
Abstract
Study Design:
Retrospective cohort.
Objective:
Provide a comparison of surgical approach in the treatment of degenerative cervical myelopathy in patients with OPLL.
Methods:
A national database was queried to identify adult (≥18 years) patients with OPLL, who underwent at least a 2-level cervical decompression and fusion for cervical myelopathy from 2012-2014. A propensity-score-matching algorithm was employed to compare outcomes by surgical approach.
Results:
After propensity-score matching, 627 patients remained. An anterior approach was found to be an independent predictor for higher inpatient surgical complications(OR 5.9), which included dysphagia:14%[anterior]vs.1.1%[posterior] P-value < 0.001, wound hematoma:1.7%[anterior]vs.0%[posterior] P-value = 0.02, and dural tear:9.4%[anterior]vs.3.2%[posterior] P-value = 0.001. A posterior approach was an predictor for longer hospital length of stay by nearly 3 days(OR 3.4; 6.8 days[posterior]vs.4.0 days[anterior] P-value < 0.001). The reasons for readmission/reoperation did not vary by approach for 2-3-level fusions; however, for >3-level fusions, patients with an anterior approach more often had respiratory complications requiring mechanical ventilation(P-value = 0.038) and required revision fusion surgery(P-value = 0.015).
Conclusions:
The national estimates for inpatient complications(25%), readmissions(9.9%), and reoperations(3.5%) are substantial after the surgical treatment of multi-level OPLL. An anterior approach resulted in significantly higher inpatient surgical complications, but this did not result in a longer hospital length of stay and the overall 90-day complication rates requiring readmission or reoperation was similar to those seen after a posterior approach. For patients requiring >3-level fusion, an anterior approach is associated with significantly higher risk for respiratory complications requiring mechanical ventilation and revision fusion surgery. Precise neurological complications and functional outcomes were not included in this database, and should be further assessed in future studies.
Keywords
Introduction
The ossification of the posterior longitudinal ligament (OPLL) of the cervical spine is an inflammatory process that results in the replacement of the PLL with lamellar bone. This can lead to a significant reduction in the cross-sectional area of the spinal canal and compression of the spinal cord, which can contribute to degenerative cervical myelopathy. 1 The prevalence of OPLL is reported to be as high as 3.0% in Asians, and range from 0.1% to 1.7% in North Americans and Europeans.2,3 In patients who require surgical treatment for degenerative cervical myelopathy, the presence of OPLL can present a significant surgical challenge with complication rates ranging from 5.2% to 57.6%.4-6 Surgical complications can include dural tear, C5 palsy, dysphagia, dysphonia, hematoma, axial pain, and other neurological complications.5,7-12 Furthermore, a prospective, multi-center study found that OPLL was an independent risk factor (odds ratio 1.8, P = 0.040) for perioperative complications in patients surgically treated for cervical spondylotic myelopathy. 13 The relatively high morbidity rate in this population has spurred numerous studies to focus on potentially modifiable risk factors.
Prior studies have compared the perioperative complications by surgical approach (anterior vs. posterior). A recent systematic review reported that the anterior approach achieved superior patient-reported outcomes and functional recovery rates, but was associated with a higher risk for complications and reoperations. The major limitations of this review, however, were the potential regional bias, as all studies were performed in Asian populations and the relatively small sample size, since the largest study included in the review only had 135 patients. 3 Other existing literature on the optimal surgical approach remains limited by single-institution analyses, complications limited to an inpatient setting, regional bias, and inadequate control of other potential confounding variables (e.g. number of levels fused, corpectomy).2,14-18
This study addresses these limitations by utilizing a nationwide, multi-center database and employing a propensity-score matching algorithm on a comprehensive set of perioperative factors. The purpose of this study is to provide a comparative analysis of surgical approach in the treatment of cervical myelopathy in patients with OPLL. This is one of the largest studies to provide national estimates on the inpatient complications and post-discharge 90-day outcomes in this patient population.
Materials and Methods
Data Source
The Nationwide Readmission Database is one of the many databases developed for the Health Cost and Utilization Project (HCUP). 11 The Nationwide Readmission Database includes a large sample size from 28 geographically dispersed States, accounting for 60% of the total U.S. resident population. This database is structured to allow for tracking of an individual’s hospital admissions across different institutions and state lines within a given year. Several perioperative factors such as patient demographics, comorbidities, insurance, and hospital level factors are collected. Since each patient encounter is associated with up to 30 ICD-9 diagnosis codes and 15 ICD-9 procedural codes, several perioperative factors which were not pre-defined in this database were included using these codes as listed in the Supplemental Appendix Table. In contrast to other data registries, the Nationwide Readmission Database includes “discharge weights,” which allow for the calculation of national estimates such as complication and readmission rates. Since this is a publicly available database that contains de-identified patient information, this study was deemed exempt by the Institutional Review Board.
Defining the Patient Population
The 2012 to 2014 Nationwide Readmission Databases were queried for all adult (≥18 years old) patients diagnosed with both OPLL (ICD-9: 723.7) and cervical myelopathy (ICD-9: 721.1, 722.71), who underwent elective cervical decompression and fusion (ICD-9: 81.02[anterior], 81.03[posterior], 3.09). These definitions are consistent with prior literature.16,19 Exclusion criteria included adult spinal deformity, metastatic cancer, trauma, infection, ≥9 level fusion, atlantoaxial fusion, non-cervical fusion, revision fusion, disc arthroplasty, and non-elective patients. The ICD-9 codes used to define many of these variables, which were not pre-defined in the database, can be found in the Supplemental Appendix Table. Those with missing data were excluded from this study. Since the Nationwide Readmission Database cannot track admission visits across database years, patients who were discharged in the last quarter of each year were excluded to account for possible readmissions and reoperations within 90 days after the index admission discharge date. The selection of this study’s population is illustrated in Figure 1.
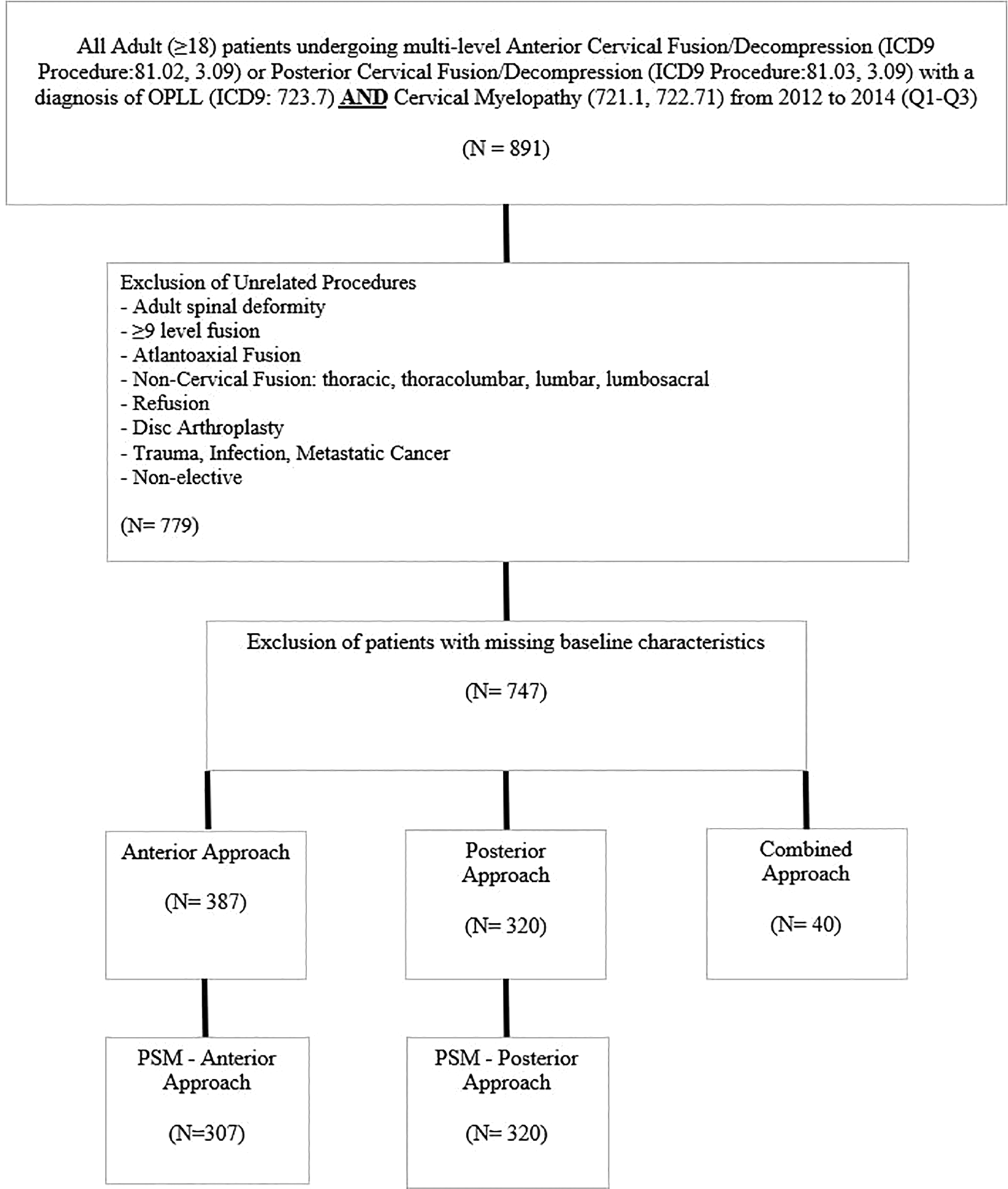
Selection criteria of the study’s patient population.
Perioperative Factors
Patient data included age, gender, income quartile and insurance type. The comorbidity profile was examined with the Charlson Comorbidity Index (CCI). Other comorbidities included alcohol abuse, current/prior smoker, depression, hypothyroidism, obesity, osteoporosis, chronic steroid use, and chronic anticoagulation. Surgical factors included fusion level, corpectomy, and bone morphogenetic protein use. Hospital factors included hospital ownership (private non-profit, private for-profit, government), and hospital teaching status (metropolitan non-teaching, metropolitan teaching, and non-metropolitan).
Outcomes of Interest
The primary outcome variables in this study were index inpatient complications and post-discharge 90-day complications requiring readmission and/or reoperation. A 90-day readmission was defined as any admission within 90 days after the discharge date of the index hospital stay. Other outcomes included length of hospital stay and discharge disposition (home, subacute rehab, and death). Inpatient complications and reasons for readmission were categorized as either medical or surgical. These complications were defined using ICD-9 codes (see Supplemental Appendix Table).
Propensity Score Matching Analysis
First, patients were categorized into those with either an anterior or posterior surgical approach. Then, a propensity score matching algorithm was employed to account for the potential selection bias inherent in surgical approach (anterior vs. posterior). Various patient, surgical, and hospital factors were included in this algorithm. For descriptive and comparative purposes, bivariate analyses were performed for both with and without propensity score matching. Chi-square or Fisher’s exact test (where appropriate) and t-tests/ANOVA were used for categorical and continuous variables, respectively. Statistical significance was defined as a P-value < 0.05. SAS software (Version 9.3; SAS Institute Inc, Cary, NC) was used for statistical analyses. Propensity score matching was performed in R version 3.0.2 (Vienna, Austria, http://www.R-project.org/) using the Matchlt (Ho, Imai, King, & Stuart, 2011) package. We used “nearest” matching method and discarded “treated” units outside the support of the distance measure of the control units.
Other Statistical Analysis
The outcomes and complications, which were significantly associated with surgical approach in the bivariate analyses, were further studied in the multivariate analyses, which involved step-wise multivariate logistic regressions. Since the number of fusion levels were not able to be fully controlled for in the propensity score matching algorithm, the multivariate models included the number of fusion levels as a variable in the regressions. Furthermore, when comparing the reasons for readmission by surgical approach, this was subcategorized by the number of fusion levels as well.
Results
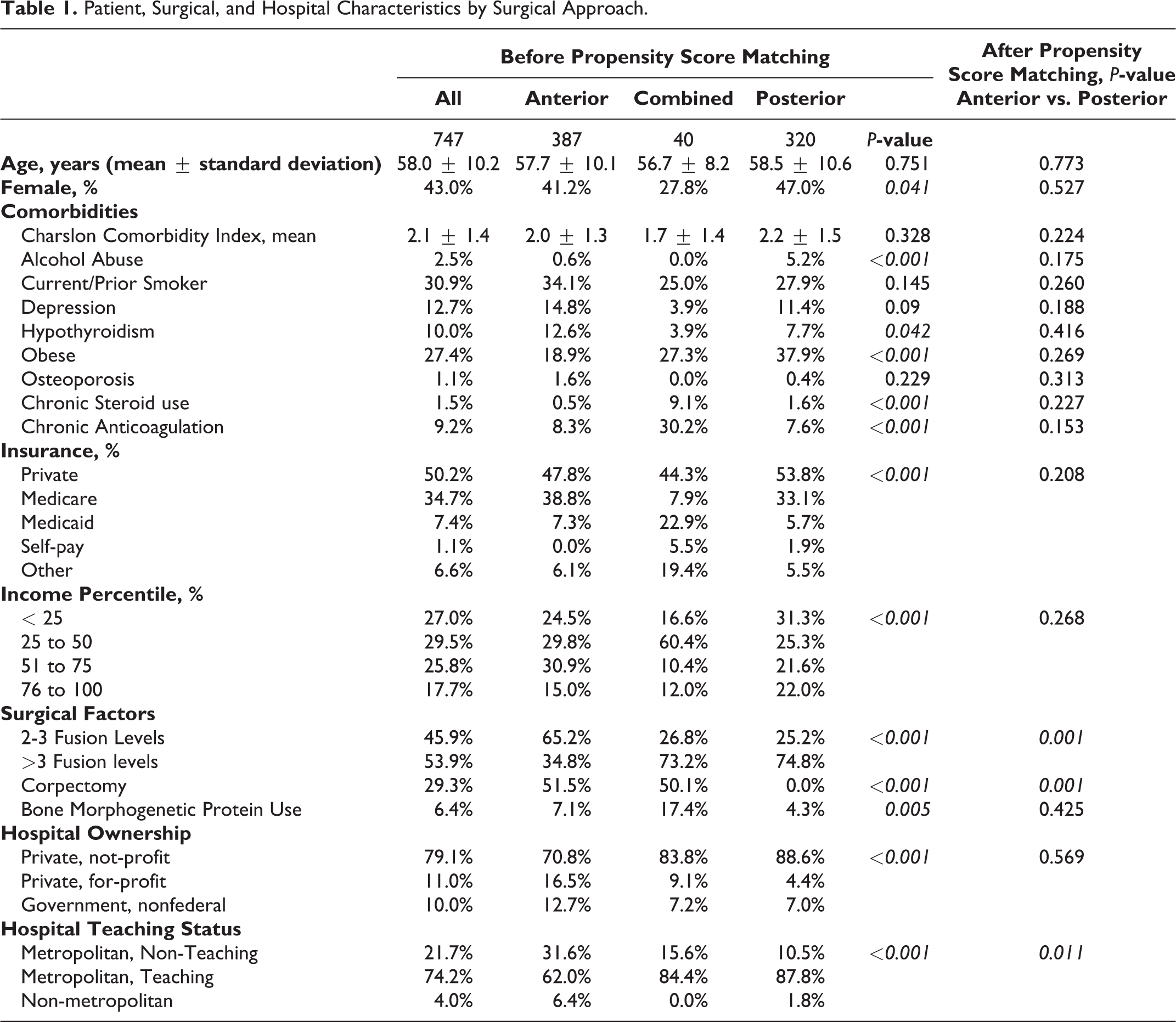
After inclusion and exclusion criteria, there were a total of 747 patients with OPLL who underwent an elective cervical decompression and fusion (anterior = 387, posterior = 320, combined = 40) for cervical myelopathy from 2012 to 2014 (Figure 1). The mean age (±standard deviation) was 58 ± 10 years old, and 43% of patients were female. Prior to propensity score matching, patient (insurance type: P < 0.001, income percentile: P < 0.001), surgical (number of fusion levels: P < 0.001, bone morphogenetic protein use: P = 0.005), and hospital factors (hospital ownership: P < 0.001, hospital teaching status: P < 0.001) varied significantly by surgical approach. A number of comorbidities varied significantly by surgical approach as well. These included alcohol abuse (anterior = 0.6%, combined = 0%, posterior = 5.2%, P < 0.001), hypothyroidism (anterior = 12.6%, combined = 3.9%, posterior = 7.7%, P = 0.042), obesity (anterior = 18.9%, combined = 27.3%, posterior = 7.7%, P < 0.001), chronic steroid use (anterior = 0.5%, combined = 9.1%, posterior = 1.6%, P < 0.001), and chronic anticoagulation (anterior = 8.3%, combined = 30.2%, posterior = 7.6%, P < 0.001) (Table 1).
Patient, Surgical, and Hospital Characteristics by Surgical Approach.
After propensity score matching, there were 627 patients (anterior = 307, posterior = 320). All perioperative factors were statistically similar between anterior and posterior surgical approaches with the exception to the number of fusion levels (>3 fusion levels: anterior = 43%, posterior = 74%, P = 0.001) and hospital teaching status (metropolitan teaching: anterior = 75%, posterior = 87%, P = 0.011). Since these factors were not fully controlled for in the propensity score matching algorithm, these variables were included in subsequent multivariate analyses.
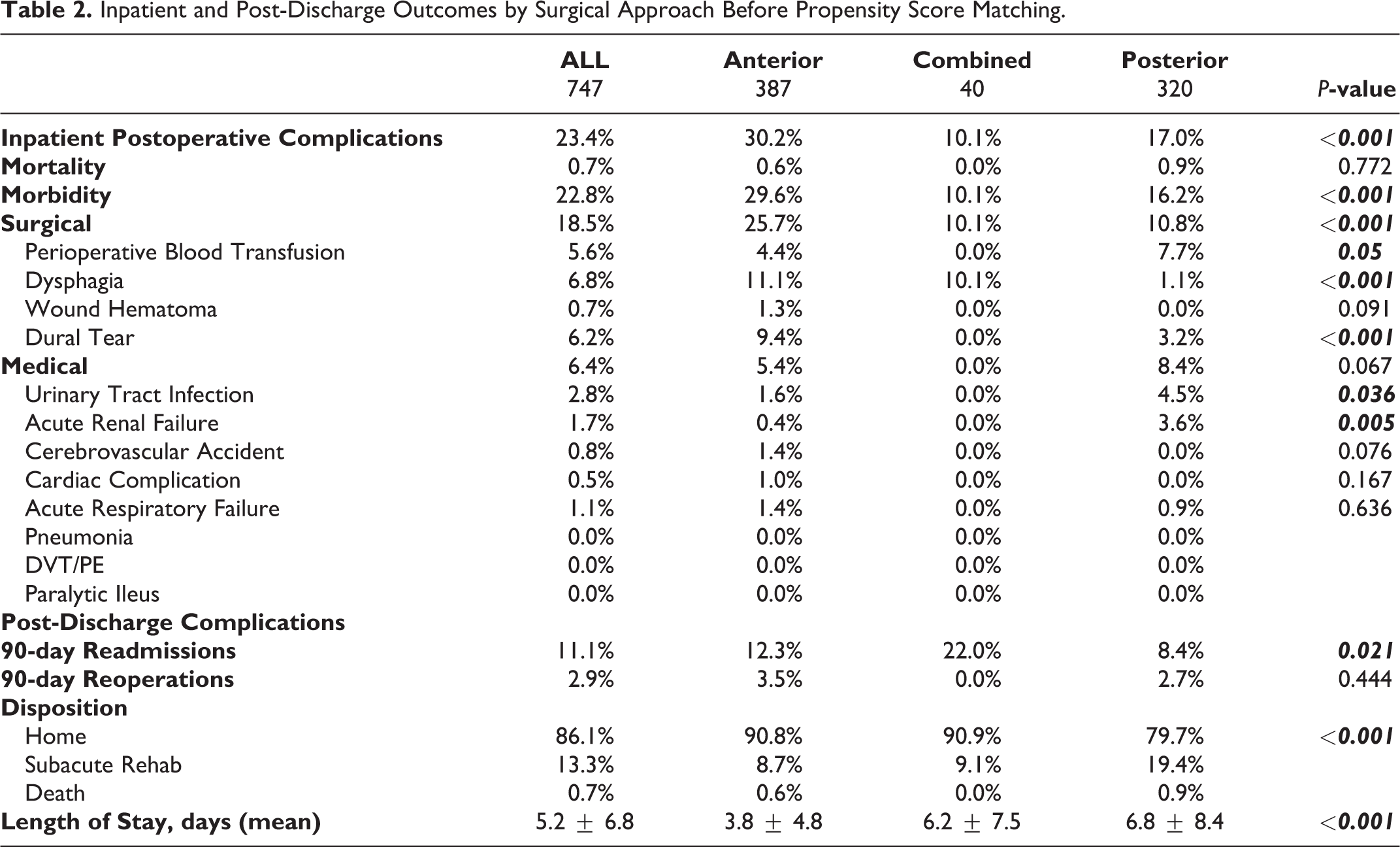
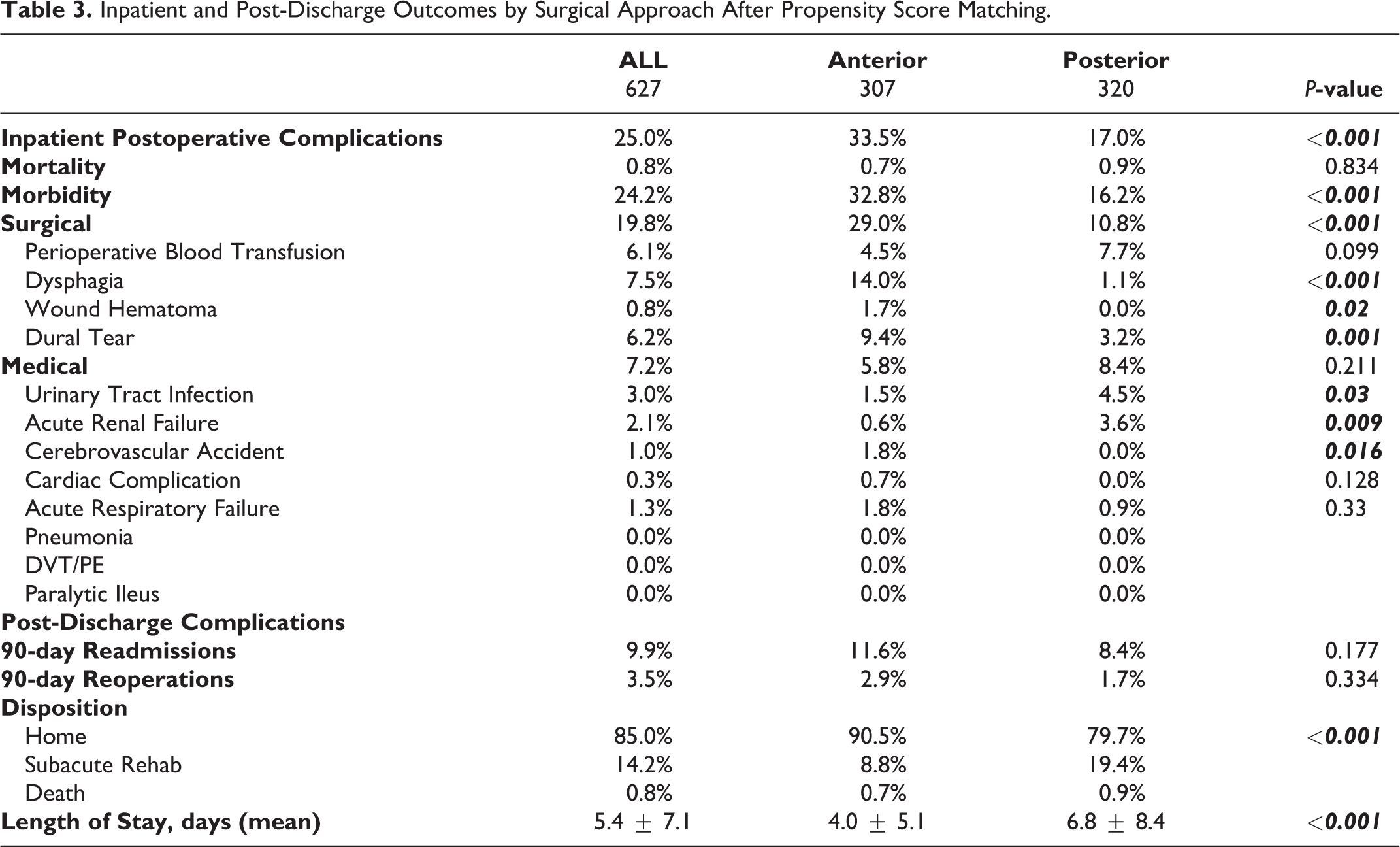
The overall inpatient morbidity rate was 24.2% (anterior = 32.8% vs. posterior = 16.2%, P < 0.001) and the mortality rate was 0.8% (anterior = 0.7% vs. posterior = 0.9%, P = 0.834). In the bivariate analyses of postoperative outcomes, the surgical complications were more common in the anterior approach (anterior = 29% vs. posterior = 10.8%, P < 0.001). Specific surgery-related inpatient complications included dysphagia (anterior = 14% vs. posterior = 1.1%, P < 0.001), wound hematoma (anterior = 1.7% vs. posterior = 0%, P = 0.020), and dural tear (anterior = 9.4% vs. posterior = 3.2%, P = 0.001). Medical-related inpatient complications appeared to be more common in posterior approach patients. These included urinary tract infections (anterior = 1.5% vs. posterior = 4.5%, P = 0.030) and acute renal failure (anterior = 0.6% vs. posterior = 3.6%, P = 0.009). Although 90-day readmission rates were significantly higher in the anterior approach group prior to propensity score matching (anterior = 12.3% vs. posterior = 8.4%, P = 0.021), neither the 90-day readmission rates nor the 90-day reoperation rates were significantly different by surgical approach after propensity score matching (Table 2). Posterior approach patients were more often discharged to a subacute rehab center (anterior = 14.2% vs. posterior = 19.4%, P < 0.001). The mean length of hospital stay was significantly longer for posterior approach patients (6.8 ± 8.4 days) than anterior approach patients (4.0 ± 5.1, P < 0.001) (Table 3).
Inpatient and Post-Discharge Outcomes by Surgical Approach Before Propensity Score Matching.
Inpatient and Post-Discharge Outcomes by Surgical Approach After Propensity Score Matching.
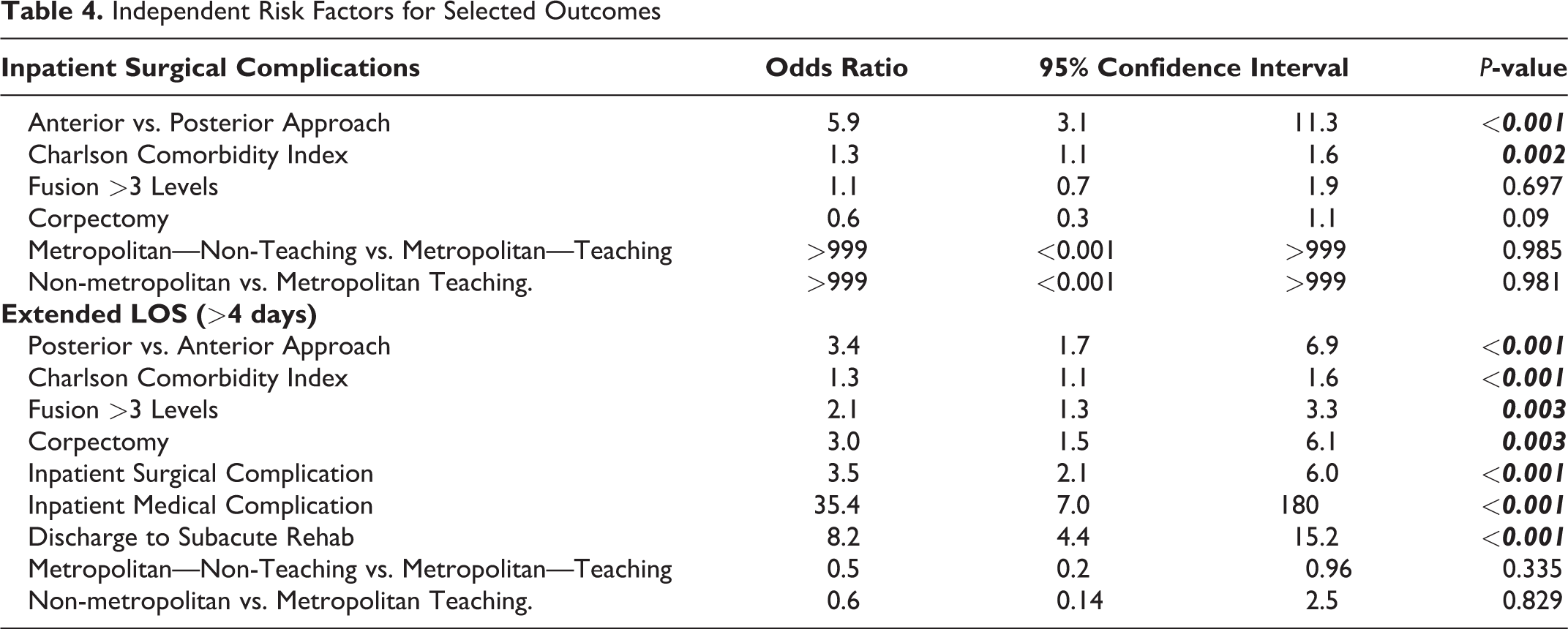
In the multivariate analyses, the anterior approach was an independent predictor for inpatient surgical complications (odds ratio 5.9). In contrast, the number of fusion levels, corpectomy, and hospital factors (ownership, teaching status) were not statistically significant factors. The posterior approach was an independent risk factor for extended length of hospital stay, >4 days (odds ratio 3.4). Other independent risk factors for LOS >4 days included CCI (odds ratio 2.1), fusion levels >3 (odds ratio 2.1), corpectomy (odds ratio 3.0), inpatient surgical complications (odds ratio 3.5), inpatient medical complications (odds ratio 35.4), and discharge to subacute rehab (odds ratio 8.4) (Table 4).
Independent Risk Factors for Selected Outcomes
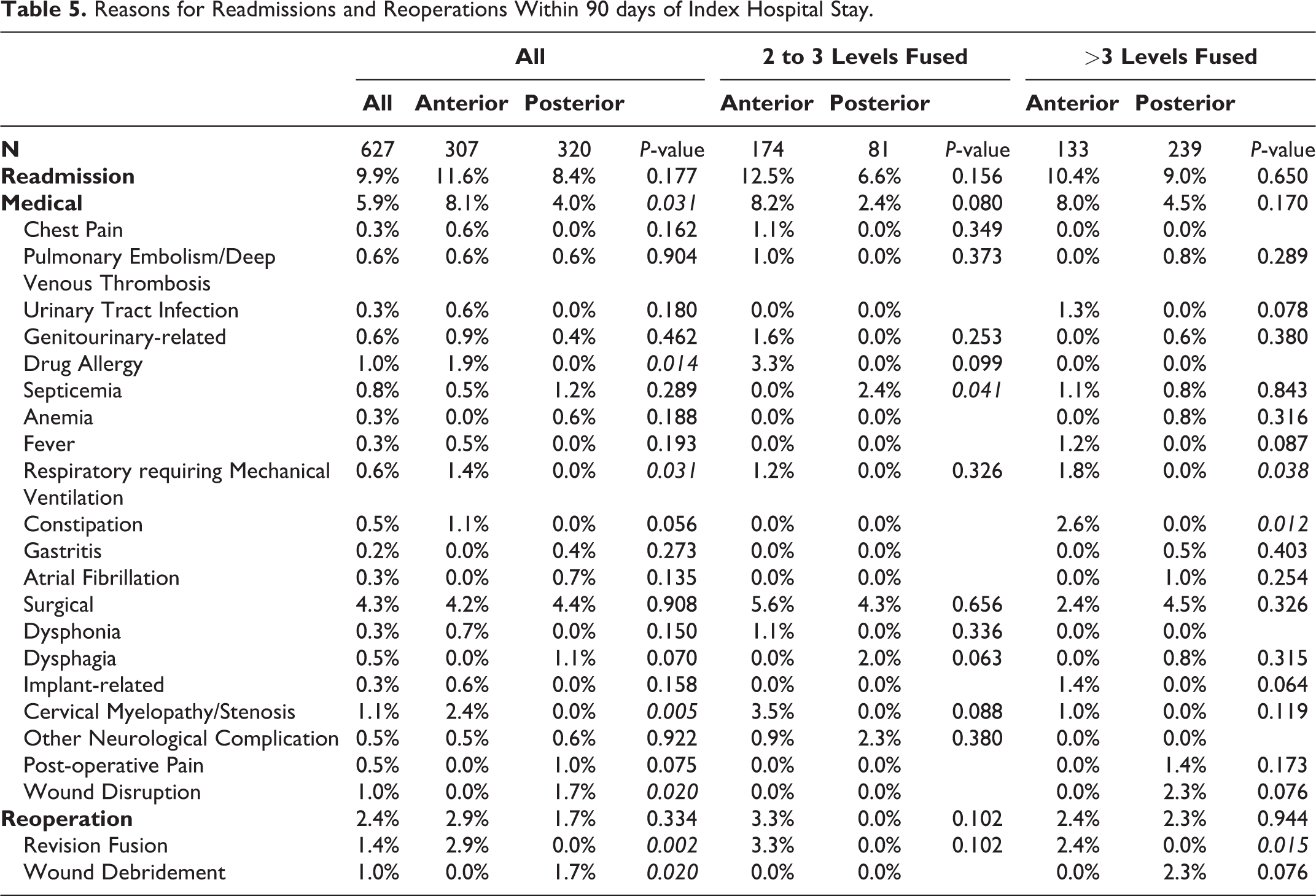
The reasons for 90-day readmission and reoperation were evaluated by surgical approach for those with 2- to 3-level fusions and those with >3-level fusions (Table 5). The rates for readmission and reoperation did not significantly vary by surgical approach for either fusion level cohort; however, patients with a posterior approach for 2- to 3-level fusions were more often readmitted for sepsis (anterior = 0% vs. posterior = 2.4%, P = 0.041) and patients with an anterior approach for >3-level fusions were more often readmitted for respiratory complications requiring mechanical ventilation (anterior = 1.8% vs. posterior = 0%, P = 0.038), constipation (anterior = 2.6% vs. posterior = 0%, P = 0.012) and revision fusion (anterior = 2.4% vs. posterior = 0%, P = 0.015).
Reasons for Readmissions and Reoperations Within 90 days of Index Hospital Stay.
Discussion
The purpose of any surgical intervention for DCM is to adequately decompress the neural elements and maintain mechanical stability. Given the diverse pathophysiology of DCM, several considerations exist when deciding the optimal surgical approach, such as the number of levels requiring decompression, approach-related complications, body habitus, short neck, surgeon preference, as well as the presence of OPLL. In situations where there is true equipoise between both approaches, prior literature suggests that equivalent outcomes and complication rates up to 2 years after surgery can be achieved.1,20,21 However, the optimal surgical approach for the treatment of degenerative cervical myelopathy in patients with OPLL remains somewhat controversial as it depends on a multitude of factors such as surgical technique, surgeon-comfort level, disease severity, the level of OPLL, cervical alignment, and potential approach-related complications. An anterior approach typically involves anterior discectomy and/or corpectomy with fusion. The main advantage of this approach is that it allows for direct decompression; however, this approach can be technically demanding especially when the ossified ligament is densely adherent to the ventral dura and manipulation can result in dural tears. A posterior approach can involve laminoplasty or laminectomy with or without fusion. This allows for indirect decompression of the entire cervical spine, in comparison to an anterior approach which is typically limited cranially to C2. However, in patients who have poor cervical kyphotic alignment, an occupying ratio ≥60%, or a negative k-line, a posterior only approach without appropriate realignment has been shown to lead to inadequate decompression and significantly poorer neurological outcomes.2,3,22,23 Despite these findings, an in-depth analysis directly comparing approach-related complications is lacking, especially for non-Asian patient populations.
Two systematic reviews have recently been published to compare the risks associated between anterior and posterior surgical approaches. Zhang et al included 11 studies in their meta-analysis, totaling 800 patients. 3 These authors reported that the anterior approach had a higher risk for postoperative complications (odds ratio 2.6) and reoperations (odds ratio 5.9). Those who underwent an anterior approach were more likely to have a dural tear, whereas those who underwent a posterior approach were more likely to have postoperative axial neck pain. However, the anterior approach achieved significantly higher postoperative Japanese Orthopedic Association (JOA) scores (odds ratio 2.4) and higher postoperative functional recovery rates (weighted mean difference = 16.4). Interestingly, for patients with an occupying ratio <60%, the postoperative recovery rates were similar between both approaches. No significant differences were observed in the postoperative cervical alignment. Given these findings, these authors recommended an anterior approach for the treatment of OPLL, especially for patients with an occupying ratio ≥60%.
In the other systematic review, Kim et al included 21 studies in their analysis, totaling 3,872 patients with cervical myelopathy and OPLL. In this study, no significant differences in the mean occupying ratios were observed between groups; however, the number of levels fused was significantly higher in the posterior group (anterior = 2.7, posterior = 4.1, P < 0.01). In contrast to other reviews, this study analyzed major neurological complications including paraplegia and quadriplegia, and found that an anterior approach was significantly associated with neurological deficits (odds ratio 2.2). The JOA improved in both groups significantly compared to baseline values, but the difference in JOA improvement between approaches was not clinically significant (1.3 points). Similar to other reviews, this study found that the complication rates were significantly higher in the anterior group. These authors concluded that a posterior approach would be superior especially for multi-level cervical myelopathy with OPLL; however, a comparative analysis of surgical approach by the number of levels fused was not included in this review. Furthermore, both systematic reviews were limited to small retrospective studies on Asian-only populations and revealed the need for a large, multi-center study on non-Asian populations.
Bernstein et al used a large national data registry to examine the trends and complications in the surgical management of OPLL. 16 In their study, these authors reported that the number of surgical cases of OPLL has significantly increased over the last decade and provided national estimates for inpatient postoperative complications, which were substantial (21%). A direct comparison of outcomes between an anterior and a posterior approach was not performed; however, complication rates appeared similar between the anterior (21%) and posterior (20%) surgical approaches. This is in contrast to our study where an anterior approach (33.5%) yielded nearly double the inpatient postoperative complications than a posterior approach (17%). This is most likely because of differences in what was defined and included as a complication between our studies. For instance, it is not clear what complications were included as “neurological,” “cervical-spine related,” “pulmonary,” “cardiac,” and “renal.” We included perioperative blood transfusion and wound hematoma, which does not appear to be captured in their study. Furthermore, their study uses a database which does not allow for the assessment of post-discharge outcomes and complications. Nevertheless, their study provided significant insight on the national-level complication rates in a non-Asian patient population with surgically treated OPLL. Specifically, the percentage of Asians or Pacific Islanders with OPLL who received surgical management, was 7.5%. This is higher than the prevalence in the United States (4.9%), which suggests a potential genetic association with OPLL. 24 The likely increased occurrence of OPLL in the Asian demographic may explain the paucity of research of OPLL surgical management in the United States; nevertheless, geographic variations to the presentation and management of these patients may exist and necessitates future national database studies in non-Asian populations to compare perioperative outcomes.
To our knowledge, our study is one of the largest ones to provide a direct comparative analysis of surgical approach in the treatment of degenerative cervical myelopathy in non-Asian patients who have OPLL. Consistent with prior literature, an anterior approach had significantly higher inpatient complications than a posterior approach. This difference was largely due to surgical complications (dysphagia: 14%[anterior] vs. 1.1%[posterior] P-value < 0.001, wound hematoma: 1.7%[anterior] vs. 0%[posterior] P-value = 0.02, and dural tear: 9.4%[anterior] vs. 3.2%[posterior] P-value = 0.001) associated with the anterior approach. Therefore, it is possible that with improved surgical technique and proficiency, complications may be reduced. Despite higher inpatient complications, the anterior approach did not result in a longer hospital stay and the 90-day readmission and reoperation rates were similar between both surgical approaches (Readmission: 11.7% [anterior] vs.8.4% [posterior] P-value = 0.177, Reoperation: 4.2% [anterior] vs. 2.8% [posterior] P-value = 0.261). Furthermore, a posterior approach more often required at least a 4-level fusion in comparison to an anterior approach; however, after controlling for the number of levels fused in the multivariate analysis, the anterior approach remained as an independent risk factor for higher inpatient surgical complications (odds ratio 5.9), and the posterior approach was an independent predictor for longer hospital length of stay by nearly 3 days (odds ratio 3.4; 6.8 days[posterior] vs. 4.0 days[anterior] P-value < 0.001). The extended hospital length of stay observed in the posterior group may be related to the higher rate of post-operative medical complications and the subsequent need for sub-acute rehab, which may delay hospital discharge. As demonstrated in prior literature, post-operative neck pain is more common with the posterior approach, which may contribute to a longer hospital stay.9,25 The reasons for readmission and reoperation did not vary by surgical approach for 2- to 3-level fusions; however, for >3-level fusions, patients with an anterior approach more often had a respiratory complication requiring mechanical ventilation (P-value = 0.038) and revision fusion surgery (P-value = 0.015).
A number of limitations should be acknowledged in this study. First, this study does not include other posterior-based procedures such as decompression-alone or laminoplasty. Only patients who required both a cervical decompression and fusion were examined in this study to minimize potential surgical-related confounding factors. It is possible that non-fusion procedures such as laminoplasty may highlight the safety for posterior approaches for multi-level disease and can be assessed in future national databases. Furthermore, differences in surgeon-technique, which was not possible to control for in this study, will likely influence intraoperative and postoperative outcomes. For instance, some authors have described an “anterior floating method,” which is a subtotal vertebral body resection and thinning, but not a complete removal of the OPLL. This allows the OPLL to float anteriorly and away from the spinal canal.26,27 In addition, Lee et al recently described the “Vertebral Body Sliding Osteotomy” (VBSO), which is a novel anterior technique that allows for direct decompression, but avoids direct manipulation of the OPLL. 28 Therefore, complications arising from attempts to excise the OPLL are effectively avoided. Due to the inherent limitations of the Nationwide Readmission Database, this study lacks the ability to monitor neurological complications in detail. A major consideration in choosing the approach is the surgeon’s perception of which approach will cause more improvement in neurologic function. The lack of precise neurological and functional outcomes, which are not included in this national database and would influence surgical decision making, is a major limitation of this study. The absence of radiographic data precludes our ability to determine the extent of OPLL or measure the K-line, since many surgeons use these factors to guide their decision in choosing a surgical approach. By using national-level data and employing both propensity-score matching and multivariate analyses, we aimed to minimize potential selection bias as much as possible. It is important to note that we used a sophisticated matching algorithm to control for an extensive list of perioperative factors; however, we were not able to perfectly match fusion levels. To adequately control for this potentially confounding factor, we included fusion levels in multivariate analyses to further delineate outcome differences by approach and fusion levels. The minimum follow-up of this study was 90 days after the index discharge date. Although this is the first nationally-based study on 90-day outcomes for this patient population, future studies should include a longer follow-up period to capture the true extent and progression of complications. Finally, no large database will ever yield as much information as a well-executed prospective or even a large retrospective study. All database studies are limited by the information that was collected. However, our study with a large cohort of subjects closely agrees with the findings of most retrospective studies that have been published on this topic. As such, it lends credence to the conclusions that have been drawn from those studies, which too are flawed by factors such as small numbers, single surgeon collections and limited follow-up. While each type of study has its own set of inherent flaws, taken together, with flaws that do not necessarily overlap, the evidence is compelling that our conclusions are likely to be true findings.
Conclusion
The national estimates for inpatient complications (25%), readmissions (9.9%), and reoperations (3.5%) are substantial after the surgical treatment of multi-level cervical myelopathy in patients with OPLL. An anterior approach resulted in significantly higher inpatient surgical complications, but this did not result in a longer hospital length of stay and the overall 90-day post-discharge complication rates were similar between approaches. For patients requiring >3-level fusion, an anterior approach is associated with a significantly higher risk for respiratory complications requiring mechanical ventilation and revision fusion surgery. These findings will be important in the preoperative surgical decision-making process for patients and surgeons.
Supplemental Material
Supplemental Material, sj-docx-1-gsj-10.1177_2192568221994797 - What Is the Impact of Surgical Approach in the Treatment of Degenerative Cervical Myelopathy in Patients With OPLL? A Propensity-Score Matched, Multi-Center Analysis on Inpatient and Post-Discharge 90-Day Outcomes
Supplemental Material, sj-docx-1-gsj-10.1177_2192568221994797 for What Is the Impact of Surgical Approach in the Treatment of Degenerative Cervical Myelopathy in Patients With OPLL? A Propensity-Score Matched, Multi-Center Analysis on Inpatient and Post-Discharge 90-Day Outcomes by Nathan J. Lee, Venkat Boddapati, Justin Mathew, Michael Fields, Meghana Vulapalli, Jun S. Kim, Joseph M. Lombardi, Zeeshan M. Sardar, Ronald A. Lehman and K. Daniel Riew in Global Spine Journal
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.