
Abstract
Background
We aim to construct a practical clinical prediction model to accurately evaluate the overall survival (OS) of patients with primary spinal tumors after primary tumor resection, thereby aiding clinical decision-making.
Methods
A total of 695 patients diagnosed with a primary spinal tumor, selected from the Surveillance, Epidemiology, and End Results (SEER) database, were included in this study. The Cox regression algorithm was applied to the training cohort to build the prognostic nomogram model. The nomogram’s performance in terms of discrimination, calibration, and clinical usefulness was also assessed in the internal SEER validation cohort. The fitted prognostic nomogram was then used to create a web-based calculator.
Results
Four independent prognostic factors were identified to establish a nomogram model for patients with primary spinal tumors who had undergone surgical resection. The C-index (.757 for the training cohort and .681 for the validation cohort) and the area under the curve values over time (both >.68) showed that the model exhibited satisfactory discrimination in both the SEER cohort. The calibration curve revealed that the projected and actual survival rates are very similar. The decision curve analysis also revealed that the model is clinically valuable and capable of identifying high-risk patients.
Conclusions
After developing a nomogram and a web-based calculator, we were able to reliably forecast the postoperative OS of patients with primary spinal tumors. These tools are expected to play an important role in clinical practice, informing clinicians in making decisions about patient care after surgery.
Keywords
Introduction
Primary spinal tumors are a very rare malignancy, accounting for approximately 5% of all bone tumors and less than .2% of all tumors.1,2 Based on histopathological features and cellular origin, common histological types of primary spinal tumors include chordoma, osteosarcoma, chondrosarcoma, and Ewing sarcoma.3,4 Given the specific location of the spine, these tumors often invade and destroy adjacent structures such as nerves, blood vessels, and bone, resulting in localized pain, nerve deficits, and pathological fractures.5,6 The prognosis of patients with primary spinal tumors has improved in recent decades with rapid advances in surgical and oncological treatment, but these spinal tumors often recur and have low survival rates.3,6,7 At present, resection of the tumor remains the mainstay of treatment for primary spinal tumors. Previous studies have shown that all types of spinal tumors can benefit from surgical resection. 8
Personalized medicine is playing an increasingly important role in cancer treatment, so understanding the factors related to the prognosis of primary spinal tumors can help to stratify risk and guide treatment for patients. A nomogram is a graph that visualizes the mathematical relationships of a Cox regression model to predict the probability of a clinical event by combining independent risk factors. 9 According to previous studies, the nomogram has been reported to have better predictive power than the classical staging system in the prognosis of many cancers and is considered a better alternative to the classical staging system.10-12 In the field of spinal surgery, previous predictive scoring systems have been applied mainly to metastatic lesions of the spine, and few practical predictive models have been applied to primary spinal tumors.13,14 Wenhao Chen and Zhongyang Gao et al. constructed some nomograms model for predicting the prognosis of patients with osteosarcoma, but patients with primary sites located in the extremities were also included in their study. Therefore, when the model was applied to predict the survival of patients with primary spinal tumors, the results may be biased.15,16 If clinicians can predict in the perioperative period which tumor patients are associated with poorer survival after surgery, it will certainly help to develop treatment strategies to prolong the survival of patients with these malignancies.
A prognostic model that works for every patient will help predict life expectancy and aid decision-making in this complex area of spinal surgery. Therefore, this study aimed to conduct a large cohort study of patients who were diagnosed with a primary spinal tumor between 2004 and 2015 and who underwent resection of the primary tumor. First, the possible impact of several preoperative parameters on postoperative overall survival (OS) is explored. Secondly, a web-based nomogram model was constructed for predicting the OS of patients with primary spinal tumors after undergoing tumor resection.
Methods
Patients and Data Collection
We collected data from the Surveillance, Epidemiology, and End Results (SEER) database of patients with primary spinal tumors in this retrospective study. The SEER database has been collecting cancer-related information (cancer stage, treatment modalities, and survival data) since 1973 and currently covers approximately 28% of the total US population.17,18 We accessed the SEER database through SEER*Stat software and then obtained data on patients diagnosed with primary spinal tumors between 2004 and 2015. The inclusion criteria for data extraction were that (1) The tumor’s primary site was in the spine, (2) the primary tumor site was undergoing resection, (3) complete clinicopathological and follow-up data were available. Exclusion criteria: (1) the spinal tumor was not the patient’s only primary tumor; (2) the patient’s survival time was shorter than 1 month; (3) relevant information about the patient was missing, such as disease stage, tumor grade, histological type, etc. Ultimately, a total of 695 eligible patients with primary spinal tumors were identified and subsequently randomly classified in a ratio of 7:3 to the SEER training cohort and the SEER external validation cohort. Also, as this study was retrospective and the patient data was used anonymously, we did not require informed consent.
In the current study, we extracted clinicopathological and demographic information about the patients, including age, race, sex, tumor grade, radiotherapy status, chemotherapy status, laterality, histological type, disease stage, tumor size, marital status, survival status, and survival time. The disease stage is categorized as (1) localized (tumor confined to the periosteum), (2) regional (tumor extending from outside the periosteum into surrounding tissues, including adjacent skeletal muscle, adjacent bone/cartilage, or skin), and (3) distant metastases have occurred. Age was divided into 2 subgroups of <60 years and ≥60 years. The selection and definition of survival endpoints play a very important role in cancer-related studies. Therefore, we selected OS as the study’s primary endpoint, which we defined as the time from diagnosis to death or the last follow-up visit.
Statistical Analysis
The SEER training cohort was used to build the nomogram and for internal validation of the nomogram, while the SEER validation cohort was used for external validation of the nomogram. Univariate Cox regression analyses were conducted to identify variables with significantly influenced OS, which were subsequently included in multivariate Cox regression analyses. Independent risk variables determined through multivariate Cox regression analysis were validated by Kaplan-Meier survival curve analysis and log-rank test. We developed a model for predicting postoperative OS of primary spinal tumors patients at 3, 5, and 8 years. Discrimination was evaluated by the C-index and the area under the receiver operating characteristic curve. The calibration curve was used to assess the goodness of fit between the predicted and observed values of the nomogram. The C-index and area under the curve values vary between .5 and 1.0, with values greater than .7 indicating a reasonable estimate. In addition, decision curve analysis was utilized to evaluate the nomogram’s clinical utility and net benefit. 19 Optimal cut-off points for mortality risk stratification were selected using X-tiles software. 20 The risk of death stratification based on the nomogram was compared using Kaplan-Meier survival curve analysis. Using the resulting survival probability formula, a web-based nomogram can be constructed using the “DynNom” software package to accurately calculate the postoperative OS of primary spinal tumors patients. All statistical analyses were carried out using SPSS 25.0 and R (www.r-project.org), with a P-value of less than .05 being considered statistically significant.
Results
Patient Characteristics
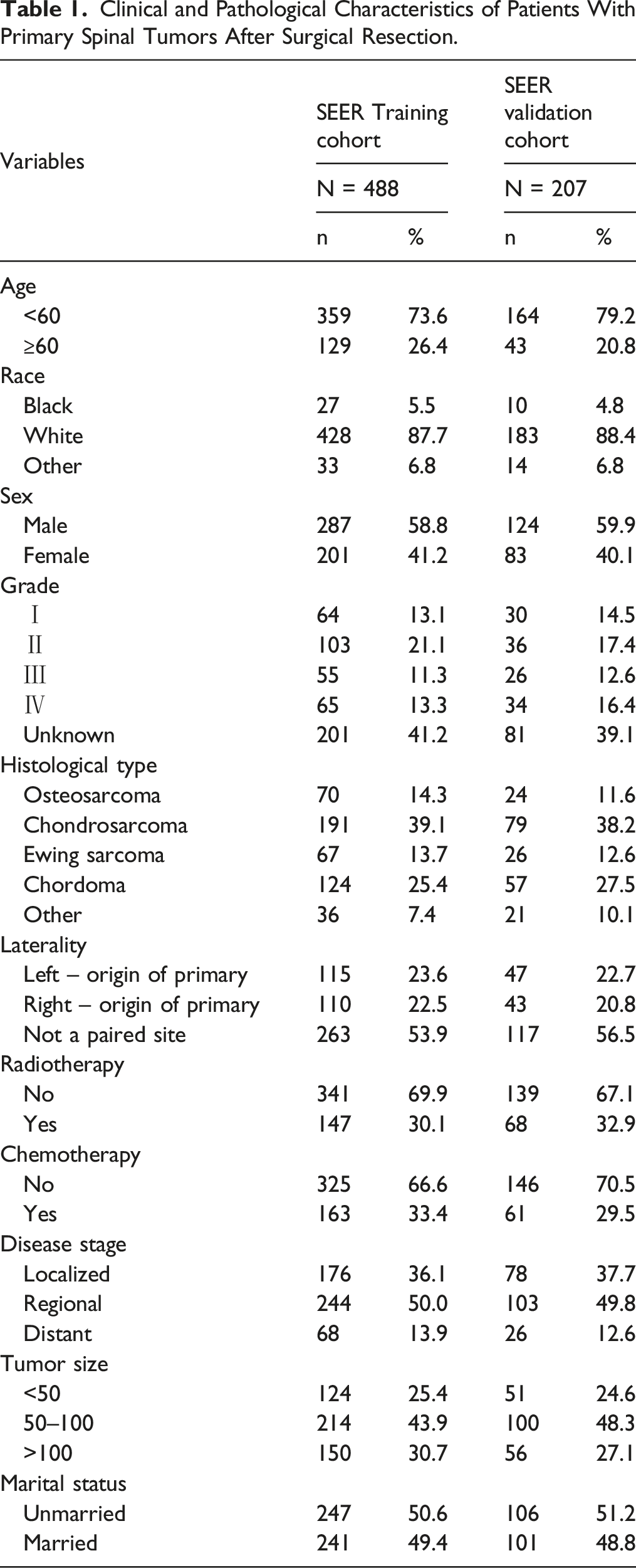
Clinical and Pathological Characteristics of Patients With Primary Spinal Tumors After Surgical Resection.
Nomogram Variable Screening
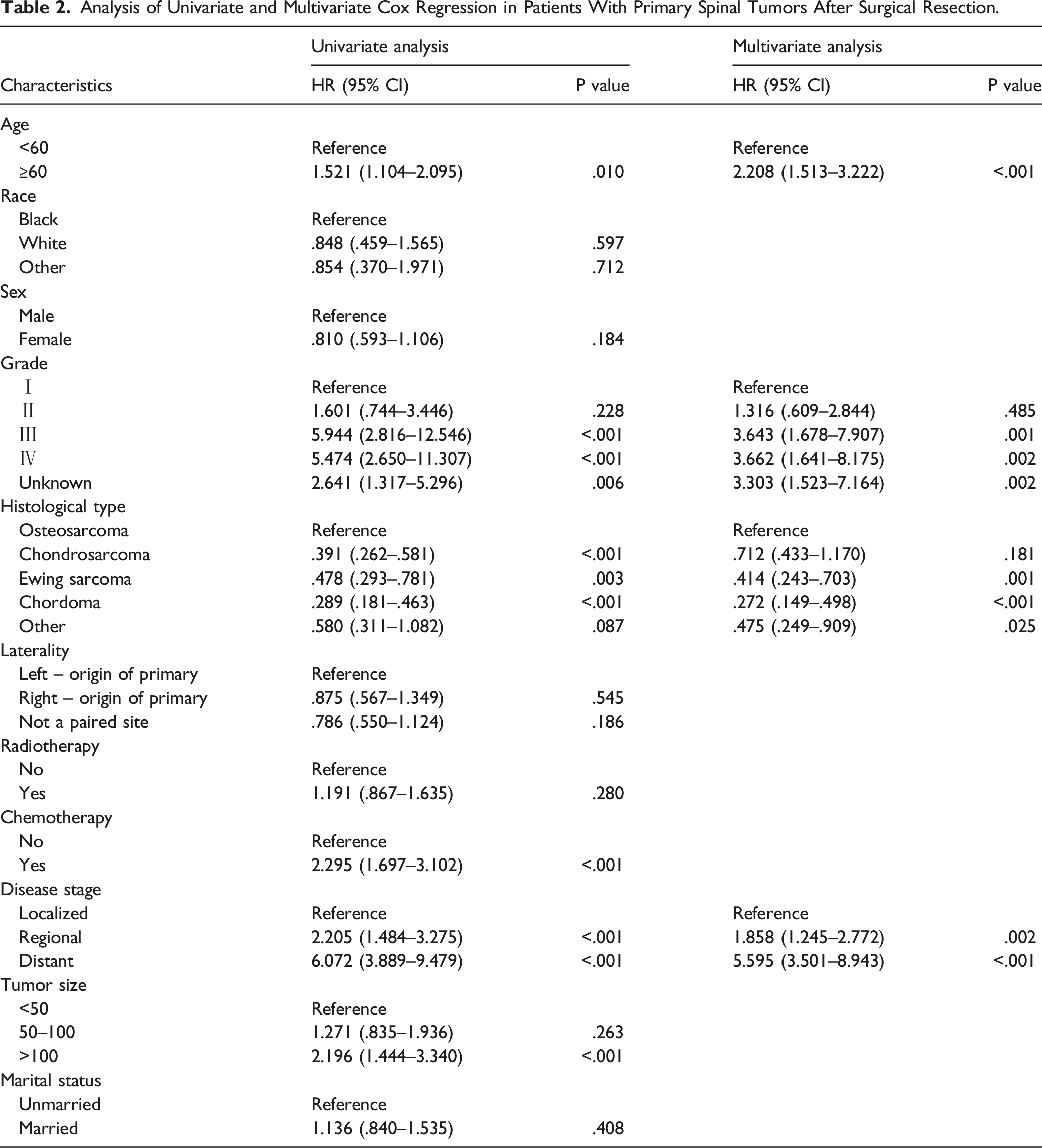
Analysis of Univariate and Multivariate Cox Regression in Patients With Primary Spinal Tumors After Surgical Resection.
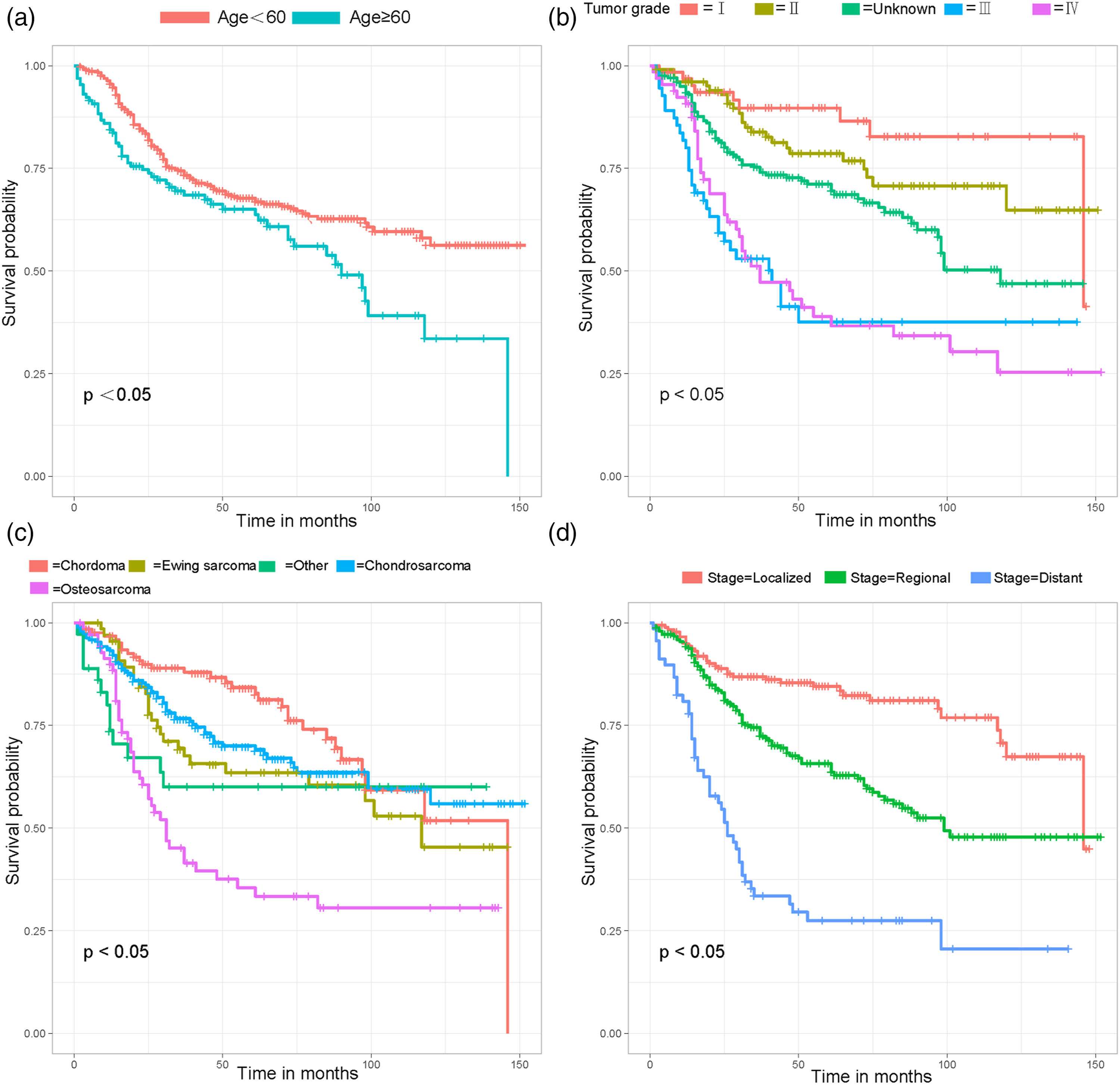
Kaplan-Meier survival curves for patient-related variables. (A) Age, (B) Tumor grade, (C) Histological type, (D) Disease stage.
Development and Validation of the Nomogram
We developed a nomogram for predicting the postoperative OS of primary spinal tumors patients based on the outcome of the Cox regression model (Figure 2). Using these nomograms, the OS probability for each patient can be determined by summing the specific values of each predictor variable. An example of using a nomogram to predict the OS for a given patient is shown in Figure 2. The probability of patient survival is determined by summing the specific values of each predictor variable and drawing a vertical line from the total score to the time axis. In this study, the total score of most patients was between 120 and 300. Prognostic nomogram for patients with primary spinal tumors after surgical resection.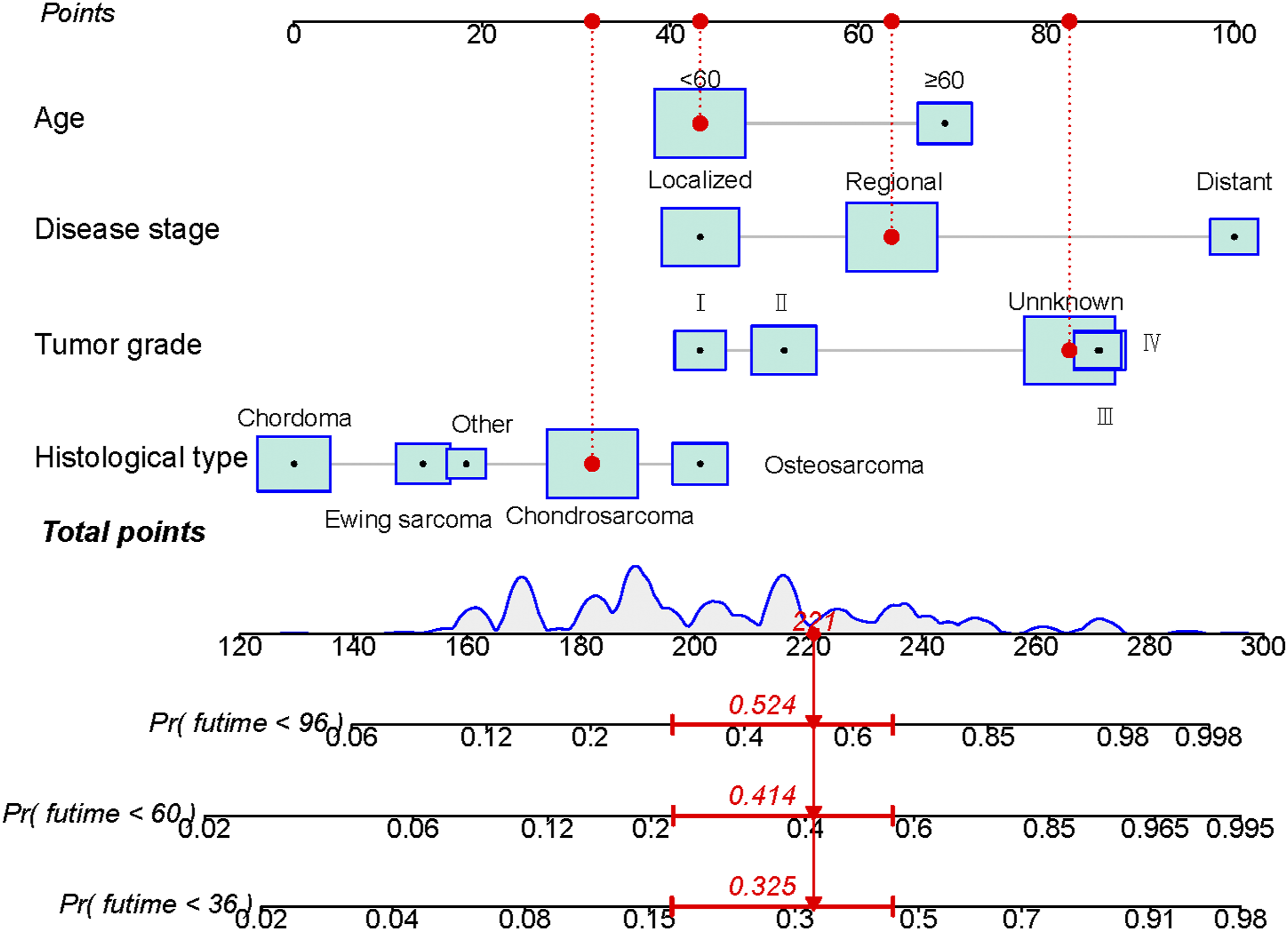
Validation of the Prognostic Nomogram
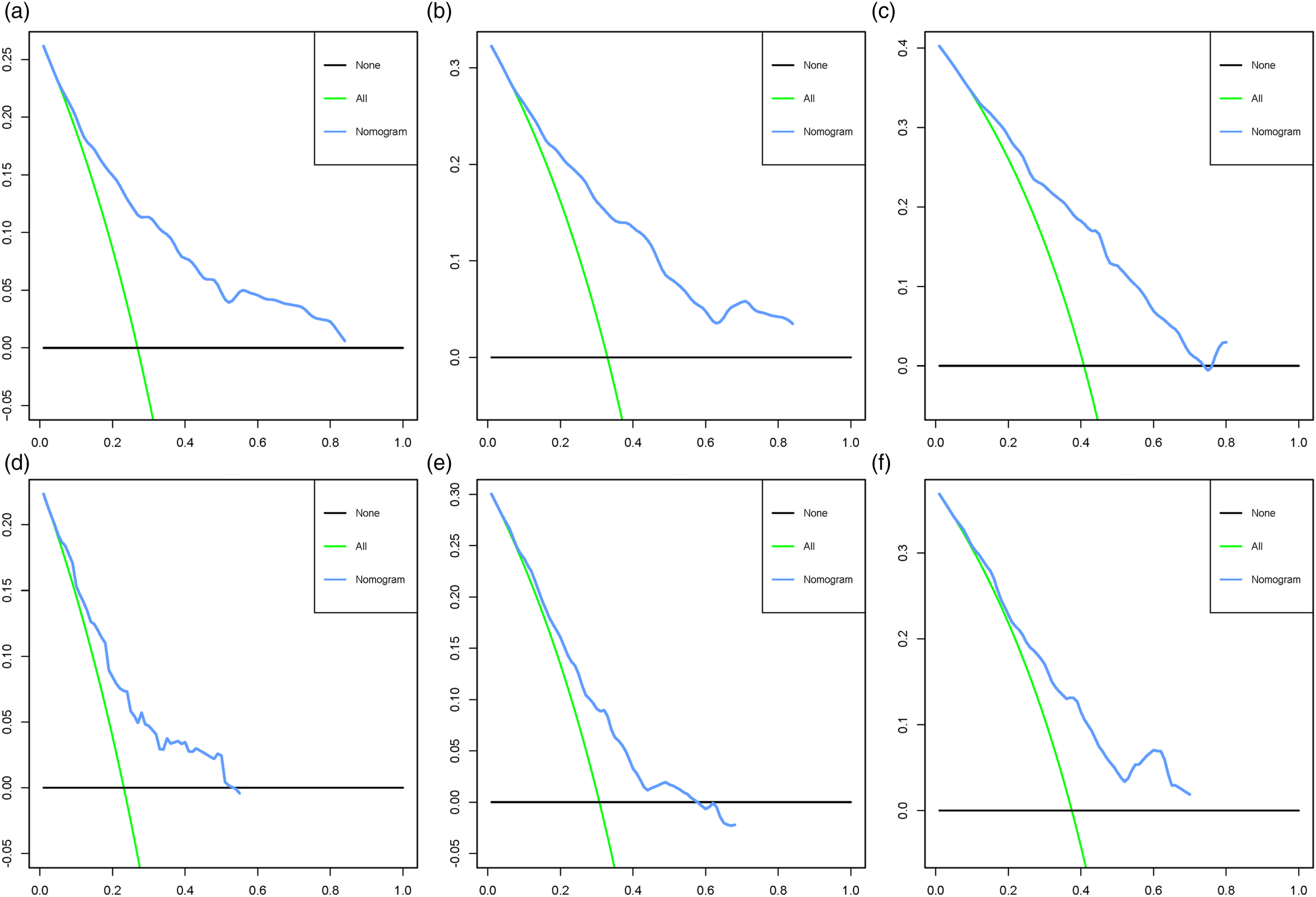
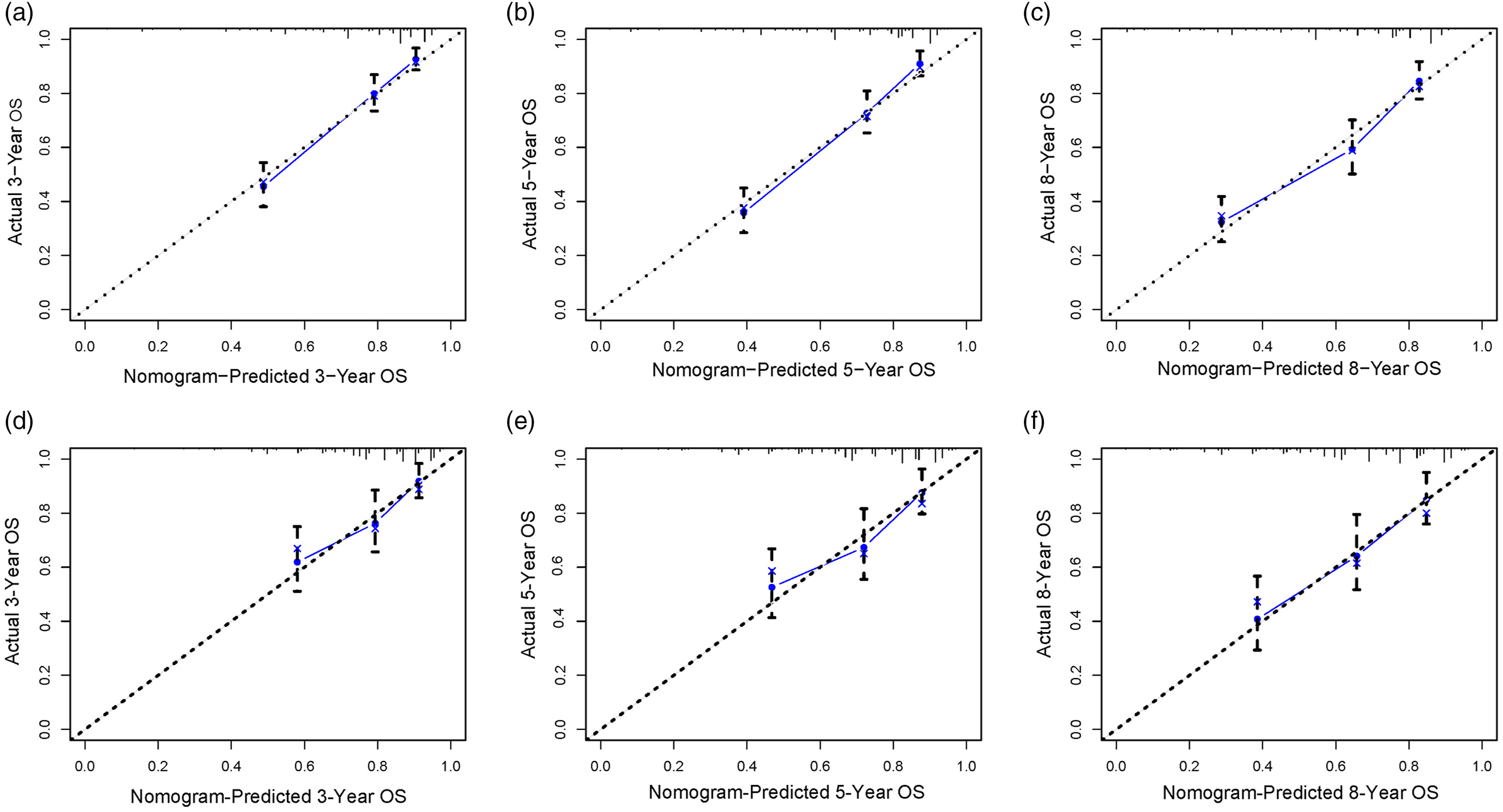
To evaluate the performance of the nomogram, we use 1000 Bootstrap resamples. The results showed that the C index was .757 (95% CI, .683–.831) in the SEER training cohort, .681 (95% CI, .546–.816) in the SEER validation cohort. In addition, the area under the curve values for predicting postoperative OS at 3, 5, and 8 years were greater than .68 in both cohorts, indicating that the nomogram has good discrimination (Figure 3). Across a wide range of mortality risks, decision curve analysis of the 2 cohorts revealed that the nomogram delivered a bigger net benefit than the “all therapy” or “no treatment” option, indicating that the nomogram had good prospective clinical efficacy (Figure 4). The nomogram’s calibration curves revealed good agreement between the nomogram’s projected and observed survival probability in both cohorts (Figure 5). Receiver operating characteristic curves for overall survival prediction of patients. (A) Training cohort, (B) Validation cohort. Decision curve analysis of the nomogram in the training cohort (A–C), validation cohort (D–F), respectively. Calibration curves for 3- (A), 5- (B), and 8-years (C) prediction in the training cohort. Calibration curves for 3- (D), 5- (E), and 8-years (F) prediction in the validation cohort. The x-axis represents the nomogram-predicted survival rates, whereas the y axis represents the actual survival rates.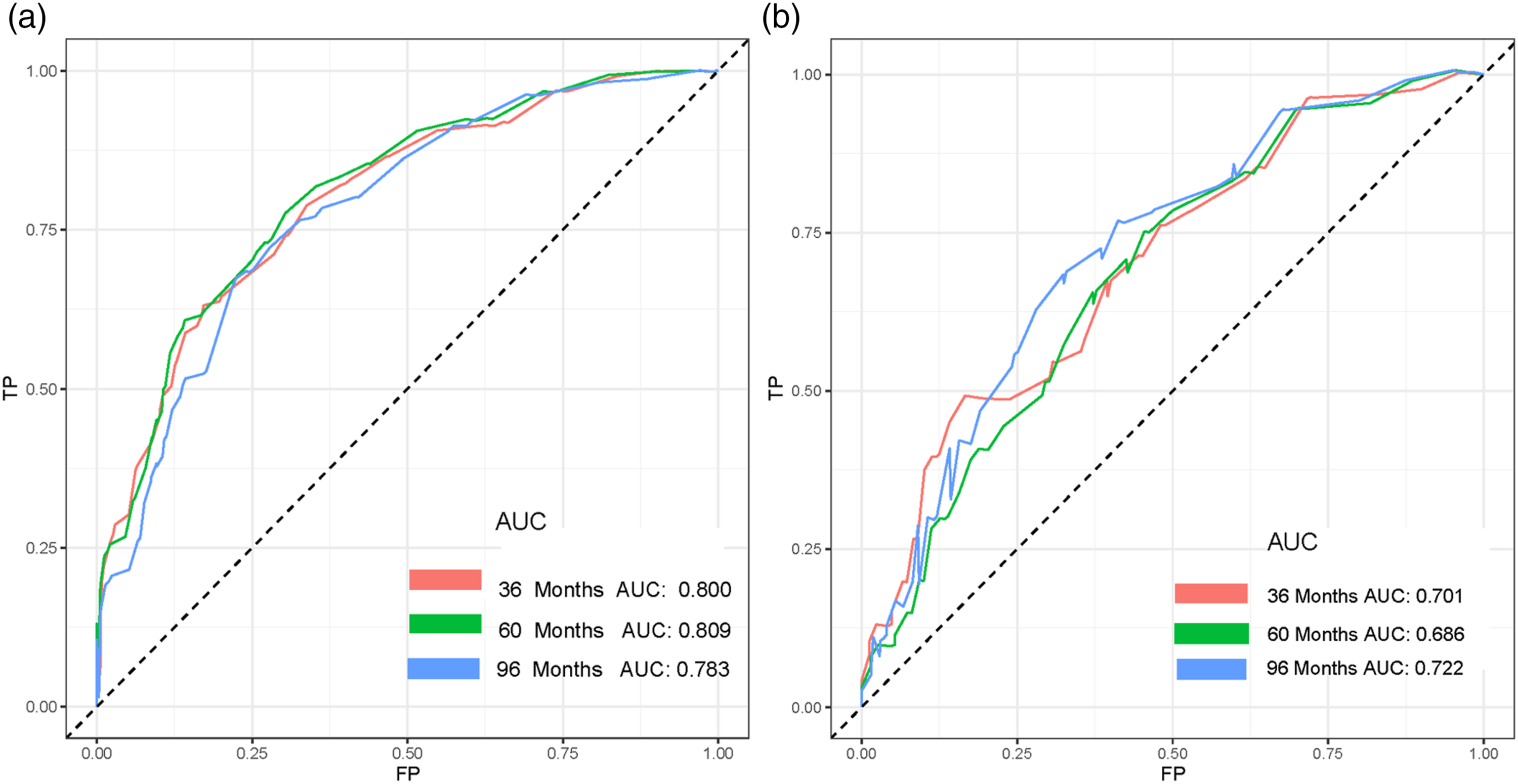
Risk Classification System
The total score of all patients was calculated based on the nomogram, and then risk stratification was performed using X-tile software. The 2 cohorts of patients with primary spinal tumors were classified into a high risk group (total score >237), a middle risk group (192 ≤ total score ≤237), and a low risk group (total score <192). To confirm the stratification of mortality risk, Kaplan-Meier survival curves and log-rank tests were utilized, and the findings revealed a significant difference between the 3 risk groups (Figure 6). The above results suggest that the risk classification system constructed based on nomogram can effectively distinguish patients with primary spinal tumors who have early death after surgery. Kaplan–Meier survival analysis and log-rank tests were performed for comparing postoperative overall survival in the high-risk, middle-risk, and low-risk subgroups of all patients in the training cohort (A) and validation cohort (B).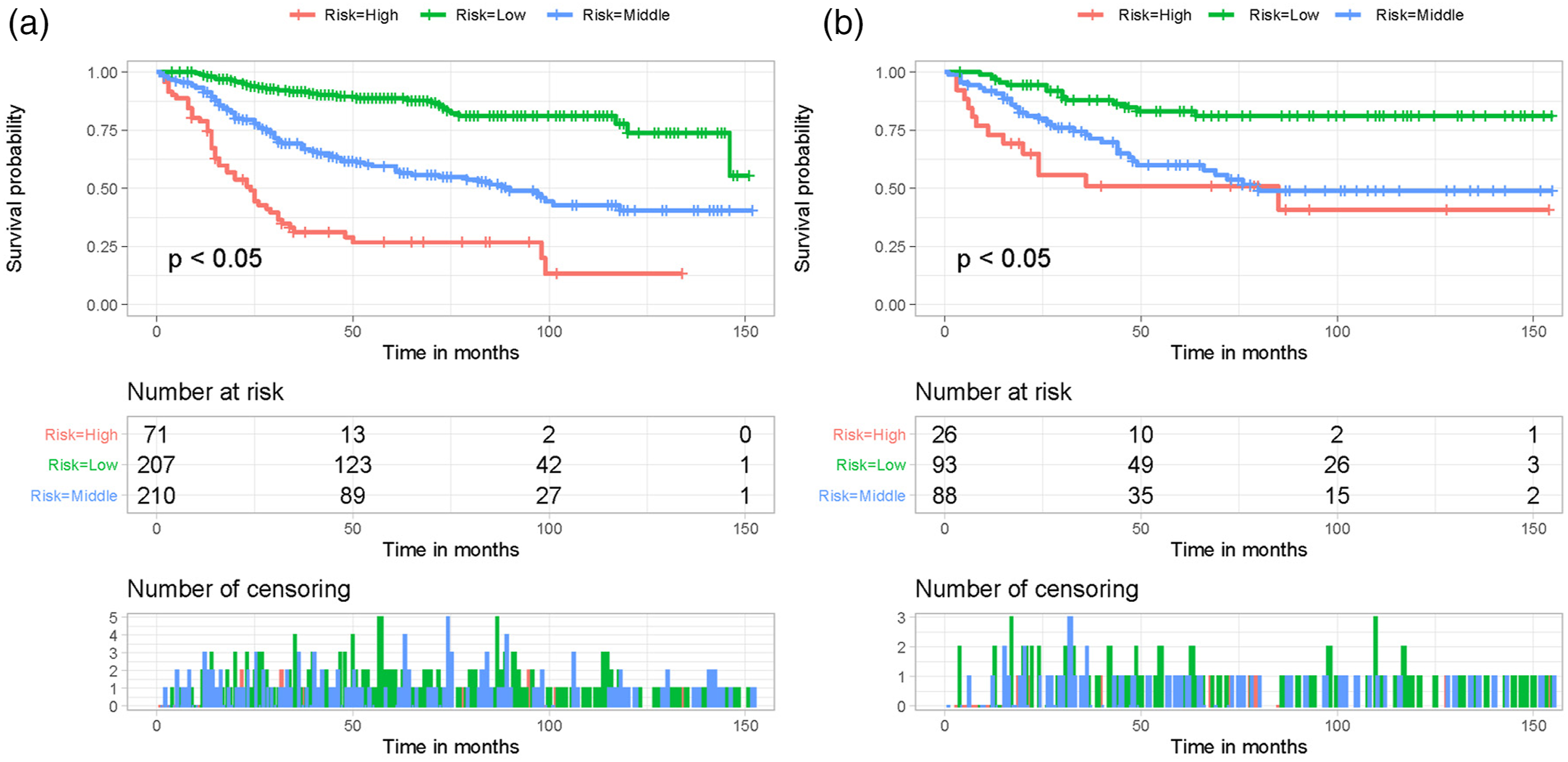
Web-Based Nomogram
As shown in Figure 7, for clinical application, a web-based nomogram was constructed for predicting the postoperative OS of primary spinal tumors patients (https://hzhspine.shinyapps.io/hzhspine/). With the use of the web-based nomogram, we can individually assess the postoperative OS of patients based on the input clinical factors. As an example of calculating OS, we included a 56-year-old white male patient with a primary spinal tumor that was localized, undifferentiated, and had a histological type of chordoma. As shown in Figure 7, the probability of survival for this patient was estimated to be 92.0%, 89.0%, and 85.0% at 3, 5, and 8 years, respectively. A web-based nomogram for predicting postoperative overall survival in primary spinal tumors. The line segments of the graphical summary showed the approximate range of overall survival rates (A). The numerical summary showed the exact values of the overall survival for patients at 36, 60, and 96 months (B).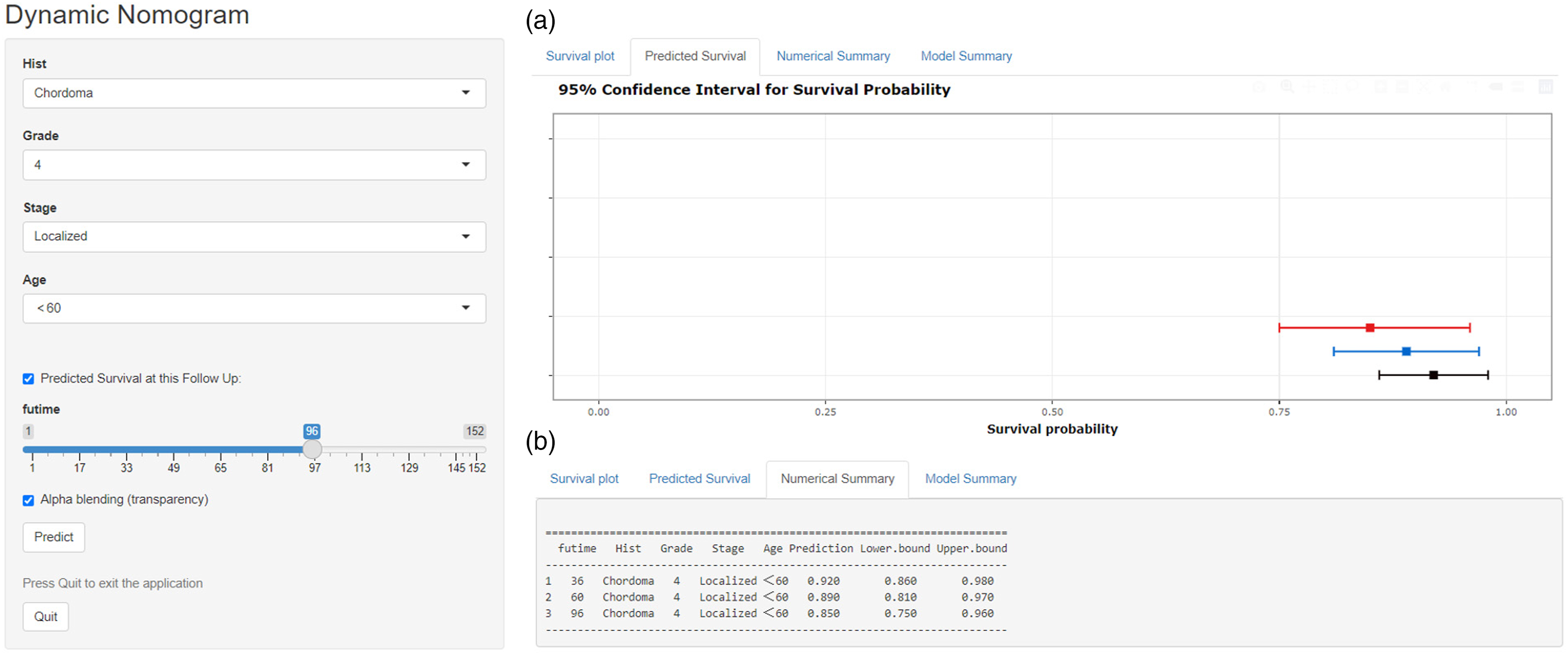
Discussion
Given the rarity of primary spinal tumors, it is difficult to provide an in-depth analysis of their clinical features. Currently, only a few studies have attempted to identify the variables related to poor survival. However, the sample size of these studies is limited, which makes their results not convincing. Also, before our study, there were few large studies to evaluate the OS and associated risk factors in primary spinal tumors patients who had undergone tumor resection.
The spine, which is a special anatomical location, is likely to be damaged by surgery and radiotherapy, making the patient’s quality of life and prognosis even less favorable. 21 With rapid advances in surgical and oncologic treatment, patients with primary spinal tumors have now reached a plateau, although their prognosis has improved from the previous period. Preoperative parameters associated with assessing the clinical characteristics and OS of primary spinal tumors patients help spine surgeons in early diagnosis and treatment decisions but have not yet been fully explored. Therefore, this study retrospectively analyzed 695 patients with postoperative primary spinal tumors from the SEER database to determine the impact of several preoperative parameters on postoperative OS. And based on this, we developed and validated the nomogram and risk stratification system to achieve accurate prediction of postoperative OS of patients. For clinicians'’ ease of use, a web-based nomogram was developed at the same time. This web-based nomogram helps physicians to quickly develop personalized treatment and follow-up plans amid their busy clinical workload.
We determined that 4 preoperative variables, namely, age, disease stage, tumor grade, and histologic type, had an impact on the postoperative OS of patients with primary spinal tumors. In several previous studies, age was shown to be a very important variable affecting the survival of patients with various cancers.22-24 Bergh et al. 25 analyzed the prognosis of 69 patients with chondrosarcoma of the spine and found that patients older than 50 years had poorer survival outcomes. Interestingly, similar results were validated in a retrospective study of 342 malignant primary bony spinal tumors that underwent surgical resection by Matthew et al. 26 The exact mechanism for this phenomenon is not clear. However, one possible explanation may be that the poor physical condition of elderly patients and their reduced tolerance to surgery, chemotherapy, and radiotherapy affects the outcome of treatment, thus making the prognosis poor.4,26 In addition, older patients may have tumors with different molecular profiles (i.e., matrix metalloproteinases) and more aggressive drug resistance genes. 27 We usually consider that patients with poorly differentiated high-grade tumors have a worse prognosis compared to patients with well-differentiated low-grade tumors. The most common histological types of primary spinal tumors include chordoma, osteosarcoma, chondrosarcoma, and Ewing sarcoma. 28 From Figure 1 and the results of multivariate Cox regression analysis, it is easy to see that patients with the histological type of osteosarcoma have the worst prognosis, while chordoma has the best prognosis. Not only was the overall median survival of primary spinal and pelvic tumors histologically related, but patients with spinal osteosarcoma had the worst prognosis, with overall median survival of only 18 months, as reported by Mukherjee et al. 8 In contrast, chordoma is mainly found in the sacrum and vertebrae, and numerous studies have shown that the average survival rate of chordoma is higher than that of other types of spinal tumors.29,30 Whether a patient has developed tumor metastasis is a very critical factor affecting the patient’s prognosis. Previous research on extremities and spine cancers has demonstrated a link between metastatic status and poor survival.31,32 In terms of disease stage, we found that the metastatic disease stage had significantly negative effects on patient survival compared to the localized or regional disease stage. We speculated that this is because these tumors may overexpress matrix metalloproteinases, allowing them to penetrate nearby structures, rendering them less susceptible to surgical excision and potentially more resistant to adjuvant therapy. 27
This study, we believe, gives some important information. First, studies identifying preoperative factors related to postoperative OS in primary spinal tumors patients are few and extremely limited in sample size. Our retrospective analysis of a large sample of recent cases identified 4 independent prognostic factors that improved our understanding of survival in primary spinal tumors patients. Second, this study constructs a practical nomogram model. Meanwhile, the highly accurate prediction and clinical application of the model were confirmed in internal and external validation cohorts. Accurate prediction of individual patient survival and stratification of mortality risk can help guide clinicians to adjust treatment strategies earlier. Despite these very meaningful results, there are still some shortcomings in the present study. First, as a retrospective cohort study, some selection bias is inevitable. Secondly, the SEER database only reports which treatments were performed (surgery, chemotherapy, radiotherapy) but does not retrospectively analyze treatment-specific information such as the regimen of chemotherapy, the dose of radiotherapy, the modality of radiotherapy, etc. Finally, future studies can add variables such as tumor markers and gene expression to this foundation to develop a more comprehensive predictive model.
Conclusion
In summary, we developed a nomogram capable of predicting postoperative OS of primary spinal tumors. The nomogram was validated in a cohort consisting of different populations and ethnicities and showed good predictive accuracy and clinical usefulness. At the same time, the construction of web-based nomograms further facilitates clinical applications, allowing clinicians to provide personalized patient counseling, timely monitoring, and clinical assessment in their work.
Footnotes
Author contributions
Zhangheng Huang and Qingquan Kong conceived and designed the study. Zhangheng Huang and Yuexin Tong performed the literature search. Zhangheng Huang and Yuexin Tong generated the figures and tables. Zhangheng Huang analyzed the data. Zhangheng Huang wrote the manuscript and Qingquan Kong critically reviewed the manuscript. Zhangheng Huang and Qingquan Kong supervised the research. All authors have read and approved the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by, China, Sichuan Science and Technology Program (2020YFS0080, 2020YFQ0007,2021JDRC0159), Science and Technology Project of Tibet Autonomous Region (XZ201901-GB-08), The National Natural Science Foundation of China (81171731), and the 1·3·5 project for disciplines of excellence, West China Hospital, Sichuan University (ZYJC21026, ZYJC21077).
Ethics approval and consent to participate
The study is based on data from public databases and therefore does not require informed consent from patients.