
Abstract
Objective
The current study aimed to explore the prognostic value of the lymph node ratio (LNR) in patients with lung neuroendocrine carcinomas (LNECs).
Methods
Data for 1564 elderly patients with LNECs between 1998 and 2016 were obtained from the Surveillance, Epidemiology, and End Results database. The cases were assigned randomly to training (n = 1086) and internal validation (n = 478) sets. The association between LNR and survival was investigated by Cox regression.
Results
Multivariate analyses identified age, tumor grade, summary stage, M stage, surgery, and LNR as independent prognostic factors for both overall survival (OS) and lung cancer-specific survival (LCSS). Tumor size was also a prognostic determinant for LCSS. Prognostic nomograms combining LNR with other informative variables showed good discrimination and calibration abilities in both the training and validation sets. In addition, the C-index of the nomograms was statistically superior to the American Joint Committee on Cancer (AJCC) staging system in both the training and validation cohorts.
Conclusions
These nomograms, based on LNR, showed superior prognostic predictive accuracy compared with the AJCC staging system for predicting OS and LCSS in patients with LNECs.
Keywords
Introduction
Lung neuroendocrine carcinomas (LNECs), including small cell carcinoma and large cell neuroendocrine carcinoma, are among the most lethal malignant tumors with aggressive clinical behavior and a poor prognosis.1–5 However, neuroendocrine tumors of the lung can be diagnostically and prognostically challenging due to their morphologic overlap with other conditions and their complex and heterogeneous biological behaviors.6–8 The identification of patients with LNECs who are at high risk of a poor prognosis will thus ensure the implementation of appropriate treatments and have a substantial impact on their prognosis.
Tumor nodal status is regarded as one of the most important prognostic markers for solid-organ malignant neoplasms and is an important element affecting therapeutic decision-making and the prognosis of various cancers.9–11 The lymph node ratio (LNR), defined as the ratio of the number of positive lymph nodes (PLNs) to the total number of resected lymph nodes (RLNs), has become an important prognostic factor for solid tumors, as well as neuroendocrine carcinomas in other sites.12–18 However, little information is available regarding the prognostic role of LNR in patients with LNECs. This study thus aimed to explore the associations of LNR with overall survival (OS) and lung cancer-specific survival (LCSS) in patients with LNECs, and to develop and validate new prognostic models to predict 3-, 5-, and 10-year OS and LCSS based on the Surveillance, Epidemiology, and End Results (SEER) database.
Methods
Study population
This retrospective study included patients with newly diagnosed LNECs according to positive histology from 1998 to 2016, based on the International Classification of Diseases for Oncology, 3rd Edition ‘(ICD-O-3)/WHO 2008’ (Lung and Bronchus) and ‘ICD-O-3 Hist/bahav’ (8013/3, large-cell neuroendocrine carcinoma, 8246/3: Neuroendocrine carcinoma, NOS and 8574/3, adenocarcinoma with neuroendocrine differentiation). The methods of data collection and patient follow-up are available on the SEER database. We excluded patients with a history of other malignancies and unknown variables, including race/ethnicity, age at diagnosis, TNM stage, American Joint Committee on Cancer (AJCC stage), marital status, survival months, number of PLNs, and number of RLNs. The included patients were randomly assigned to a training group or a validation group.
Variables
The following variables were identified from the dataset: year of diagnosis (1998–2003, 2004–2010, 2011–2016), age at diagnosis (<60 or ≥60 years), race (White, Black, or other), marital status (married or unmarried), primary site (main bronchus, upper lobe, middle lobe, lower lobe, and overlapping lesion of lung), laterality (left, right, or bilateral), grade (I/II or II/IV), SEER summary stage (localized, regional, or distant), tumor size (<3, 3–5, or >5 cm), AJCC stage (I/II or III/IV), T stage (T0/T1/T2 or T3/T4), N stage (N0/N1 or N2/N3), M stage (M0 or M1), surgery for primary site (no/unknown, wedge resection, lobectomy, or pneumonectomy), chemotherapy (yes or no/unknown), and radiotherapy (yes or no/unknown). The LNR was stratified into three risk groups by X-tile 19 (0.0, 0.0–0.2, and >0.2). The primary outcome of this study was OS and the secondary outcome was lung cancer-specific survival (LCSS). All the information in the SEER database has been de-identified and is freely available to the public, and no ethics committee approval for the analysis was therefore required. The authors signed a data-use agreement and obtained permission from the SEER program to use these data. The study was conducted according to the Declaration of Helsinki (as revised in 2013).
Statistical analysis
Categorical variables were reported as number and percentage and continuous measurements were presented as mean and range. Categorical variables were compared using χ2 tests and continuous variables were compared using t-tests or Mann–Whitney U tests. Survival differences among different LNR groups were compared by Kaplan–Meier survival analysis and log-rank tests. Multivariate analyses were conducted using Cox regression analysis. A nomogram was formulated with potential risk factors (P < 0.05) based on results of multivariate analysis. A time-dependent receiver operating characteristic curve (td-ROC), calibration curve, and decision curve analysis (DCA) were calculated to evaluate the predictive performance of the prognostic nomograms. All statistical analyses were performed using R (version 3.4.3; www.r-project.org). A two-sided P value <0.05 was defined as statistically significant.
Results
Patient characteristics
From 1998 to 2016, 1564 patients with LNECs were included in the study and assigned randomly to a training group and a validation group at a ratio of 7:3 (training cohort, n = 1086; validation cohort, n = 478). There were no significant differences between the two sets, according to analysis of variance (Table 1). The median survival times were 38.0 (10.0, 82.0) months in the training set and 41.0 (11.0, 92.5) months in the validation set. Other clinical and pathological features are listed in Table 1.
Clinicopathological characteristics of all patients.

AJCC, American Joint Committee on Cancer; RLN, resected lymph node; PLN, positive lymph node; LNR, lymph node ratio; OS, overall survival; LCSS, lung cancer-specific survival.
Independent prognostic factors for OS
Univariate and multivariate analyses were performed to identify factors that were significantly associated with OS (Table 2). In the training cohort, year of diagnosis, age at diagnosis, sex, primary site, laterality, tumor grade, SEER summary stage, AJCC stage, T stage, N stage, M stage, tumor size, chemotherapy, surgery primary site, radiation, and LNR were significantly associated with OS in univariate analysis (P < 0.05), while age at diagnosis, tumor grade, summary stage, M stage, surgery for primary site, and LNR were also autonomous prognostic determinants for OS in multivariate analysis.
Univariate and multivariate analyses of factors associated with overall survival.

HR, hazard ratio; CI, confidence interval; AJCC, American Joint Committee on Cancer; LNR, lymph node ratio.
Kaplan–Meier survival curves demonstrated a significant association between poorer OS and an LNR >0.2, compared with groups with a lower LNR, in both the training and validation cohorts (Figure 1a, 1b).
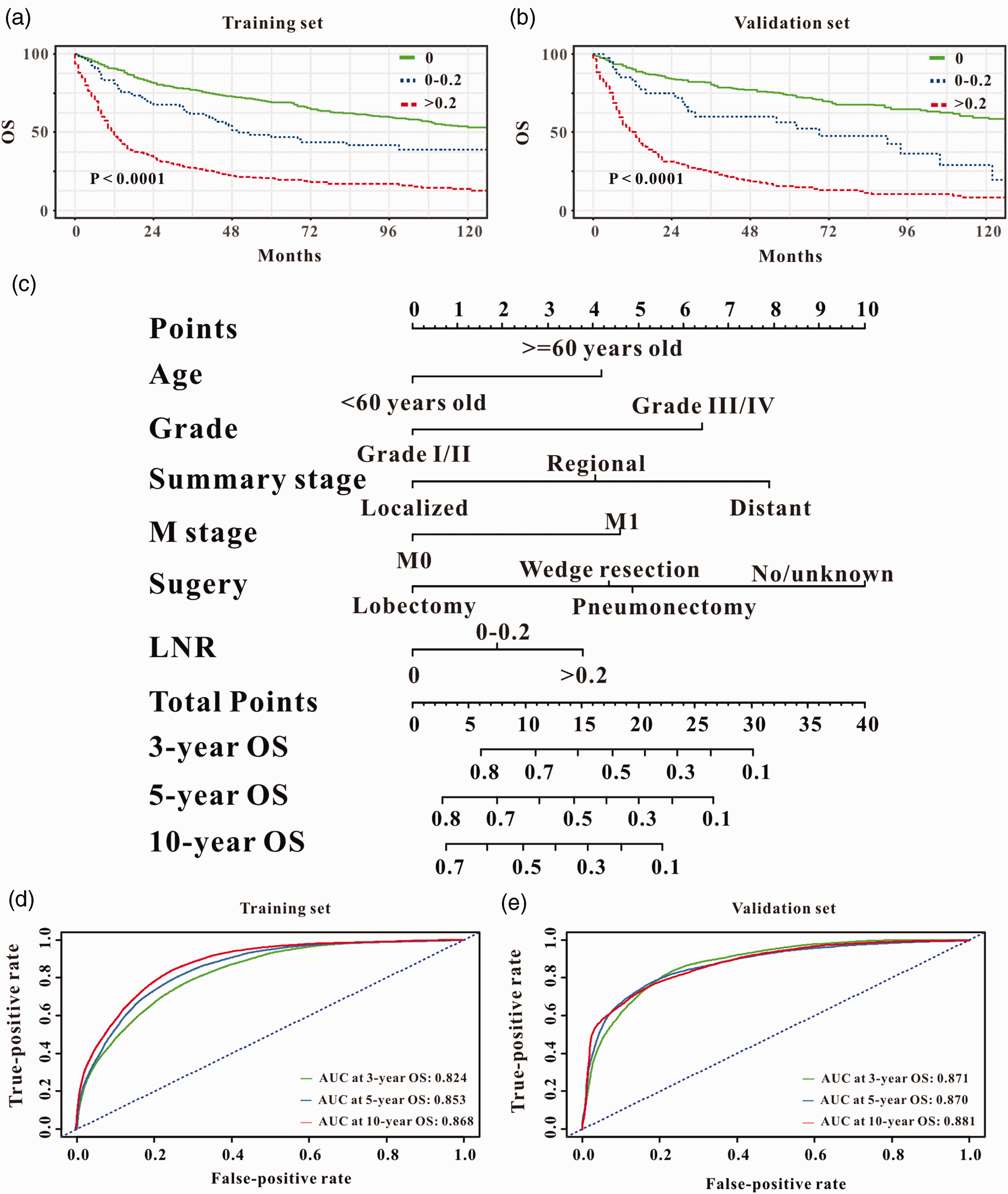
Prognostic importance of lymph node ratio (LNR) in patients with lung neuroendocrine carcinomas. Kaplan–Meier curves for overall survival (OS) for all patients stratified by LNR in the (a) training and (b) validation cohorts. Prediction of 3-year, 5-year, and 10-year OS (c) in patients with LNECs using a survival nomogram. Predictive ability of survival nomograms measured by time-dependent receiver operating characteristic (td-ROC) curves. td-ROC curves for 3-year, 5-year, and 10-year OS in patients in the (d) training and (e) validation cohorts.
Development and validation of prognostic nomogram for OS
Based on the results of multivariate analysis, we formulated a prognostic nomogram to predict 3-, 5-, and 10-year OS in the training cohort (Figure 1c). td-ROC analyses (Figure 1d, 1e) revealed that the prognostic nomogram could accurately predict 3-year (area under the curve [AUC] = 0.821), 5-year (AUC = 0.857), and 10-year (AUC =0.870) OS in the training set, and 3-year (AUC = 0.876), 5-year (AUC = 0.874), and 10-year (AUC = 0.876) OS in the validation set in patients with LNECs. The calibration curves of the survival nomogram are shown in Figure 2a–2f. The plots were close to the 45° line, indicating that the survival nomogram was well-calibrated in the training and validation sets.

Calibration curves for predicting overall survival (OS) in the training (a–c) and validation sets (d–f).

Prognostic importance of lymph node ratio (LNR) in patients with lung neuroendocrine carcinomas. Kaplan–Meier curves for LCSS for all patients stratified by LNR in the (a) training and (b) validation cohorts. Prediction of 3-year, 5-year, and 10-year LCSS (c) in patients with LNECs using a survival nomogram. Predictive ability of survival nomograms measured by time-dependent receiver operating characteristic (td-ROC) curves. td-ROC curves for 3-year, 5-year, and 10-year LCSS in patients in the (d) training and (e) validation cohorts.

Calibration curves for predicting overall survival (OS) and lung cancer-specific survival (LCSS) in the training and validation sets. The 3-year, 5-year, and 10-year OS calibration plots in the (a–c) training and (d–f) validation cohorts.
Development and validation of prognostic nomogram for LCSS
Multivariate analysis identified age at diagnosis, tumor grade, summary stage, M stage, surgery for primary site, tumor size, and LNR as autonomous prognostic determinants for LCSS in the training cohort (Table 3). Moreover, Kaplan–Meier curves also demonstrated a significant association between poorer LCSS and an LNR >0.2 compared with groups with a lower LNR, in both the training and validation cohorts (Figure 3a, 3b).
Univariate and multivariate analyses of factors associated with lung cancer-specific survival.

HR, hazard ratio; CI, confidence interval; AJCC, American Joint Committee on Cancer; LNR, lymph node ratio.
Based on the results of multivariate analysis, we formulated a prognostic nomogram to predict 3-, 5-, and 10-year LCSS in the training cohort (Figure 3c). td-ROC analyses (Figure 3d, 3e) revealed that the prognostic nomogram could accurately predict 3-year (AUC = 0.855), 5-year (AUC =0.866), and 10-year (AUC = 0.876) LCSS in the training set, and 3-year (AUC =0.895), 5-year (AUC = 0.905), and 10-year (AUC = 0.884) LCSS in the validation set in patients with LNECs. The calibration curves of the survival nomogram are shown in Figure 4a–4f. The plots were very close to the 45° line, indicating that the survival nomogram was well-calibrated in the training and validation sets.
Comparison with AJCC TNM staging system
The C-index of the nomogram for OS in the training cohort was 0.834 (95% confidence interval [CI]: 0.810–0.858), which was significantly higher than that of the AJCC TNM staging system (0.702, 95% CI: 0.670–0.733). The C-index of the current nomogram for OS (0.874, 95% CI: 0.843–0.905) remained superior to that of the AJCC staging system (0.723, 95% CI: 0.677–0.768) in the validation cohort. Moreover, the nomogram for LCSS performed better than the AJCC staging system in the training set (0.844 vs. 0.725) as well as in the validation set (0.861 vs. 0.756).
In DCA, the current nomograms presented greater net benefits and a wider field of threshold probability compared with the AJCC staging system for both OS and LCSS in the training (Figure 5a, 5c) and validation cohorts (Figure 5b, 5d), indicating that these nomograms had superior predictive abilities for the prognosis of patients with LNECs. A higher threshold probability resulted in a more robust estimation of decision results. The results indicated that the formulated nomograms provided better predictions of survival in patients with LNECs.

Decision curve analysis (DCA) of survival nomograms to determine their clinical use. DCA of survival nomogram for overall survival in the (a) training and (b) validation sets. DCA of lung cancer-specific survival nomogram in the (c) training and (d) validation sets.
Discussion
The current study aimed to evaluate the association between LNR and survival status in patients with LNECs. To the best of our knowledge, this is the first study to demonstrate that elevated LNR may be an independent prognostic factor for OS, as well as LCSS, in patients with LNECs. Notably, survival nomograms incorporating LNR and other significant clinical variables showed good ability for predicting OS and LCSS in patients with LNECs.
Lymph node involvement is regarded as one of the most important indicators informing therapeutic decision-making and the prognosis of patients with malignant tumors. Norifumi et al. demonstrated that lymph node metastasis was significantly associated with disease-free survival in a retrospective study of 95 consecutive patients with pancreatic neuroendocrine tumors undergoing pancreatic resection, and patients required lymph node dissection to improve prognosis. 20 Using data from the National Cancer Database and SEER database, Adam et al. concluded that the number of positive locoregional lymph nodes was an independent prognostic factor in patients with colon neuroendocrine tumors, and they developed a new nodal staging system that could predict survival more accurately than current staging systems. 21 In the current study, LNR was considered an independent predictive factor for OS and LCSS in 1564 patients with LNECs, based on univariate and multivariate analyses. We then generated two prognostic nomograms by combining LNR with other informative clinical features, which showed good predictive values for OS and LCSS, respectively, in patients with LNECs.
The AJCC staging system has been widely used for prognostic prediction in patients with lung cancer and other malignant tumors.22–25 However, previous studies have shown that lymph node status in the AJCC staging system might not adequately reflect the extent of disease, due to the influence of surgery. 26 LNR, which reflects not only nodal disease but also the quality and extent of lymphadenectomy, has recently been demonstrated to be a good prognostic factor for malignant tumors.26–29 Li et al. reported that patients with gastric neuroendocrine tumors with an LNR >0.132 had an increased likelihood of all-cause mortality and cancer-specific death compared with patients with an LNR value ≤0.132. 30 The prognostic significance of LNR was also verified in a retrospective study of 1778 patients with resected N2 stage lung squamous cell carcinoma. 31 Consistent with those results, our study also suggested that a higher LNR value was associated with poorer OS and LCSS in patients with LNECs. In addition, we combined LNR with other significant variables to create survival nomograms, which showed better predictive abilities for OS and LCSS compared with the AJCC staging system, implying that these combined indexes might be useful for accurately predicting the prognosis in patients with LNECs.
As an easy-to-use statistical predictive instrument, nomograms can digitize risk by creating an intuitive graph and have been widely used in clinical practice.32–35 A nomogram merging some conducive variables is a readily accessible tool to help clinicians clarify a diagnosis, 32 predict survival, 36 and decide the follow-up interval for their patients. 37 In the current study, we successfully created two survival nomograms based on the LNR and other informative factors to predict OS and LCSS in patients with LNECs. These survival nomograms achieved better predictive performances than the AJCC staging system, as reflected by the C-index and DCA curves for both the training and validation sets. These survival nomograms might thus be applied in a clinical setting to reliably predict OS and LCSS in patients with LNECs.
This study had some limitations. First, it was a retrospective study using data from the SEER database and may have selection bias due to the ethnic homogeneity of the patient population. Second, some prognostic factors, including serum tumor markers, vascular infiltration, laboratory results, and detailed treatment strategies, which may have had an impact on patient prognosis, were not accessible in the SEER database. Moreover, the limitations of the SEER database meant that we could not obtain information on the exact chemotherapeutic drugs used for LNEC patients. In addition, patients were first diagnosed with LNECs over a considerable period of time and chemotherapy drugs may change over time. We therefore classified chemotherapy as performed or not to investigate its prognostic role for LNECs, but this might not be an accurate reflection of the role of chemotherapy. This might also explain why chemotherapy and radiotherapy were not included in the final nomogram for the prognosis of LNEC patients. Finally, although the prognostic nomograms performed better than the AJCC staging system in the current study, further studies are needed to validate our survival nomograms in patients with LNECs.
Conclusions
The novel survival nomograms provide an applicable tool with good discrimination and calibration abilities for predicting the prognosis of LNECs. These nomograms may have superior prognostic capabilities for patients with LNECs compared with the current AJCC staging system. Further studies are needed to validate and improve this model.
Footnotes
Data availability statement
All data used in this study are available from the corresponding author on a reasonable request.
Ethics statement
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interest
The authors have no conflicts of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.