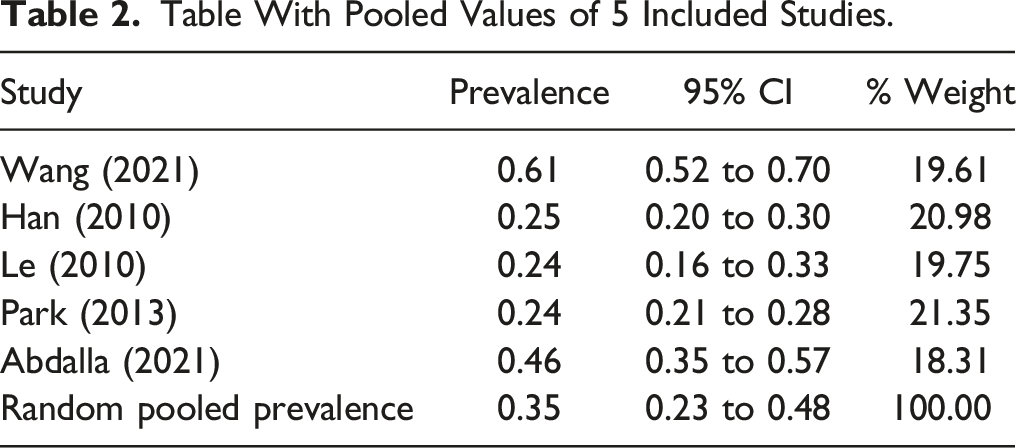
The range of prevalence of asymptomatic CSCC in patients with LSS in these five studies was between 24 to 61 percent. In the Wang et al study,
18
141 cases of LSS with a mean age of 61 ± 9.1 years were evaluated for CSCC, and the reported prevalence was 61 percent (95% CI: 52 to 70). This study found that LSS symptom duration, the presence of redundant nerve root, dural sac cross-sectional area, and pelvic incidence were significantly associated with the risk of CSCC. Additionally, a strong positive linear relationship was reported between the lumbar stenosis index (LSI) and the degree of CSCC. In the Han et al study,
28
the prevalence of CSCC in patients with LSS was reported as 25%. In contrast to the Wang et al study, there was a significant difference in the prevalence of CSCC in patients under and over 40 years old.18,28 In the Lee et al study, the prevalence of CSCC in patients with LSS was reported as 24%.
17
Similar to the Wang et al study, a positive linear relationship was found between LSI and CSCC.17,18 In the Park et al study, the prevalence of CSCC in TSS was also reported as 24%.
29
Abdalla et al study noted a 46% incidence.
30
In two of the five studies, the prevalence was reported as 24 percent and a third study reported the prevalence as 25%. The random pooled prevalence is 35% (95% CI: 23 to 48) as seen in Figure 3 and Table 2 Meta-analysis of the prevalence of asymptomatic cervical spinal cord compression (CSCC) in individuals with lumber spinal stenosis (LSS). Table With Pooled Values of 5 Included Studies.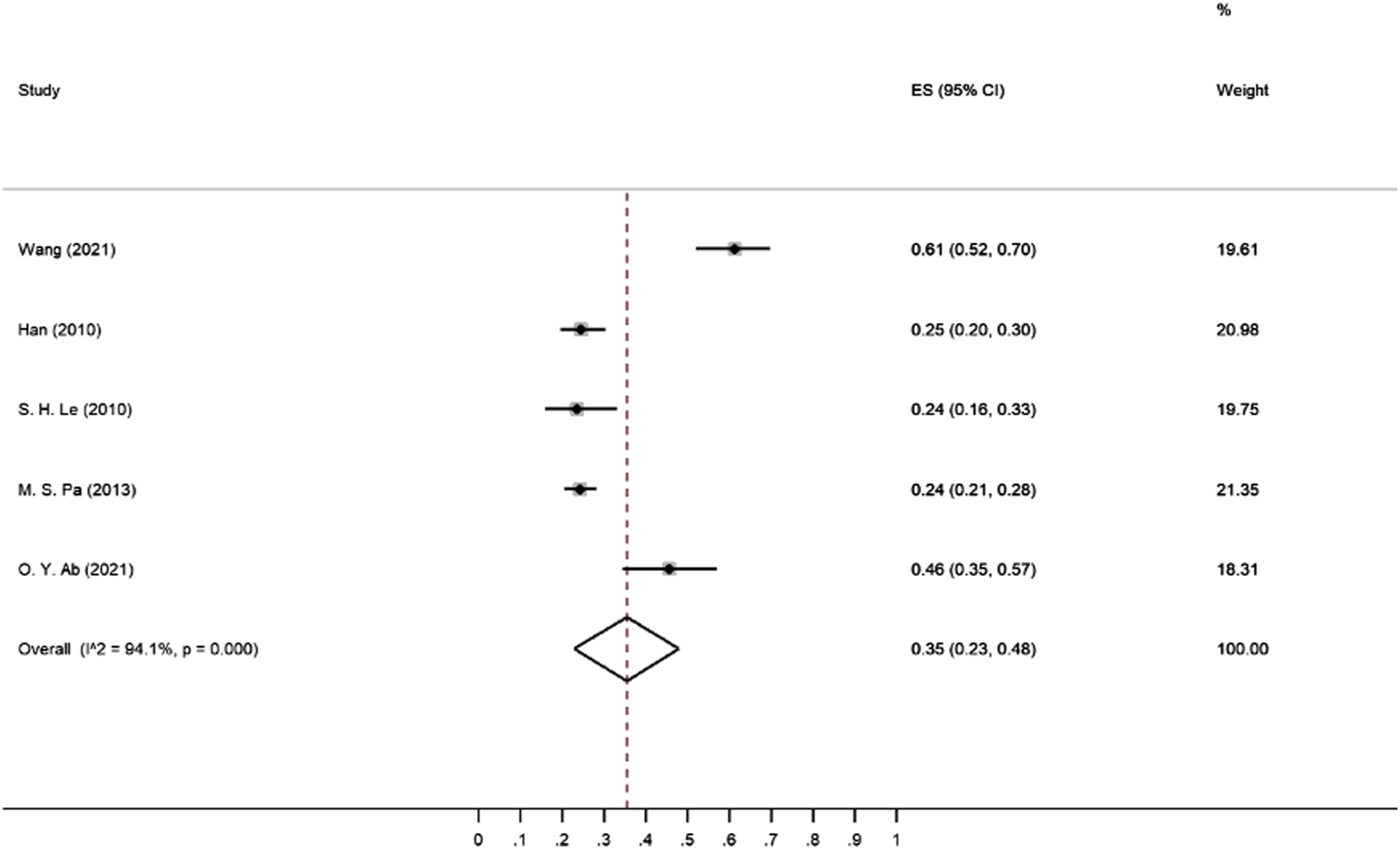
Discussion
In the current study, there was a pooled prevalence of asymptomatic CSCC in symptomatic LSS patients of 35% (range: 24-61). Asymptomatic CSCC is not uncommon and prevalence rates are known to increases with age, with a reported prevalence between 25%-60% in patients over 60 years old.12,31 However, in LSS patient, asymptomatic CSCC may be related to factors beyond the simple aging process. 17 There is little data on the natural history of asymptomatic cervical stenosis, but one study with a 4-year follow-up indicated that 19.7% of these patients became symptomatic. 13 Additionally, pain in the lower limb in LSS may be caused by CSCC as pressure on the cervical spinal cord can stimulate the nerve track connecting the spinothalamic tract of the spinal cord to the lower limb.17,21,31 In these patients, surgical treatment of LSS may not result in sufficient clinical outcomes if the source of lower limb pain is CSCC.14,32-34 Furthermore, prolonged surgical positioning in individuals with LSS, including the commonly employed prone or lateral positions during spine operations, can lead to worsening of cervical compression and possible neurologic injury.17,23 Hence, it is imperative to exercise increased caution when initially positioning LSS patients at the outset of surgery. Furthermore, regular positional reassessments during extended procedures are recommended. This approach will help prevent circumstances that could potentially result in heightened compression within the cervical spine.
This meta-analysis presented the specific prevalence rates of asymptomatic CSCC among different demographic groups. According to one analysis, the prevalence of CSCC without signs and symptoms of myelopathy in a healthy population was 24.2%, and it increases to 35.3% in individuals over 60 years of age. 35 Interestingly the pooled prevalence of asymptomatic CSCC in patients with symptomatic LSS is 35%, which is close to their findings for patients over 60 years old. While we were not able to perform subgroup analysis based on age, these findings might suggest that although healthy patients under 60 years old have asymptomatic cervical cord compression in about 24%, However, the prevalence could be higher in patients with LSS in the same age group, making them at higher risk for developing DCM as they have long years to live.
Thus the progression rate of cervical myelopathy in patients with CSCC is between 1%-5% per year, and this risk is cumulative over time, putting younger patients at a higher risk.13,36,37 Thus, a patient with CSCC has a 50% chance of progression of myelopathy over 20 years. 38 Additionally, certain patient factors, such as younger age and a lack of access to healthcare, may further increase this risk. It is important to take these factors into account when deciding on treatment and follow-up options.
Several screening tools for cervical myelopathy (DCM) have been proposed,39–41 with one method suggested by Nouri et al. 41 targeting patients with lumbar radiculopathy or LSS. This method assigns points based on the presence of signs or symptoms of DCM, as well as comorbidities that predispose or are frequently associated with cervical myelopathy. Patients with a score of ≥3 points are recommended to undergo a cervical MRI examination. Preliminary results of this screening method showed that out of 97 patients screened, 26 screened positive (≥3 points) and 18 had a subsequent cervical MRI. Of the 18 patients, 7 (38.9%) were diagnosed with cervical myelopathy. 41 This suggests that if this screening method were used in a population of 100 patients with lumbar symptoms, only about 7% would be diagnosed with DCM based on their cervical MRIs. However, our findings indicate that if all 100 patients with lumbar symptoms underwent cervical MRI, even without any DCM symptoms, about 35% of them should have CSCC in their imaging. This suggests that while the screening method proposed by Nouri et al. 41 may be cost-effective, one can also consider screening patients with symptomatic LSS.
In comparison to another meta-analysis by Smith et al., 35 which found a 24.2% prevalence of asymptomatic CSCC in the general population, our focused review revealed a higher prevalence (35%) in patients with symptomatic LSS. This difference could be attributed to the presence of degenerative spinal processes in LSS patients or congenital stenosis, potentially making them more prone to develop similar conditions in other parts of the spine. While Smith et al.’s study provides a valuable epidemiological insight into the prevalence of spinal cord compression; it does not specifically address the value of cervical MRI screening in patients already undergoing MRI for LSS. Our data suggests the potential benefit of such an approach in detecting co-existing pathologies early, possibly improving patient outcomes, but more studies are required to substantiate these preliminary findings.
Prior research indicates that patients with imaging signs of spinal cord compression but no evident myelopathy symptoms, can still show electrophysiological markers of cervical radiculopathy or central conduction deficit.42,43 These markers may herald the onset of myelopathy. Furthermore, the AOSpine Clinical Practice Guideline for DCM suggests that such patients be informed about the potential risk. 8 It even proposes considering either surgical treatments or non-operative approaches such as routine monitoring or structured rehabilitation as options. 8 However, a considerable knowledge gap exists in our understanding regarding the risk of developing myelopathy in asymptomatic CSCC patients who also exhibit symptomatic LSS, compared to CSCC patients without LSS. This study underscores the necessity for further research in this area. It remains to be seen whether these patients carry similar or even higher progression risks compared to patients with electrophysiological abnormalities, particularly since an additional symptomatic degenerative pathology may be present in another part of the spine. This could potentially alter the risk prediction and treatment strategies in this subset of patients.
Quantitative MRI methodologies such as Diffusion Tensor Imaging (DTI) may serve as a tool for categorizing patients according to risk levels. A multitude of research efforts have unanimously indicated a correlation between fractional anisotropy and mean diffusivity with disease severity, along with clinical parameters in DCM. 44 Furthermore, fractional anisotropy has been observed to be diminished at the compression site in asymptomatic patients. 45 Additionally, it has been proposed that the duration of symptoms warrants deeper exploration concerning its impact on DTI parameters in upcoming DCM research. 46 This insight could be integrated into clinical procedures, implying that DTI parameters or alternative quantitative imaging techniques might aid in better understanding the progression risk in asymptomatic CSCC amongst patients with symptomatic LSS.
While this study has presented insightful findings, certain limitations should be factored into the interpretation of its results. To begin with, the analysis incorporated a rather limited set of studies, totaling five, which may not offer a comprehensive view of the subject matter. However, the 95% CI of the pooled prevalence for asymptomatic CSCC in symptomatic LSS patients lies between 23% and 48%. This indicates that future investigations might yield results within this interval. Therefore, even at the lower limit, nearly one-quarter of symptomatic LSS patients might present with asymptomatic CSCC. This represents a sizable patient group worthy of consideration.
An additional limitation of this study is that it exclusively comprises retrospective and cross-sectional studies, rated as level III evidence. This classification extends to the pooled analysis, making it level III evidence as well. Although more robust evidence levels would have been preferable, our primary objective was to resolve a clinical question: how many patients undergoing medical examination and imaging for LSS concurrently present with asymptomatic CSCC? Until more rigorous studies emerge, cross-sectional or retrospective studies provide an appropriate framework to answer this query. Hence, we maintain that even with the level III evidence, this pooled analysis carries significant clinical relevance and is sufficiently supported by this evidence tier.
Additionally, the lack of age-specific data on the prevalence of CSCC in the included studies makes it difficult to draw conclusions about specific age groups. Furthermore, the inconsistent definition of asymptomatic patients across studies may have resulted in underreporting or over reporting of the condition. Another important limitation to be aware of is that some of the included studies included patients who had undergone surgery for LSS, which may mean that these patients had a more severe degenerative disease and it is not possible to determine how the results vary based on disease severity.
Conclusions
Approximately a third of patients with symptoms of LSS may also have concurrent radiographic cervical stenosis. A careful physical evaluation should be performed on these LSS patients to confirm no myelopathy symptoms due to the high rate of cervical stenosis in this population. These patients may develop new neurological symptoms in the form of DCM in the future. Based on these findings, we also strongly recommend that spine surgeons exercise particular caution during the positioning of patients who are undergoing surgery for lumbar stenosis.
Supplemental Material
Supplemental Material - The Prevalence of Asymptomatic Cervical Spinal Cord Compression in Individuals Presenting With Symptomatic Lumbar Spinal Stenosis: A Meta-Analysis
Supplemental Material for The Prevalence of Asymptomatic Cervical Spinal Cord Compression in Individuals Presenting With Symptomatic Lumbar Spinal Stenosis: A Meta-Analysis by Farzin Farahbakhsh, Sepehr Khosravi, Vali Baigi, Masoud Pourghahramani Koltapeh, Amirmahdi Khayyamfar, Zahra Eskandari, Zahra Ghodsi, James Harrop, and Vafa Rahimi-Movaghar in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tehran University of Medical Sciences, [grant number is 1401-4-101-63630].
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.