
Abstract
Introduction
Degenerative lumbar spinal stenosis (DLSS) is an age-related condition that consists of chronic compression of nerve roots due to osteoarthritic changes in the spine. 1 The reduction in the spinal canal diameter disturbs the blood supply and function of the neurological structures of the region, thus generating radicular pain, neurological deficit, and neurogenic claudication.1,2 In addition, it can be related to mechanic instability that may result in back pain and segmental hypermobility observed in images of the lumbosacral spine. 2 Non-surgical management is usually indicated as the first treatment line, and that strategy is enough to alleviate the symptoms in most cases. However, surgical decompression and fusion of the unstable segments may be recommended when conservative approaches become ineffective.3-6
The surgical options include various techniques classified into 2 main categories; direct decompression (DD) and fusion procedures consist of a posterior-only approach to resect bone, ligament, cyst, or disc material causing the nerve impingement, followed by instrumented fusion with screws and an interbody device such as a PLIF (posterior lumbar interbody fusion) or a TLIF (transforaminal lumbar interbody fusion).7-9
Indirect decompression (ID) procedures encompass inserting a large interbody device through an abdominal approach that restores the disc height and spinal canal dimensions by stretching the ligaments.7-9 This way, the nerve roots impingement can be resolved without resecting any structure. This category includes anterior, lateral, and oblique lumbar interbody fusion (ALIF, LLIF, OLIF, respectively) techniques.7-11
Although both strategies have proved to be safe and effective in reducing symptoms in patients with DLSS and instability, there is no clear recommendation for using 1 or the other. Moreover, there is a knowledge gap concerning the differential effectiveness of these techniques to treat such patients. Accordingly, we decided to conduct a systematic review of the literature and meta-analysis to respond to that question.
Our primary objective was to compare the clinical outcomes of pain and disability for both strategies to treat patients with degenerative lumbar spinal stenosis and instability. Secondary aims were to determine if the complications rate, blood loss, and surgical timing differed.
Methods
Types of Studies
Our study intended to analyze experimental, prospective, randomized clinical trials. However, observational, comparative investigations, including case-control or cohort (prospective or retrospective) studies, were also considered. Duplicate publications, review articles, case reports and case series, conference papers, letters were not eligible.
Types of Participants
Adult (>18 years old) participants diagnosed with degenerative lumbar spinal stenosis and instability were included. The diagnosis of LSS was made through the clinical setting and imaging, including MRI or CT myelography demonstrating a reduction in the spinal canal diameter. Instability was defined if at least 1 of these findings was present in the report12,13: 1. Significant (VAS > 7) mechanical back pain (pain that increases with loading). 2. Flexion-extension lumbar X-Ray showing at least 3 mm of slippage between 2 vertebral bodies, or 11° of rotational angulation. 3. Degenerative Spondylolisthesis
Articles related to participants with previous lumbosacral procedures, more than 3 pathological segments, spinal deformity (coronal Cobb angle > 30°, sagittal SVA > 10 cm), pathology other than degenerative, < 6 months of follow up, and studies with less than 15 participants were excluded.
Types of Interventions
Studies were not excluded based on the expertise of the surgical team, the assistive technology used (e.g., neuronavigation, fluoroscopy, free-hand technique), or the hardware provider. However, we only included those related to participants treated with lumbar interbody cages and screws, including standard (pedicular screws) or cortical bone trajectory (CBT) techniques. Articles about “dynamic” stabilization hardware (e.g., interspinous process devices) and arthroplasty procedures were excluded.
Intervention Group: ID
Patients in this group were treated with a combined procedure including abdominal and posterior stages, either synchronic or a-synchronic, with or without positioning change (e.g., single-position, flipping, etc.). The abdominal stage involved the insertion of a lumbar interbody device (LIF) using an anterior (ALIF), lateral or direct (LLIF), or oblique (OLIF) technique. The posterior stage included stabilizing the affected segments utilizing screws and rods. This last stage did not include any resection of posterior arch structures (e.g., lamina, facet joints, ligaments, etc.). Articles that included 10% or more of participants who received direct decompression techniques were excluded.
Control Group: DD
Patients in this group were treated with a posterior-only intervention. This procedure included instrumentation and resectioning any tissue thought to compress the neural structures. This resection could involve laminectomy, facetectomy, flavectomy, and any combination of them. Also, this procedure could involve the insertion of a lumbar interbody device (e.g., TLIF, PLIF)
Types of Outcome Measures
To acknowledge any difference in the effectiveness of these surgical strategies to reduce radicular and lumbar symptoms in patients with LSS and instability, we evaluated postoperative pain and disability. Articles that did not report at least 1 of these endpoints were excluded from the analysis. Also, to evaluate the invasiveness of the treatments, the surgical complications rate, blood loss, and surgical time as secondary outcomes were analyzed.
Primary Outcomes
Pain was evaluated using the visual analogue scale (VAS) instrument. As the outcome measure, postoperative VAS value (single post-intervention assessment) at 12 months after the surgery was used.
Disability was assessed using the Oswestry Disability Index (ODI) and the Japanese Orthopedics Association Back Pain Evaluation Questionnaire (JOABPEQ)14-16 measured at 12 months postoperative. Both metrics were analyzed as single post-intervention measures.
Secondary Outcomes
The complication rate was assessed considering the number of patients over the number of participants in each group (risk ratio). Clinical and surgical adverse events (e.g., surgical site infection, hematoma, neurological deficit, vascular lesions, visceral lesions, hardware failure) were included.
Intraoperative blood loss considered the volume of blood loss throughout the procedure and was analyzed as a continuous variable expressed in millilitres. Surgical time was measured in minutes and considered a continuous variable.
Search Methods for Identification of Studies
The literature review was conducted using the following sources: 1. The Cochrane Controlled Register of Controlled Trials (CENTRAL), employing the Cochrane Database of Systematic Reviews (CDSR) 2. MEDLINE PubMed 3. Science Direct
The last search was conducted on August 12, 2021. Authors decided not restrict the search based on the date of publication, language, publication status or format.
The detailed PICO and the search strategy can be found in Supplemental Appendix 1. The search strategy was constructed after discussion and consensus of all authors.
Selection of Studies
Two authors (MG, EY) independently inspected the bibliographic quotes and identified relevant abstracts. The full text was analyzed and discussed in detail when disagreement was present. A third independent author (AG) was consulted if an agreement was not reached. Elimination of duplicated articles and selection of eligible studies was done using Rayyan (https://rayyan.ai/reviews/259507).
Data Extraction and Management
Two investigators (AG, GCW) conducted data extraction independently. The software Google Forms was used to create a data collection sheet to ensure consistency and compare information extracted in duplicate. Also, the form was piloted with 5% of the included articles to assess usability. A third author (JPC) discussed disagreements on the data when observed a significant discrepancy. When numerical information was unavailable in tables or the manuscript, data was extracted from graphics and figures using the software PlotDigitalizer (version 2.6.9).
Assessment of Risk of Bias in Included Studies
Two investigators (CC, AMC) independently assessed the risk of bias for primary outcomes using the Risk of Bias in non-randomized studies of interventions (ROBINS I) tool. 17 A third author (AFJ) discussed disagreements when a significant discrepancy was present.
Measures of Treatment Effect
For dichotomic values (e.g., complications and adverse effects), a standard estimation of relative risk using a confidence interval of 95% was calculated. Continuous metrics, including pain, blood loss, and surgical time were compared by analyzing the mean difference (MD). For disability, the standardized mean difference (SMD) between groups was used since there were 2 different tools to assess that outcome (ODI and JOABPQ). 18
Dealing With Missing Data, Publication Bias, and Heterogeneity Assessment
Articles were excluded from the final analysis if outcome data was unavailable for both primary endpoints. Statistical heterogeneity was assessed utilizing visual inspection of graphics and using the I2 test. The authors considered substantial statistical heterogeneity when the value of I2 was above 50%, and in those situations, an assessment of reasons for that heterogeneity was performed. 18 Funnel plot analysis was conducted to determine the possible effect of small unreported studies. 18
Data Synthesis
Data was analyzed using the software RevMan version 5.4.1. When there was evidence of homogeneity among studies, a fixed-effects model was performed. However, if significant heterogeneity (defined as an I2 statistic of 50% or more) was present, a random-effect model was used. The statistical analyses were conducted following the guideline of the Cochrane Handbook for Systematic Reviews of Interventions (v6.2). 18
Protocol Registration, Quality, and Evidence Assessment
The protocol was registered at PROSPERO on November 15, 2021. 10
The review was conducted as protocol, except for changes in the participating authors.
AMSTAR 2 checklist to evaluate the study quality was used. 19 The report was performed following the PRISMA guideline. 20
Global certainty of evidence was assessed using the GRADE framework and software (GRADEpro GDT: GRADEpro Guideline Development Tool [Software]. McMaster University and Evidence Prime, 2021. Available from gradepro.org).
Results
Results of the Search
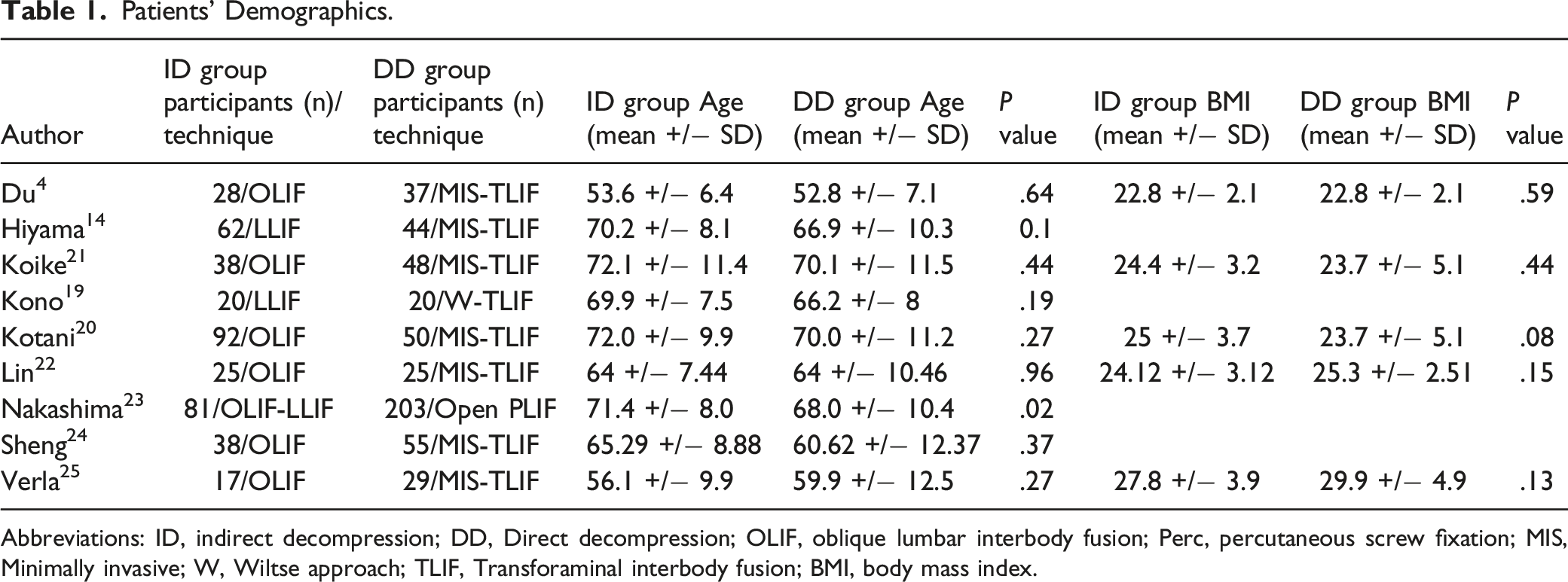
A total of 1935 articles were identified from the 3 databases consulted. Of the 1575 non-duplicate papers examined and evaluated, 20 met the inclusion criteria and were full text analyzed; 10 were excluded after examination and 1 after data extraction. After careful assessment, the data of the 9 included articles were extracted. The flow of studies and the demographics of the selected articles can be depicted in Figure 1 and Table 1. PRISMA flow chart. Patients’ Demographics. Abbreviations: ID, indirect decompression; DD, Direct decompression; OLIF, oblique lumbar interbody fusion; Perc, percutaneous screw fixation; MIS, Minimally invasive; W, Wiltse approach; TLIF, Transforaminal interbody fusion; BMI, body mass index.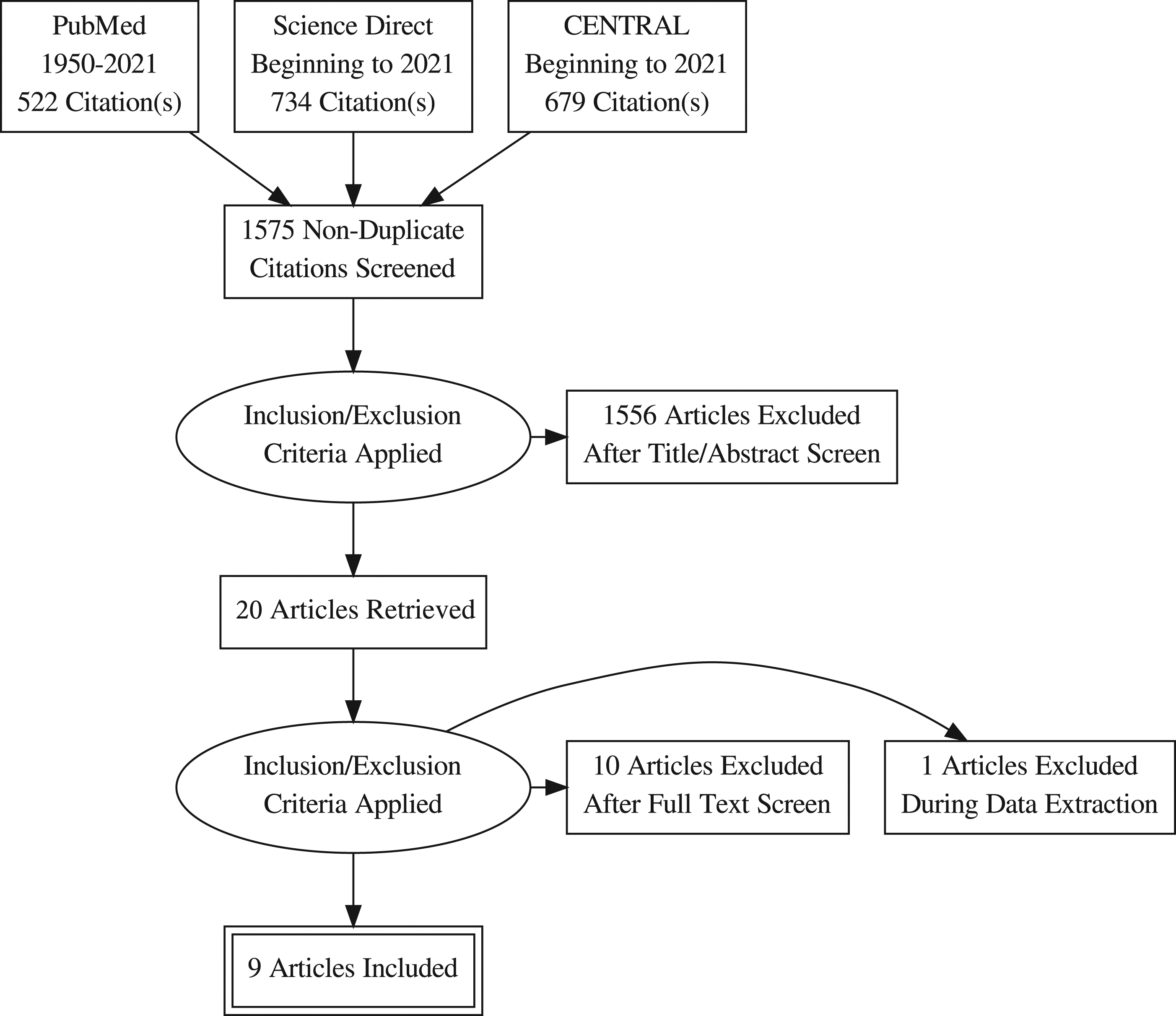
Included Studies
Nine retrospectives and comparative studies were included in this systematic review and meta-analysis. No prospective, randomized, controlled trials were identified. A total of 1004 patients were included, accounting for 452 (45%) in the indirect decompression and fusion (ID) group and 552 (55%) in the direct decompression and fusion (DD) group.
The main findings of the analyzed studies are summarized below:
Du et al. compared the outcomes of patients treated with OLIF and percutaneous screws instrumentation (OLIF+Perc) vs TLIF using the Wiltse approach (W-TLIF). 26 Allocation of patients was done according to the feasibility of performing the OLIF technique after assessing the preoperative CT and MRI. Accordingly, direct decompression and fusion were indicated in patients with no corridor between the psoas and the aorta. Surgical time and blood loss were significantly lower (P < .001 both) in the ID group. However, there was no significant difference between the 2 groups considering disability (P = .088) and pain (P = .064) nor in the complication rate (14.3% vs 16.2%, P = .446).
Hiyama et al. compared the outcomes of patients diagnosed with degenerative lumbar spondylolisthesis treated with LLIF and percutaneous screws instrumentation (LLIF+Perc) or direct decompression using minimally invasive TLIF (MIS-TLIF) technique. 27 Participants' characteristics were similar between both groups, except that 5 patients in the ID group had a 3-level procedure against 0 in the DD group. They found that surgical time and blood loss were significantly lower (P < .001 both) in the ID group, but there was no significant difference in the postoperative pain (P = .064) at 12 months of follow-up.
Koike et al. analyzed clinical and imaging outcomes in patients treated with single-level decompression and fusion procedure. 22 Group ID had OLIF and percutaneous screws instrumentation (OLIF+Perc), and group DD an MIS-TLIF. The allocation of patients was unclear. They found that surgical time and blood loss were similar in both groups and that there was no significant difference in the disability and pain at 12 months of follow-up. The main limitations of this study are related to the allocation of patients according to a specific time frame and not to their clinical or radiographic features.
Kono et al. compared the outcomes of 40 patients diagnosed with unstable degenerative lumbar spondylolisthesis at the L3-4 or L4-5 levels treated with LLIF (n = 20) and posterior instrumentation and those who had direct decompression (n = 20) and Wiltse TLIF. 28 Participants' allocation was time-based, and those who were treated before November 2014 received a DD procedure and those after an ID procedure. Although they found that surgical time and blood loss were significantly lower (P < .001 both) in the ID group, there was no significant difference in the postoperative disability at 12 months of follow-up. In terms of complication rate, there was a significant difference between groups; 55% in the ID group and 15% in the DD group experienced undesired postoperative events (P < .05).
Kotani et al. reviewed the cases of 142 patients who underwent decompression and fusion surgery for degenerative LSS and instability at the L3-4 and L4-5 segments between 2013 and 2018. 29 Group ID had an OLIF and percutaneous screws instrumentation (OLIF+Perc), and group DD an MIS-TLIF. The preoperative background of patients significantly differed in terms of lumbar function and mental health according to the JOABPEQ tool. Moreover, the allocation of patients was based on the time frame they were operated. Indeed, those treated before 2015 received MIS-TLIF, and those after had OLIF procedure. They found that surgical time and blood loss were similar in both groups and that there was no significant difference in the disability and pain at 12 months of follow-up. The main limitations of this study are related to the allocation of patients according to a specific time frame and not to their clinical or radiographic features. Also, there is a high risk of patients overlapping between this study and Koike et al. 22 There is no information regarding this in the report.
Lin et al. reviewed the medical records and images of patients treated with single-level decompression and fusion with OLIF or MIS-TLIF in the 2012-2017 period. 30 They included 25 patients treated with OLIF (ID group) and selected 25 matched controls who had MIS-TLIF procedure (DD group). They found that operative time and blood loss were significantly lower in the ID group than in the DD. However, they could not demonstrate any difference in complication rate, pain, and disability. The authors excluded those participants with OLIF at L4-5 that required further decompression due to persistent symptoms.
Nakashima et al. retrospectively reviewed the outcomes of a cohort of participants that received surgery for lumbar spinal stenosis and spondylolisthesis. 31 Group ID included 81 participants treated with OLIF or LLIF and posterior instrumented fusion, and group DD 203 patients with conventional PLIF. The pre-intervention background was similar, except for mean age and higher fusion levels in the ID participants. The data showed that pain, disability, and complication had no significant difference among groups. The authors excluded participants with neurological deficits from the ID but not from the DD cohort.
Sheng et al. compared the results of a cohort of patients diagnosed with symptomatic lumbar spondylolisthesis and stenosis treated with MIS-TLIF or MIS-OLIF. 23 Out of 202 patients in the cohort, only 38 were included in the ID group and 55 in the DD group. Although inclusion and exclusion criteria are mentioned in the report, it is unclear how they allocated patients to 1 or the other treatment group or selected the study’s final participants. Age and female populations were significantly higher in the ID group, and there was no statistical method to assess this potential confounder. However, they found that the surgical time and blood loss were significantly lower (P < .001 both) in the ID group. The primary limitations include an incomplete description of interventions, inclusion and exclusion criteria, and assessment and mitigation of confounders.
Verla et al. analyzed the clinical outcomes of patients that underwent single-level LLIF (ID, n = 17) or TLIF (DD group, n = 29) for the treatment of degenerative lumbar spondylolisthesis and stenosis. 32 Postoperative pain and ODI at 12 months did not differ between groups (VAS = ID: 3.7 +/− 2.4 vs DD: 2.6 +/− 2.6, P = .60; ODI: ID 23.12 +/− 14.3; DD: 26.71 +/− 11.6; P = .30). The average blood loss trended more in the DD cohort; however, it was not statistically significant (P = .09).
Excluded Studies
Characteristics of Excluded Articles.
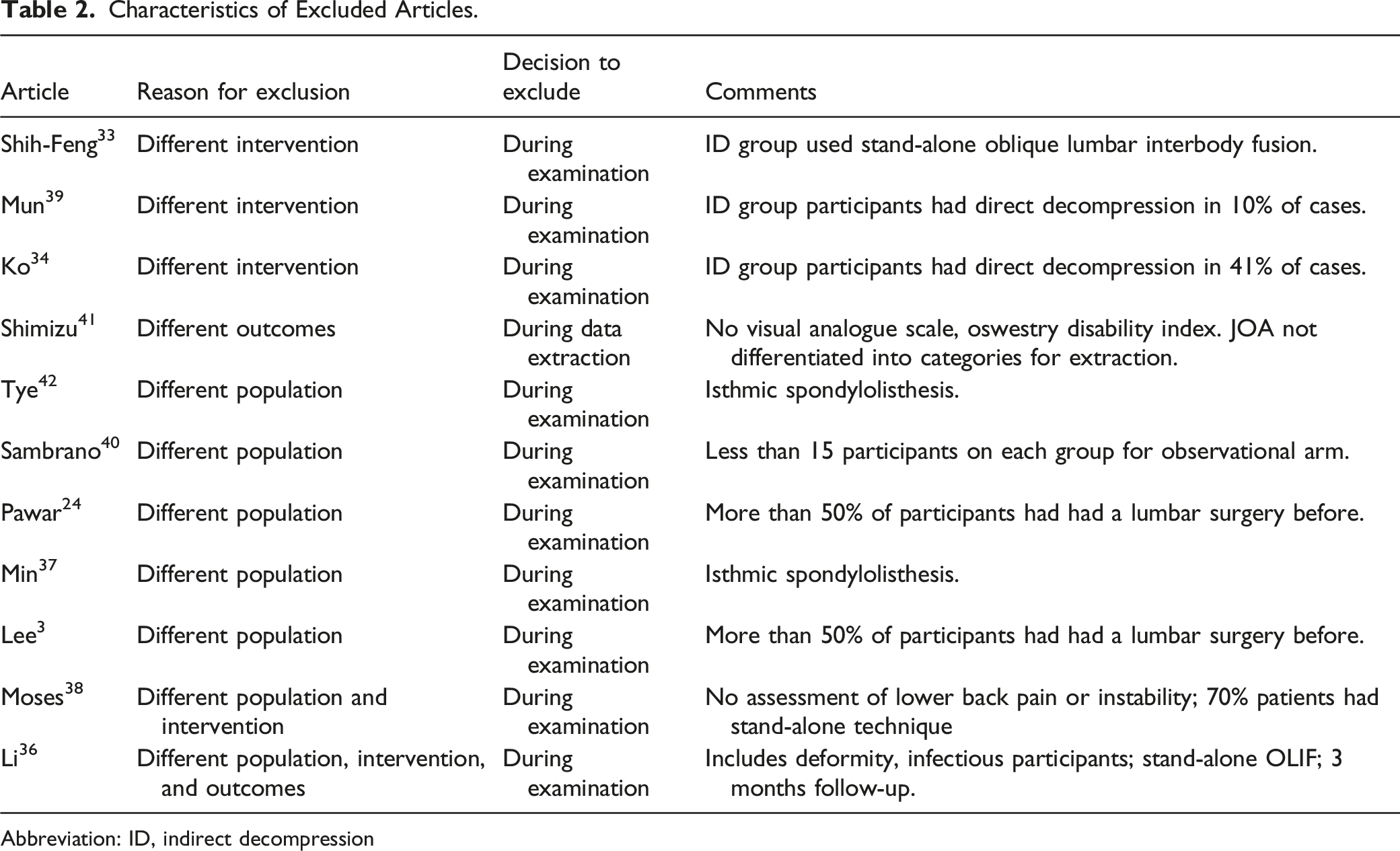
Abbreviation: ID, indirect decompression
Risk of Bias in Included Studies
As previously stated, since we only included retrospective, comparative studies, we used ROBINS I to assess the risk of bias. Figure 2 summarizes the bias assessment for the included articles. Overall, it can be appreciated that except for 1 article,
30
there was no proper assessment of confounders domains nor detailed measures to control them, which can induce bias. Also, 2 studies30,31 excluded from the intervention group (ID) but not from the comparison group (DD) those patients who had severe compressive or claudication symptoms or neurological deficit, thus adding some component of selection bias. The risk in the rest of the categories was unclear or low for most studies. Risk of Bias assessment.
Publication bias was assessed by visual evaluation of the funnel plot for primary outcomes. The graphics showed an asymmetric pattern for pain and symmetric for disability. As stated before, this assessment should be carefully interpreted.
Effects of Interventions
Pain
A random-effects model was used since high heterogeneity (I2 = 67%) was present. The VAS score in the indirect decompression group at 12 months was slightly lower (MD -0.18, 95% CI -0.50 to 0.14; participants = 872), but there was no statistical difference (Figure 3). Among the included articles, only one did not include data regarding pain.
28
Forest plot for pain.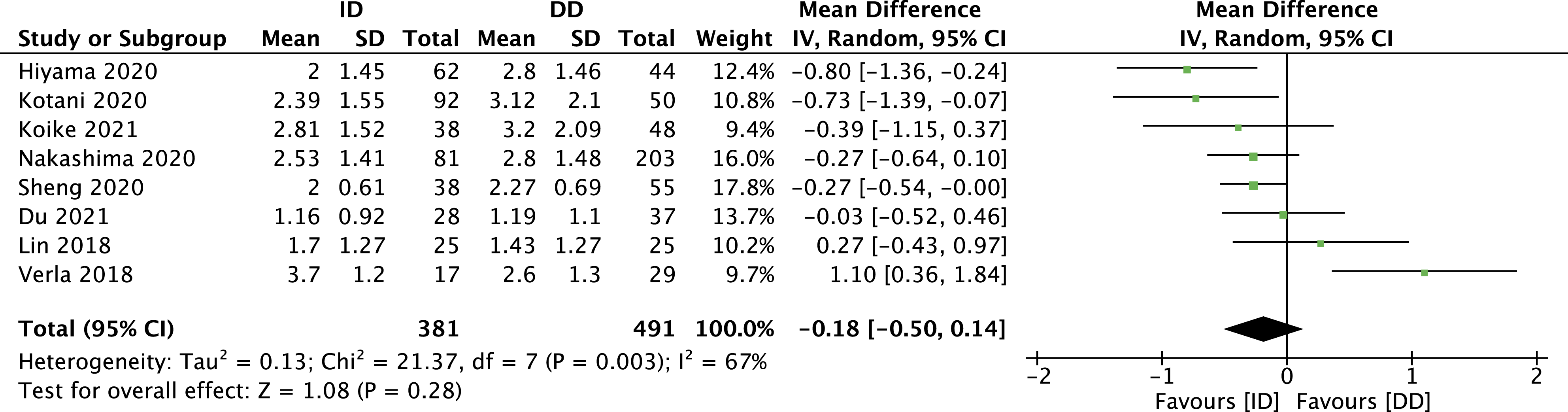
Disability
For disability, the heterogeneity was low (I2 = 39%); thus, a fixed-effect model was used. Since there were 2 different metrics for this outcome (ODI and JOA), we analyzed the standard mean difference (SMD). Although a minimal difference favoured the ID group, it was insignificant (SMD -.17, 95% CI -.35 to .00: participants = 578) (Figure 4). Three articles did not include this outcome in their report.22,27,29 Forest plot for disability.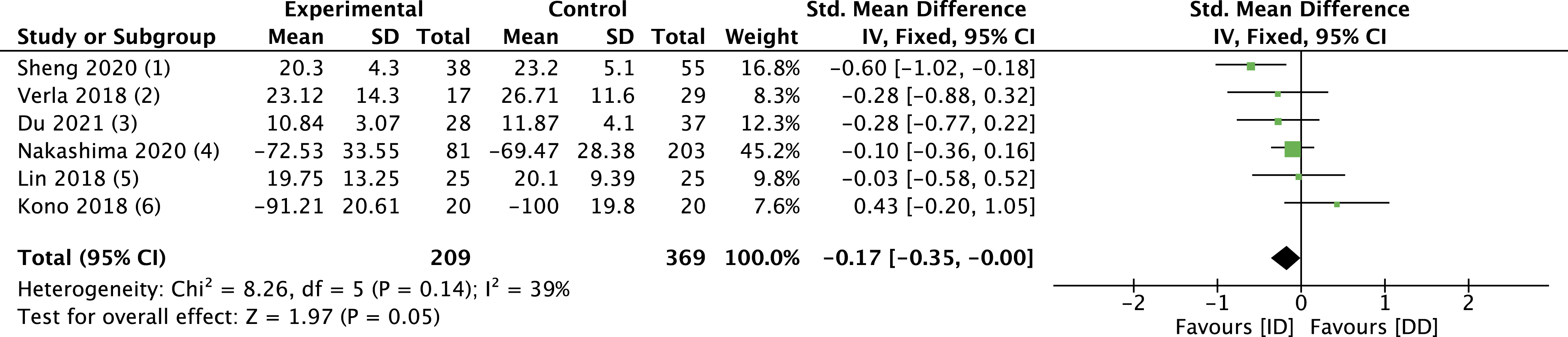
Postoperative Complications
Out of 401 participants in the ID group, 63 experienced a postoperative complication, and 75 were reported among the 511 patients enrolled in the DD group. The statistical analysis showed no difference in the risk of experiencing an adverse event between groups (RR 1.02, 95% CI .74 to 1.41: I2 = 0%) (Figure 5). All the included articles reported complications. Forest plot for complications rate.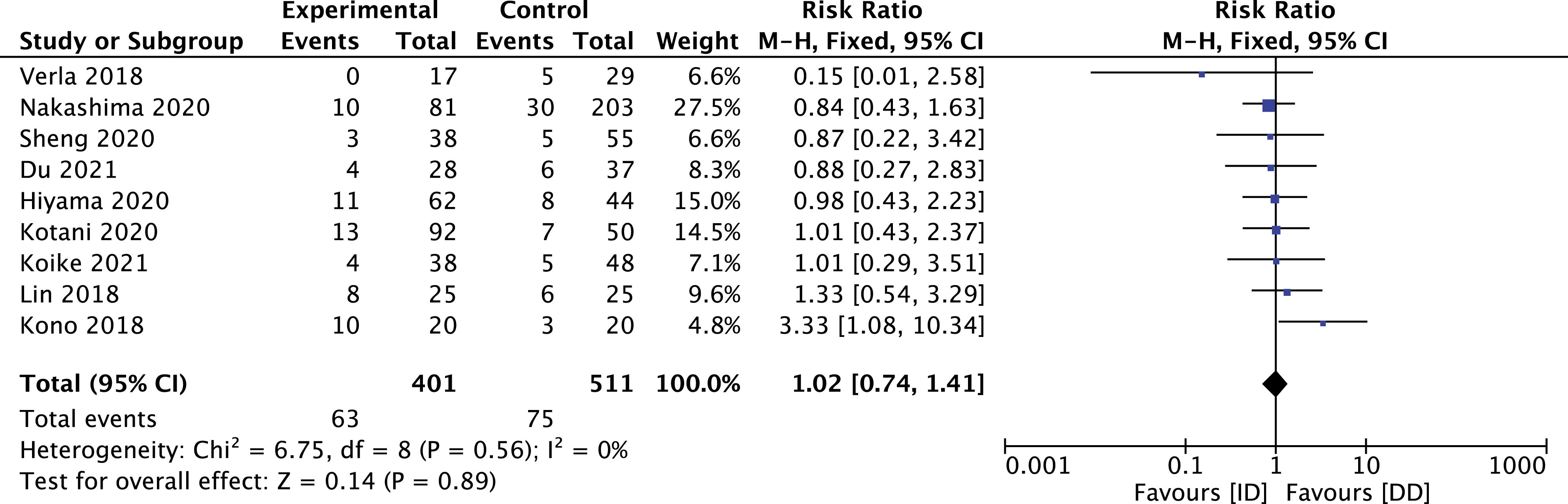
Frequency and Type of Reported Complications.
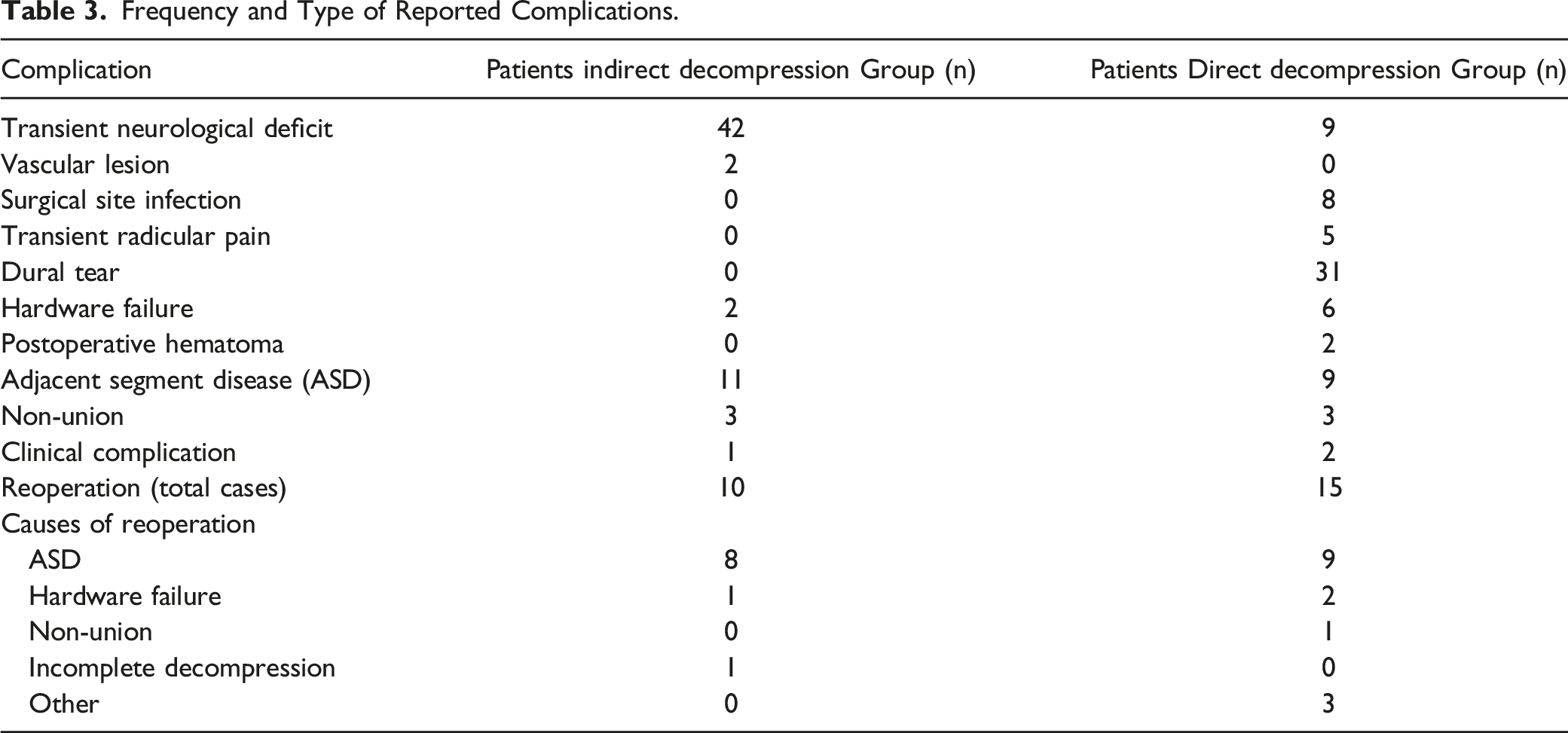
In contrast, the most common complication in the DD group was dural tear (n = 31), but no case required reoperation due to cerebrospinal fluid leak.26-28,30-32 In addition, 8 participants had a surgical site infection and 5 transient radicular pain in the DD group vs none in the ID group. Finally, ten patients in the ID group and 15 in the DD group required a reoperation, most frequently due to adjacent segment disease. In the indirect decompression cohort, 1 case of reoperation was reported to be due to incomplete symptoms relief.
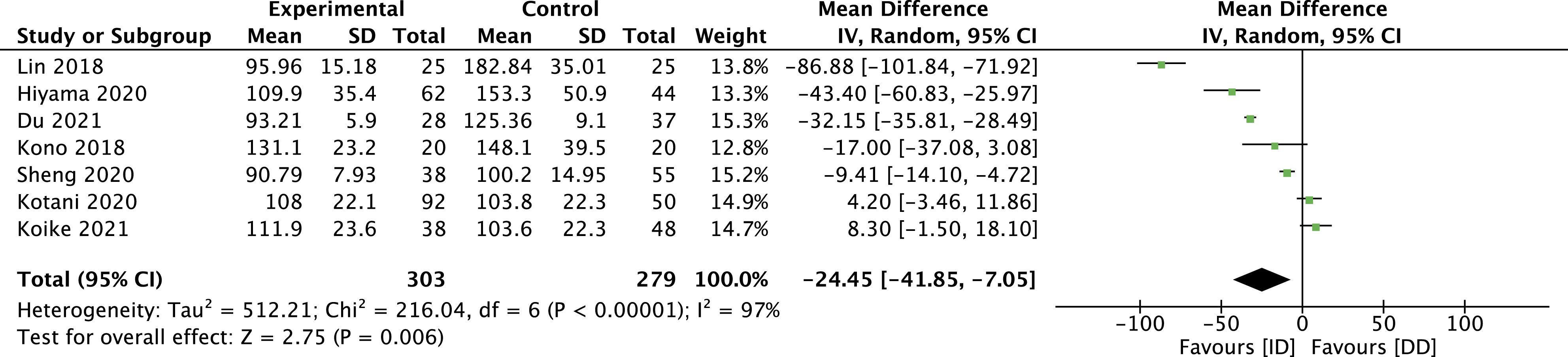
Blood Loss and Surgical Time
These outcomes demonstrated considerable heterogeneity, as demonstrated by an I2 test of 92% and 97%, respectively. Moreover, the reports were incomplete in describing the methodology for measuring them. Notwithstanding, there was a difference in favour of the ID group for both outcomes with a significant statistical difference. Indeed, for blood loss, the mean difference was −84.85 mL (95% CI -117.42 to −52.28), and for the surgical time was −24.45 min (95% CI -41.85 to −7.05) (Figure 6 and 7). Forest plot for blood loss. Forest plot for surgical time.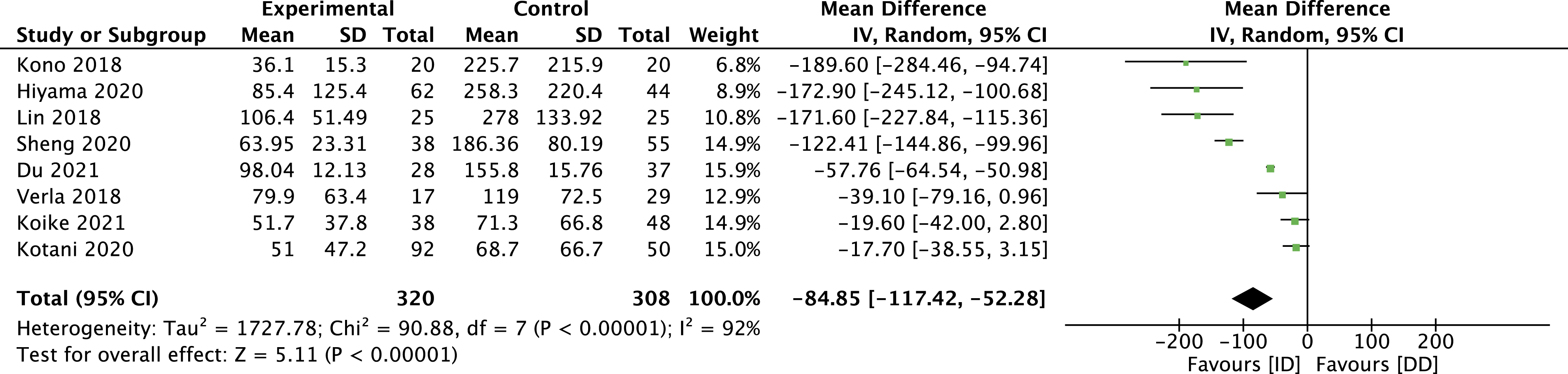
Certainty of Evidence
Summary of Findings (GRADE).
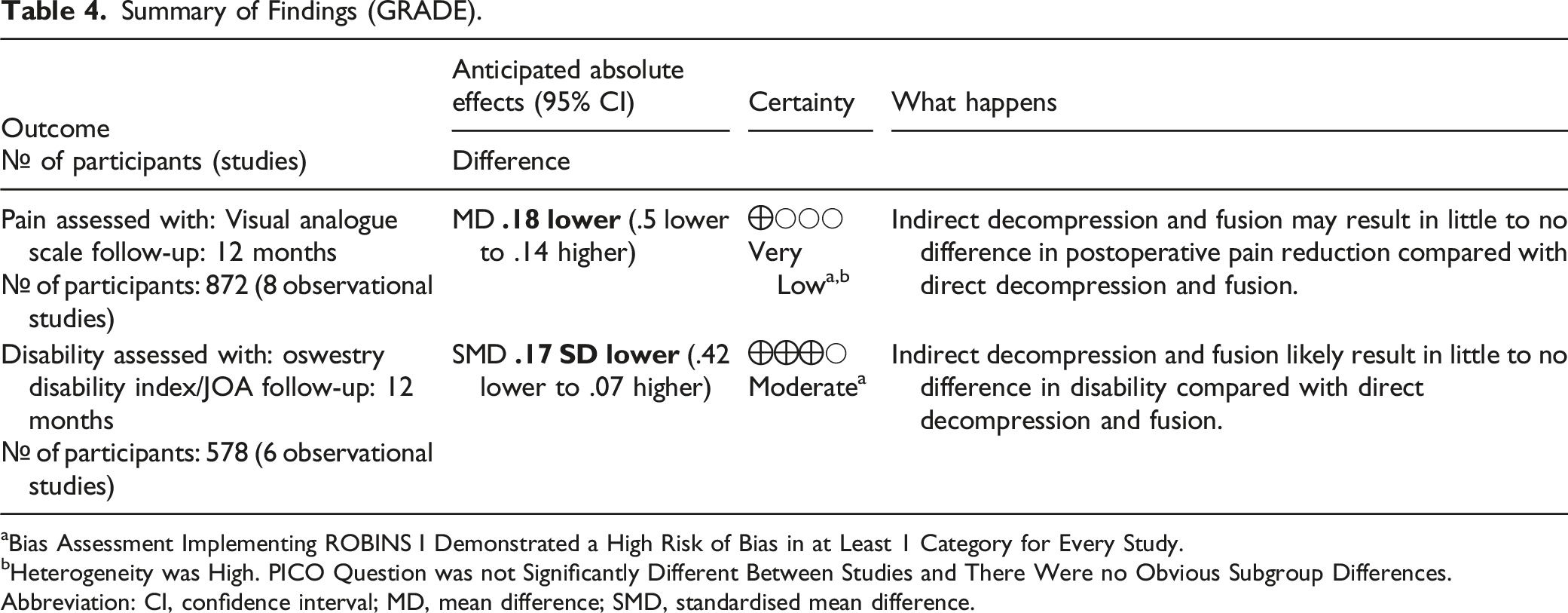
aBias Assessment Implementing ROBINS I Demonstrated a High Risk of Bias in at Least 1 Category for Every Study.
bHeterogeneity was High. PICO Question was not Significantly Different Between Studies and There Were no Obvious Subgroup Differences.
Abbreviation: CI, confidence interval; MD, mean difference; SMD, standardised mean difference.
Discussion
In the setting of intractable leg and lower back pain and evidence of lumbar spinal stenosis and instability, there is an agreement to perform a decompression and fusion procedure.4,6,43 However, there is a lack of robust evidence to select the most effective strategy among the variety of techniques available.
Our systematic review and meta-analysis showed that patients diagnosed with lumbar spinal stenosis and instability due to degenerative conditions had similar clinical outcomes if treated with indirect or direct decompression and fusion techniques. Although there was a minimal difference that favoured the ID group in postoperative pain and disability 1 year after the procedure, it was not statistically significant.
These results are consistent with similar publications that explored the effectiveness of these strategies in treating LSS. Cho et al. conducted a metanalysis comparing radiological and clinical outcomes of patients treated with either combined anterior and posterior or posterior-only approaches and demonstrated that postoperative lower back and leg pain were similar between groups. 25 However, it differs from our investigation because the researchers did not assess the role of indirect or direct decompression and included patients diagnosed with isthmic and degenerative spondylolisthesis.
Our analysis revealed no difference in the complication rate between groups. Nevertheless, we could appreciate that the profile of the adverse events was different; in the ID group, it included transient neurological deficit, hardware failure, and vascular lesion, and in the DD group, transient neurological deficit, dural tear, surgical site infection, and hardware failure. The low quality of reporting complications among publications did not allow us to conduct a quantitative analysis.
We also decided to compare the invasiveness of both strategies by assessing intraoperative blood loss and surgical time. Both outcomes showed to favour the ID group significantly, but the heterogeneity of the results was very high. The methodology employed to obtain the data was poorly described in the included articles, and we believe that the source of this variance could be due to dissimilarities in the measurement of these parameters. In addition, although significant from a statistical point of view, the absolute difference was too small to become clinically meaningful. Accordingly, these results should be carefully interpreted.
Our study has several limitations that should be acknowledged. In the first place, although we identified 9 comparative articles and pooled the data from 1004 patients, only 2 studies enrolled more than 50 participants in each group.29,31 Such a small number of participants may lead to increased heterogeneity and reduced applicability of the results.
Secondly, although we tried to stretch our inclusion criteria to accept only studies including participants with symptomatic lumbar spinal stenosis and instability, we are aware that there is controversy in qualifying the stability of lumbosacral segments in the setting of degenerative disease. That discrepancy in definitions may be present in the criteria used by the investigators in the indexed studies, thus leading to heterogeneity in the results.
One study 31 excluded patients with neurological deficit from the ID but not from the DD cohort, and another 30 excluded participants who required reoperation due to persistent compressive symptoms. Although this could support the argument that, at least in the mentioned articles, the comparison encompassed milder cases in the ID group, the fact that pain and disability scores were homogeneous between groups in the pre-intervention setting suggests that the participants were similar at baseline. Ultimately, the decision-making process to allocate participants was consistently under-reported in the selected articles, denoting a considerable source of bias.
The diversity of procedures included in our study may represent another significant limitation. Indeed, the ID group encompassed surgical techniques with different positioning and workflow (e.g., single and flipped position), approach to the intervertebral disc (e.g., oblique, lateral), posterior hardware (e.g., standard pedicle, cortical bone trajectory screw), assistive technology (e.g., navigation, fluoroscopy). Comparing so many different techniques may introduce heterogeneity that could alter the interpretation of the pooled data. However, as far as we know, this is the first systematic review that aims to compare the outcomes under conditions reflecting the real-life use of indirect and direct decompression techniques.
Finally, bias in the review process could have been introduced in several steps, including the search strategy, the inclusion and exclusion of articles, data extraction, and statistical analysis. We used several quality assessments tools and followed guidelines to reduce this occurrence.
Conclusions
The current meta-analysis shows that indirect and direct decompression and fusion techniques are similarly effective in reducing pain and disability in patients with lumbar spinal stenosis and instability. The ID group had significantly lower intraoperative blood loss and surgical time values.
Additional prospective, randomized investigations would be required to corroborate our results.
Supplemental Material
Supplemental material - Is Indirect Decompression and Fusion More Effective than Direct Decompression and Fusion for Treating Degenerative Lumbar Spinal Stenosis With Instability? A Systematic Review and meta-Analysis
Supplemental material for Is Indirect Decompression and Fusion More Effective than Direct Decompression and Fusion for Treating Degenerative Lumbar Spinal Stenosis With Instability? A Systematic Review and meta-Analysis by Martin J. Gagliardi, Alfredo J. Guiroy, Gaston Camino-Willhuber, Andrei F. Joaquim, Charles A. Carazzo, Ezequiel Yasuda, Juan P. Cabrera, and Alejandro R. Morales Ciancio in Global Spine Journal
Footnotes
Acknowledgments
This study was organized by members of the AO Spine Latin America Study Group MISS. AO Spine is a clinical division of the AO Foundation, which is an independent medically guided not-for-profit organization. Non-financial support was provided directly through AO Spine Latin America regarding article review.
Declaration of Conflicting Interests
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.