
Abstract
Study Design
Retrospective cohort study
Objectives
The goal of this study was to determine the clinical characteristics of patients with primary spinal osteosarcoma and to construct a practical clinical prediction model for patients to achieve an accurate prediction of overall survival.
Methods
This study included 230 patients diagnosed between 2004-2015 from the Surveillance, Epidemiology, and End Results database. Independent risk factors were screened in the training set using Cox regression algorithms, and a prognostic model was developed. Internal and external validation sets were used to test the nomogram model's calibration, discrimination, and clinical utility. A risk classification system based on the nomogram was developed and validated.
Results
Four independent prognostic factors were identified, and based on this a nomogram model was developed for predicting patient prognosis. The C-index of the training set was .737, while that of the validation set was .693. The time-varying area under the curve values was greater than .720 in both cohorts. The calibration curves proved that the prediction model has high prediction accuracy. The decision curve analysis showed that the nomogram is clinically useful. A risk classification system was established, which allows all patients to be divided into two different risk groups.
Conclusions
A nomogram and risk classification system was developed for patients with primary spinal osteosarcoma to accurately predict overall patient survival and achieve risk stratification of patient mortality. These tools are expected to play an important role in clinical practice, informing clinicians in making decisions.
Introduction
Primary bone tumors of the spinal regions are uncommon, accounting for only about 5% of all primary bone tumors. 1 Among the common pathological types, chordoma, chondrosarcoma, and Ewing sarcoma have a similar prognosis, with osteosarcoma having the worst prognosis.2,3 Osteosarcoma often involves the long bones of the skeleton, and less than 5% of osteosarcomas occur in the axial bones, with a 5-year survival rate of only 38%. 4 Due to their special location, spinal tumors are not only fast-growing but also insidious, making it difficult to diagnose them at an early stage.5,6 Due to the lack of anatomical barriers to tumor spread, spinal tumors often cause compression of adjacent organs, blood vessels, and nerves at the time of diagnosis. 7
Nomogram is a visual statistical prediction tool for identifying clinically relevant prognostic factors and is now widely used in a variety of cancers. 8 In many previous reports, nomograms showed higher accuracy in predicting the prognosis of tumor patients compared to the TNM staging system. Given the special anatomical location of the spine, it is difficult for the traditional TNM staging system to accurately predict the prognosis of patients with primary spinal osteosarcoma. Tumor site, tumor size, tumor grade, age, surgery, and presence of distant metastases have been identified as risk variables for patients with osteosarcoma in the previous studies. 9 Furthermore, numerous prognostic models for patients with particular histological kinds of osteosarcoma and patients with osteosarcoma whose main tumor site is in the bones of the extremities have been created.8,10,11 However, no nomograms for predicting survival in spinal osteosarcoma patients have been reported. We used the Surveillance, Epidemiology, and End Results (SEER) cancer registry database to analyze independent risk variables in patients with primary spinal osteosarcoma and on this basis constructed nomograms to accurately predict survival outcomes in individual patients.
Methods
Database
Surveillance, Epidemiology, and End Results (SEER) is a US population-based cancer database that collects data on cancer patients from 18 registries, covering approximately 30% of the US population. SEER Stat 8.3.9.2 was used to find all patients with spinal and pelvic osteosarcoma in the SEER database from 2004 to 2015. Ethics committee permission and patient consent are not necessary because no specific personal information is publicly available in the SEER database.
Patient Selection
The following were the research's inclusion criteria: (1) Osteosarcoma with histological confirmation; (2) diagnosed between 2004 and 2015; (3) primary site in the spine; (4) complete follow-up. The excluded criteria were as follows: (1) survival months <1 month; (2) the data about patients' demographic characteristics, disease characteristics, and treatment information (surgery, radiotherapy, and chemotherapy) were unknown. Finally, 230 patients with spine and pelvis osteosarcoma compounded the criteria. They were divided into a training set and a validation set at random in a 7:3 ratio, with the training set being used to identify independent prognostic factors and establish the prognostic nomogram. The validation set is then defined as the patient population used to validate the performance and predictive accuracy of the constructed nomogram. Overall survival was the endpoint of the study and was defined as the time between the first diagnosis of primary spinal osteosarcoma and the patient's death or last follow-up visit.
Prognostic Variables Definitions
The variables extracted from the SEER database included those patients' demographic characteristics, disease characteristics, and treatment information. Age is a continuous variable, so we used the X-tile software (version 3.6.1) to find the suitable cut-off values for age. The results showed that the age cut-off values of 38 and 66 were appropriate. Sex is a binary variable divided into males and females, and the race was stratified into three groups (white, black, and others). The tumor size is into two groups (≥ 80 and <80 mm). Stages were classified as localized, regional, and distant, while the histological type was classified as osteosarcoma, chondroblastic osteosarcoma, and others. The definition of localized is a tumor that is confined to the periosteum, while the definition of regional is a tumor that extends from outside the periosteum into the surrounding tissue. Treatment information (surgery, radiotherapy, and chemotherapy) and marital status were divided into yes and no.
Statistical Analysis
The statistical analyses in this study were performed using SPSS (version 25.0) and R software, with a P-value of <.05 deemed statistically significant. First, the univariate Cox regression analysis was performed to find the correlation between each prognostic variable of overall survival. The variables with a P-value of less than .05 in the univariate Cox analysis were then chosen and included in the multivariate Cox analysis. The hypothesis of Cox regression analysis was tested using Kaplan-Meier survival curve analysis and the log-rank test. The RMS package in R software was used to create a nomogram model for predicting 1-, 3-, and 5-year overall survival of patients based on identified independent risk variables. After that, 1-, 3-, and 5-year calibration curves and decision curve analysis were established to exhibit the nomogram's correction ability and clinical benefits, respectively. Finally, for 1-, 3-, and 5-year overall survival, receiver operating characteristic (ROC) curves were produced, and the corresponding area under the curve (AUC) value was utilized to reflect the nomogram's differentiation ability. The nomogram was used to calculate the total patient score and subsequently determined the cut-off values to construct a risk classification system.
Result
Demographic Baseline Characteristics
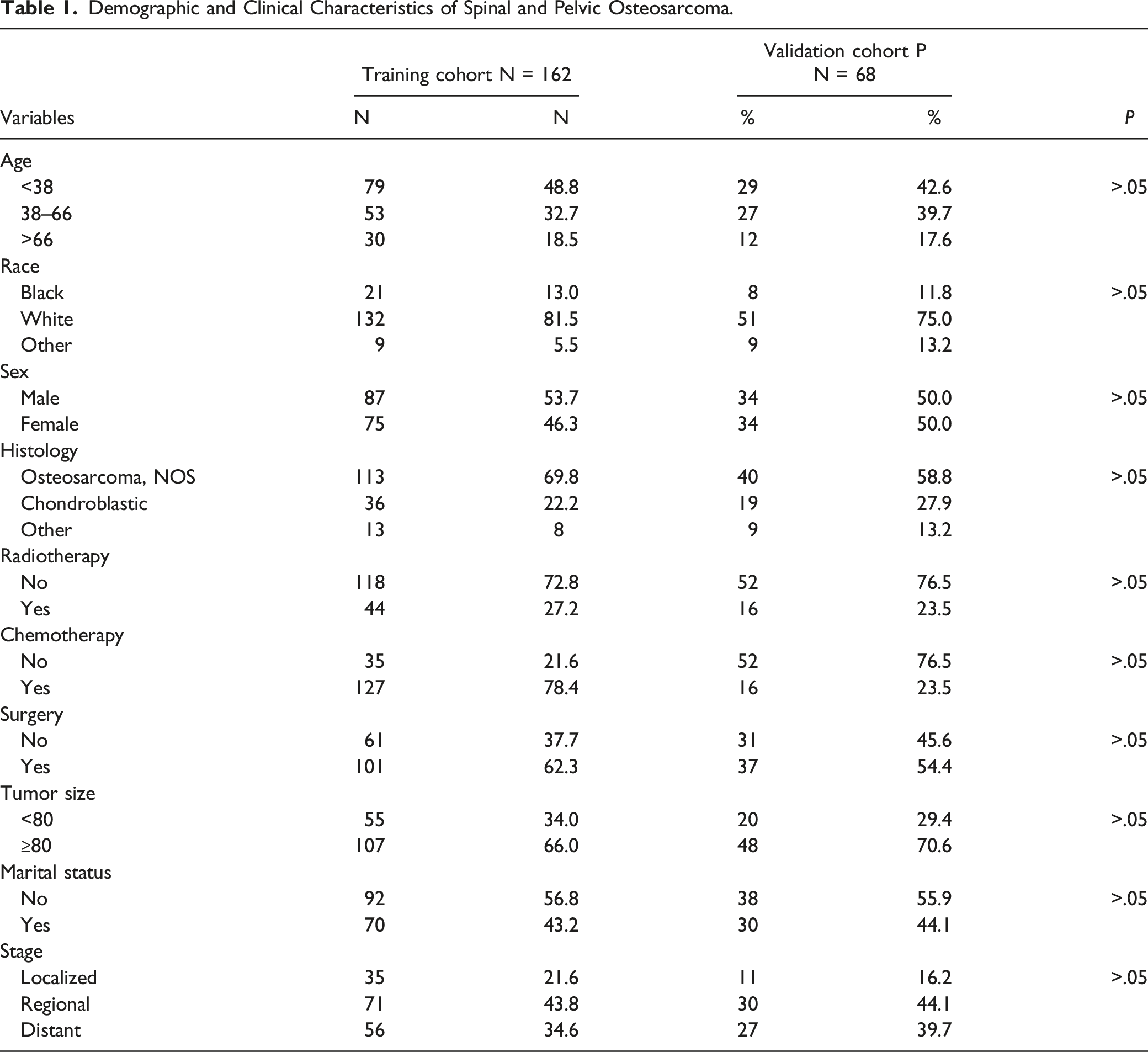
The flow of this study is shown in Figure 1. The entire set was collected from 230 patients with osteosarcoma whose tumor primary site was located in the spine from the SEER database. A training set and a validation set were randomly divided in a certain proportion. Ultimately, the training set (for the construction and internal validation of the prediction model) consisted of 162 patients and the validation set (for the external validation of the prediction model) consisted of 68 patients. Table 1 showed the specific demographic and clinicopathologic characteristics of patients with spinal osteosarcoma. As is evident from this table, patients younger than 38 years of age comprised nearly half (47.0%) of the total set. Of these, the vast majority were white (79.6%), while there was no significant difference in the proportions of males (52.6%) and females (47.4%). Patients diagnosed with spinal osteosarcoma had tumors that were usually larger than 8 cm in size and extended beyond the periosteum and were predominantly common types of osteosarcomas. Regarding treatment, the vast majority of patients received chemotherapy (78.3%) and surgery (60.0%), while those who received radiotherapy (26.1%) were in the minority. A total of 160 (69.6%) patients had died by the time of the final follow-up. The median survival of patients in the overall set was 18 months in all cases. Flow chart of this study. Demographic and Clinical Characteristics of Spinal and Pelvic Osteosarcoma.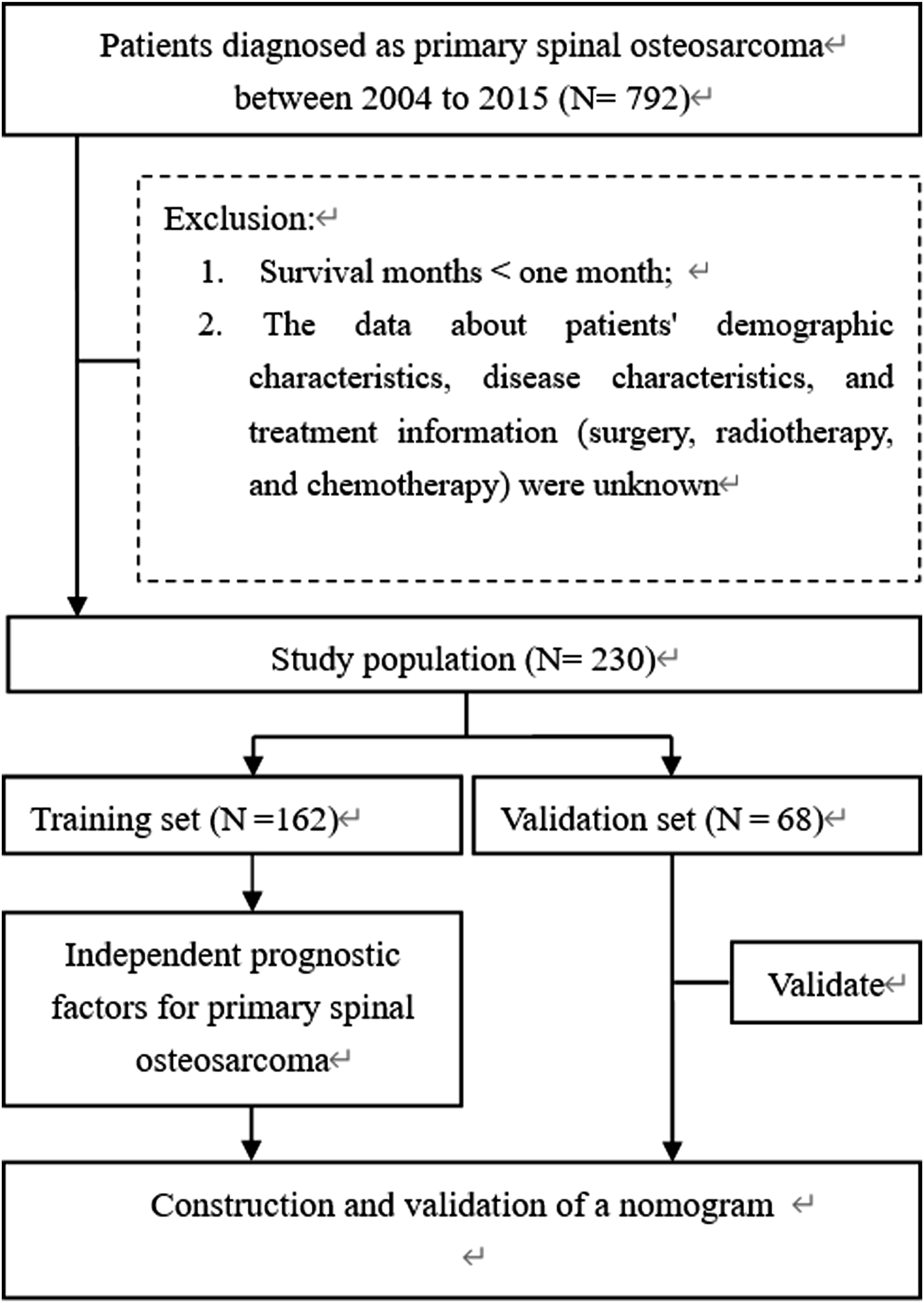
Prognostic Factors for Overall Survival
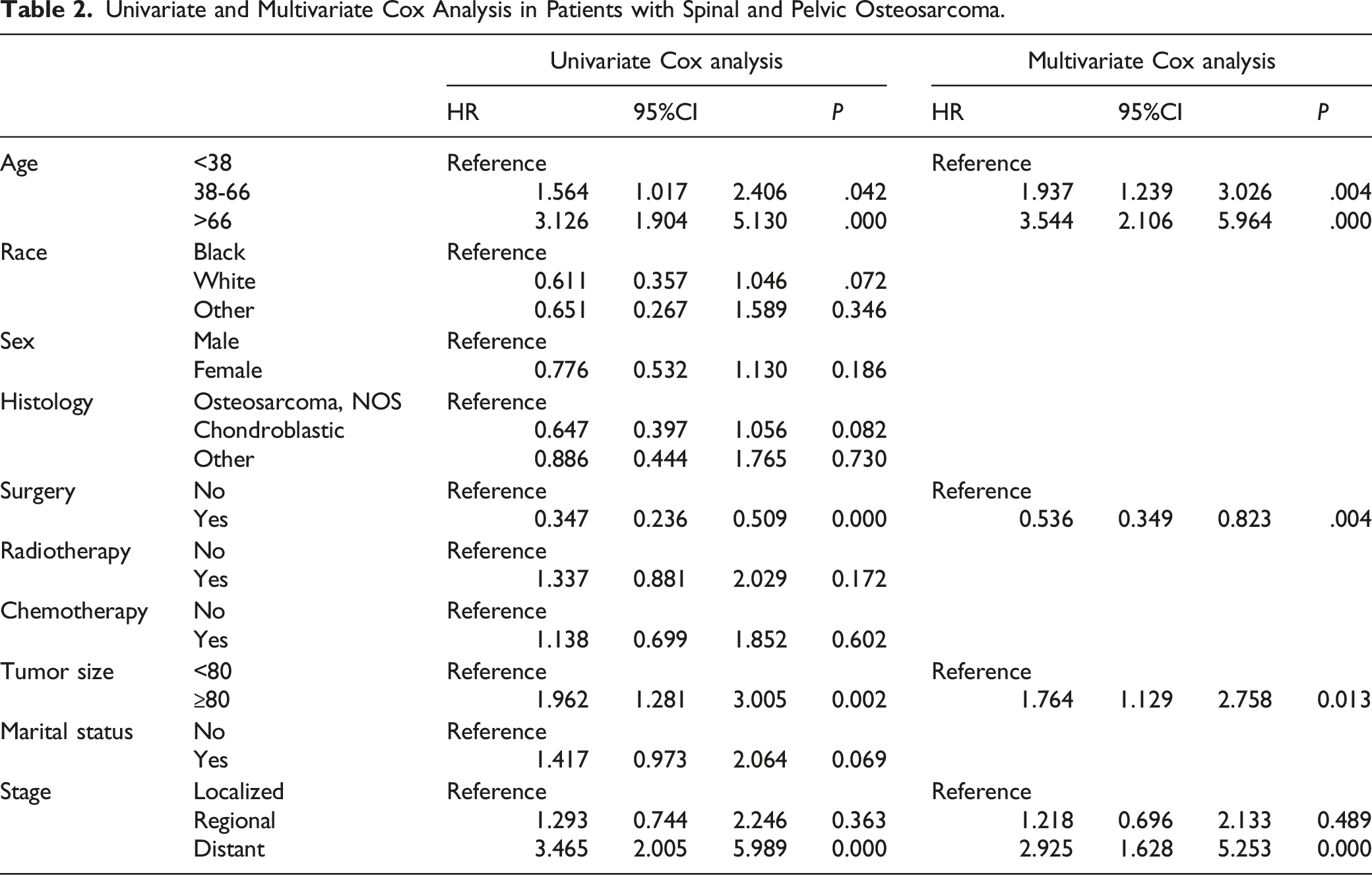
Univariate and Multivariate Cox Analysis in Patients with Spinal and Pelvic Osteosarcoma.
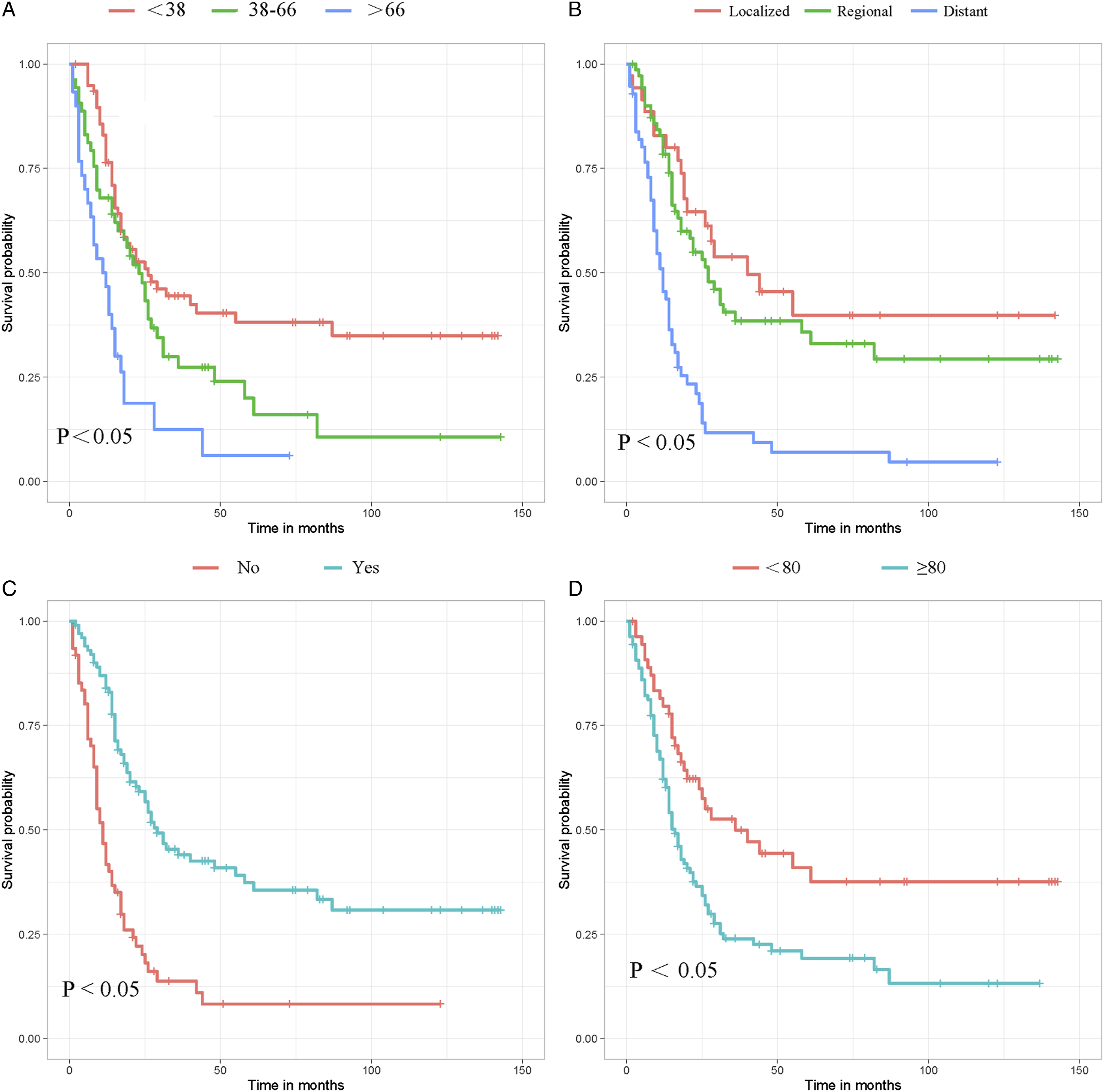
Kaplan-Meier survival curves for patient-related variables. (A) Age, (B) Stage, (C) Surgery, (D) Tumor size.
Establishment and Validation of the Nomogram
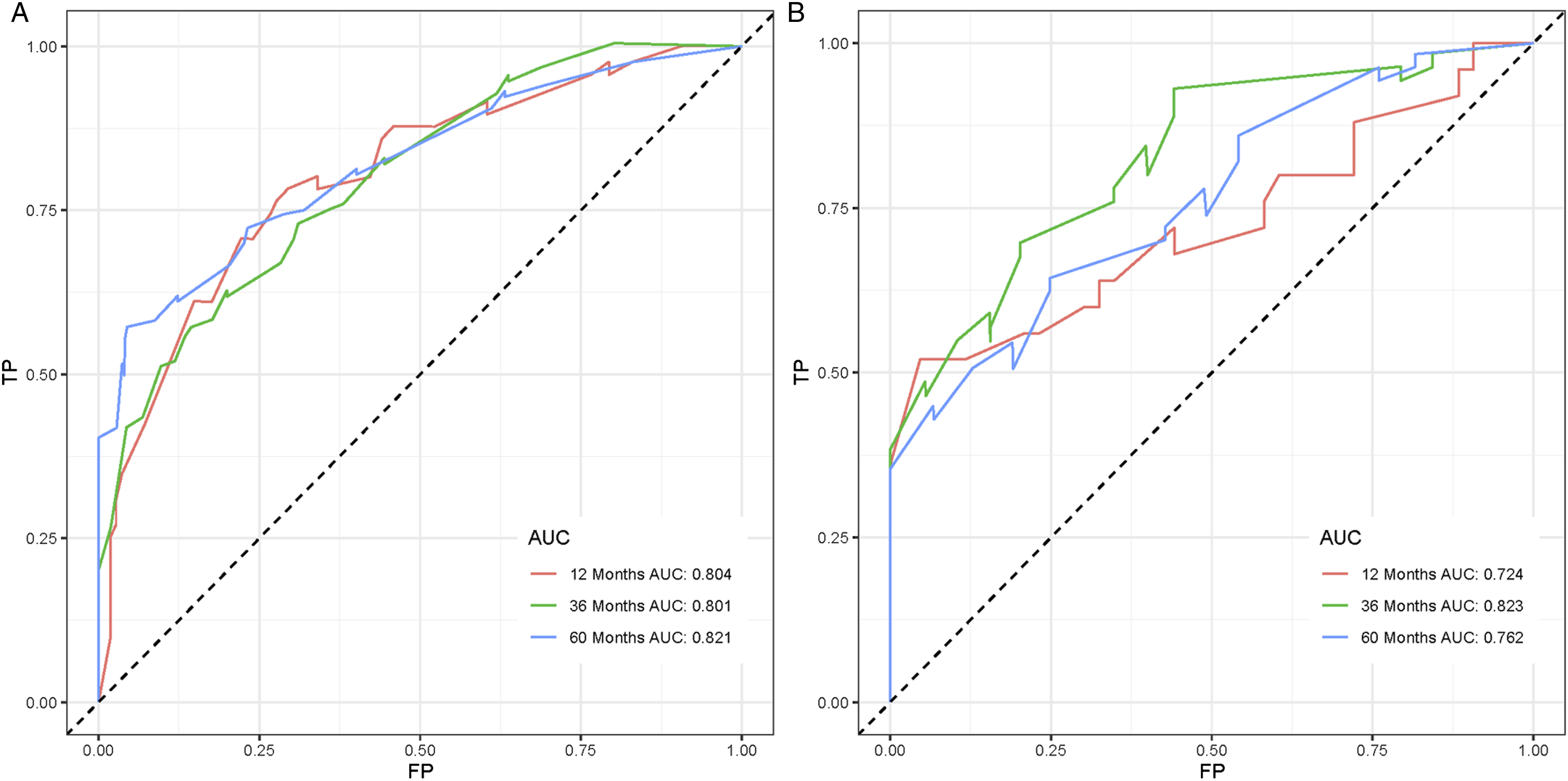
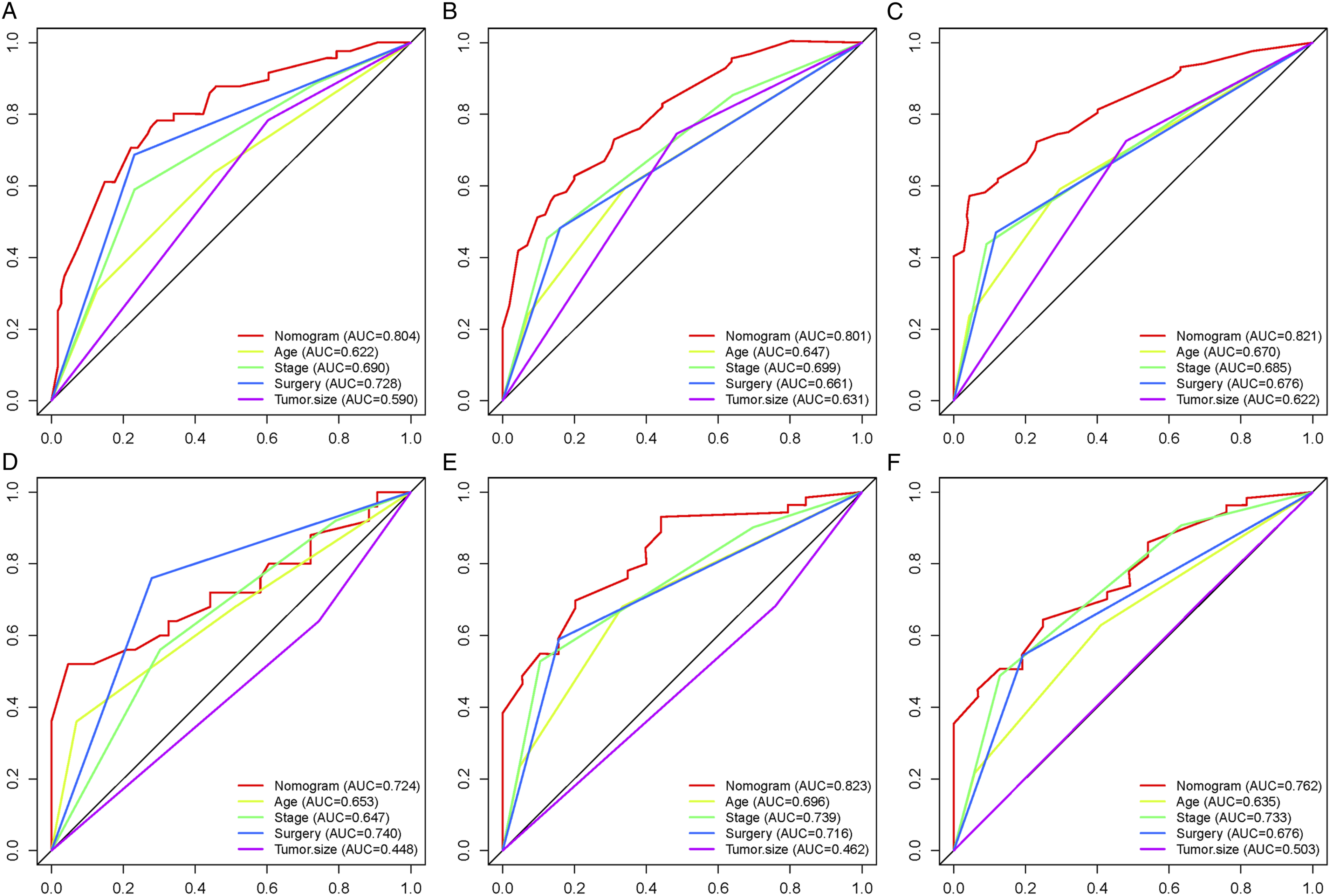
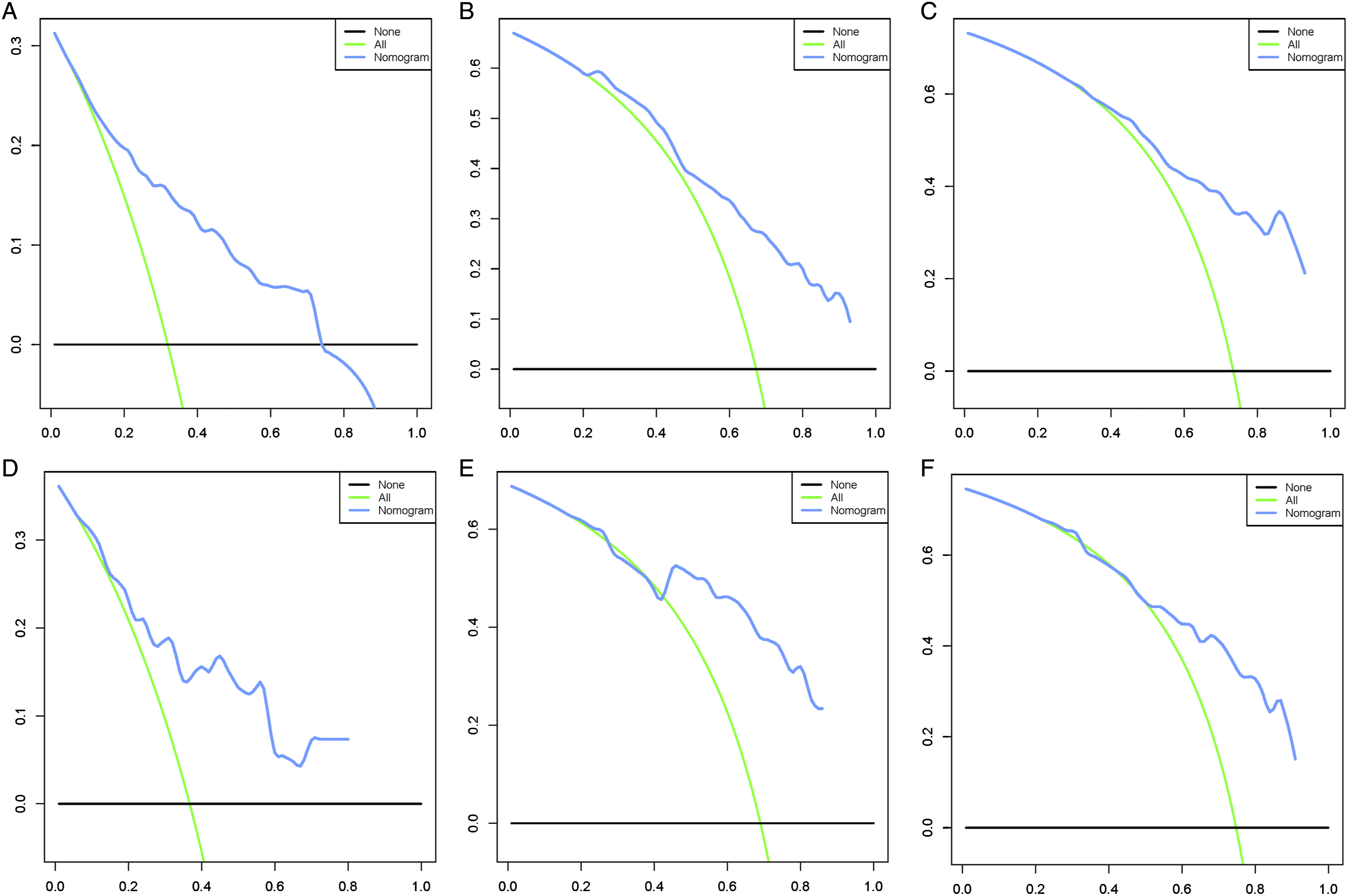
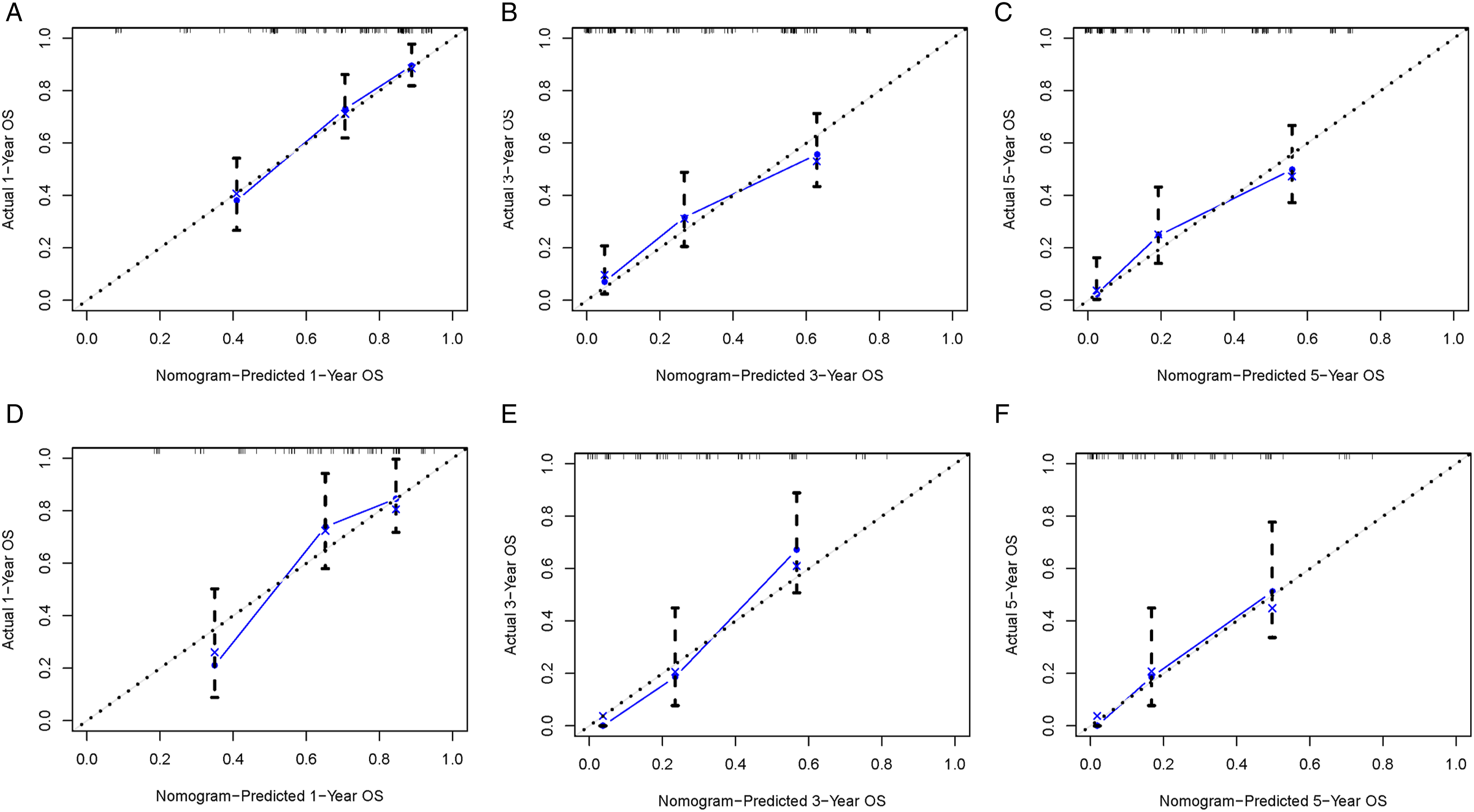
We combined four independent prognostic factors for overall survival and developed a nomogram for predicting the overall survival (Figure 3). By obtaining relevant clinical data of patients such as stage, tumor size, age, and surgery, we can easily observe the corresponding scores of each prognostic factor from the nomogram to calculate an overall score. Meanwhile, by making a vertical line on the total score axis, we can get the overall survival rate of that patient at 1, 3, and 5 years (Figure 3). For ease of understanding and application, we present an example as follows: a 25-year-old patient was diagnosed with spinal osteosarcoma with a tumor size of 100 mm. The patient was treated surgically and some time later was found to have distant metastasis of the tumor. By settlement, we found that his total score was 186, and the mortality rates predicted by the corresponding model for the patient at 1, 3, and 5 years were 29.8%, 75.4%, and 83.1%, respectively. To facilitate the clinical application of our line graphs, we have also created a web-based nomogram (https: // hzhorthopaedics. shinyapps.io / webnomogram/). To evaluate the discriminatory performance of the model, we calculated the C-index and the area under the receiver operating characteristic curve of the model in 2 sets, respectively. The model was internally validated in the training set with AUC values of .737, .804, .801, and .821 for the C index and predicted 1, 3, and 5 years of overall survival, respectively (Figure 4). We also externally validated the model in the validation set, and the results showed that the C-index and the AUC values for predicting overall survival at 1, 3, and 5 years were .693, .724, .823, and .762, respectively (Figure 4). The above results indicated that the nomogram had a good identification ability. To further verify the superiority of the model, we further compared the difference in prediction accuracy between using the nomogram model and individual prognostic factors to predict overall survival. As shown in Figure 5, the accuracy of using the model to predict overall survival at 1 year, 3 years, and 5 years was significantly superior compared to prediction using a single independent prognostic factor. Analysis of the decision curves for the internal validation set and the external validation set showed that the nomogram provided a greater net benefit than the "treat all" or "no treatment" strategy across a wide range of mortality risks, suggesting that the nomogram has good potential clinical validity (Figure 6). In addition, calibration curves were plotted in two cohorts to predict overall survival at 1, 3, and 5 years (Figure 7). As shown in Figure 7, the curves fall close to the ideal dashed line at 45°, indicating a high fit between the model-predicted outcomes and those that occurred. The nomogram for patients with spinal osteosarcoma. Receiver operating characteristic curves for patients. (A) Training set, (B) Validation set. Comparison of the prediction accuracy between the nomogram and independent prognostic factors. The receiver operating characteristic curves of nomogram and all independent predictors at 1- (A), 3- (B), and 5-years (C) in the training set and at 1- (D), 3- (E), and 5-years (F) in the validation set. Decision curve analysis for 1- (A), 3- (B), and 5-years (C) prediction in the training set (A-C), validation set (D-F), respectively. Calibration curves for 1- (A), 3- (B), and 5-years (C) prediction in the training set. Calibration curves for 1- (D), 3- (E), and 5-years (F) prediction in the validation set.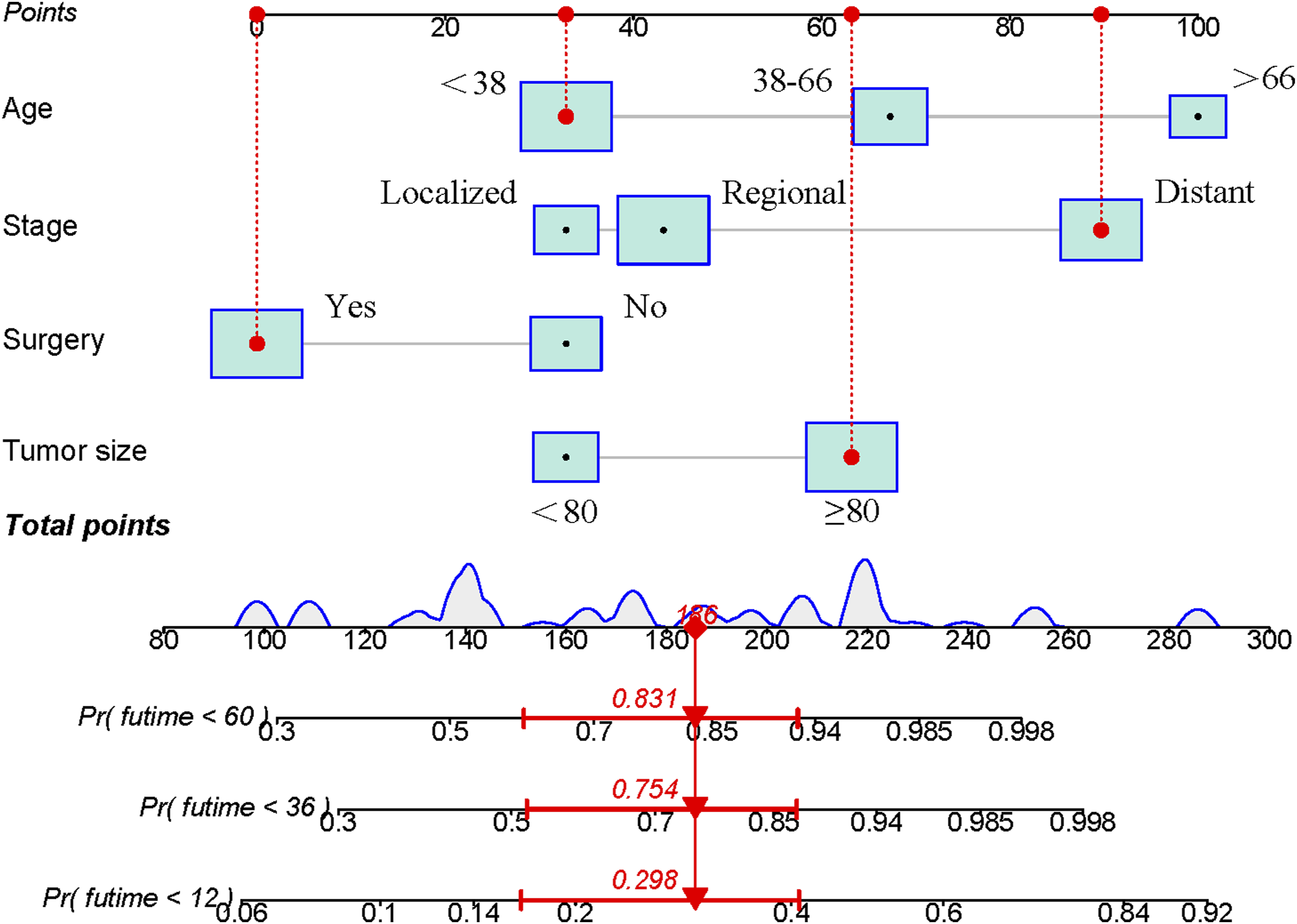
Risk Classification System
To facilitate the stratification of mortality risk for patients, we further constructed a risk classification system based on the nomogram model. First, the nomogram model was used to calculate the total scores of the patients in the training and validation sets. Concomitantly, we used the X-tile software to determine the appropriate truncation value to achieve the truncation of the total score. The optimal cutoff value for the total score was 223, so we included patients with a total score less than 223 in the low mortality risk group, while patients with a total score greater than or equal to 223 were included in the high mortality risk group. To verify the validity and correctness of the risk differentiation system, we further plotted Kaplan-Meier survival curves for the different mortality risk subgroups in the 2 sets. In the training set, the median survival time was 7 months (95% confidence intervals, 3.338-10.662) for patients at high risk of death and 25 months (95% confidence intervals, 19.237- 30.763) for patients at low risk of death. As shown in Figure 8, patients in different mortality risk subgroups in both cohorts showed significant differences, i.e., patients in the low mortality risk group had a significantly better prognosis than patients in the high mortality risk group. It further strongly demonstrates that our constructed nomogram-based risk classification system can effectively distinguish between high risk and low risk patients, thus enabling the stratification of patients' mortality risk. Kaplan–Meier survival analysis were performed for comparing overall survival in the high risk and low risk subgroups of all patients in the training set (A) and validation set (B).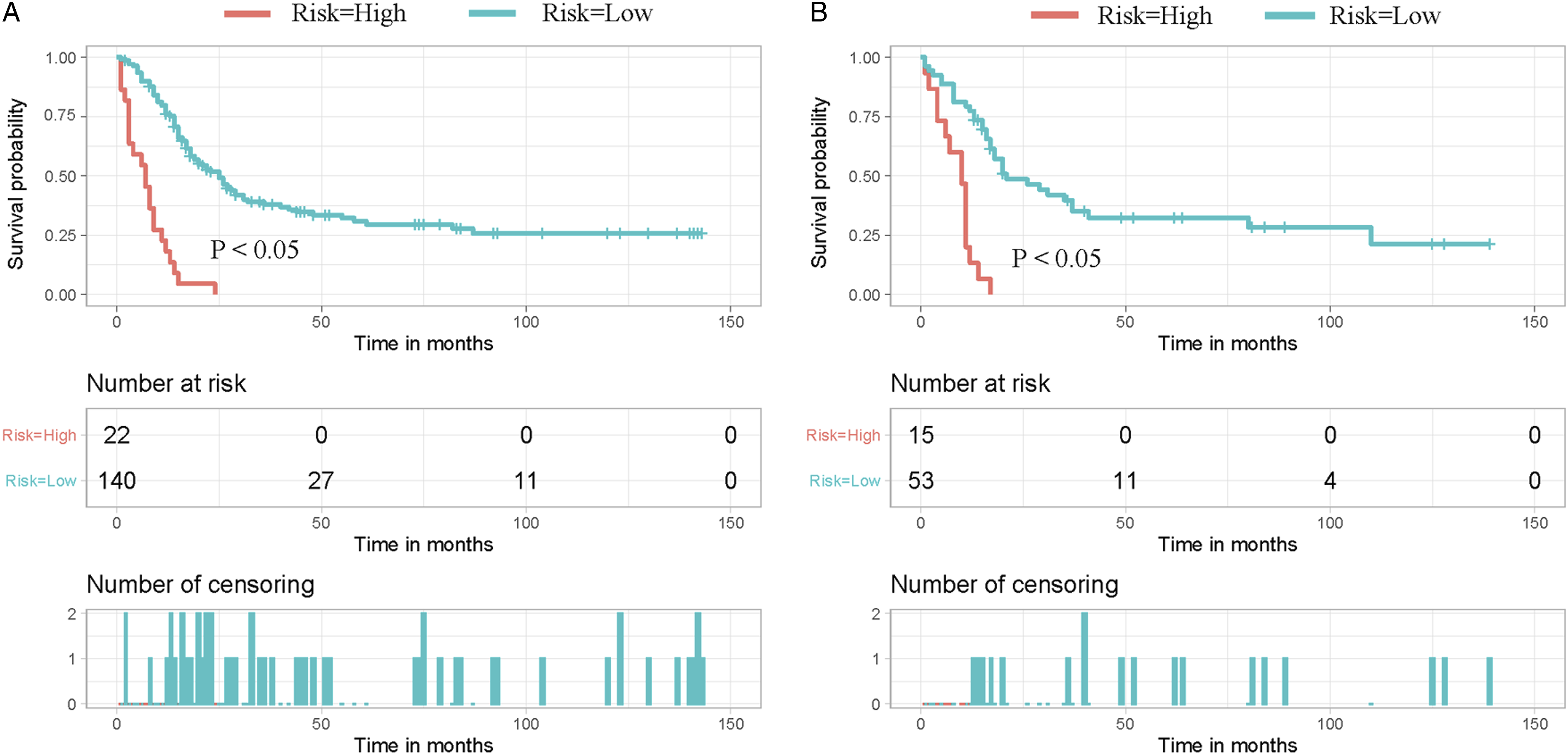
Discussion
Osteosarcoma is 1 of the most frequent malignant bone tumors, and it has the highest prevalence among primary bone tumors, with a 5.6/1 million incidence and a 60% 5-year overall survival rate. 11 Due to the specificity of the spine location, its potential for local invasive destruction and systemic metastasis is high, 12 and it easily invades key structures of the spinal cord and nerve roots, thus its prognosis is poor, with overall survival of only 18 months. 13 In this study, we identified age, stage, tumor size, and surgery as independent prognostic factors for patients. Based on this, we developed a novel nomogram and risk classification method based on this to achieve patient stratification and accurate overall survival prediction.
It was found that as age increases, the overall survival of patients decreases subsequently. This may be since elderly patients are more prone to distant metastases, as well as their relatively poor physical condition, their poor tolerance to surgery, chemotherapy, and radiation therapy, and the high number of postoperative and other treatment complications, which in turn reduces survival time. 14 Previous studies have shown that tumor size is a prognostic variable for osteosarcoma, 15 which is the same as our findings. Through our analysis, we found that the larger the tumor, the worse the prognosis of the patients. The reason for this may be due to the high number of blood vessels and nerves adjacent to the medial skeleton, and tumors originating in these areas often present with symptoms such as nerve compression, vertebral instability, and pathological fractures, which adversely affect the quality of life and overall survival. 16
At the same time, the primary surgical goal in osteosarcoma is to obtain negative margins, and due to the anatomical limitations of the spine. The larger the tumor the more difficult it is to achieve negative margins, further reducing the patient's overall survival. Surgeons have difficulty obtaining adequate margins for tumor removal, and the procedure is often accompanied by extensive bleeding, with severe bleeding even leading to hemorrhagic shock in patients. However, for patients with spinal osteosarcoma, the need for and importance of surgery is self-evident. The stage is likewise an independent prognostic indicator in patients. Several studies have shown that patients with metastases from other sites have significantly shorter survival than patients without metastases. Differences in the stage will change the manner, extent, and type of treatment for patients. For example, isolated lesions may receive local treatment, whereas metastases require systemic treatment. 10
Surgery is the main treatment modality for patients with osteosarcoma and has the effect of removing the tumor, relieving local pain, and decompressing the spinal cord. 17 David et al showed that surgical treatment significantly improved overall survival in patients with spinal osteosarcoma, with a 5-year survival rate of 43% in patients with spinal osteosarcoma after surgical resection, compared to 22% without surgery. 1 This is the same as our findings, where the overall survival rate of operated patients was higher than that of non-operated patients at 3 and 5 years. Both radical and palliative surgery reduce the tumor load of patients to some extent, and the reduction of tumor load may delay the development of complications such as cachexia, thus reducing the risk of cancer death in patients. 18
Before the 1970s, treatment options for osteosarcoma were limited to surgical resection, and currently, long-term overall survival for patients with osteosarcoma has been improved based on multidrug chemotherapy regimens such as anthracyclines and adriamycin. 19 However, in our study, chemotherapy was not a prognostic influencing factor in improving the prognosis of patients. The reason for this may be the late stage of patients, as well as the large tumors, which are adverse factors that lead to poor response to chemotherapy drugs and reduce the overall survival of patients. 20 Osteosarcoma is relatively insensitive to radiation therapy, while the radiation dose required for radiotherapy in patients with osteosarcoma is relatively high. 21 Due to the special spinal structure, too high a dose of radiotherapy will damage the normal function of the spinal cord, causing irreversible or even fatal harm. 22 Therefore, effective radiation doses cannot be achieved in radiotherapy for osteosarcoma, making it difficult to improve overall survival. However, radiotherapy can be used as a palliative measure for patients who cannot undergo surgery or after palliative surgery, especially for patients with spinal cord compression. 23
At the same time, there are shortcomings in our study. First, this study is based on the SEER database, which is a retrospective study and inevitably suffers from selection bias, and further studies should be done after expanding the sample and including patients from more geographical areas. Second, the SEER database does not describe detailed treatment information such as surgical approach, postoperative margins, chemotherapy regimen, radiotherapy dose, etc., so we could not conduct a deeper analysis. Third, targeted therapy and immunotherapy for malignant tumors are now being carried out to varying degrees, and our study needs to be expanded accordingly.
Conclusion
This study updates our current knowledge of the clinical features of primary spinal osteosarcoma. In addition, a nomogram model and risk classification system for predicting prognosis in primary spinal osteosarcoma patients was developed. By building a prognostic model, over-or under-treatment can be avoided and inform clinicians in developing treatment plans.
Footnotes
Author Contributions
Zhangheng Huang and Qingquan Kong conceived and designed the study. Zhangheng Huang and Chao Huang performed the literature search. Zhangheng Huang, Yu Wang, and Ye Wu generated the figures and tables. Zhangheng Huang, Chuan Guo, and Weilong Li analyzed the data. Zhangheng Huang wrote the manuscript and Qingquan Kong critically reviewed the manuscript. Zhangheng Huang and Qingquan Kong supervised the research. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by, China, Sichuan Science and Technology Program (2020YFS0080, 2020YFQ0007,2021JDRC0159), Science and Technology Project of Tibet Autonomous Region (XZ201901-GB-08), The National Natural Science Foundation of China (81171731), and the 1·3·5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC21026, ZYJC21077).
Ethics approval and consent to participate
The study is based on data from public databases and therefore does not require informed consent from patients.
Availability of Data and Materials
The data for this study can be found in the SEER database. Data were downloaded and processed as described in Materials and methods.